
Abstract
The 2024 National Population and Housing Census documented that 5.5 million persons over the age of two in Uganda are living with a disability and could benefit from rehabilitation. Understanding the factors contributing to limited access to rehabilitation services, how these services are being delivered in Uganda, and what the priorities are related to physical rehabilitation is necessary before developing new rehabilitation interventions or community-based rehabilitation programs. In this methodological paper, we explain how a participatory approach was used to collectively define and identify rehabilitation priorities and how this approach will inform the development of accessible physical rehabilitation interventions within the Kasese District. First, we completed an environmental scan of relevant rehabilitation literature to identify what existed, then we conducted virtual meetings with team members in Canada and Uganda to share knowledge around current physical rehabilitation needs and identify research gaps in service delivery. Finally, we hosted community-led in-person meetings with people living with a disability to identify and define rehabilitation priorities to improve access to basic rehabilitation services in Kasese, Uganda. The use of a participatory approach led to mutual learning opportunities and capacity building between community-based health workers from a lower-income country and academics from a higher-income country. It facilitated the development of international partnerships and the co-creation of action-based rehabilitation research priorities. Our priorities, based on the needs of persons living with a disability in the Kasese District of Uganda, will inform the development of future community-based rehabilitation projects.
Keywords
Access to rehabilitation, while poorly measured, is limited in low-and middle-income countries (LMIC, Bright et al., 2018), yet the need for rehabilitation services continues to increase globally (Cieza et al., 2020). Rehabilitation is defined by the World Health Organization (WHO) as “a set of interventions designed to optimize function and reduce disability” (WHO). In 2017, the World Health Organization launched the Rehabilitation Call for Action 2030 (Gimigliano & Negrini, 2017), documenting ten priority areas, including the development of rehabilitation service delivery models to improve equitable access to health care. This priority aligns well with the United Nations’ Sustainable Development Goal 3 to “ensure healthy lives and promote well-being for all at all ages” as well as with the Institute of Population and Public Health’s mandate to improve coherence, support informed decision-making, and foster international alliances in global health research activities (Canadian Institutes of Health Research [CIHR], 2021).
Uganda is a multi-ethnic East African country with an estimated total population of 50 million people. Kasese is a district within the Rwenzururu region of Uganda where 55.5% of the population is below 18 years old, with only 23.2% of households using grid electricity reported (Uganda Bureau of Statistics, 2024). The Kasese District borders the Democratic Republic of Congo, which has a long history of conflict and violence (Khisa & Rwengabo, 2022), a context that often leads to increased rehabilitation demands and reduced provision of services.
The 2020 Persons with Disability Act, from the government of Uganda, advocates for the respect and promotion of the fundamental human rights and freedoms of Persons with Disabilities, including non-discrimination in the provision of health services, non-discrimination in the provision of education services, non-discrimination in employment and access to justice, information, and training (Inclusive features, 2021). Within this Act, it is stated that rehabilitation should be offered and provided to all persons living with a disability. However, a substantial gap in rehabilitation provision for persons living with a disability still exists in Uganda, one of 33 countries reported to have limited access to rehabilitation (Burke & Persi Vicentic, 2014). According to the 2024 National Population and Housing Census, the prevalence of Ugandans over the age of two living with a disability is estimated to be 5.5 million persons (13.2% of the population) (Uganda Bureau of Statistics, 2024). Access to physical rehabilitation is critical to the motor development of children and the function of adults living with a disability. However, evidence suggests that only 26% of persons in Uganda living with a disability utilize rehabilitation services (Zziwa et al., 2019). Furthermore, the country reveals a limited workforce to offer physical rehabilitation services, with only 276 physiotherapists currently registered with the Uganda Association of Physiotherapy and 736 physiotherapists/occupational therapists registered on the Allied Health Professionals Council (Allied Health Professionals Council, 2025). This misalignment between the awareness of rehabilitation services, the needs/demands, and the delivery of /access to rehabilitation services would suggest important discrimination in the provision of rehabilitation services. It also demonstrates that capacity-building projects aimed at improving health equity for persons living with a disability are essential.
Initiatives, although limited, targeting the knowledge and awareness of rehabilitation as well as the delivery of rehabilitation care have emerged in Uganda. For example, a research group from the Mbarara University of Science and Technology have identified priorities related to physiotherapy education (O’Sullivan et al., 2017). Using an appreciative inquiry workshop, they developed a partnership aiming at facilitating knowledge-sharing. The Learning, Acting, and Building for Rehabilitation in Health Systems (ReLAB-HS) from Johns Hopkins International Injury Research Unit have investigated the use of assistive technology to improve access to rehabilitation services within the public health system. However, this initiative was focused on districts in the North and East of Uganda. In rural, underserved areas of the Kasese District, rehabilitation research priorities have not yet been established. This further contributes to the inequities in rehabilitation service delivery. Another study by Zziwa et al. (2019) identified factors contributing to access to rehabilitation services. The most significant factors included low socio-economic status, education level, age, sex (i.e., male access > female), and awareness of services (Zziwa et al., 2019).
Rigorous co-development of research priorities based on these factors, as well as the needs of persons living with a disability (PWD) in the rural context of Kasese, is an essential step in improving equitable access and delivery of rehabilitation services.
Before implementing new solutions, a culturally informed understanding of factors and context contributing to poor access to rehabilitation services and how these services are being delivered in the Kasese District is necessary. With the growing use of technology within rehabilitation, this is an ideal time to use telecommunication platforms to facilitate knowledge exchange and capacity-building between health care providers, described as teleconsultation (Deldar et al., 2016) and build-capacity around the use of remote rehabilitation interventions described as telerehabilitation. Our team has previously shown the feasibility and effectiveness of using telerehabilitation with PWD in rural settings (O’Neil et al., 2023, 2024). Since teleconsultation has the potential to facilitate capacity building and knowledge exchange between knowledge-users, researchers, and community partners, potentially leading to training on the use of telerehabilitation, we used teleconsultation models to facilitate capacity building between rehabilitation professionals in Canada and community-based health care providers in the Kasese District of Uganda.
Objectives
With an overarching goal of optimizing access to rehabilitation services for PWD, we intend to explain how we used a participatory approach to collectively identify and define rehabilitation priorities, and how this approach will inform the development of future rehabilitation interventions. Precisely, in this methodological paper, we explain how using a participatory approach facilitated the development of international partnerships and the co-creation of action-based rehabilitation priorities and research questions based on the needs of PWD in the Kasese District in Uganda.
Methodology
Participatory Approach
This project was guided by the CIHR’s Framework for Action on Global Health Research, which positions a) transformative impact, b) alignment and international collaborations, and c) capacity-building and communication as pillars within global health research (CIHR, 2021). Based on these pillars, we used a community-based participatory approach to identify research priorities around access to rehabilitation services in Kasese District, Uganda. Participatory research is an approach that prioritizes the needs of a person, most often persons who are in situations of inequities, by using validated research methods and harmonizing these methods with persons’ engagement and partnerships (Brydon-Miller et al., 2020; Cornish et al., 2023; Duea et al., 2022). To operationalize this approach, an advisory committee typically ensures that voices from the community are well represented (Duea et al., 2022; Pratt & Hyder, 2016), following relational and transformative principles that put forward lived experience and action-driven changes (Cornish et al., 2023).
Iterative and Multifactorial Research Planning Methods
Based on participatory action research principles of building trust, exchanging knowledge, fostering relationships, and prioritizing actions (Jones et al., 2022), our international collaborative team discussed the following main topics for the research planning project: What are the current rehabilitation needs, how are those needs assessed, and can technology be used to deliver rehabilitation services? Which research questions related to rehabilitation needs and service delivery should be tackled first? We used a participatory approach to create meaningful knowledge-sharing spaces by using practices grounded in health equity and justice throughout five sequential steps:
Critical Steps Before the Research Planning Project: Creating Space
First, we partnered with Non-Governmental Organizations (NGOs) from Canada (CanUgan) and Uganda (Kadupedi) in 2021. Over the course of one year, we secured a stable internet connection and created a communication hub between Ottawa, Canada and Kasese District, Uganda. We used the communication hub to pilot the use of teleconsultation and train members of the team on using teleconsultation. With communication facilitated between members of CanUgan, Kadupedi, and the University of Ottawa, School of Rehabilitation Sciences, we co-developed this research planning project.
Environmental Scan Using TRIC Form: Sharing Knowledge
We conducted an environmental scan using the Template for Rehabilitation Information Collection (TRIC) form (World Health Organisation, 2019). The TRIC form guided the search strategy, data collection, and development of the data extraction form. We used key domains included in the TRIC form to paint a current picture of the rehabilitation provision in Uganda. Key domains included demographic and general information, rehabilitation needs and provision, assistive technology and devices, and human resources. We searched two scientific databases (Web of Science, PubMed) and gray literature, including policy reports around rehabilitation, and rehabilitation professional associations (e.g., physiotherapy, occupational therapy, community-based rehabilitation), using key domains of the TRIC form as search terms. Sources without scientific data, from areas other than Uganda, were excluded. Two team members extracted data on 1) social determinants and health equity indicators such as age group, sex/gender, area (i.e., rural or urban), income, ethnicity, level of education and language, and 2) specific rehabilitation needs (i.e., health conditions, age), and provision (i.e., human resources, service delivery, access, assistive devices). We also added a telerehabilitation/teleconsultation section to the data extraction form to align with the teleconsultation and telerehabilitation objectives of our planning project.
Virtual Knowledge Exchanges: Strengthening Collaborations and Capacity Building
Informed by findings documented with the environmental scan, we hosted four virtual meetings over one year, allowing a group of interdisciplinary experts, including physiotherapists, rehabilitation specialists, a social worker, community-based health care providers, and an engineer, to share knowledge and compare lived experiences with rehabilitation needs before the in-person visit. These virtual conversations provided space for lived experience and context to the findings identified by the TRIC form.
In-Person Community Visits: Building Trust and Fostering Relationships
We conducted in-person community visits over the course of 9 days to establish action-based research priorities based on the needs of persons with lived experiences and those living with a disability from various communities within Kasese District. Members of the Kadupedi team, including adults living with disabilities, women, and community-based health care providers, were invited to this process of needs identification. The community representative chaired the meetings to ensure higher engagement of community experts who are usually underrepresented. In addition, the chair, a local and native speaker, acted as an interpreter to ensure all persons could participate in the meeting in their preferred language. Six community meetings (n~350) were organized by the Kadupedi team to ensure adequate representation from the district. Community members were invited to sign a meeting participation form if they wanted; all meetings were voluntary and used a strength-based approach (Coghlan & Brydon-Miller, 2014), which allowed us to identify collective knowledge needs.
Co-Creation of Action-Driven Research Priorities and Questions: Prioritizing Action
As part of our health equity principles and mutual learning space, the last in-person meeting served to finalize and order the research priorities. This meeting was co-chaired by an academic from the University of Ottawa, Canada, a community member from Kadupedi and approximately twenty board members of Kadupedi representing persons living with various disabilities. First, an extensive list of rehabilitation needs, current technologies, and research priorities informed by the environmental scan (step 1), co-created during previous virtual knowledge exchange and in-person meetings (steps 2 and 3), was presented. Then, board members and community members representing a larger group of PWD shared knowledge around rehabilitation needs and collaboratively prioritized rehabilitation needs for children and adults and voiced their priorities related to rehabilitation delivery within the Kasese District. Women were invited to speak first and share their top rehabilitation research priorities, followed by the same process with other members. An iterative process of choosing “top three” priorities was conducted until everyone agreed. We conducted a final virtual meeting with the initial international team of experts to tailor research questions based on the voices of the community. The goal of this meeting was to validate the priority list established during the in-person visit and generate a methodology for potential research questions that were coherent, collaborative, and aligned with the needs of PWD in Kasese, Uganda. We considered sub-topics such as the continuum of care, age, health conditions, and sex when deciding on the order of priority.
Concrete Ethical Practice to Reduce Inequities
We co-developed and agreed on a research planning practice aiming at reducing inequities by combining knowledge and experiences from westernized academic perspectives and traditional non-westernized community views. We scheduled the in-person visit to avoid the summer rainy season in Uganda and promote accessibility within rural areas. The in-person community meetings were co-chaired by representatives from Canada and Uganda. Females and experts living with a disability were always invited to speak first. A member of the Uganda team assisted with interpretation when needed to ensure that everyone had a voice. Since a survey prepared by the Economic Research Center in 2021 still reports gender disparity in decision-making positions (Economic Policy Research Center, 2021), we put specific measures in place throughout the research planning project to reduce sex-based inequities. We used a round table process during the last day of in-person meetings to provide everyone with the same opportunity to share. Mothers’ and children’s rehabilitation needs were prioritized as topics of conversation in the development of the research priority list. These various practices ultimately resulted in a robust international partnership that led to a co-created list of rehabilitation priorities and co-developed action-based research questions. This development project was reviewed and exempted by the uOttawa REB since it met quality improvement and planning project criteria. This was clearly stated to our partners. As a team, we continued to follow these criteria throughout the project. We explained the planning process to all PWD in various communities, and those who shared their voices were asked to sign an attendance sheet.
Results From Our Multi-Step Participatory Approach
Environmental Scan
Based on results from our environmental scan and data collected from the literature using the TRIC form, the top causes of disabilities linked to traumatic causes were falls for children and road traffic injuries for adults (Lin et al., 2019; Siddharthan et al., 2021; Zheng et al., 2021). Both injuries often lead to brain injuries (Mehmood et al., 2018), spinal cord injuries (Stothers et al., 2017), and orthopedic injuries (Zheng et al., 2021). Our scan also showed that the main causes of disabilities linked to non-communicable diseases were cerebral palsy and spina bifida for children (Andrews et al., 2019; Kakooza-Mwesige et al., 2017; Sims-Williams et al., 2018; Tann et al., 2021; Warf et al., 2011) and orthopedic injuries and cardiovascular illness for adults (Siddharthan et al., 2021). The top causes related to communicable diseases were malaria in children (Mpimbaza et al., 2020) and HIV among adults (Government of Uganda & Ministry of Health, 2022). Although this literature was situated in a Ugandan context, few studies were specific to Kasese District.
When exploring service provision and assistive devices using domains from the TRIC form, we identified limited and contrasting information related to community-based rehabilitation (CBR) programs. Two studies on CBR and wheelchair provision identified CBR workers as being well-positioned for assistive device provision (Hamid et al., 2017; Seymour et al., 2019) due to their presence within communities and knowledge of the field. However, a report developed by the Uganda Ministry of Health on assistive technology and capacity assessment describes a lack of assistive device lists and procedures to connect and coordinate potential beneficiaries to providers (Ministry of Health & Clinton Health Access Initiative, 2020). This is often due to limited training for CBR workers and challenges in maintaining program sustainability (Brydges & Munro, 2020).
Technology, including mobile devices such as cellular phones, smart applications, and wearables, is becoming increasingly vital in health care for service provision and health monitoring. However, results from our environmental scan of the literature show that their use is still emerging in rural areas and LMICs. A study in a sub-region of northern Uganda investigated the use of mobile phones among prosthetic users and revealed that a higher percentage of prosthetic users own mobile phones compared to non-users (Yagos et al., 2022). Two other studies were conducted on the use of mobile phones among persons post-stroke and their families. One identified that mobile phones could facilitate communication and social wellbeing, motivate and organize daily life, and promote belonging (Kamwesiga et al., 2017). The other study exploring the impact of mobile-phone-supported rehabilitation intervention named F@CE on caregivers was conducted in an urban area and documented a reduction in the burden of care by providing caregivers with education (Eriksson et al., 2021). This review demonstrated a critical gap in the literature on rehabilitation needs, service provision, and telerehabilitation specific to the Kasese District, Uganda and highlighted the necessity for participatory approaches to determine the rehabilitation priorities within this context.
Capacity-Building Using Virtual Meetings
Each step of the participatory approach allowed for capacity building. Along with the initial year of partnership building, we created an equitable knowledge-sharing space, built teleconsultation skills, and established a collective understanding of the project’s objectives. In the first virtual meeting, we took the time to introduce each other, state our positionality, and share some experiences. In the second and third meetings, we explored perspectives from lived experiences with rehabilitation needs, rehabilitation research, policies, and service provision priorities. We also reviewed and discussed the findings from the environmental scan. We discussed the lack of scientific evidence related to rehabilitation interventions or community-based rehabilitation programs in the Kasese District. Our community experts on the research team shared that rehabilitation data from the east of the country may be lacking due to civil unrest and limited reach within the area. From their experience, they reported that persons living with disabilities hide, and in their opinion, there is a need to increase awareness and advocacy for the rights of PWD within the district. When reflecting on the possible causes of mobility issues in the rural areas of the Kasese District, they shared that cerebral palsy in children and growing adults, combined with epilepsy and hypertension leading to stroke and paralysis, were the main observed causes of mobility impairments. They also raised concerns around the impact of landmines from the civil war that may cause amputations in older individuals. As far as the provision of rehabilitation services within the community in the Kasese District, the main access barriers to services in rural areas shared by our experts were 1) the distance to rehabilitation services (e.g., hospital-rehab services: 187km; distance of rehabilitation center in Fort Portal: 87km), combined with limited methods of transportation (not everyone has a car); only two public hospitals in Kasese; 2) the fees linked to services, for example Kagando and St-Marys are private hospitals with service fee, and Rokuki hospital is in a public center which does not charge for services; 3) long wait times for rehabilitation services and assessment, follow-ups are not done as required; and 4) a lack of awareness of the impact of rehabilitation services. In the fourth meeting, we primarily targeted the preparation of the in-person visit. Combining the findings from the environmental scan and exchange from virtual meetings allowed us to prepare precise discussion points as well as identify areas of need in the Kasese District.
Co-Development of Action-Driven Research Questions From an In-Person Participatory Approach
Team members strengthened relationships with disability associations under Kadupedi and organized 6 community visits in the Kasese District (Figure 1).
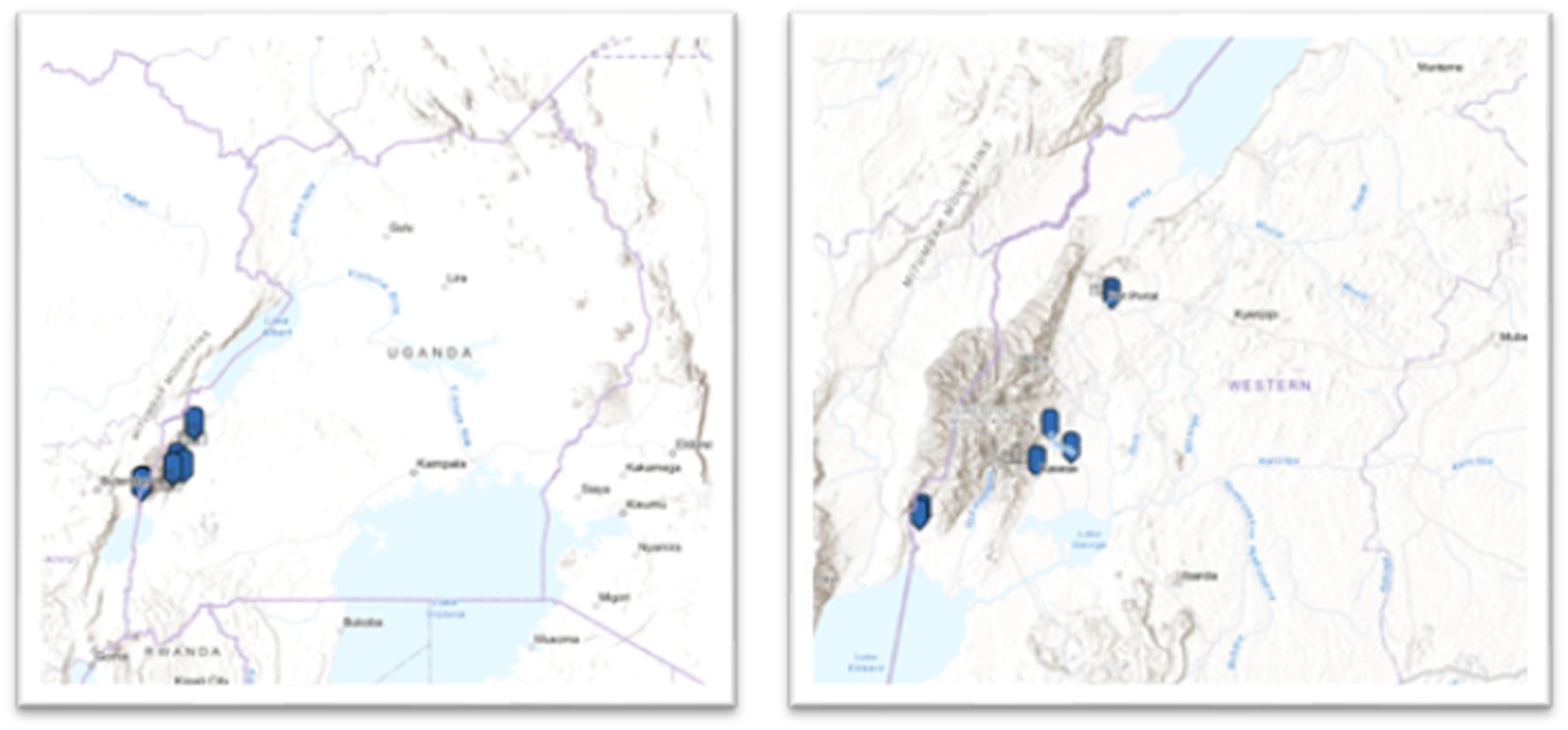
Map of In-Person Visits in the Kasese District During Our Visit in June 2024. The map on the Left Demonstrates Overall Location of the Kasese District Within Uganda. The map on the Right Shows the Location of the 6 Communities Visited Within the Kasese District
During the in-person visits, we solidified international partnerships and co-created a district profile based on shared perspectives from PWD in the Kasese District. This iterative and sequential participatory research planning approach allowed us to understand and identify how rehabilitation services are currently being offered in the Kasese District through a policy, governance, and person-centric lens (Figure 2).
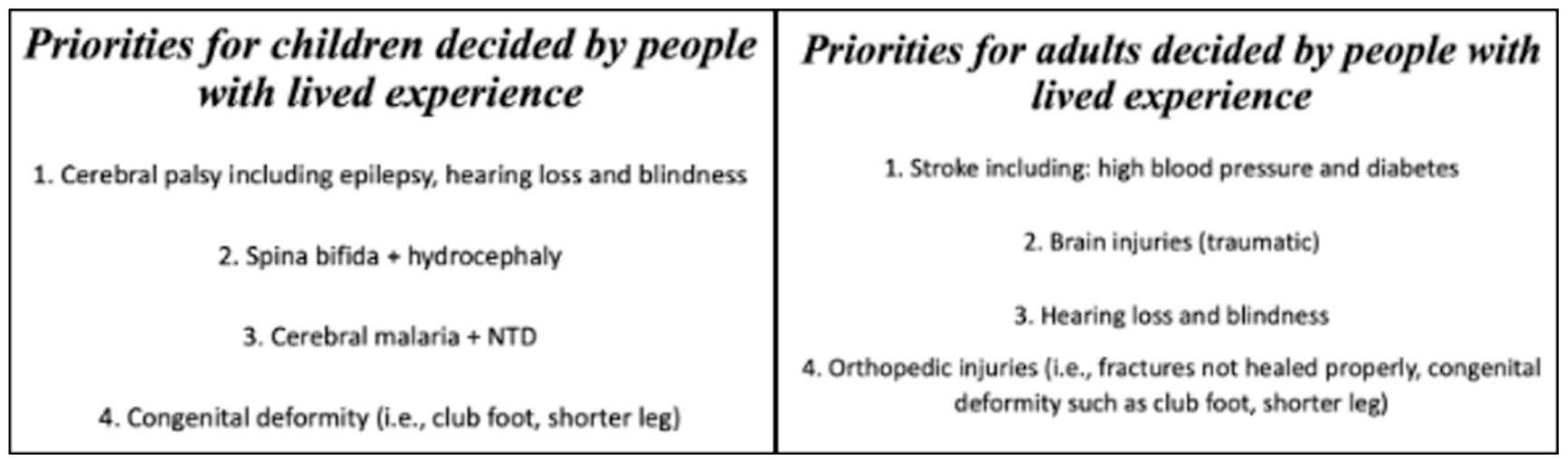
Summary of Rehabilitation Needs Documented by Environmental Scan Using the TRIC Form and Community Partnership In-Person Meetings. Right Box: Representation of Needs in Adults. Left Box. Representation of Needs in Children.
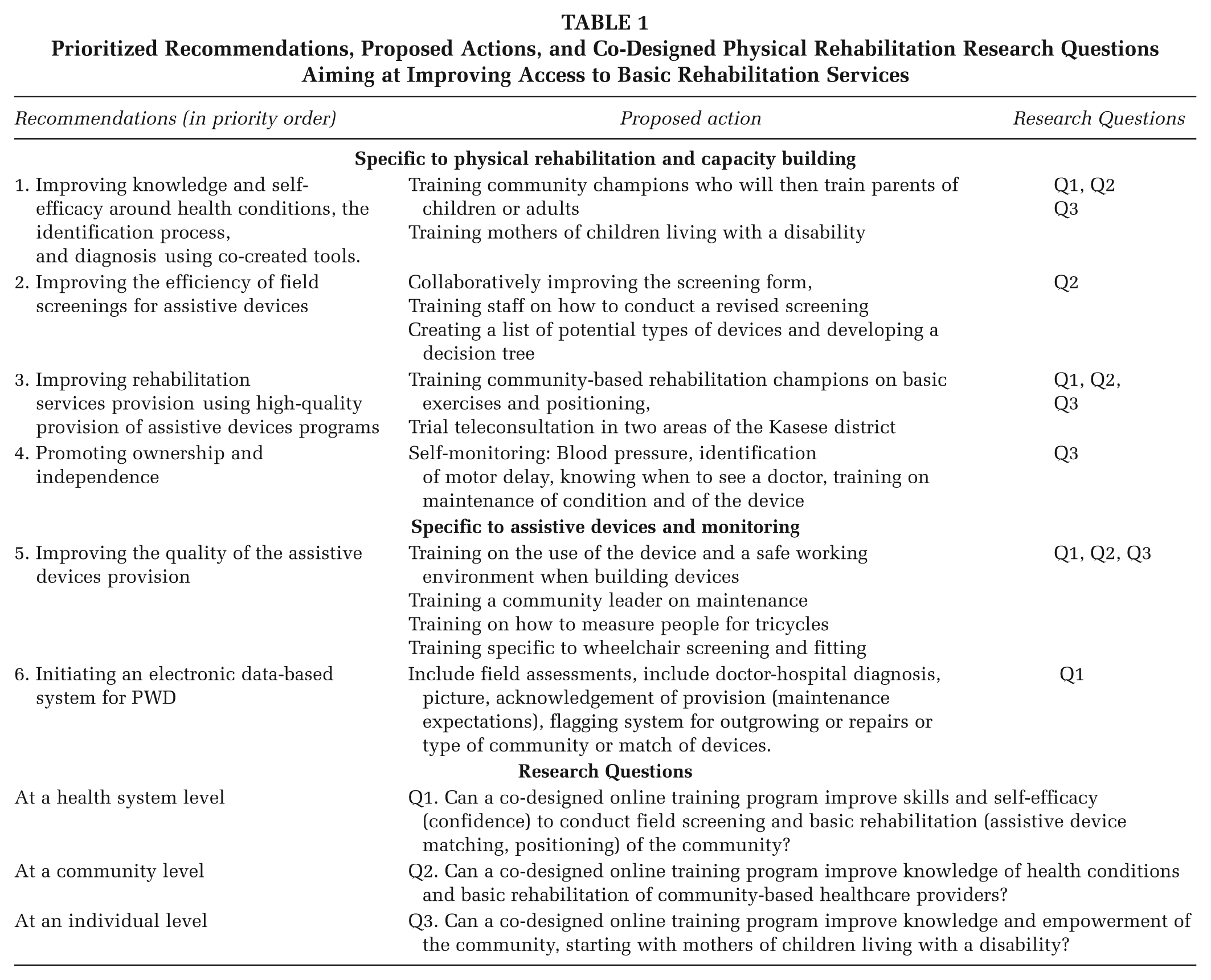
Once the community visits were completed, the advisory board and team of experts identified rehabilitation research priorities based on shared perspectives voiced by PWD and community-based health care providers. This ensured that the proposed priorities were actionable, culturally appropriate and feasible for the Kasese District (Table 1).
Prioritized Recommendations, Proposed Actions, and Co-Designed Physical Rehabilitation Research Questions Aiming at Improving Access to Basic Rehabilitation Services
Discussion
Implications for Practice
Solid and relational partnerships are necessary to foster the development of long-lasting relationships and successful implementation of rehabilitation projects (Pratt & Hyder, 2016; Suarez-Balcazar et al., 2005). Our project demonstrates that a collaborative learning process can solidify intentional and ethical partnerships and can be done in-person, using teleconsultation, or using a hybrid format.
Time, Space, and Context
Allocating time to develop international partnerships facilitated knowledge-sharing and sustainability (Boothroyd et al., 2017). As astutely described by Lurch and Andrion, the consideration of a dynamic space where power is shared is essential to the development of equitable physiotherapy interventions (Lurch & Andrion, 2024). The use of multiple virtual meetings provided the space to build a strong partnership over one year. It provided the team with the necessary time to know each other, share each other’s expertise, strengths, and positionality. Intentionally setting a knowledge-sharing space was essential to ground our project in health equity. This research planning project provided a platform and context for underrepresented groups to have a voice in rehabilitation research. The approach used was participatory, contextual, catalytic, ethical, and empathically valid (Belone et al., 2016). We created environments, both virtual and in-person, where communities that were holding knowledge, experts in their conditions with critical lived experience, could easily participate in the development of meaningful identification of physical rehabilitation actions within the research project. This intentional approach led to setting a context where time and space were respected and allowed for diversity of ideas (Suarez-Balcazar et al., 2005). The in-person meetings were also essential to creating a stigma-free space where all persons could learn about basic physical rehabilitation and share their lived experiences.
Capacity-Building and Communication
The use of a participatory approach rooted in partnership and mutual learning was key to the success of this project. Building core-knowledge was key to the success of the community meetings (Tremblay et al., 2017). As highlighted in the literature, the lack of awareness around rehabilitation services is an important factor contributing to poor access. Capacity building activities emerged throughout the project to ensure that mutual learning of rehabilitation services and growth opportunities were available for all team members, including academic and community. For example, during our virtual and in-person meetings, the research-academic team learned about community-based rehabilitation and how PWD strive to reduce stigma and socially participate in their respective communities. Improving knowledge and self-efficacy around health conditions and basic rehabilitation, starting with the priorities identified in the literature and by community members, is critical.
The community members learned about basic teleconsultation use and rehabilitation provision, building capacity in community-based rehabilitation, and technology literacy, respectively. Factors such as mutual respect, complicity, and ongoing meetings provided excellent opportunities for mutual learning (Tremblay et al., 2017). The creation of a meaningful and effective knowledge-sharing space facilitated the engagement of community members throughout the research planning process. Together, we co-developed participatory research principles, set the timeline, and planned methods to facilitate reaching out to the community. Concretely, we proposed to pilot teleconsultation and eHealth knowledge mobilization activities specific to assistive devices as our next step.
Limitation of this Approach
The rehabilitation priorities identified and defined in this project are community-centered and specific to the Kasese District and the communities with whom the priorities were developed. The rural and remote context, combined with limited digital or rehabilitation literacy, needs to be considered within the priorities as well as future action-based research. It will be crucial to support education and use frugal-low-bandwidth based technology when developing our initiatives. Finally, the main focus of this planning project, being community-driven, limited the input of policy decision-makers and might have neglected the integration of policy and governance. We intend to extend invitations to broader policy leaders in the area in our next project.
Implications for Research: Transformative, Ethical, and Action-Driven
The co-creation process is key to successfully carrying out future projects based on the lived experiences of persons living with a disability, their families, caretakers, and community health workers (Belone et al., 2016; National Academies of Sciences, Engineering and Medicine, 2019). The participatory approach allowed us to compare the information documented in the environmental scan with those experiences reported by PWD in the community and explore their needs specific to the Kasese District. As described in implementation science, understanding the fit or context, dynamically involving end-users, and the use of implementation frameworks are necessary strategies to adapt and implement new solutions (Belone et al., 2016; Wensing & Grol, 2019). This comparative research approach enabled us to identify gaps in the scientific and gray literature while considering lived experience as equally essential, therefore leading to potential solutions that are evidence- and experience-driven. It also allowed us to identify key inequities and data limitations specific to rehabilitation service delivery and access. Documenting physical rehabilitation data that is context- specific is vital to understanding the needs of a community and tailoring sustainable interventions. The inclusion of policy-informed data combined with action-driven solutions is central within a participatory approach (Cornish et al., 2023).
Conclusion
From the perspective of equitable and inclusive rehabilitation and through building strong international partnerships, this project established action-based research priorities co-developed with PWDs from Uganda. This participatory approach allowed us to establish six action-driven rehabilitation priorities based on the existing evidence and lived experiences within a specific context, thus informing the co-development of future research projects. This process allowed us to combine the results from the environmental scan with the community rehabilitation needs specific to the Kasese District. Using a participatory approach and allocating time for research planning ensured that resultant research projects would be guided by ethical and person-centered processes. Concretely, we defined three research questions targeting access to and provision of rehabilitation services for PWD in the Kasese District. We learned that planning time for international relationship building and informal discussion on the current literature, as well as lived experiences, are key elements to document the rehabilitation needs of PWD. It also allowed our team to form strong partnerships based on respect and mutual knowledge-sharing, key to future testing and implementation of new solutions. Future projects using such participatory approaches based on these specific co-designed priorities could have a significant impact on health equity and the wellbeing of PWD in Uganda. Participatory approaches used in this planning project provide a framework for the co-creation of research priorities among other equity-seeking groups or those living in violent conflict contexts.
Footnotes
Author’s Note:
The authors would like to acknowledge the KADUPEDI–an umbrella organization of all associations of Persons with Disabilities in Kasese District team, who welcomed us into their family; the KADUPEDI board members who continue to advocate for the rights of people living with disabilities within their districts; the people living with a disability and their parents, especially mothers, who shared their time and experiences during our visit, and most importantly, who continue to advocate for their children, particularly Janet Kabugho. The authors also acknowledge other CanUgan members who facilitate communications and trusted this team with the project. The authors would like to thank Maryam Khaleqi-Sohi for her work on the literature review. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been funded by CIHR Planning and Dissemination Grant (PCS 191027).