
Abstract
Neuromyelitis optica spectrum disorder (NMOSD) is an acquired neurological disorder primarily affecting physical and visual functioning. There is a lack of empirical evidence in the existing literature about the nature of speech, language, and cognitive deficits associated with NMOSD. Hence, this case study provides assessment information about a 32-year-old female diagnosed with NMOSD who was administered the following formalized tests via teleconference: the Apraxia Battery for Adults–2nd edition, Cognitive Linguistic Quick Test, and Western Aphasia Battery-Revised. The participant, classified as having anomic aphasia, demonstrated good auditory and reading comprehension, writing difficulties, apraxia of speech, and mild difficulties with cognitive tasks requiring writing.
Keywords
Speech-language pathologists often work with persons who have communicative-cognitive deficits resulting from rare diagnoses. Neuromyelitis optica spectrum disorder (NMOSD), sometimes referred to as Neuromyelitis Optica (NMO), is one such diagnosis. It is a rare relapsing inflammatory demyelinating autoimmune disease that affects the central nervous system (CNS), resulting in severe physical and/or visual disability (Eaneff et al., 2017; Pfeuffer et al., 2017). Approximately 4,000–8,000 people live with NMOSD in the United States (U.S. Food and Drug Administration, 2019) with the average age of diagnosis at 37.8 years (Pfeuffer et al., 2017). The cause is unknown, but it may result from an infection or other autoimmune disease (Papp et al., 2021). White individuals have the lowest prevalence and incidence of NMOSD; persons of African ethnicity demonstrate the highest prevalence and incidence of NMOSD (Papp et al., 2021).
Previously, NMOSD was thought to be a form of multiple sclerosis (MS) and some people with the disorder have brain lesions; however, NMOSD has been determined to be a distinct pathology (Blanc et al., 2008). A serum autoantibody, referred to as NMOSD antibody, binds specifically to aquaporin 4, the dominant CNS water channel protein found in the brain that is predominantly located within the optic nerve and spinal cord; approximately 70% of persons with NMOSD have the NMOSD antibody (Blanc et al., 2008; Lennon et al., 2004; Venero et al., 1999). Identification of this biomarker (Wingerchuk et al., 2015) along with the severity of optic neuritis or transverse myelitis can ideally lead to NMOSD being quickly and accurately diagnosed (Eaneff et al., 2017). Persons with NMOSD typically present with fatigue, pain, stiffness, anxiety, depression, bowel and bladder problems, and excessive daytime sleepiness (Eaneff et al., 2017). In one study, 45% of adults with NMOSD self-reported burning sensations/pain as their major complaint, whereas 35% reported vision impairment as the primary disability (Eaneff et al., 2017). Walkers, wheelchairs, and other devices can aid mobility in persons with NMOSD (Eaneff et al., 2017).
Adults with NMOSD have also self-reported speech, language, and cognitive difficulties, although the accounts tend to be rather generic and nonspecific. For example, Takahashi and colleagues (2017) reported on a 63-year-old man with spinocerebellar ataxia type 31 who developed NMOSD 14 years after the onset of cerebellar signs. Sudden new symptoms included: paraplegia, bowel and bladder difficulties, weakness, incoordination, saccadic eye movements, and slurred speech. The researchers believed the co-occurring diagnoses were unrelated, but they speculated that underlying inflammation could be a plausible unifying factor. As another example, Blanc and colleagues (2008) administered a neuropsychological test battery to 30 people with NMOSD. Nine (30%) had impaired long-term memory, one (~3%) had impaired short-term memory, six (20%) had slowed processing speed, eight (~27%) had executive dysfunction, and four (~13%) had language impairments.
Given the sparsity of information about communicative and cognitive effects of the disorder, the purpose of this case example was to describe the performance of a young adult with NMOSD on standardized speech, language, and cognitive measures administered via teleconferencing. Measures include the Apraxia Battery for Adults–Second Edition (ABA-2; Dabul, 2000), the Cognitive Linguistic Quick Test (CLQT; Helm-Estabrooks, 2001), and the Western Aphasia Battery–Revised (WAB-R; Kertesz, 2007). All are tests that speech-language pathologists routinely administer to their adult clients. Information about performance on these types of measures will also allow speech-language pathologists to better identify adults who may have NMOSD and to provide appropriate speech therapy services to persons diagnosed with this disorder.
Case Example
Participant
This case study was reviewed by the University of Northern Iowa’s Institutional Review Board, and participant consent was obtained prior to initiating the case review. The participant for this case description, H. H., was a 32-year-old female. She was diagnosed with relapsing-remitting MS in 2015 due to poor balance and vision impairments in which her depth perception and peripheral vision faded throughout the day. She fully recovered in 4 months. In June 2018, H. H. was planning to complete her last final exam in nursing school when she noticed right arm weakness and numbness while eating breakfast. She also tripped while attempting to inform her former spouse of what was happening. Within the first 24 hr, H. H. could talk but had slight word-finding difficulties. By 48 hr post-onset of the arm weakness and numbness, she had no speaking abilities and had progressed to right-sided hemiplegia and global aphasia. Her vision was also affected, and she was formally diagnosed with NMOSD. Doctors believe that she was misdiagnosed with MS in 2015, which could have instead been the start of NMOSD.
H. H. received speech, physical, and occupational inpatient and outpatient therapies September 2018–March 2019. During this time, an evaluation revealed apraxia of speech and Broca’s aphasia. Between March 2019 and the present, H. H. has received individual and group speech therapy almost continuously. Currently, H. H. resides with her significant other and receives individual speech-language therapy twice a week from a university clinic and aphasia group therapy once a week from a hospital, all via teleconference. Her most recent individual treatment goals have focused on typing correct medical abbreviations, typing medical terms with correct spelling, answering questions after reading a passage, and completing case studies related to the NCLEX (i.e., National Council Licensure Examination), a standardized test individual must pass in order to become a registered nurse or licensed practical nurse. She wears glasses, because she is near-sighted, but reports no other visual impairments. She receives Rituxan (i.e., rituximab) infusions every 6 months and takes Baclofen to combat her spasticity. H. H. does not work or drive, yet she no longer needs a cane and is independent in all her cares.
Tests Administered
H. H. completed the ABA-2 (Dabul, 2000), CLQT (Helm-Estabrooks, 2001), and WAB-R (Kertesz, 2007) via Zoom across three 2-hr sessions; one test was given per session. H. H. completed all tests while at home as she did not have transportation from her rural location to the clinic. No specific remote adaptations have been reported by the ABA-2’s test author or publisher, thus, the test was given as stated. A copy of the CLQT response booklet was sent ahead of time to H. H. to use during the assessment; CLQT administration followed remote test recommendations. The WAB-R was administered using the remote-adapted stimulus book. H. H. took pictures of writing tasks performed and emailed them to the research team to score.
Test Performance
Scores on the ABA-2 (Dabul, 2000), CLQT (Helm-Estabrooks, 2001), and WAB-R (Kertesz, 2007) are in Tables 1–3, respectively. H. H.’s test scores indicated varying severity of impairment levels typically falling in the mild range. She had particular difficulties on the ABA-2’s Increasing Word Length task with multisyllabic words. During this subtest, she frequently attempted a production, would stop, say “No,” and then re-attempt the target production; she displayed this pattern several times per target utterance. When describing the ABA-2’s action picture, H. H.’s productions tended to be telegraphic in nature (i.e., “People are at a c-carnival scene. Uh, highwire act and . . . um, women on her horse. Um, clown in entertaining some people while the line, lion tamer tames, tames a lion. Yeah.”).
Results for the Apraxia Battery for Adults–Second Edition (ABA-2).
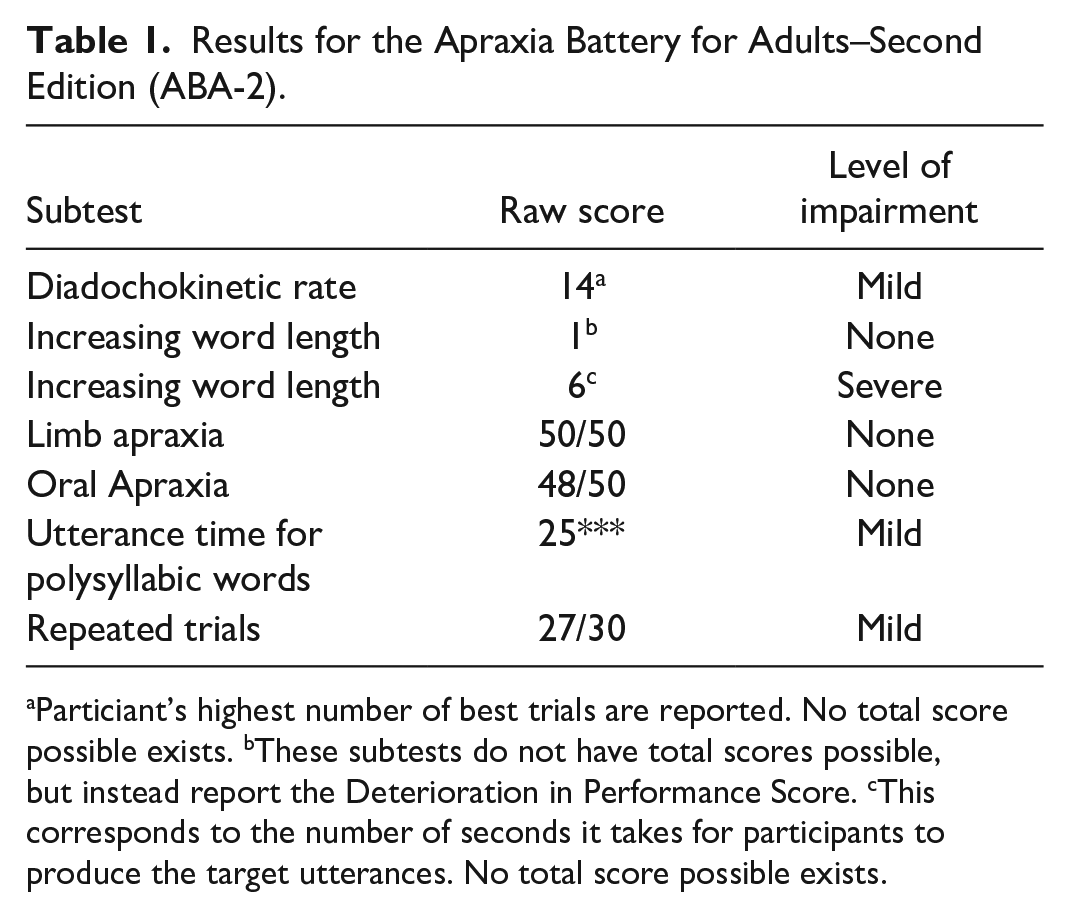
aParticiant’s highest number of best trials are reported. No total score possible exists. bThese subtests do not have total scores possible, but instead report the Deterioration in Performance Score. cThis corresponds to the number of seconds it takes for participants to produce the target utterances. No total score possible exists.
Results for Domains on the Cognitive Linguistic Quick Test (CLQT).
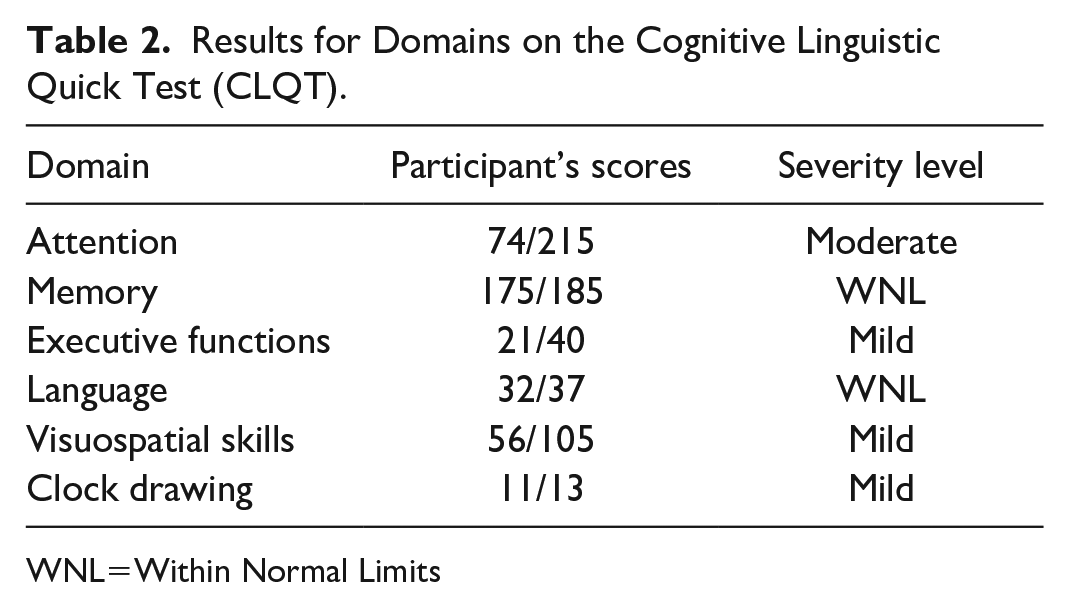
WNL=Within Normal Limits
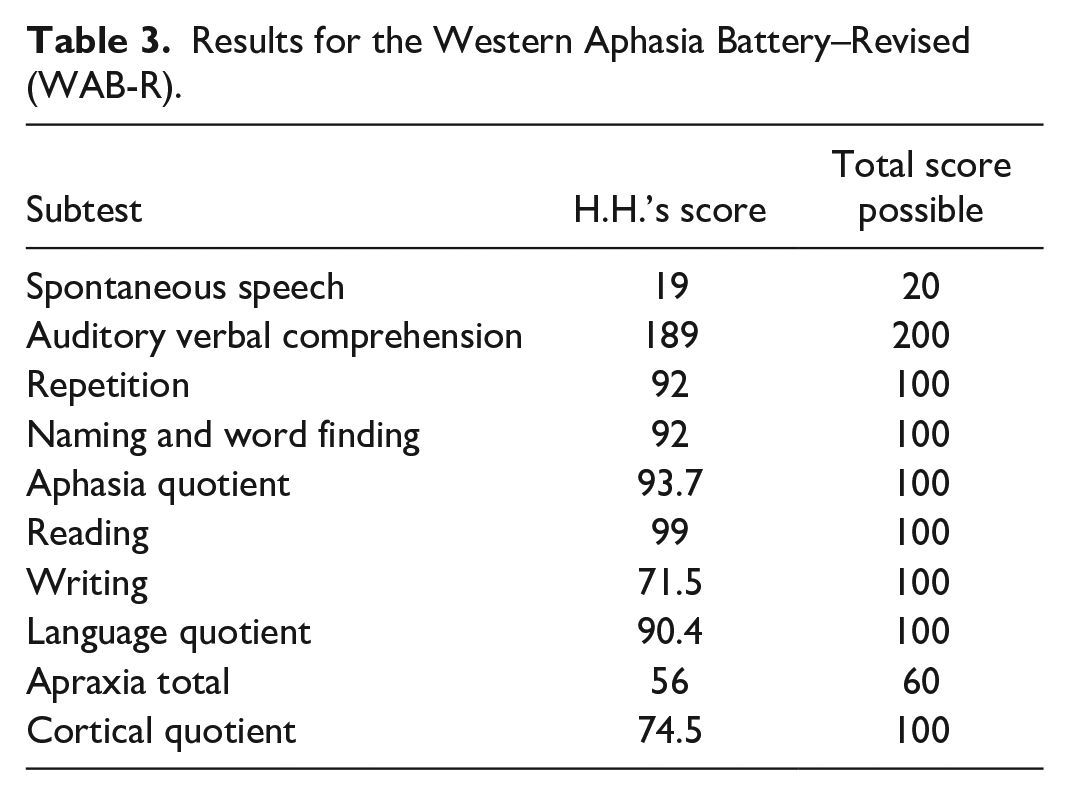
Results for the Western Aphasia Battery–Revised (WAB-R).
On the CLQT, H. H. had the lowest scores on the Symbol Trails and Mazes subtests, earned full points in the Personal Facts subtest, and on the remaining subtests, earned only one point less than the total points possible. Her short story recall included correct content with some repetitive verbalizations noted (i.e., “Anna . . . was . . . given a r-ruby ring for her birthday? And . . . she someh-someh-somehow lost it. But she pulled up, she pulled out her handkerchief, her handkerchief, and there it was.”). Many deficits she evidenced on the CLQT can be explained by difficulty writing due to her right-sided hemiplegia, leading her to write with her non-dominant left hand.
On the WAB-R, she had difficulties with the writing subtest due to motor impairments. During the Spontaneous Speech subtest, she produced grammatically correct utterances and evidenced self-correction abilities when describing the action picture (e.g., “The dog is chasing the boy,” “Somely, someone is fishing,” “A, no, a girl is making a san, sand castle,” “Um. The dad is reading a book and mom is having a glass of wine”). H. H.’s utterances on the WAB-R’s picture description were likely longer and more complete in nature versus her productions on the ABA-2’s picture description because she had been given the WAB-R in her previous inpatient and outpatient settings. Overall, H. H. displayed nonfluent, telegraphic speech with generally intact auditory and reading comprehension as is characteristic of anomic aphasia; her speech production was characterized by verbal apraxia. She had intact memory and language abilities as per the CLQT, yet moderate difficulties with certain cognitive tasks requiring writing were noted. Many of these difficulties were due to her hemiparesis and needing to use her non-dominant left hand, such as difficulty placing numbers in the appropriate place on the Clock Drawing. She did well on the simpler Symbol Trails and Maze; however, she had difficulties correctly delineating appropriate paths for the more complex Symbol Trails and Maze.
H. H. provided self-reports in terms of how her speech, language, and cognition had been affected by her diagnosis. At the onset of NMOSD, she could only say single words and had extreme difficulty writing. Her attention levels were significantly decreased, in part, due to the heavy doses of medications she was given. However, H. H. reported that 6 months after her diagnosis, she believed her attention returned to normal. She did not provide the research team any test results to support this statement. She also stated how 3.5 years of therapy had assisted in improving her speech and language. Specifically, she could now carry on a conversation and her handwriting was greatly improved from her initial post-onset ability.
Discussion
NMOSD is a rare disease that affects the CNS and is typically characterized by physical and/or visual disabilities (Eaneff et al., 2017; Pfeuffer et al., 2017). Takahashi et al. (2017) briefly reported on an adult with a recent onset of NMOSD who developed slurred speech. Eaneff et al.’s (2017) study included self-reports of persons with NMOSD having speech and cognitive challenges, and Blanc et al. (2008) found that up to one third of their participants had some kind of cognitive impairment. Few other researchers have documented speech, language, and cognitive characteristics of people with NMOSD.
As noted, H.H. had relatively intact auditory and reading comprehension with nonfluent, telegraphic, apraxic speech. She was classified as having anomic aphasia according to her recent performance on the WAB-R. Notably, her classification of aphasia had changed since 2018. H. H. was initially classified as having global aphasia when her symptoms were at their worst. During inpatient and outpatient therapies H. H. received between 2018 and 2019, testing indicated she had Broca’s aphasia. Thus, it is possible to see changes in aphasia classifications over time and in response to therapy, although H. H.’s trajectory of improvement may or may not be the case for others who have NMOSD. The possibility of changing abilities indicates the need for ongoing assessment in any persons with aphasia, not just those who have more typical etiologies (e.g., strokes, traumatic brain injuries) (Murray & Coppens, 2017; Pashek & Holland, 1988; Potagas et al., 2017).
H. H. evidenced some deficits on the CLQT, yet most of these could be explained by her need to write with her non-dominant left hand. Her CLQT Memory and Language Domain scores were WNL. H. H. accurately named all pictures in the Confrontational Naming subtest and earned almost the full points on the Generative Naming and Story Retell subtests. Blanc et al. (2008) reported 9/30 (30%) of persons with NMOSD had long-term memory deficits, one had short-term memory deficits, and 4/30 had language impairments on a neuropsychological battery. Thus, it is apparent persons with NMOSD can have differing speech-language and communicative-cognitive presentations. This information adds to the limited literature base in the hopes that clinicians who may have patients with NMOSD find this case description useful.
Limitations for this clinical tutorial must be considered. This is a case description, thus, only one participant is described. All testing was done via teleconference with remote recommendations followed when provided by tests’ publishers, but it is possible H. H. would have had different test results had these tests been given in person. Accordingly, recommendations for future research should include completing these assessments on more persons with NMOSD and administering such formalized tests in person.
Footnotes
Acknowledgements
The authors would like to thank H.H. for participating in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.