
Abstract
With the rapidly aging Hispanic/Latino population in the United States and the traditional caregiving roles of women in this culture, it is critical to study caregiving stress in the largest yet understudied subgroup—women caregivers of Mexican origin. This descriptive feasibility study aimed to adapt a research protocol to examine the impact of long-term caregiving stress on coronary heart disease risk among women caregivers of Mexican origin, using the allostatic load model and the Framingham Risk Score. A purposive sample of 20 women providing family care to a dependent older relative for at least 24 hours per week over the past 6 months was recruited through community networks, home health care agencies, promotoras, the local chapter of the Alzheimer’s Association, and hospital outpatient services in a U.S.–Mexico border city. Multiple approaches were employed, including structured interviews and the collection of biological samples. Key adjustments included refining terminology to align with participants’ preferences, managing complex data collection, and adjusting recruitment criteria to reflect cultural norms. COVID-19-related delays necessitated further adaptations, including proactive licensing management and alternative recruitment strategies. Inclusion and exclusion criteria were revised multiple times to better reflect family caregiving dynamics, ensuring continuity despite staff turnover and rising costs due to the study’s extended duration and inflation. By addressing these challenges, we laid the groundwork for research on long-term caregiving among women of Mexican origin. Future research will focus on developing preventive interventions to reduce caregiving stress and coronary heart disease risk, ultimately supporting aging-in-place for dependent older adults in their care.
Keywords
Family caregivers within Hispanic/Latino (H/L) populations are experiencing an alarming decline in health, a trend that demands urgent public health attention. As the number of H/L individuals aged 65 and older in the United States is projected to quadruple by 2060 (Administration on Aging & Administration for Community Living, 2019), caregiving needs will rise sharply, disproportionately affecting H/L women due to enduring cultural expectations (Nava-Schellinger, 2021). Despite this, there is a stark gap between caregiving responsibilities and the resources available to support these caregivers, especially those from socioeconomically disadvantaged backgrounds (Yam, 2017).
According to Bose et al. (2021), nearly 40% of H/L caregivers receive no outside help, and 75% lack access to paid support, compared to just 11% among non-Hispanic white caregivers. These disparities are compounded by the shift to community-based care models, which place increased pressure on families. Among H/L caregivers, women of Mexican origin represent the largest subgroup yet remain notably understudied. Most of the existing research treats H/L populations as a monolith, overlooking cultural dynamics and chronic stress exposures specific to this group. Previous studies indicate that women caregivers face higher risks for coronary heart disease (CHD) compared to men (Haley et al., 2010), yet the mechanisms driving this risk—especially among Mexican-origin women—remain poorly understood.
This feasibility study used McEwen’s (2006) Allostatic Load model and the Framingham Risk Score (FRS; Shulman et al., 2016) to assess the 10-year CHD risk among Mexican-origin women caregivers in a U.S.–Mexico border region by examining challenges encountered during implementation to refine the research protocol aimed at reducing caregivers’ stress-related biopsychosocial burden, thereby supporting older care recipients to age in place.
The study was initially approved by an Institutional Review Board in 2019 but was completed in 2024 due to COVID-related delays. All participants provided informed consent during home visits following a bilingual recruitment process. Research assistants screened participants for eligibility and ensured voluntary, non-coercive participation using culturally appropriate outreach materials in both English and Spanish.
Materials and Methods
This descriptive feasibility study recruited a purposive sample of 20 women caregivers from communities in a U.S.–Mexico border city between 2019 and 2024. Bilingual flyers were used for outreach and were revised during the study to better reflect participants’ cultural self-identification, shifting from the term “Mexican American” to “women of Mexican origin.”
Initial eligibility criteria required participants to identify as being of Mexican origin, be between 50 and 64 years of age, and provide unpaid care to an older adult aged 60 or above with advanced heart failure, classified as Class III or IV by the New York Heart Association. Participants were also required to have provided at least 30 hours per week of direct physical care—such as dressing, bathing, toileting, transferring, personal hygiene, or feeding—for a minimum of 6 months.
Exclusion criteria included primarily performing indirect caregiving tasks, difficulty carrying out caregiving responsibilities, incoherent responses during screening, or a self-reported history of heart disease or mental health conditions. Primary outcome measures included self-reported caregiving burden, psychosocial stress moderators, biomarkers of allostatic load, and a 10-year CHD risk estimate using FRS.
Results
This feasibility study revealed multiple logistical, cultural, and methodological challenges across all phases of implementation. These challenges were addressed through adaptive strategies that enhanced participant engagement, data quality, and protocol feasibility. Key challenges and corresponding resolutions are summarized in Table 1.
Logistical Methodological Challenges Across All Phases of Implementation
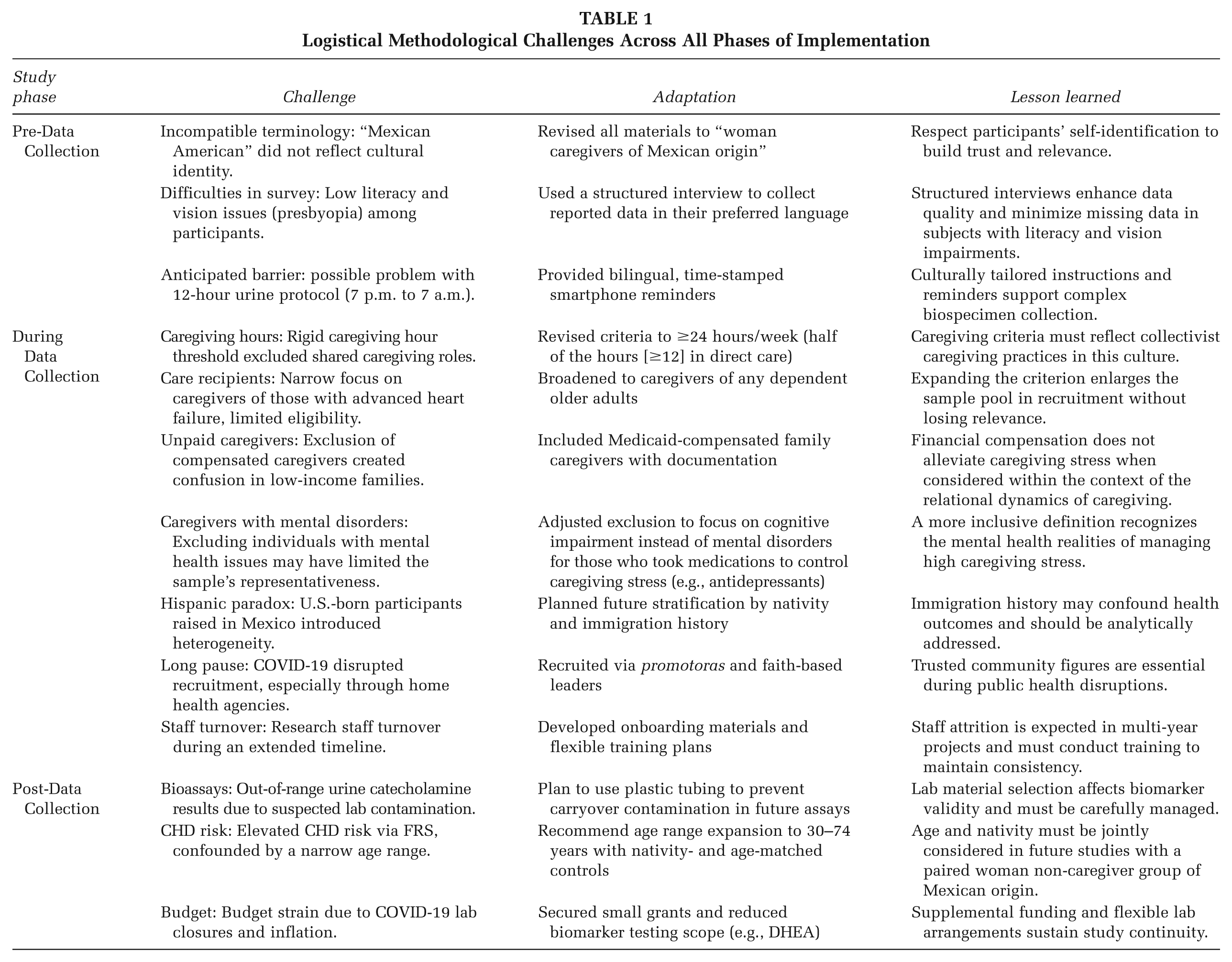
Pre-Data Collection
Recruitment materials initially referred to participants as “Mexican American women caregivers.” However, many Mexico-born women rejected this label, preferring the term “women of Mexican origin” to better reflect their cultural identity. This revision improved recruitment outcomes and highlighted the importance of cultural congruence in participant engagement (Nava-Schellinger, 2021).
The research team initially had concerns about the feasibility of 12-hour urine collection due to the complexity of the process. However, participants successfully completed biospecimen collection when provided with bilingual instructions and smartphone-based reminders, underscoring the value of culturally and linguistically relevant communication strategies.
Due to the high prevalence of limited formal education and vision impairments among participants—45% reported difficulty reading printed materials, and 15% reported being unable to read—interviewer-administered surveys were conducted in participants’ preferred language. Most participants opted to complete the survey in Spanish, highlighting the importance of offering linguistically appropriate instruments. This approach minimized missing data and enabled the inclusion of individuals with limited literacy, consistent with best practices in research involving underserved populations (Yam, 2017).
During Data Collection
The original eligibility requirement of 30 hours per week of direct care over 6 months proved too rigid. In Mexican-origin families, caregiving is often shared among relatives, consistent with cultural values of familism and collectivism (Taylor et al., 2012). The revised threshold—24 total hours per week, including at least 12 hours of direct care—better aligns with national caregiving averages and improved inclusivity (American Association of Retired Persons [AARP] & The National Alliance for Caregivers, 2020).
The initial focus on caregivers of individuals with New York Heart Association (NYHA) Class III or IV heart failure was also limiting, as most families were unfamiliar with this classification. Although heart disease remains the second leading cause of death among H/L populations (Centers for Disease Control & Prevention [CDC], National Center for Health Statistics, 2024), this criterion was broadened to include caregivers of any dependent older adult, thereby enhancing recruitment while preserving clinical relevance.
We encountered complexity in defining “unpaid” caregiving because some family caregivers received modest income-based stipends through Medicaid. Participants receiving Medicaid stipends were retained in the study, with payment status carefully documented. This approach acknowledged the economic realities of caregiving without undermining its relational and emotional context (Bose et al., 2021).
The criterion was revised to exclude only individuals who were unable to understand the study procedures or complete the informed consent and screening process. This allowed inclusion of participants who manage caregiving stress with anti-anxiety or antidepressant medications (Haley et al., 2010).
Unexpected complexity also emerged related to immigration history. Some U.S.-born participants who were raised in Mexico exhibited health profiles more consistent with immigrant populations, echoing patterns observed in the “Hispanic paradox” (Ro & Van Hook, 2021). Future studies should control for both nativity and early-life environment to account for these variations.
The COVID-19 pandemic severely disrupted collaboration with home health care agencies due to concerns about liability. Recruitment efforts subsequently shifted to trusted community figures, such as church pastors and promotoras—H/L community health workers known for providing culturally tailored education and services. Turnover among research staff, particularly graduating students, was managed through structured onboarding materials and detailed documentation, which ensured continuity throughout the study.
Post-Data Collection
Allostatic load was assessed using 13 biomarkers across four subscales: neuroendocrine, inflammatory, cardiovascular, and metabolic. The neuroendocrine subscale was excluded due to suspected carryover contamination in catecholamine samples, likely caused by binding to stainless steel tubing. Plastic tubing will be used in future studies.
Among the remaining three subscales, the metabolic domain—comprising waist-to-hip ratio, total cholesterol, high-density lipoprotein (HDL), and glycated hemoglobin (HbA1c)—yielded the highest average scores. This finding aligns with the elevated prevalence of metabolic syndrome in Mexican American populations (Heiss et al., 2014). Using the FRS, which is validated for estimating 10-year CHD risk in H/L populations (D’Agostino et al., 2008), participants in this sample exhibited significantly elevated CHD risk compared to age- and gender-matched population norms, as determined by Student’s t-test. However, the small sample size limits the generalizability and statistical power of these findings.
The study also faced financial challenges due to inflation and the COVID-19 pandemic-related laboratory closures. Bioassay costs increased by 20%–35%, and staff turnover within laboratories disrupted the sample processing process. To mitigate these issues, the research team secured small supplemental grants, prioritized cost-effective biomarkers, and excluded costly tests such as dehydroepiandrosterone sulfate (DHEA-S) from the neuroendocrine domain. In addition, partnerships were formed with laboratories willing to offer discounts on reagents nearing expiration.
Discussion
This feasibility study confirmed the viability of a culturally responsive protocol for estimating CHD risk among women caregivers of Mexican origin. Although limited by a small sample size, the study provided critical insights into the structural, cultural, and methodological adaptations necessary for conducting research with this underrepresented population at high risk for CHD.
A major contribution was the appropriate refinement of inclusion and exclusion criteria to reflect the lived experiences of Mexican-origin woman caregivers. Adjusting the caregiving threshold to 24 total hours per week—with at least 12 hours of direct physical care—more accurately captured the shared caregiving dynamics typical of familistic cultures (Taylor et al., 2012). Broadening eligibility from caregivers of individuals with advanced heart failure to those caring for any dependent older adult improved recruitment while maintaining the study’s focus on chronic illness-related caregiving stress.
Findings also underscored the importance of linguistic and literacy accommodations. Structured, bilingual interviews enhanced participant engagement and data quality, particularly for individuals with limited reading ability or vision impairments such as presbyopia. In addition, including caregivers who received Medicaid stipends acknowledged the complex economic realities of caregiving in the border region (Bose et al., 2021).
Biomarker analyses revealed elevated metabolic risk, consistent with known disparities in metabolic syndrome among Mexican American women (Heiss et al., 2014). Although urine catecholamine data were excluded from the neuroendocrine subscale of allostatic load due to suspected contamination, FRS indicated significantly elevated 10-year CHD risk compared to population norms.
The study demonstrated adaptability in response to pandemic-related challenges. When formal recruitment channels became inaccessible, trusted community partners maintained the study’s momentum. Similarly, supplemental micro-grants and partnerships with flexible laboratories helped offset budget constraints.
While generalizability is limited, the findings support the need for a larger, controlled study comparing caregivers to non-caregiver women of Mexican origin. Matching participants on variables such as age, nativity, and immigration history will help isolate the specific physiological impacts of caregiving stress.
Implications for Practice and Research
This feasibility study offers critical guidance for both public health practice and future research focused on H/L caregivers. Several key implications emerged:
Culturally congruent terminology and flexible inclusion criteria are essential for accurately identifying and engaging caregivers in collectivist cultures. Public health practitioners and researchers must specifically design criteria, tools and/or interventions that reflect these caregiving dynamics.
Structured, bilingual interviews proved critical in overcoming literacy and vision-related barriers and should be more widely adopted in both research and service delivery. This approach highlights the importance of communication strategies that uphold participant dignity while enhancing data validity.
Elevated metabolic allostatic load and CHD risk, even among relatively young participants, underscore the urgency of early screening and preventive intervention. The use of physiological indicators, such as FRS, supports the development of interventions that address both behavioral and biological risk factors.
Immigration history significantly influences health profiles. In border regions, future studies must stratify or control for nativity and cross-border life experiences. Incorporating these variables will yield more accurate estimates of caregiving stress and more effective, equity-driven public health interventions.
Conclusion
This study demonstrated the feasibility of assessing chronic disease risk among women caregivers of Mexican origin using a culturally responsive, biomarker-informed protocol. Key adaptations to recruitment strategies, eligibility criteria, and data collection methods were crucial for engaging an underrepresented population that faces significant social and structural barriers. The elevated metabolic risk and CHD estimates observed among participants highlight the urgent need for early intervention strategies that address both physiological and sociocultural dimensions of caregiving stress. These findings lay the groundwork for future comparative studies and intervention trials aimed at reducing health disparities in caregiver populations. Investing in culturally grounded, equity-focused research is crucial for advancing health promotion and enhancing outcomes for historically marginalized communities across the lifespan.