
Abstract
Purpose:
To evaluate the safety and performance of the Treovance stent-graft.
Methods:
The global, multicenter RATIONALE registry (ClinicalTrials.gov; identifier NCT03449875) prospectively enrolled 202 patients (mean age 73.0±7.8 years; 187 men) with abdominal aortic aneurysms (AAA) suitable for endovascular aneurysm repair (EVAR) using the Treovance. The composite primary safety endpoint was site-reported all-cause mortality and major morbidity. The primary efficacy outcome was clinical success. Further outcomes evaluated included technical success; stent-graft migration, patency, and integrity; endoleak; and aneurysm size changes.
Results:
Technical success was 96% (194/202); 8 patients had unresolved type I endoleaks at the end of the procedure. There was no 30-day mortality and 1% major morbidity (1 myocardial infarction and 1 bowel ischemia). Clinical success at 1 year was confirmed in 194 (96%) patients; 6 of 8 patients had new/persistent endoleaks and 2 had aneurysm expansion without identified endoleak. A total of 8 (4%) reinterventions were required during the mean 13.7±3.1 months of follow-up (median 12.8). At 1 year, the Kaplan-Meier estimate for freedom from reintervention was 95.6% (95% CI 91.4% to 97.8%). Other estimates were 95.5% (95% CI 91.7% to 97.6%) for freedom from endoleak type I/III and 97.4% (95% CI 94.2% to 98.9%) for freedom from aneurysm expansion. Thirteen (6.4%) patients died; no death was aneurysm related.
Conclusion:
The RATIONALE registry showed favorable safety and clinical performance of the Treovance stent-graft for the treatment of infrarenal AAAs in a real-world setting.
Keywords
Introduction
Endovascular aortic repair (EVAR) is a less invasive alternative to open surgical repair and has become the preferred method for abdominal aortic aneurysm (AAA) treatment because of improved mortality outcomes, fewer operative complications, and fewer postoperative adverse events.1–4 Prior randomized controlled trials and registries estimated short-term 30-day mortality to be approximately 1% to 2%.5–14 Since their introduction, endovascular devices have improved and increased the applicability of EVAR to a wide range of AAA anatomies, but severely angulated infrarenal aortic necks and tortuous iliac arteries still restrict commercially available devices to limited prespecified anatomies.15,16 Long-term success of EVAR is determined by rates of aneurysm sac growth, endoleak, and reintervention.13,17 Consequently, next-generation device development focuses on mechanisms to improve long-term stent-graft performance and effectiveness.18,19
The Treovance abdominal stent-graft system [Terumo Aortic (formerly Bolton Medical), Sunrise, FL, USA] is Conformité Européenne–marked for repair of infrarenal AAAs. Unique features include a trimodular design to adapt better to various anatomies and 3 main body lengths (80, 100, and 120 mm) to facilitate cannulation time by approaching close to the aortic bifurcation. A detachable sheath minimizes trauma to access vessels during introduction and withdrawal of the delivery system. The main body has an overlapping proximal end configuration with 3 seal points per apex: the larger diameter devices (30–36 mm) have 6 peaks (18 seal points) and the smaller (20–28 mm) have 5 (15 seal points). The device is the only AAA stent-graft with dual proximal fixation; infrarenal barbs provide additional fixation and contribute to migration resistance in large, angulated necks. The device’s lock stents (dull barbs on the legs of the bifurcated graft) are designed to reduce component separation and type III endoleaks. Assessments of pullout forces 20 showed that increasing infrarenal angulation decreases the force needed to dislodge modular stent-grafts. A comparison of 6 different stent-grafts demonstrated strong fixation for the Treovance (pullout forces of 39.3 to 23.9 N from 0° to 90°). The stent-graft performed favorably in the ADVANCE 21 clinical trial as well as single-center and dual-center cohorts.22–24
The objective of this global registry was to evaluate safety and performance of the Treovance stent-graft in patients with infrarenal AAAs.
Methods
Study Design
The RATIONALE registry was a global, prospective, multicenter clinical investigation to collect clinical data on the use and performance of the Treovance stent-graft at up to 1 year. Investigators from 32 institutions in 17 countries (Appendix) enrolled patients prospectively after the decision to treat but before implantation. Data were recorded on a web-based electronic case report form (OpenClinica), which was monitored and queried when necessary, but there was no monitoring board or adjudication committee. Data were also reviewed with automatic filters to detect missing information and inconsistencies. The registry was conducted in accordance with the Declaration of Helsinki and patients gave consent prior to participation. The ethics approval process was in accordance with requirements at each institution. The trial was registered on the National Institutes of Health website (ClinicalTrials.gov; identifier NCT03449875).
Inclusion/Exclusion Criteria
Patients between the ages of 18 and 85 years were eligible for entry in the registry if they had an infrarenal AAA >4.5 cm for women and >5 cm for men and met the infrarenal neck criteria specified in the instructions for use (IFU): length ⩾10 mm with a <60° proximal angle, a <45° suprarenal angle, and an inside diameter of 17 to 32 mm or length ⩾15 mm with a 60° to 75° proximal angle, a <45° suprarenal angle, and an inside diameter of 16 to 30 mm. Iliac artery requirements for use of the Treovance were a distal iliac neck ⩾10 mm long with an inside diameter of 7 to 13 mm or a ⩾15-mm-long iliac neck with an inside diameter of >13 to 20 mm. Other criteria included no significant infrarenal or distal iliac neck calcification or thrombus formation; lowest renal artery ⩾90 mm from the aortic bifurcation; and a total treatment length ⩾130 mm. The main exclusion criteria were dissection or a ruptured aneurysm, prior AAA repair (endovascular or surgical), conical necks, and/or serious cardiovascular, respiratory, metabolic, infectious, renal, or hematologic comorbidity.
Patient Population
Between February 2014 and April 2017, 202 patients (mean age 73.0±7.8 years; 187 men) were enrolled and followed prospectively. The majority of patients (Table 1) were white (91.6%), male (92.6%), and had a risk factor profile typical of vascular disease patients. More than half were classified American Society of Anesthesiologists class III/IV (58.0%). The mean length of the proximal neck was 25.7±12.1 mm, and the mean aneurysm sac size at baseline was 58.6±10.8 mm (Table 2). The mean suprarenal angle was 14.8°±14.6°, and the mean infrarenal angle was 27.7°±20.2°; 21 (10.4%) patients had an infrarenal angle ⩾60°. Regarding access site characteristics, 34 (16.8%) patients had iliac artery involvement; 36 (17.9%) had moderate or severe calcification in access artery; and 50 (24.8%) had moderate or severe tortuosity of the access artery.
Baseline Data for the 202 Patients in the Registry. a
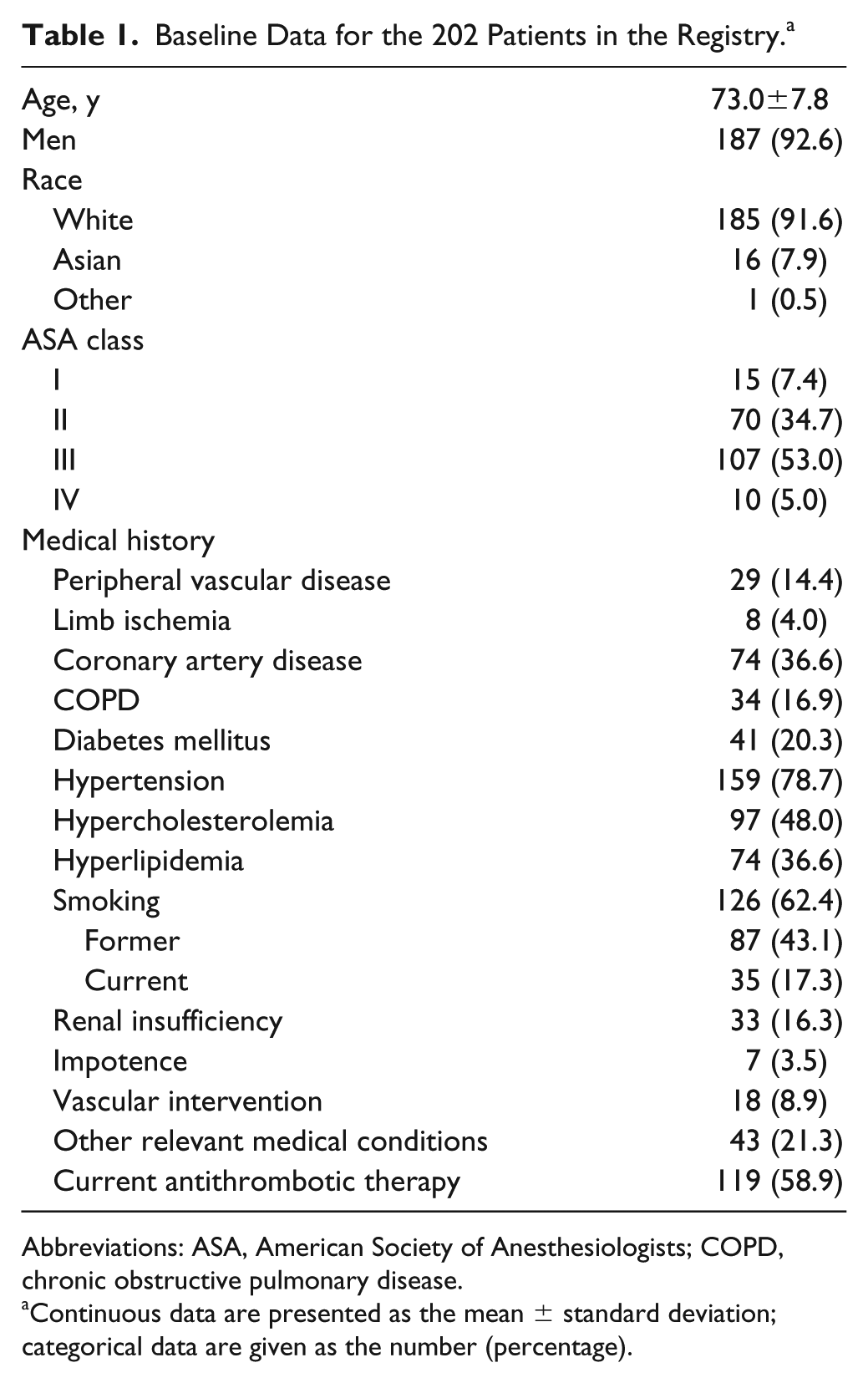
Abbreviations: ASA, American Society of Anesthesiologists; COPD, chronic obstructive pulmonary disease.
Continuous data are presented as the mean ± standard deviation; categorical data are given as the number (percentage).
Lesion Measurements/Characteristics and Device Sizing for the 202 Patients in the Registry. a
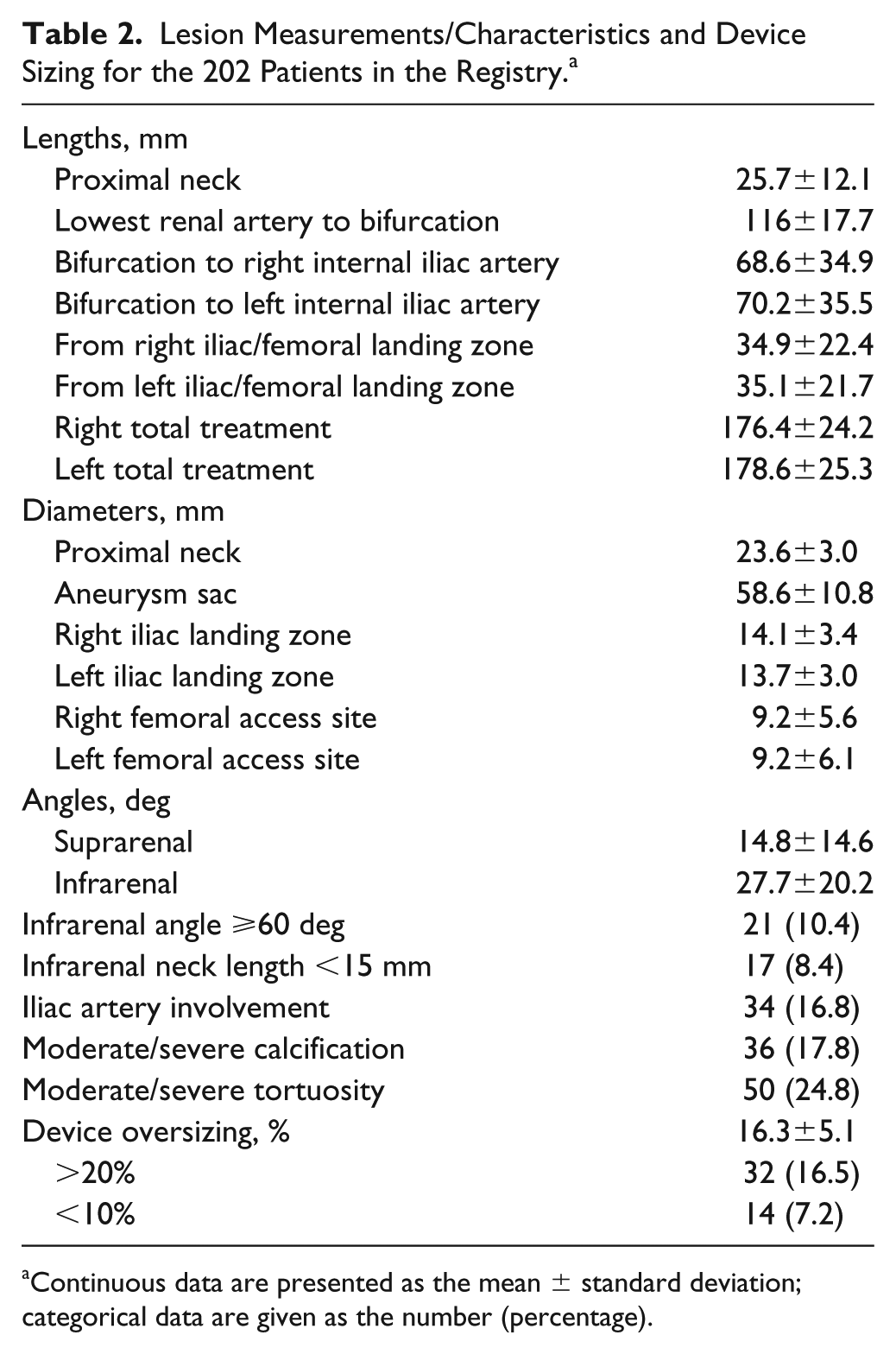
Continuous data are presented as the mean ± standard deviation; categorical data are given as the number (percentage).
Definitions and Outcomes
The composite 30-day primary safety endpoint was site-reported all-cause mortality and major morbidity, the latter categorized as stroke (excluding transient ischemic attack), myocardial infarction, renal failure requiring renal replacement therapy (excluding renal insufficiency), respiratory failure (excluding chronic obstructive pulmonary disease or pulmonary complications), bowel ischemia, or aneurysm rupture. Aneurysm-related mortality was death due to aneurysm rupture, a primary or secondary procedure, or surgical conversion. During data analysis, adverse events were codified and graded as complications according to the Society for Vascular Surgery EVAR reporting standards whenever possible. 25
The primary efficacy outcome was clinical success. According to current guidelines, 25 clinical success required successful deployment of the endovascular device at the intended location without death as a result of aneurysm-related treatment, type I/III endoleak, graft infection or thrombosis, aneurysm expansion (diameter ⩾5 mm or volume ⩾5%), aneurysm rupture, or conversion to open repair. Primary clinical success was achieved without the need for an additional or secondary surgical or endovascular procedure; assisted primary clinical success referred to the use of an additional or secondary endovascular procedure, while secondary clinical success involved the use of an additional/secondary surgical procedure. 25
Primary technical success was defined as the successful introduction and deployment of the device in the absence of surgical conversion, mortality, type I/III endoleaks, or graft limb obstruction. The use of unplanned endovascular procedures to achieve success was termed assisted primary technical success, while secondary technical success referred to the use of unplanned surgical procedures.
Further outcomes evaluated included device delivery, stent-graft migration, patency (blood flow through the treated vessel and stent-graft), integrity (absence of stent-graft fractures, kinking, or twisting leading to occlusion or ischemia), endoleak, aneurysm size changes, limb ischemia, vascular access complications, and type of anesthesia. Baseline data [including computed tomography (CT)] were collected prior to any surgical intervention, after the procedure, prior to hospital discharge, and up to 1-year follow-up according to standard practice at each site and including at least 1 postimplant CT scan.
Statistical Analysis
All variables were reported descriptively with no hypothesis testing; categorical variables are given as the frequencies and percentages, while continuous variables are presented as the mean ± standard deviation with 95% confidence interval (CI), median, and interquartile range (IQR; Q1, Q3). All enrolled patients were evaluated in follow-up. Continuous variables were compared with the Wilcoxon signed-rank test. Freedom from reintervention, type I/III endoleak, and aneurysm expansion were analyzed using the Kaplan-Meier method. Statistical significance was set at p<0.05. All analyses were performed with SAS software (version 9.4; SAS Institute, Inc, Cary, NC, USA).
Results
Technical success was confirmed in 96.0% of patients (Table 3); success was assisted in 9 with the use of extensions or cuffs and balloon angioplasty to fix intraoperative endoleaks and intraoperative limb occlusion, and 1 patient with severe bilateral access vessel calcification required thromboendarterectomy and a crossover bypass following access vessel rupture. The 8 failures were due to unresolved type I endoleak at the end of the procedure.
Intraoperative and Perioperative Results for the 202 Patients in the Registry. a
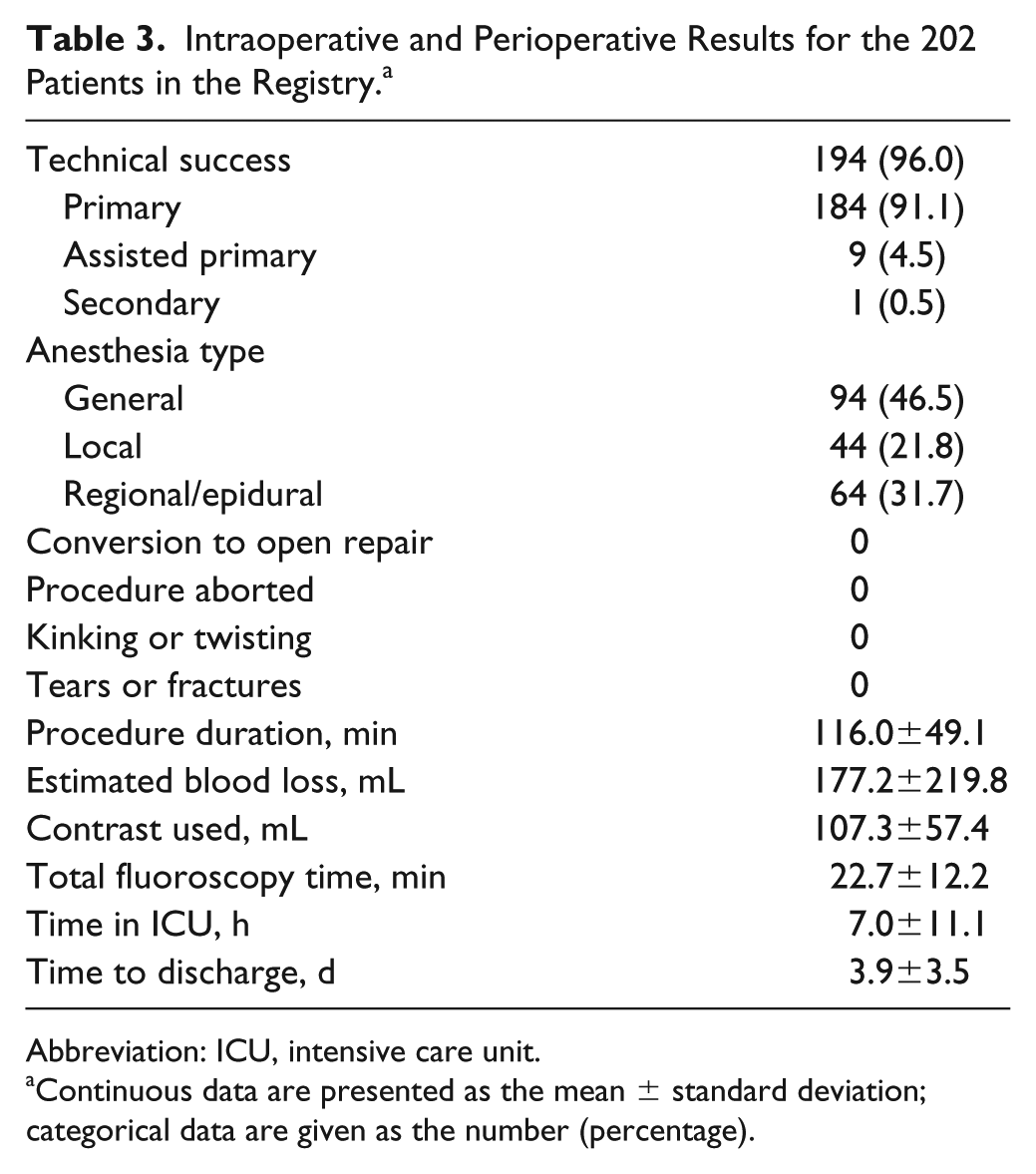
Abbreviation: ICU, intensive care unit.
Continuous data are presented as the mean ± standard deviation; categorical data are given as the number (percentage).
More than half (108, 53.5%) of the interventions were conducted using local or locoregional anesthesia. One third of patients (68, 33.7%) had percutaneous access; 17 (8.5%) had access vessel dilation but none required thrombectomy or conduits. Mean procedure time was 116±49.1 minutes, during which 107.3 mL of contract was used in conjunction with 22.7 minutes of fluoroscopy. The mean estimated blood loss was 177.2 mL (3 patients had blood loss ⩾1000 mL). Fewer than half the patients (98, 48.5%) required intensive care unit admission; of those, 33 were admitted for ⩽6 hours. The mean hospital stay from the day of implant was 3.9±3.5 days.
There was no mortality and 1% major morbidity [1 myocardial infarction (nonserious, resolved in 3 days) and 1 bowel ischemia] during the perioperative period (Table 4); the single cerebrovascular event was a temporary speech disorder (recovery within 24 hours); the other cardiac complication was atrial fibrillation. Four (2.0%) limb occlusions occurred; 1 was resolved during the index procedure as noted above and was not associated with thrombosis. The other 3 occurred during follow-up and 2 were treated with endovascular repair, 1 with a bypass. Of the 8 (4%) patients with type I endoleaks at the end of the procedure, 6 endoleaks resolved by the first follow-up (5 spontaneously and 1 with a limb extension); 2 were persistent at first follow-up. Three of the patients whose type I endoleak resolved spontaneously had device oversizing >20%.
Complications in the 202 Patients in the Registry. a
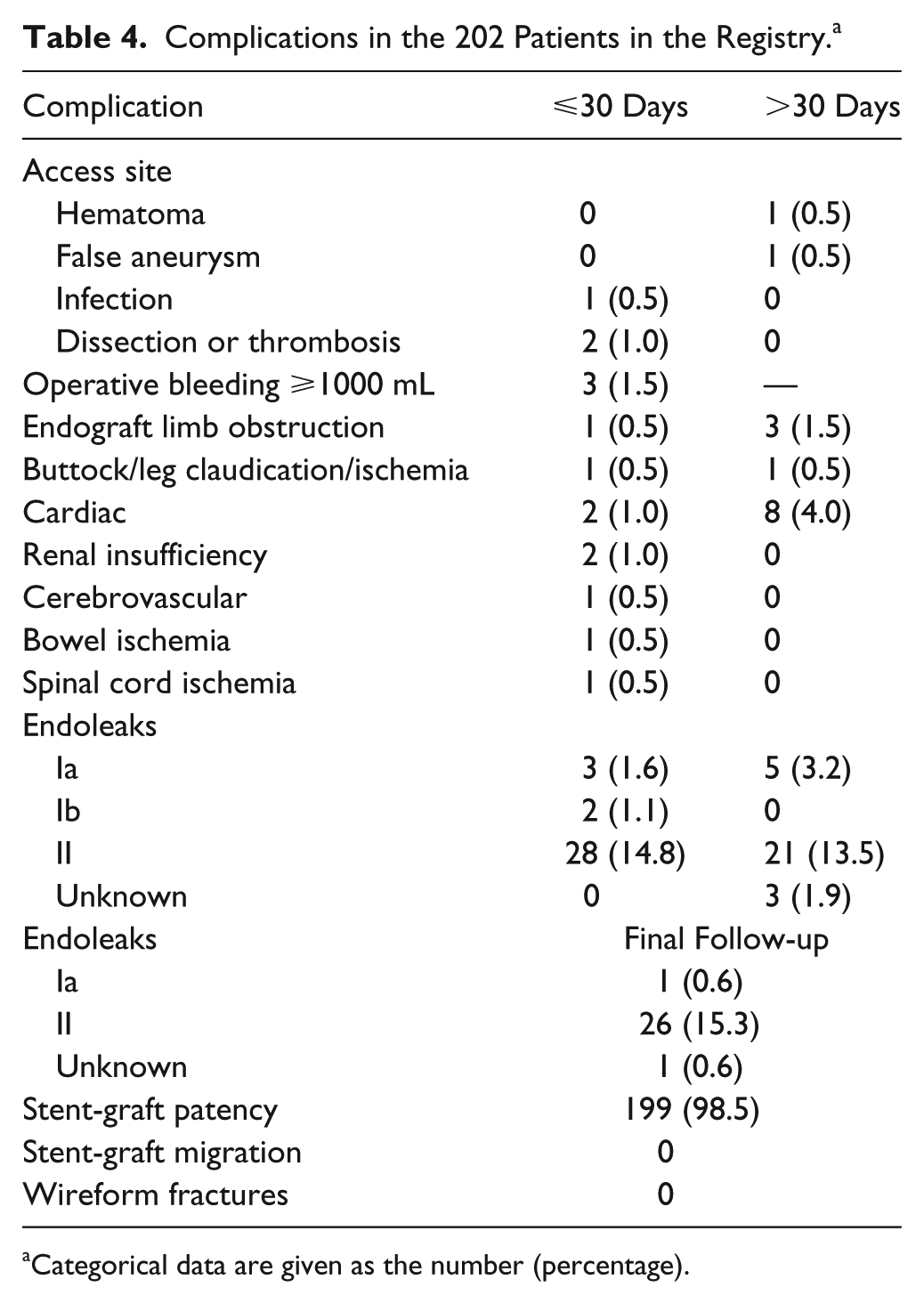
Categorical data are given as the number (percentage).
Clinical Success and Reintervention
Mean duration of follow-up was 13.7±3.1 months (median 12.8; IQR 4.7, 32.6). Clinical success at last follow-up was confirmed in 194 (96%) patients (Table 5): 187 (92.6%) without reintervention (primary clinical success) and 7 (3.5%) with reintervention (6 assisted primary and 1 secondary). There were 8 (4%) clinical failures. Two of these had aneurysm expansion associated with type II endoleak. The other 24 (11.9%) patients with type II endoleak at final follow-up were counted as a clinical success because there was no aneurysm size increase. Among the 8 failures, 2 others had borderline (5 mm) aneurysm diameter increase.
One-Year Clinical Results in the 202 Patients in the Registry. a
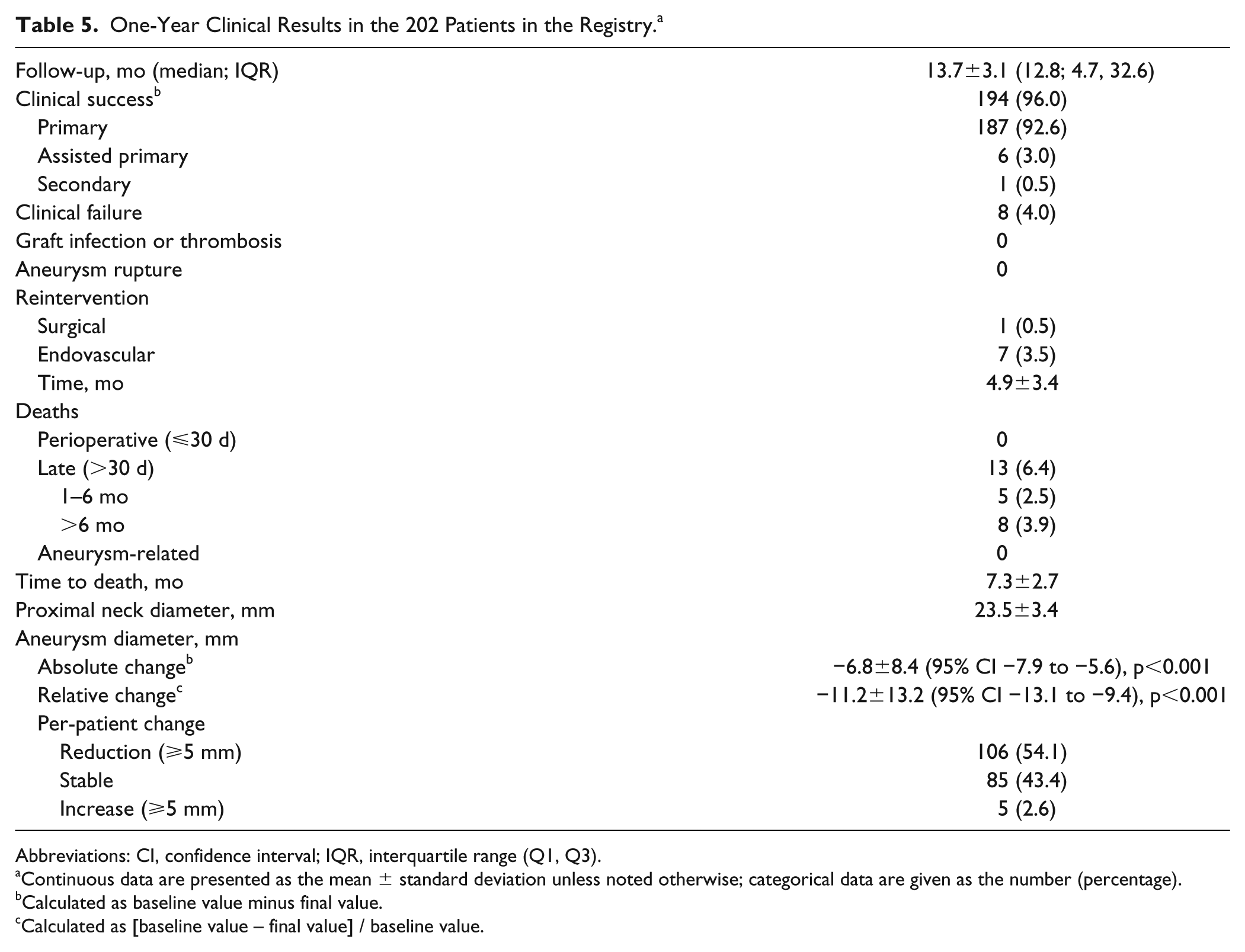
Abbreviations: CI, confidence interval; IQR, interquartile range (Q1, Q3).
Continuous data are presented as the mean ± standard deviation unless noted otherwise; categorical data are given as the number (percentage).
Calculated as baseline value minus final value.
Calculated as [baseline value – final value] / baseline value.
Thirteen (6.4%) patients died during the follow-up period (Table 5); no death was aneurysm-related. Six (3%) patients died after myocardial infarction; other causes were cancer (n=4), cardiac disorder (n=2), and amyotrophic lateral sclerosis (n=1).
There was 1 (0.5%) surgical reintervention (femorofemoral crossover bypass for right iliac limb occlusion) and 7 (3.5%) endovascular reinterventions: 2 Palmaz stents implanted, and individual cases of left limb extension, angioplasty, embolization, and cuff/endoanchor. Overall, the Kaplan-Meier estimate of freedom from reintervention was 95.6% (95% CI 91.4% to 97.8%) at 1 year (Figure 1).
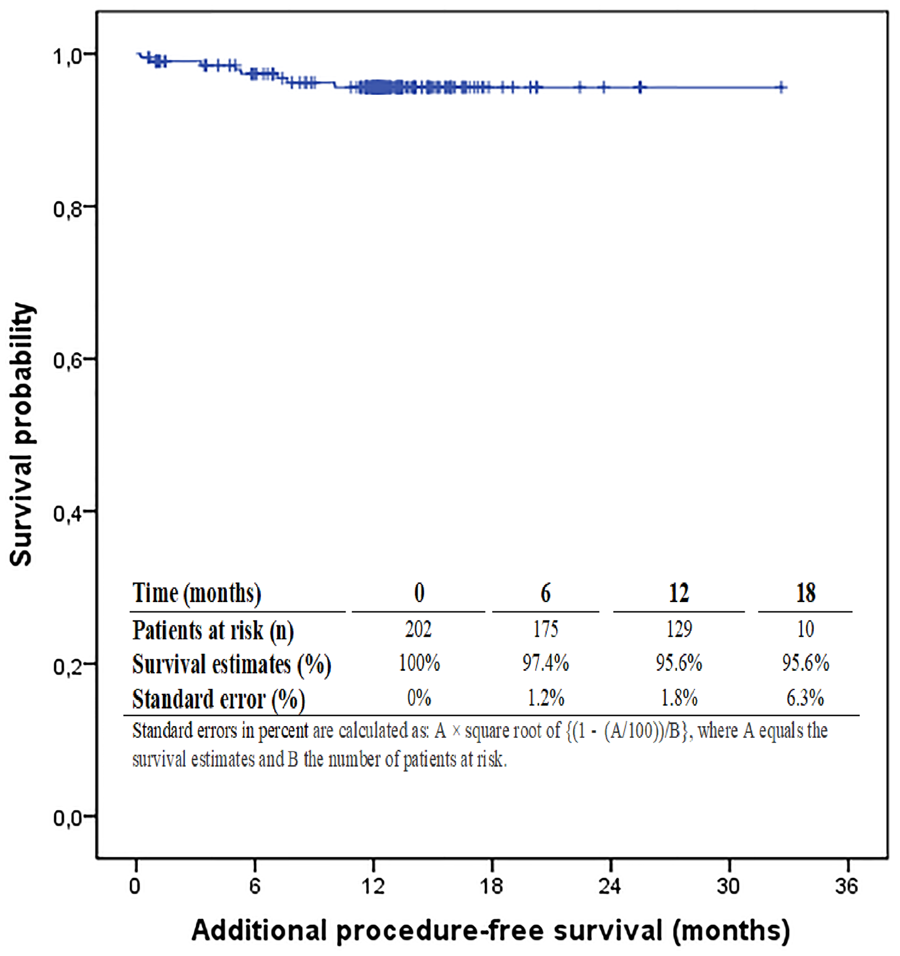
Reintervention-free survival.
Endoleak Analysis
At 1 month, there were 5 type I endoleaks (Table 4), 2 persistent from the index procedure (1 treated and resolved and 1 lost to follow-up) and 3 new leaks (1 resolved spontaneously, 1 was not treated and persisted, and 1 was lost to follow-up). At 6 months, 1 type I persistent endoleak was treated and resolved, 4 were secondary (1 was treated and resolved, 1 was untreated and persistent, 1 was lost to follow-up, and 1 resolved spontaneously). At final follow-up, a single type I endoleak persisting from the second follow-up was treated and resolved.
Overall, the Kaplan-Meier estimate of freedom from endoleak type I/III at 1 year was 95.5% (95% CI 91.7% to 97.5%). There were no type III endoleaks. The majority of endoleaks were type II (15.3% at 1 year). Of the 14 patients with perioperative type II endoleaks, 7 had resolved by the first follow-up, 2 by the second follow-up, 1 by the final follow-up, and 4 persisted at final follow-up. There were no secondary interventions for type II endoleak. Of the 26 patients with type II endoleaks at final follow-up, 20 were persistent and 6 were identified at that visit. Two type II endoleaks were associated with aneurysm diameter increase as noted previously.
Mean absolute change in aneurysm size was –6.8±8.4 mm (mean relative change −11.2%; p<0.001); 106 (54.1%) patients had at least a 5-mm reduction and 191 (97.4%) patients had a decreased or stable aneurysm sac size at last follow-up (Figure 2). The freedom from aneurysm expansion estimate was 97.4% (95% CI 94.2% to 98.9%) at 1 year. No changes were appreciated in the diameter of the proximal neck: mean diameter was 23.6±3.0 mm at baseline and 23.5±3.4 mm at 1 year.
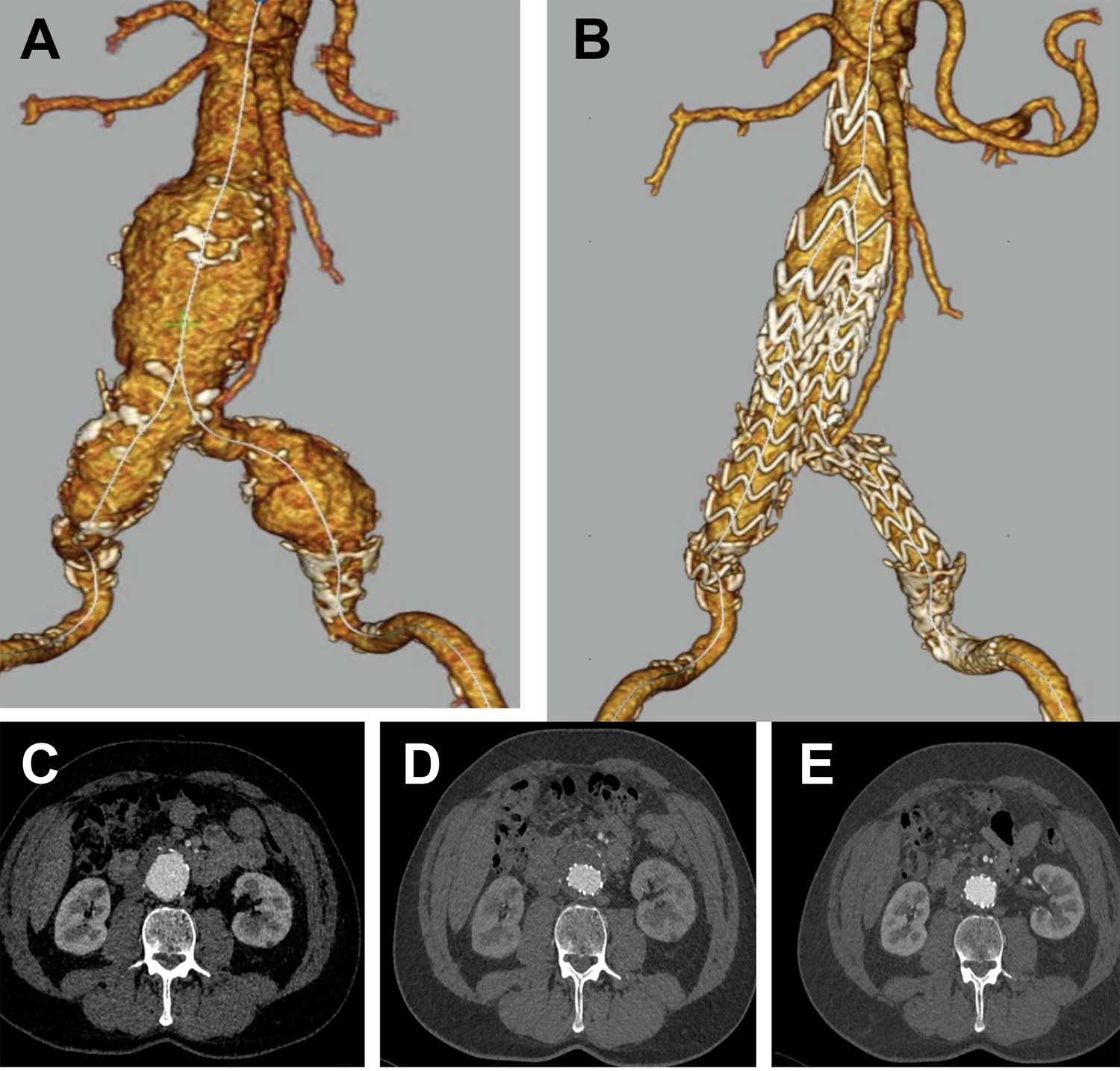
Computed tomography (CT) angiography reconstruction (A) before and (B) after endovascular repair. Axial CT scan images show the aneurysm at (C) baseline, (D) shortly after implantation without any endoleak, and (E) at 1-year follow-up with aneurysm sac shrinkage.
Discussion
Early clinical studies with the Treovance abdominal stent-graft system in AAA patients (including hostile anatomies) demonstrated feasibility and safety.21–24 However, these investigations involved relatively small cohorts. The more robust RATIONALE registry results show favorable 1-year safety and clinical performance of the Treovance stent-graft in a real-world setting, with 54% of patients having a ⩾5-mm reduction in aneurysm sac size at 1 year compared with 32% in OVATION, 26 36% in GREAT, 27 and 41.3% in ENGAGE. 13 There was no migration, in line with 1-year results from the other registries.26,27
There were no aneurysm-related deaths and all-cause mortality was 6.4% at 1 year. Three patients with intraoperative type I endoleak resolved by the first CT follow-up had device oversizing >20%, suggesting that the stent had not fully expanded intraoperatively, causing gutters that remained until full expansion and apposition in the following 72 hours. Early type Ia endoleak due to incorrect estimation of the required diameter has been reported and supports a selective, conservative strategy.28,29
The 4% reintervention rate in the RATIONALE registry is comparable to the 4.6% rate in the 500-patient subcohort of the ENGAGE registry (the authors considered their rate low compared with results of the DREAM, OVER, and EVAR-1 studies). 13 In the Excluder GREAT registry, 27 the reintervention rate was 7.0% in the 400 patients followed for 1 year. The reintervention rate was 14.5% in a large (n=1736) retrospective EVAR review of procedures performed in 17 institutions in the United States between 2000 and 2010 using a variety of earlier generation devices. 30 With newer generation devices, type III endoleaks are infrequent (2.1%) but not yet eliminated. 31 In RATIONALE, the majority of endoleaks were type II (15.3% at 1 year compared with 9.9% in ENGAGE 13 ); there were no type III endoleaks at any time.
The RATIONALE registry enrolled 17 (8.4%) patients with proximal neck length <15 mm compared with 4.1% reported in ENGAGE. 13 A quarter of patients did not receive devices sized according to recommendations, which suggests that optimal device sizing is still an issue. 29 The 8 available Treovance sizes (20–36 mm) should be considered as part of careful case planning. A possible link between device sizing >20% and early type I endoleaks that resolve spontaneously by discharge needs to be explored further.
As expected of a device with low-profile delivery (18-F to 19-F), one-third of patients implanted with Treovance had percutaneous access, which is associated with a high success rate, shorter operation time, shorter length of stay, and fewer wound complications compared with cutdown.32–34 This compares with 17.5% in the GREAT registry using the C3 Gore Excluder. 27
Limitations
Follow-up was only 1 year in this registry; it is generally accepted that EVAR requires longer-term data to evaluate if the benefit of EVAR (over open surgical repair) is lost over time, as some studies assert. 35 However, the 1-year results are in line with those of the ENGAGE registry, suggesting that similarly good longer-term results might also be expected based on important indicators, such as sac size reduction and rate of secondary intervention.
There was no centralized core laboratory evaluating interobserver and intraobserver variability in aneurysm measurements. Differences in standard clinical practice with regard to case planning, surveillance, and imaging were also clear in the registry. Some sites performed CT imaging prior to discharge and there was no 30-day visit; other sites had no 6-month visit. This also affected the already challenging issue of aneurysm sac size measurement; standard reporting recommendations advise that the first postoperative CT scan should be baseline for subsequent comparison, 25 but this is impracticable unless it occurs prior to discharge. All endpoints, including death, were investigator-reported and there was no monitoring board or adjudication committee.
Given the challenge to improve indefinite surveillance of all EVAR patients to ensure long-term follow-up, standardizing follow-up protocols remains an area for improvement. Finally, this registry made a concerted effort to meet standard reporting criteria and thus improve both the quality of results and the usefulness in everyday clinical practice. More needs to be done to standardize collection and reporting of key endpoints and improve longer term standard surveillance of EVAR patients.
Conclusion
This prospective observational study shows favorable safety and 1-year outcomes of the Treovance stent-graft for the treatment of infrarenal AAAs in a real-world setting.
Footnotes
Appendix
The RATIONALE investigators: Marek Iłżecki, Samodzielny Publiczny Szpital Kliniczny Nr 1, Lublin, Poland. Hartmuth Görtz, Bonifatius Hospital, Lingen, Germany. Matthias Thenholt and Maher Fattoum, Theresienkrankenhaus und St. Hedwig-Klinik, Mannheim, Germany. Semih Buz, Deutsches Herzzentrum Berlin, Germany. Rosario Mancusi, Casa Di Cura Villa Dei Fiori, Acerra, Italy. Piergiorgio Cao, Azienda Ospedaliera San Camillo Forlanini, Rome, Italy. Domenico Benevento and Giancarlo Palasciano, Azienda Ospedaliera Universitaria Senese, Siena, Italy. Feras Abdallah, Manchester Royal Infirmary, Central Manchester University Hospitals, Manchester, UK. John Boyle, Addenbrooke’s Hospital, Cambridge University Hospitals, Cambridge, UK. S. Llagostera Pujol and Carlos Esteban, Hospital Germans Trias i Pujol, Badalona, Spain. Nilo Mosquera, Complexo Hospitalario Universitario de Ourense, Spain. Enrique Aracil Sanus, Hospital Universitario Ramón y Cajal, Madrid, Spain. Ignacio Iglesias Negreira, Hospital HM Modelo, A Coruña, Spain. J.T.F.J. Raymakers, ZiekenhuisGroep Twente, Almelo, the Netherlands. Joost van Herwaarden, University Medical Center Utrecht, the Netherlands. Georgios Pitoulias, “Georgios Gennimatas” Thessaloniki General Hospital, Thessaloniki, Greece. Theodoros Kratimenos, Evaggelismos General Hospital, Athens, Greece. Carl Magnus Wahlgren, Karolinska University Hospital, Solna, Sweden. Claes Forssell, Linköping University Hospital, Linköping, Sweden. Greg Fulton, Cork University Hospital, Cork, Ireland. Lars Lönn, Rigshospitalet, National Hospital and University of Copenhagen, Denmark. Gustav Pedersen, Haukeland University Hospital, Bergen, Norway. Jorge Vergara, Hospital Barros Luco Trudeau, Santiago, Chile. Manuel Espíndola Silva, Hospital de la Dirección de Previsión de Carabineros de Chile, Santiago, Chile. Stephen Wing-Keung Cheng, Queen Mary Hospital, University of Hong Kong, China. Phan Minh Anh, Cho Ray Hospital, Ho Chi Minh, Vietnam. Carlos David Calderas, Instituto Urológico San Román, Caracas, Venezuela. Patrick Bohan, Terumo Aortic, Sunrise, FL, USA.
Authors’ Note
This study was presented at LINC (January 30, 2018; Leipzig, Germany).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Raman Uberoi, Carlo Setacci, Mario Lescan, Antonio Lorido, David Murray, Zoltán Szeberin, Tomasz Zubilewicz, Vincent Riambau, Angsu Chartrungsan, and Jörg Tessarek report receiving research grants from Terumo Aortic (formerly Bolton Medical) for the conduct of this study. Carlo Setacci, Mario Lescan, Vincent Riambau, Angsu Chartrungsan, and Jörg Tessarek report receiving proctoring/personal fees from Terumo Aortic (formerly Bolton Medical) outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from Terumo Aortic (formerly Bolton Medical).