
Abstract
This Short Take describes the rationale for, and use of, a decision-making process in community-engaged comparative effectiveness research, co-led by community researchers and academic researchers. The contribution of this methodological guide is to (1) ensure that all partners have a voice in contributing to major study decisions; (2) distribute power equally; (3) avoid power differentials; (4) increase trust; and (5) promote shared governance in research.
Introduction
Community-engaged research aims to improve trust, promote respect, and address community priorities and preferences (National Institutes of Health 2011). When building community-engaged research teams, it is important that every member’s expertise is valued regardless of traditional power differentials (Pellicano et al. 2014; Wallerstein et al. 2019). Developing methods congruent with shared governance principles while aligning actions with community research priorities is central to successful teams (Oetzel et al. 2015). Our team faced the specific need to reduce power differentials, promote voices of minority perspectives, and develop practices that value strengths and preferences of community partners who identify as neurodivergent.
Majority-rule decisions are the norm within many societies and are commonly adopted in research teams. Some evidence suggests majority rule is not negatively associated with team performance (Schippers and Rus 2021) and may result in better decisions (Kuroda et al. 2023). However, marginalized communities do not make up the majority and even if they raise significant concerns about harms, a majority vote could proceed. There is some evidence that societies that prefer majority rule lean more toward consensus decisions when a substantial minority group is present (Bor et al. 2021).
Consensus-based decisions are another method of decision making where a group discusses all perspectives and comes to an agreement, usually requiring a certain agreement level (e.g., 70–100%) (Newman et al. 2011). Consensus-based decisions have been described by community-based participatory research teams to ensure shared decision making, although consistency and specific use of consensus methods are not well known (e.g., Cary et al. 2023). Barriers include requiring strong verbal skills and sufficient time and ability to bring all members together concurrently to address concerns in a group (Newman et al. 2011).
For neurodivergent team members with different communication preferences, a prolonged defense of a viewpoint that is contrary to the larger group may increase feelings of isolation, particularly under stress. Modifications to consensus decisions are needed to ensure that minority viewpoints are respected. Another approach used in supporting decision making of historically marginalized communities includes “enclave deliberation,” in which a group with an affiliated identity deliberates outside of the majority group (e.g., Abdullah et al. 2016). This reinforces the importance of creating a supportive environment for neurodivergent community research partners to deliberate, thus reducing power differentials. Therefore, our team modified and operationalized a decision-making process (Nicolaidis et al. 2011) that did not rely on extensive verbal discussion and allowed individuals to express and address their concerns and feel valued. This adapted consensus decision-making approach validates member concern by allowing a veto option. We describe this as the AASET Decision-Making Process. The research team included one neurodivergent and three neurotypical study leaders, three study staff identifying as neurodivergent, and a 13-member community council of autistic, neurodivergent, and/or caregivers of autistic individuals.
Practical Steps for Decision Making within Participatory Action Research
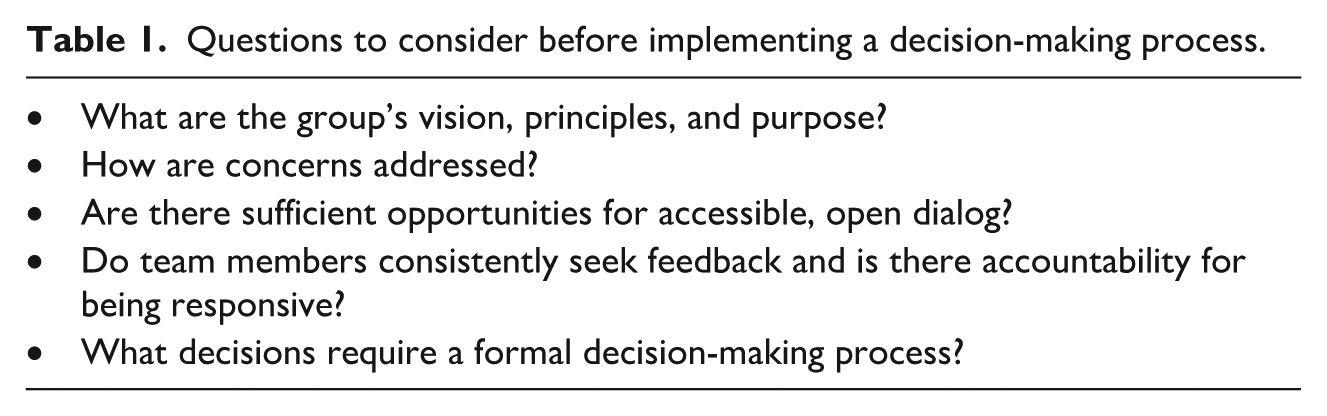
The AASET Decision-Making Process was informed by our team’s shared principles, preferred forms of communication (e.g., emails, use of nonspoken communication), and Engagement and Compensation Guidelines (Shore and Benevides, 2018). The process assumes that teams interested in adopting this process already have mechanisms in place for building trust and respectful consideration of perspectives. Teams must adequately prepare to engage in a meaningful decision-making process (see Table 1 for guiding discussion questions).
Questions to consider before implementing a decision-making process.
The research team described above used the AASET Decision-Making Process to make major study decisions. We defined major decisions as those impacting participants in the study, including drafting and approving patient-facing consent forms, recruitment documents, and questionnaires. Decisions that did not directly impact participant recruitment or engagement, such as decisions about data management, were not subject to this process. The AASET Decision-Making Process involves three steps, each with specific goals and methods (Figure 1).
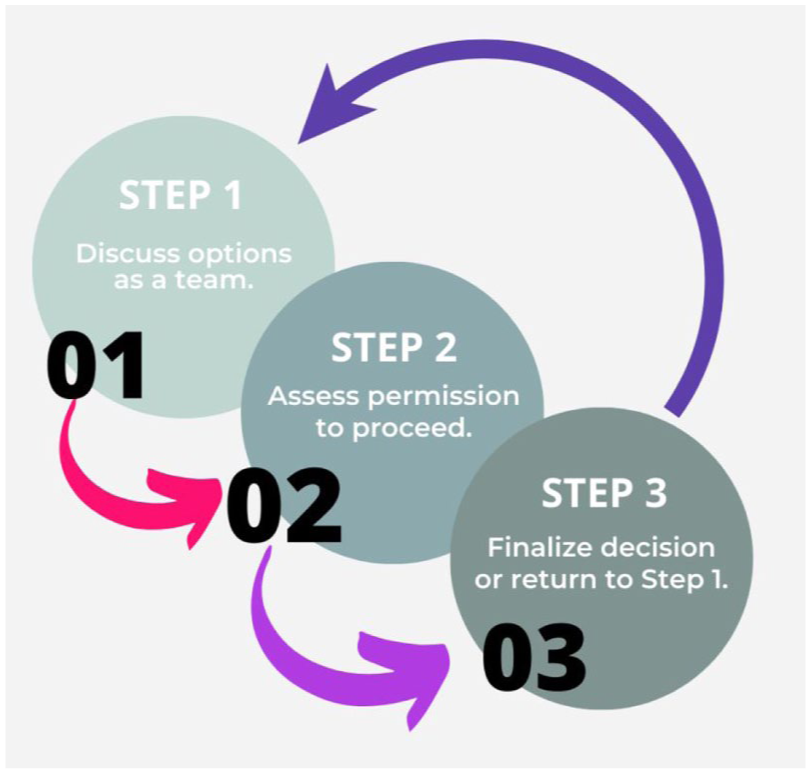
AASET Decision-making Process Steps.
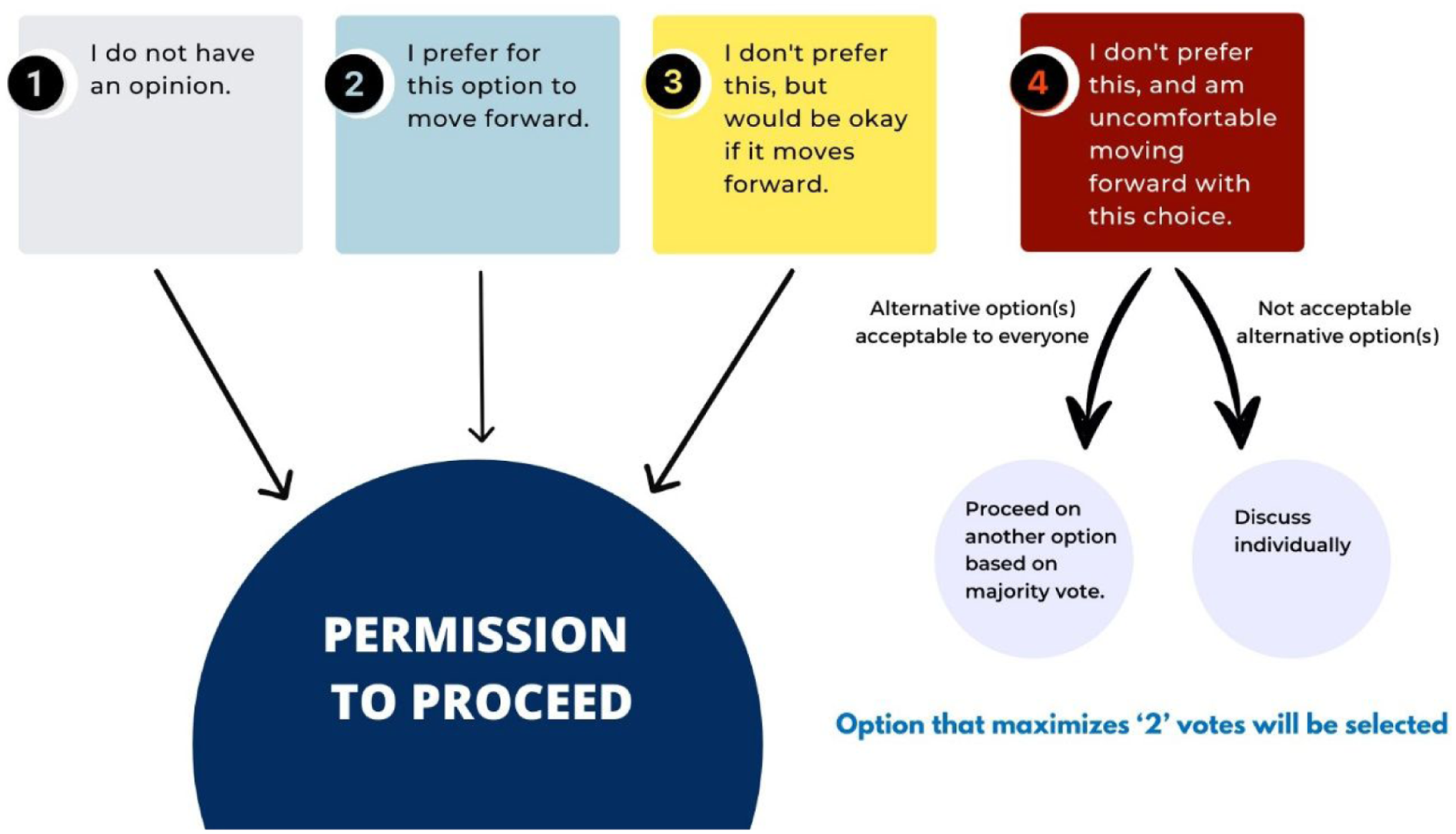
Selecting a final decision in Step 3.
If the majority choice contained a #4 vote, the team chose the next best option without a #4 vote (if there were any), or the person voting a #4 was contacted privately to share more about their concerns with that option. The choice of a private conversation by email or Zoom was recommended by the team to promote feeling safe expressing a view that may not be in the majority and aimed to increase trust in the process. Our team also emphasized that the conversation should not center around changing the person’s mind, but rather clarifying concerns and identifying potential solutions. For example, a person may vote #4 based on something that could easily be resolved (e.g., a wording change) or required further discussion (e.g., a concern with the implications for patient participants).
If the discussion concluded with a resolution that did not dramatically alter the process or product, the change was made, and the vote was finalized. If the #4 vote discussion resulted in more substantial modifications, the change was made aligned with community partner recommendations. The process or product was then sent back for a vote with a description of the change. If the vote resulted in no viable options (e.g., #4 vote), the team could either discuss viable options that were not previously identified or table the decision until more information or options were available.
Communicating the Decision
It is essential to share the results of the vote with the team contributing to the decision at the end of Step 3. We described the results of the vote via email, during a virtual meeting, and/or a video. We evaluated partner perceptions of decision-making processes through anonymized surveys. There have been no concerns expressed with this process in the three years of use.
Illustrative Example of a Vote to Modify a Questionnaire
One of the major decisions in our suicide prevention study was to ensure questionnaires were accessible and clear to participants. Step 1 sought open-ended input on the Suicide-Related Coping Scale (SRCS; Stanley et al. 2017) from the community council. Members had the opportunity to provide feedback via Zoom meetings with breakout rooms and/or a one-on-one meeting with engagement leaders and study staff notetakers. We solicited feedback on the items, response options, and structure.
Following Step 1, the study leadership reviewed and organized the feedback into discussion themes, specific comments, and potential revisions. Revisions were shared back with the community council and documented in both a written document and a video illustrating specific anonymized feedback and the resulting changes. We relied on Universal Design (Dong et al. 2023; Nelson 2014) to communicate changes.
Step 2 of the decision-making process involved seeking a formal vote on the revised version. We requested a vote from the community council via an online form on the revised SRCS: (1) instructions; (2) response scale; and (3) each item. Of the 19 items, three had at least one #4 vote; these votes resulted in a second round of discussion with those voting #4. Concerns raised included word choice that impacted clarity and the wording of response options. One-on-one Zoom meetings were held to discuss concerns and recommendations to address them. These recommendations were brought back to the study leadership team for discussion, and modifications were made aligned with community partner feedback. Another round of votes was held and the revised SRCS was approved. The approved version was submitted to the Institutional Review Board.
Conclusion
The use of a decision-making process that is inclusive of non-majority perspectives is necessary for participatory action research. The AASET Decision-Making Process combines a consensus approach with the ability for minority perspectives to prevent an option from proceeding until all major concerns are addressed, thus leveling power differentials. This approach has been successful in ensuring community research partners feel their perspectives are heard and respected, building trust and ensuring co-ownership of the research process. It also contributes to shared learning, as reasons for concern with different choices during a decision are not always clear until people are asked to vote. Future areas for inquiry include assessing adoption and impact in other teams, evaluating perceptions of this process by other team members (e.g., study principal investigators), and developing guidance about how to support members when major concerns are raised. This process opens the door for more productive communication and ensures that research is more equitable in its reach.
Footnotes
Acknowledgements
We acknowledge our Community Council members who have participated in the implementation of this process and provided guidance on how to best support our team in making decisions collaboratively.
Author’s Note
The statements and views presented in this article are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors, or Methodology Committee.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research described in this article was funded by the Patient-Centered Outcomes Research Institute award (PCORI; SP-2020C3-20951).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.