
Abstract
Keywords
Introduction
The most common access vessel in non-cardiac endovascular interventions is the femoral artery, followed by the brachial artery. 1 The latter is commonly used for supra-aortic interventions, visceral vessel interventions, and in cases of difficult femoral artery access.1,2 Despite the superficial course of the brachial artery, puncture and closure at the level of the elbow can be challenging because of the limited underlying bone surface, the proximity of veins and nerves, and vessel mobility. 3 Some vascular surgeons favor cutdown techniques to reduce the risk of access complications. 4 However, many others will perform percutaneous brachial punctures and use manual compression as the standard means of achieving hemostasis. 5
The Perclose ProGlide Suture-Mediated Closure System (Abbott Vascular, Redwood City, CA, USA) could be an attractive alternative for brachial artery closure based on use of the precursor 6-F Perclose device (Abbott Vascular Devices) after coronary interventions in two small series.6,7 Our team has a broad experience with ProGlide closure for transfemoral aortic interventions, and we and others have used this device successfully in more proximal upper extremity arteries.8,9 To our knowledge, use of the ProGlide in the brachial artery has not been described in the literature.
The goal of this study was to assess the feasibility of the ProGlide closure of the brachial artery, evaluating access-related complications and reinterventions in patients who underwent a transbrachial endovascular intervention and to compare these results with manual compression.
Materials and Methods
Study Design
A pilot study was begun in 2016 at the Maastricht University Medical Center to evaluate the ProGlide for puncture closure in >4-mm-diameter brachial arteries when a >6-F sheath was used in an endovascular intervention. The operators involved in the study were highly experienced users (>100 ProGlides). All patients gave informed consent to the index procedure. Data collection and evaluation of anonymized data for this retrospective study was approved by the local ethics committee.
Safety monitoring for the study was based on a 60-patient historical cohort in whom brachial artery hemostasis had been achieved by manual compression in interventions performed between 2014 and 2017. A control group was derived from this cohort by matching to the test group based on the use of ultrasound-guided puncture, type of intervention, periprocedural anticoagulation, and a minimum 6-F sheath size.
Procedure and Follow-up
All patients received antibiotic prophylaxis prior to the procedure. Patients were positioned with the access arm abducted at a 90° angle. After ultrasound identification and measurement of the distal brachial artery, an ultrasound-guided puncture was performed using a 4-F, 10-cm-long cannula from a micropuncture set (Cook Medical, Bloomington, IN, USA). Correct puncture was confirmed with ultrasound or radiography, and the intervention was performed through a sheath of suitable diameter for the specific intervention. After sheath insertion, each patient received 5000 units of heparin; additional heparin (2500 units) was administered as needed to maintain the activated clotting time >250 seconds. At the end of the procedure a ProGlide was inserted over a Glidewire (Terumo, Tokyo, Japan) and deployed according to the instructions for use.
Each patient was examined for periprocedural and access complications during hospitalization and at the 30-day visit. Computed tomography was performed during follow-up for the performed interventions.
Data Collection and Outcomes
The historical cohort was identified by interrogating a prospectively maintained database. Data for the ProGlide group and the historical cohort were retrieved from the electronic hospital database, including patient demographics, comorbidities, interventional results, access characteristics and complications, and access-related reinterventions.
The primary outcome was access complications leading to reinterventions; the secondary outcome was brachial access–site complications (hematoma, hemorrhage, neurological complication, pseudoaneurysm, and arterial occlusion).
Statistical Analysis
Continuous data are presented as the mean; categorical data are given as the number. The Mann-Whitney U test was used to evaluate continuous variables. Categorical outcomes were compared using the Fisher exact test. The threshold of statistical significance was p<0.05. Statistical analysis was performed using SPSS for Windows software (version 24.0; IBM Corporation, Armonk, NY, USA).
Results
Seven patients (mean age 67.9 years; 6 men) were enrolled in the study before it was stopped in 2017 (Table 1). Target vessels included the thoracic and abdominal aorta and supra-aortic vessels. All interventions were completed successfully. Four patients experienced 6 access-site complications (Table 2). Two patients developed a hematoma leading to pressure neuropathy of the radial nerve, 1 patient had a pseudoaneurysm, and 1 patient suffered a brachial artery occlusion. There were 3 access-related reinterventions: surgical evacuation of a hematoma, thrombectomy and repair of the occluded brachial artery, and surgical repair of the pseudoaneurysm.
Patient Demographics and Medical History. a
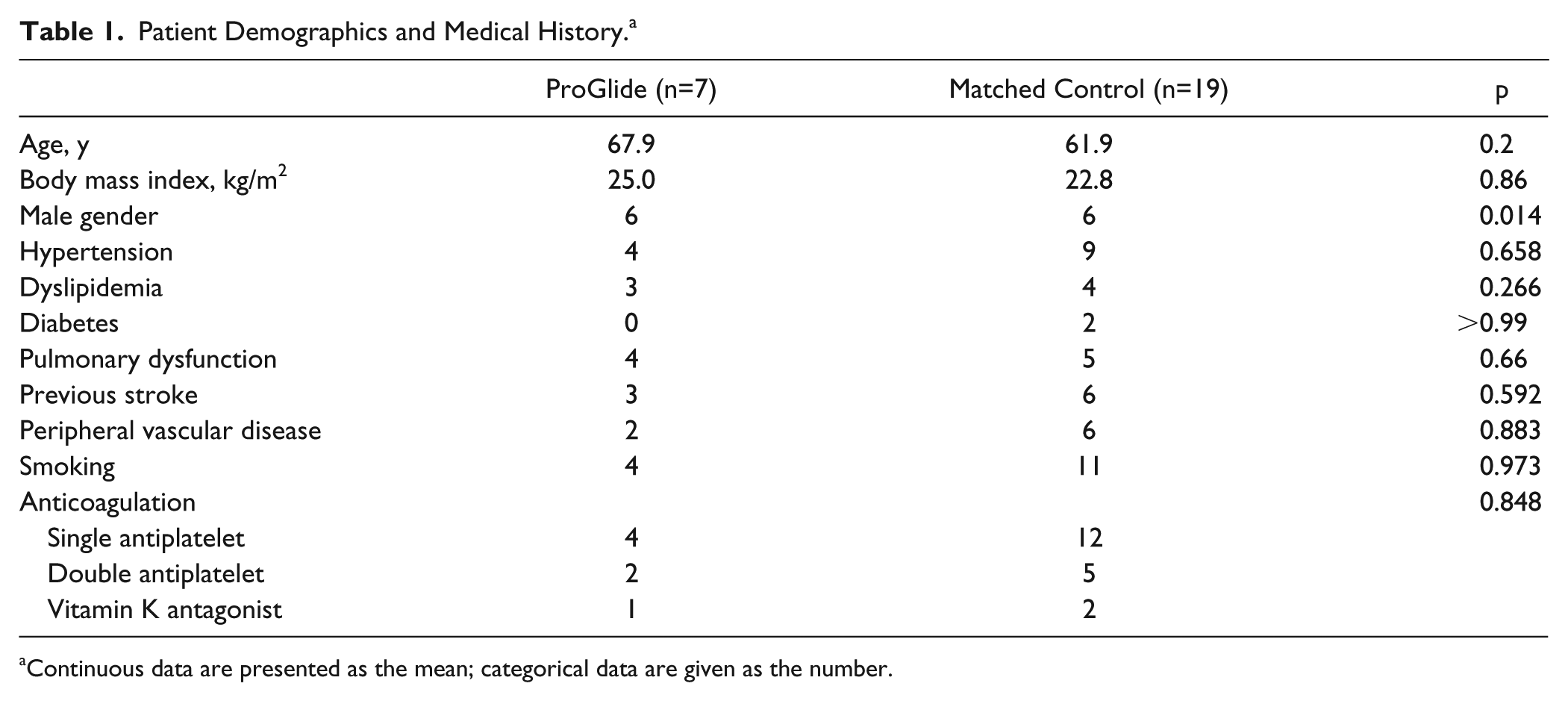
Continuous data are presented as the mean; categorical data are given as the number.
Procedure Outcomes.
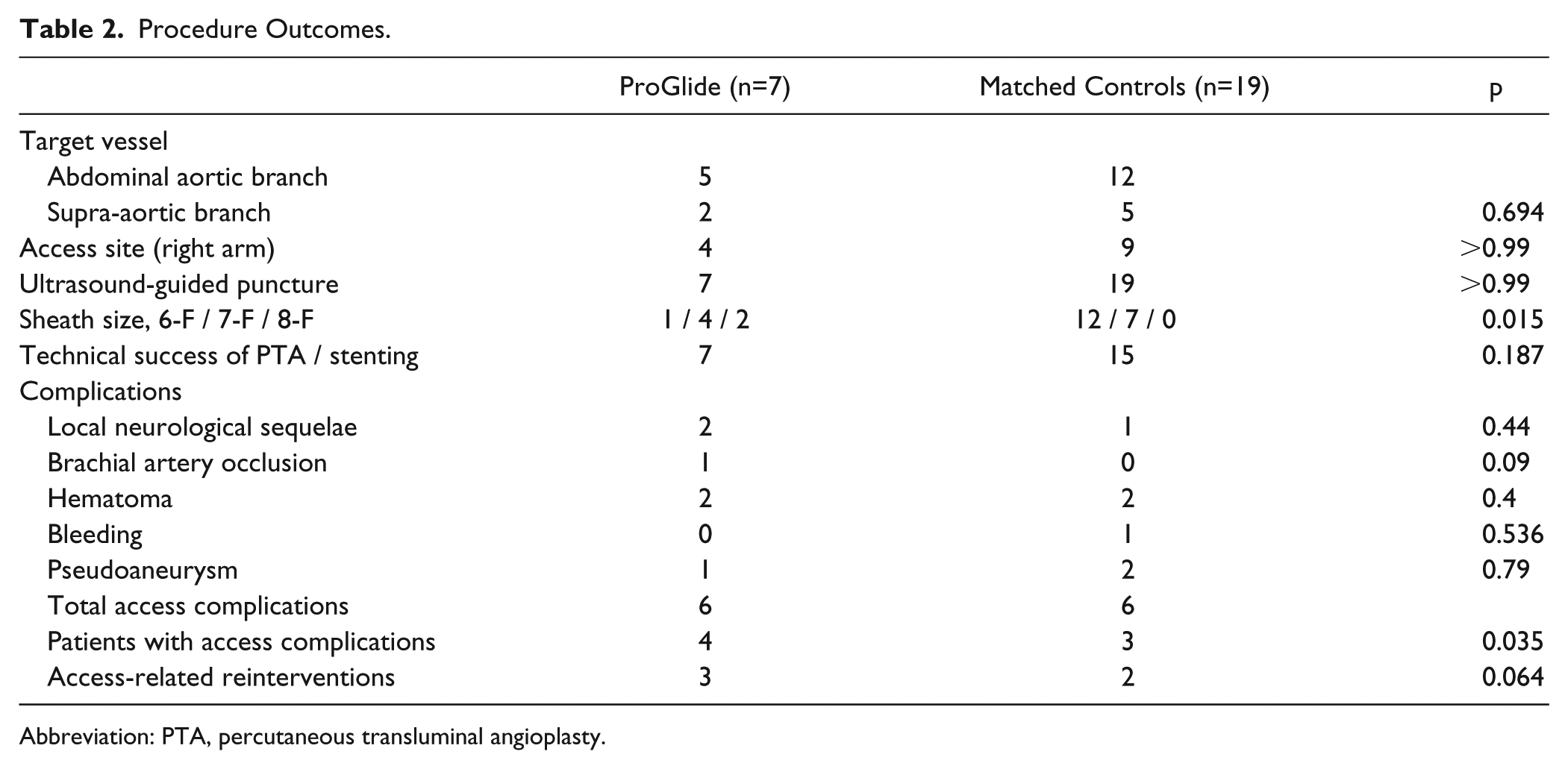
Abbreviation: PTA, percutaneous transluminal angioplasty.
In an interim analysis, these results were compared to a 19-patient matched control group (mean age 61.9 years; 6 men) selected from among the 60-patient historical cohort in whom brachial artery hemostasis had been achieved by manual compression. Baseline characteristics (Table 1) of the 2 groups differed only in the greater proportion of men and the use of larger sheaths in the ProGlide patients (Table 2). In terms of outcomes (Table 2), the ProGlide group had proportionally more patients experiencing access-related complications (57% vs 16% for manual compression, p=0.035) and resultant reinterventions (43% vs 11%, p=0.064). On this basis the trial was stopped.
Discussion
While the ProGlide has proven to be feasible, safe, and cost-effective in several types of percutaneous transfemoral interventions, 10 there has been no reported experience with this generation of the device in transbrachial interventions. Other vascular closure devices (VCDs) have been reported as safe and feasible for use in the brachial artery; however, despite these results, percutaneous closure has not been adopted in the brachial artery, essentially because the positive results could not be reproduced by others. We hypothesized that the ProGlide would be suitable for use in the brachial artery because the device is more delicate than other VCDs that have already proven to be feasible in the brachial artery (Table 3). Unfortunately, 4 of 7 patients experienced access-related complications, leading to reinterventions in 3. In both the entire 60-patient historical cohort with manual compression for brachial artery closure and the matched subgroup, access complications and resultant reinterventions were proportionally less. It was on this basis that the pilot study on ProGlide closure of the distal brachial artery was halted.
Results of Vascular Closure Device Use in the Brachial Artery.
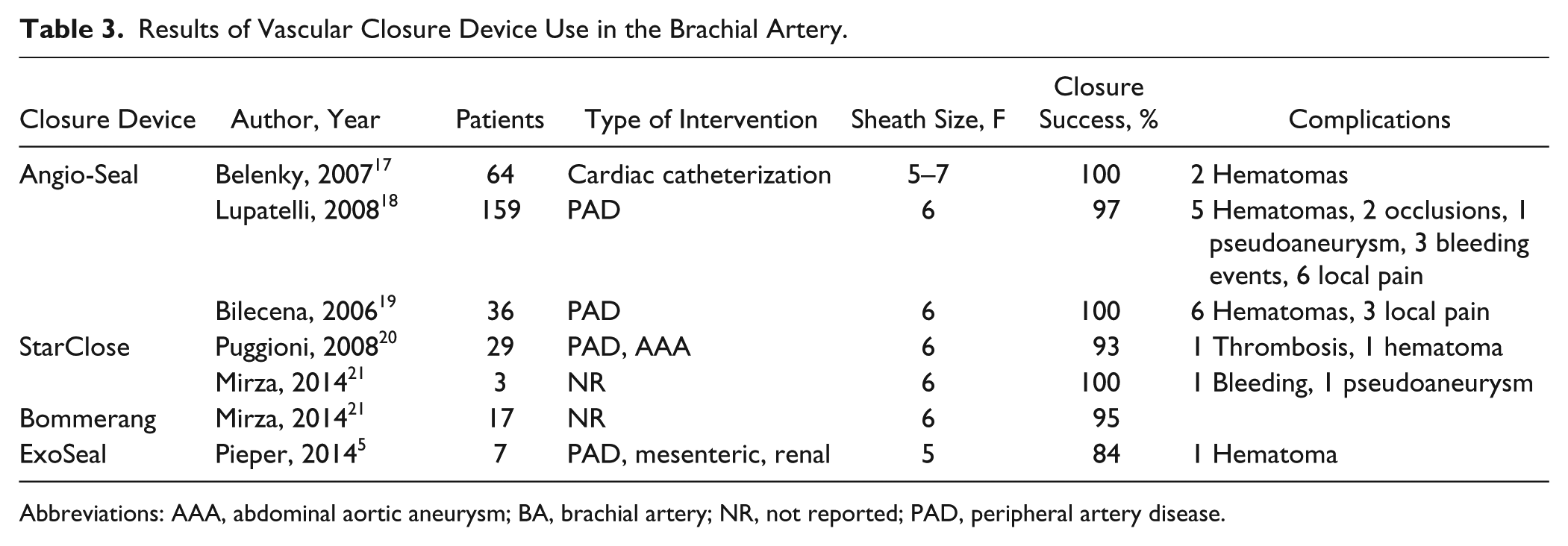
Abbreviations: AAA, abdominal aortic aneurysm; BA, brachial artery; NR, not reported; PAD, peripheral artery disease.
The brachial artery can be accessed in different fashions. Knowles et al 11 described significantly fewer access complications after open exposure (2% vs 17%) compared with percutaneous access of the high brachial artery. Furthermore, in 2019 Mirza et al 12 published a large retrospective analysis of the 243 patients who underwent proximal brachial artery cutdown to undergo fenestrated/branch endovascular aortic repair; just 3 patients developed a serious access-related complication. Bertoglio et al 9 focused on the use of the ProGlide after a percutaneous approach of the axillary artery and outlined in their discussion that the ProGlide was unsuccessfully used 3 times in the high brachial artery. Kim et al 7 used a suture-mediated closure device 8 times in the brachial artery to achieve hemostasis after coronary interventions and imaging; they encountered 2 access complication and 1 reintervention. Previous results of the ProGlide in the brachial and axillary arteries are summarized in Table 4.
Results of the ProGlide Suture-Mediated Closure System in the Axillary and Brachial Arteries.
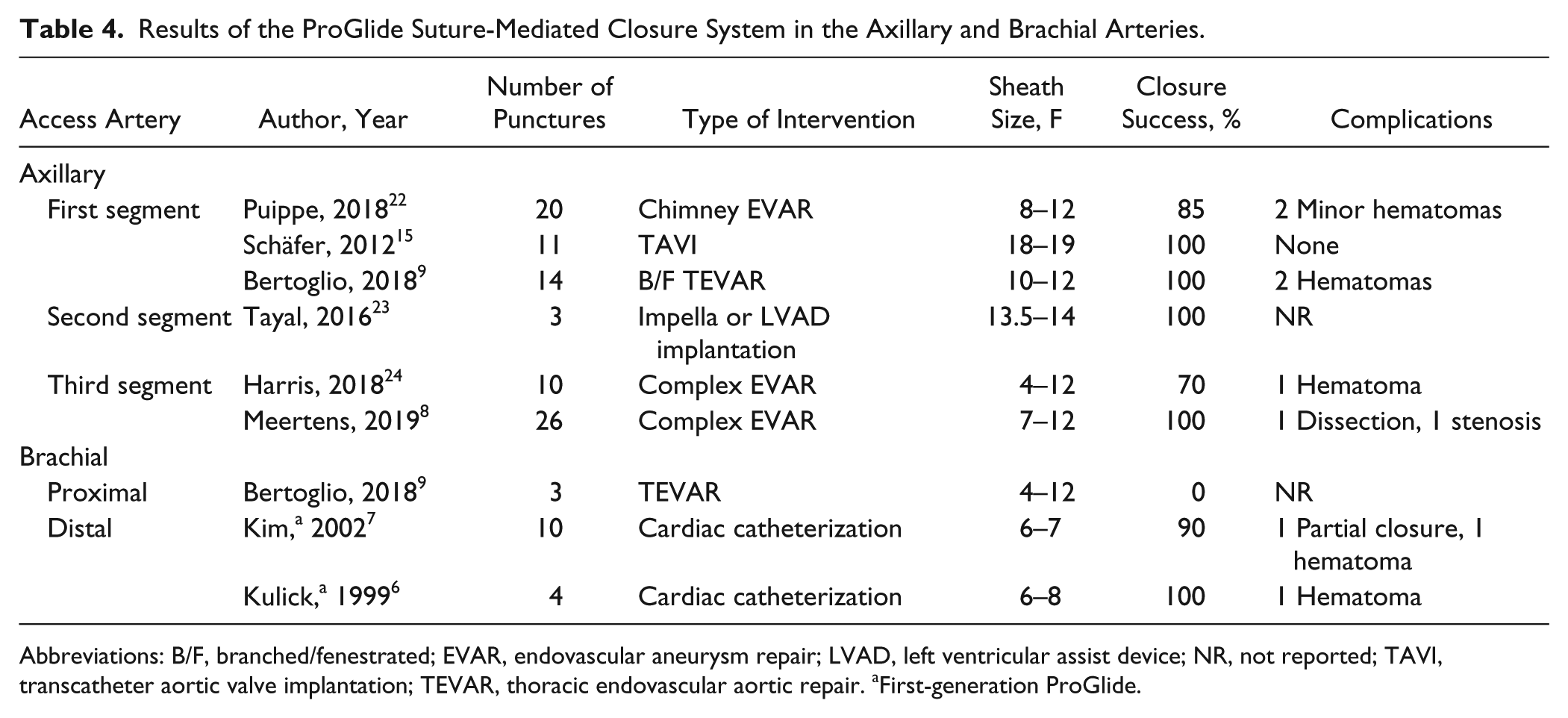
Abbreviations: B/F, branched/fenestrated; EVAR, endovascular aneurysm repair; LVAD, left ventricular assist device; NR, not reported; TAVI, transcatheter aortic valve implantation; TEVAR, thoracic endovascular aortic repair. aFirst-generation ProGlide.
There are several possible causes that might contribute to failure of the ProGlide in the brachial artery. Kenth at al 13 showed that a larger sheath size increases the complication rate in transbrachial interventions. The average diameter of the distal brachial artery is 4.4 mm. 14 The smaller diameter of the brachial artery may lead to incomplete deployment of the footplate of the device, resulting in the suture penetrating the posterior wall and occluding the vessel. Furthermore, the superficial location of the brachial artery may lead to involvement of the dermis in the suture, thus only partially closing the access puncture. Moreover, not only the size 14 but also the composition distinguishes the brachial artery from the femoral artery, which contains more elastic fibers than the vessel walls of the upper extremity arteries. 15 Therefore, the brachial artery wall is thinner, which may lead to rupture of the suture through the vessel wall when force is applied.15,16
Limitations
The limitations of our study are the small sample size, the retrospective design of the control group, the lack of randomization and blinding, and the fact that no post-closure duplex was performed for quality assessment. Based on our high complication and reintervention rate we are reluctant to perform further evaluation of the ProGlide for brachial closure.
Conclusion
Based on this pilot study, it is not advisable to use the ProGlide device in transbrachial interventions due to the increased incidence of complications and access-related reinterventions. Manual compression remains the standard for hemostasis after distal brachial artery puncture; when larger sheaths are necessary, cutdown over the artery is a safe alternative.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.