
Abstract
Tobacco use remains a leading cause of preventable death in the United States, and smoking is disproportionately concentrated among individuals who have experienced trauma. Trauma-informed care offers a framework for addressing tobacco use in this population, yet few training programs provide guidance on integrating trauma-informed principles into cessation treatment. To address this, our team added a tobacco treatment module to the Trauma, Addictions, Mental Health, and Recovery (TAMAR) training for behavioral health providers in two California counties. We conducted semi-structured qualitative interviews with seven community-based providers who completed the training and analyzed them using inductive thematic analysis. Participants described the module as relevant and actionable. Participants reported changes in practice after the training, including adding tobacco questions to intake workflows, incorporating mindfulness strategies to help clients manage cravings, and integrating cessation goals into treatment planning. Participants viewed trauma-informed cessation care as requiring empathy, cultural humility, nonjudgment, and an understanding of the role of trauma in tobacco use. Barriers included limited time, staffing constraints, insufficient cessation training, rigid workflows, and a lack of physical space to deliver the training. Facilitators included organizational support, leadership buy-in, and access to professional development in providing cessation care. Participants emphasized that one-time trainings are insufficient to sustain trauma-informed tobacco treatment. Effective implementation requires organizational infrastructure, repeated reinforcement of skills, and materials that support real-time application. Findings highlight the need to align trauma-informed cessation curricula with the realities of diverse community settings and to expand training opportunities for professionals serving populations experiencing trauma.
Keywords
Tobacco use is the leading preventable cause of death in the United States (U.S. Department of Health and Human Services, 2024). Individuals with Adverse Childhood Experiences (ACEs) and those who experience trauma bear disproportionate tobacco-related harm (Abufarsakh et al., 2024). Among these populations, an estimated 27% of people with posttraumatic stress disorder (PTSD) smoke cigarettes compared with 9.9% of the general population (Agaku, 2026), and people with multiple ACEs report heavier tobacco use (Abufarsakh et al., 2024).
Trauma-informed care provides a framework for recognizing and responding to the impact of trauma in health care delivery (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014). However, few programs offer guidance on applying these principles to tobacco cessation treatment. To address this, we integrated tobacco treatment into the Trauma, Addictions, Mental Health, and Recovery (TAMAR) program (National Association of State Mental Health Program Directors [NASMHPD], 2023). TAMAR is a nationally recognized, trauma-specific group intervention that trains providers working with clients who have experienced trauma across justice, behavioral health, and community settings (NASMHPD, 2023). The TAMAR manual for providers comprises a 16-module psychoeducational curriculum that combines education about trauma’s impact with examples of self-regulation techniques, including mindfulness and creative expression, that can be used with clients (NASMHPD, 2023). In 2023, we added a tobacco treatment module to the TAMAR manual that covers the relationship between trauma and tobacco use, misconceptions about cessation, and practical cessation guidance, including the 5As (Ask, Advise, Assess, Assist, Arrange) and pharmacotherapy (NASMHPD, 2023). The tobacco treatment module is included in the standard TAMAR curriculum used nationally across health care and correctional settings.
In 2023 and 2024, we trained 82 public health professionals in two California counties. We invited the 64 individuals who completed the post-TAMAR evaluation survey to participate in qualitative interviews. Seven individuals representing program coordinators, tobacco treatment specialists, public health administrators, and research staff working with clients who had experienced trauma agreed to participate. In this Practice Note, we describe applications and lessons learned from the TAMAR tobacco treatment module, as experienced by the seven participants. Our objective was to understand participants’ perspectives on essential components of trauma-informed cessation care to inform curricula and best practices for tobacco treatment. The study was considered exempt by the University of California, San Francisco Institutional Review Board (IRB#-23-40523). We conducted semi-structured qualitative interviews lasting approximately 45 minutes (August–October 2024, 9–12 months after the training). Interviews were audio-recorded and transcribed verbatim by a professional transcription service. The study team coded transcripts in Excel and Atlas.ti.v.24 using inductive thematic analysis, iteratively developing codes and organizing them into themes. The semi-structured interview guide is available as supplementary material. Participants received a US$50 gift card for their contribution. We present participant demographics and professional roles with quotes emblematic of themes in Table 1.
Key Themes, Subthemes, and Emblematic Quotes
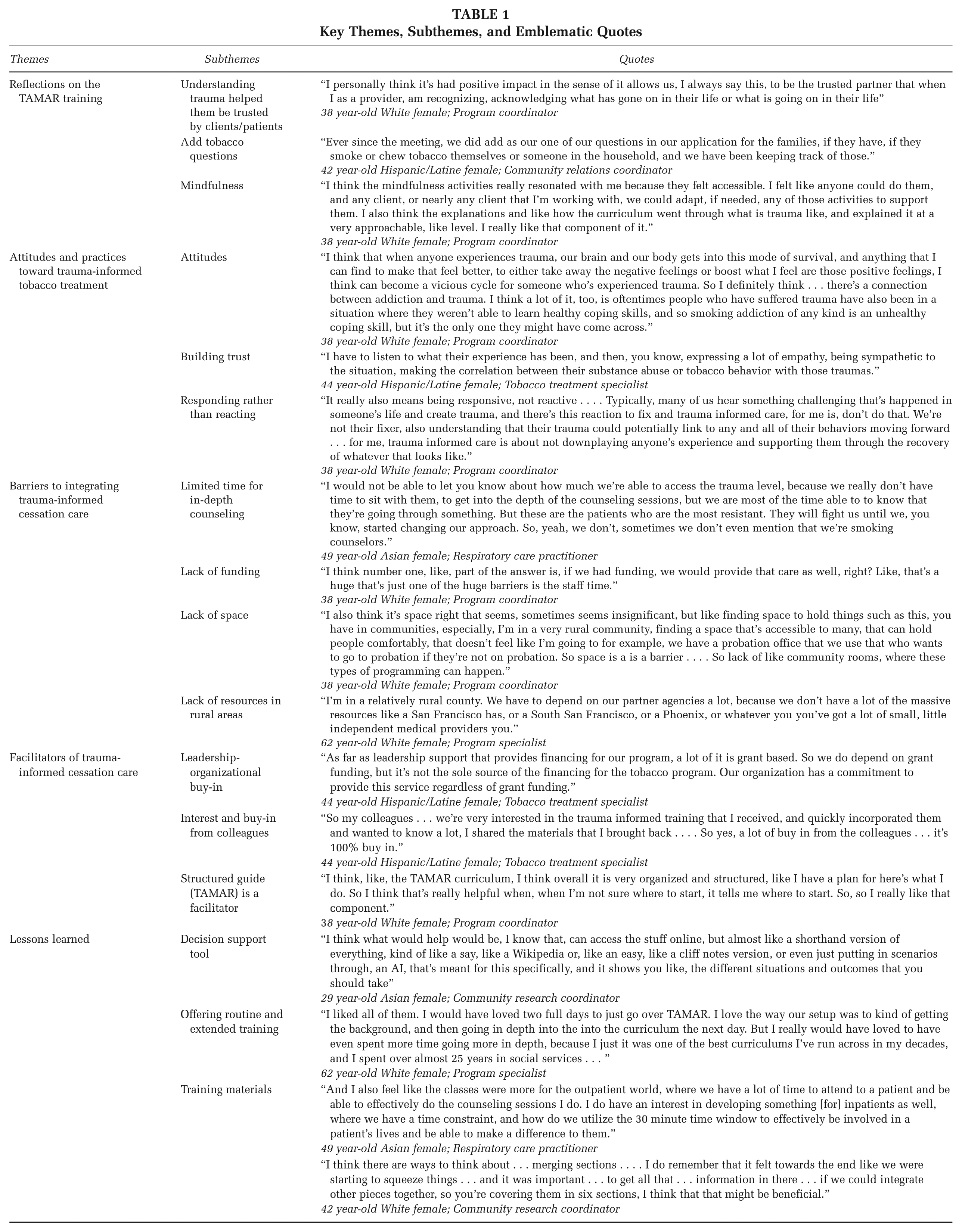
Reflections on the TAMAR Training
Participants described the tobacco module in the TAMAR training as relevant, engaging, and practical (Table 1). Several said it reinforced their understanding of trauma and introduced new ways to integrate tobacco-related content into client care. As a result of the training, participants added tobacco-related questions to intake forms, started using mindfulness exercises to help clients manage cravings, and integrated tobacco cessation as a client goal in treatment planning. Participants said TAMAR helped normalize conversations about trauma and tobacco use within professional teams and fostered shared understanding of the importance of professional development in trauma-informed care to support tobacco cessation.
Attitudes and Practices Toward Trauma-Informed Tobacco Treatment
Participants reported their clients used tobacco to regulate trauma-related distress, especially when lacking healthy coping skills (Table 1). They reported helping clients make the connection between tobacco use and stress, anxiety, and traumatic events. Participants viewed trauma-informed tobacco treatment as a process of building trust, being empathetic, listening, having cultural humility, and avoiding judgment. They talked about trauma-informed care as recognizing the role of trauma in tobacco use behaviors, using client-centered communication, and avoiding triggering language.
Barriers to Implementing Trauma-Informed Cessation Care
Some providers described limited time or staffing to provide cessation support beyond brief advice (Table 1). Others worked in clinical settings such as cancer care centers or inpatient hospitals and found it difficult to approach patients being treated for chronic illnesses until they had built rapport. Some spoke of the difficulty in providing cessation support when clients were not ready to quit and said they lacked training in tobacco cessation. Participants reported organizational workflows that lacked prompts or forms to assess tobacco use, making it harder to initiate conversations. Others reported fewer resources in rural communities compared with urban areas. Participants emphasized that infrastructure must align with the realities of their work settings, and a lack of mobile outreach, private space for conducting assessments, and limited physical spaces for holding classes and trainings were barriers to providing trauma-informed care.
Facilitators of Trauma-Informed Cessation Care
Organizational support and leadership buy-in facilitated the integration of trauma-informed cessation care (Table 1). In some settings, trauma-informed care was already part of the organizational culture, which made it easier to apply these principles to tobacco use. Participants described how training and professional development, including the TAMAR training, gave them language and tools to feel more confident addressing trauma and tobacco use with their clients.
Lessons Learned
Participants emphasized the need for regular opportunities to reinforce trauma-informed practices (Table 1). While the TAMAR training provided valuable tools, several noted that a single training was not enough to sustain long-term changes in practice, highlighting the need for ongoing professional development in trauma-informed principles and cessation treatment. Materials need to align with learners’ practical needs, including quick-reference guides or visual tools to support application in community settings during real-time client interactions. Curricula must align with specific work settings, such as inpatient hospital units and community-based research roles.
Implications for Practice
Integrating trauma-informed principles into tobacco cessation treatment requires infrastructure and training approaches that align with diverse community and clinical settings. Ongoing training opportunities in trauma-informed cessation care for behavioral health and other health care professionals, including extended and recurrent training formats, could align cessation services with the needs of behavioral health populations.
Supplemental Material
sj-pdf-1-hpp-10.1177_15248399261449740 – Supplemental material for Implementing Trauma-Informed Training for Tobacco Use for Health Care Professionals in Two California Counties
Supplemental material, sj-pdf-1-hpp-10.1177_15248399261449740 for Implementing Trauma-Informed Training for Tobacco Use for Health Care Professionals in Two California Counties by Mark R. Hawes, Jessica Safier, Brian Clark, Maria Pamatmat, Catherine Bonniot, Christine Cheng, Raul Almazar, Joan Gillece and Maya Vijayaraghavan in Health Promotion Practice
Footnotes
Authors’ Note:
We would like to thank the study participants and the creators of the TAMAR training module for their support for this work. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The qualitative research project was supported by the Smoking Cessation Leadership Center.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.