
Abstract
While digital family-based interventions show promise for preventing youth risk behaviors, including violence victimization and perpetration, low engagement can negatively impact the effectiveness and benefits of these programs at the population level. We investigated factors associated with family engagement with a digital dating violence (DV) prevention program developed for youth who have been exposed to intimate partner violence and their mothers. Hypothesized engagement predictors included population and family attributes as well as two program delivery factors—action planning and text message reminders—that were intended to promote program completion. Mothers were asked to complete the self-guided web-based program, entitled eMoms and Teens for Safe Dates (eMTSD), together with their adolescent over a 6-week period (n = 101 dyads). Using a factorial design, participants were randomly assigned to four groups with distinct program delivery features. Population and family attributes were measured at baseline. Two outcome measures assessed program engagement: level of program completion and mother- and adolescent-reported subjective experiences with program modules. Ordinal regression models did not provide evidence that tested program delivery factors were associated with program completion levels. Adolescent mental health and mothers’ perceived program relevance were positively linked to program completion, while adolescent exposure to caregiver violence was negatively associated with program completion. Maternal mental health, adolescent exposure to DV victimization, and family financial stress were associated with more positive subjective experiences with program content. Findings suggest family-based programs should consider how to optimize content and delivery to maximize personal relevance and address mental health challenges among potential participants.
Introduction
Theory and empirical research suggest that families play a powerful role in shaping adolescents’ involvement in interpersonal violence, including violence between individuals in peer (peer violence) and dating (dating violence) relationships (Hebert et al., 2019; Labella & Masten, 2018; Lösel & Farrington, 2012). Family factors, including parenting practices, communication, monitoring, and interparental conflict, shape adolescents’ normative beliefs, emotion regulation, and social problem-solving skills, which in turn influence their risk of engaging in and exposure to these forms of violence. Evaluation research supports the effectiveness of family-based programs in reducing interpersonal violence and other adolescent problem behaviors (Doucette et al., 2021; Haggerty et al., 2013; Matjasko et al., 2012). Yet, despite their promise for supporting families and achieving population-level prevention effects, family-based programs often suffer from low “engagement,” indicated by low rates of program initiation, attendance, or active participation (Chacko et al., 2016; Finan et al., 2020; Haine-Schlagel et al., 2022; LoBraico et al., 2021).
Digital delivery of program content (e.g., via website, text messages, or mobile app) is one strategy that can address common obstacles to engagement in traditional face-to-face family-based programs. By allowing families the flexibility of engaging in the program when and where they choose, digital programs can avert barriers such as transportation difficulties, schedule conflicts, the need for childcare, and perceived stigma (Finan & Yap, 2021). Further, digital programs that require no or minimal professional support may be widely offered at low cost, thereby overcoming structural barriers that prevent the dissemination of family-based programs by community agencies (Haggerty et al., 2006).
An emerging body of research suggests the promise of digital family-based programs for preventing dating (DV) and peer (PV) violence as well as other youth problem behaviors, across diverse populations (Baumel et al., 2017; MacDonell & Prinz, 2017; Morgan et al., 2024; Rizzo et al., 2021; Valero et al., 2024). For example, in a systematic review of 24 studies evaluating digital behavior parent training programs, Morgan et al. (2024) found that all studies reported improvements in at least one behavioral or feasibility outcome. Nonetheless, studies suggest that participant engagement remains a challenge when implementing digital programs (Baumel et al., 2017; Bourdeau et al., 2021; Byrnes et al., 2019; Morgan et al., 2024; Rojas et al., 2021). Systematic reviews show that engagement indicators are often not reported or examined as outcomes in studies evaluating digital interventions (MacDonell & Prinz, 2017; Morgan et al., 2024). In their review of technology-delivered family-focused interventions, MacDonell and Prinz (2017) found that approximately 30% of studies did not report participant completion rates. Consequently, we have a limited understanding of the factors that influence engagement in such interventions.
The Current Study
Research identifying predictors of engagement with digital, family-based prevention programs can inform targeted strategies to enhance participation and encourage developers to explore alternative ways to deliver essential content, thereby improving outcomes for families who drop out or disengage early (LoBraico et al., 2021). Accordingly, the current study aimed to identify predictors of engagement with eMoms and Teens for Safe Dates (eMTSD), a self-directed, web-based program for preventing DV among youth exposed to intimate partner violence (IPV). In this context, IPV refers to violence between caregivers, which adolescents may witness or be indirectly affected by. eMTSD aims to disrupt the intergenerational transmission of IPV by fostering a protective family environment. Guided by Perski et al.’s (2017) conceptual framework, we examined two engagement outcomes—program completion and subjective experience—and their associations with (1) program delivery attributes, (2) population and family characteristics, and (3) demographic covariates.
Conceptual Framework
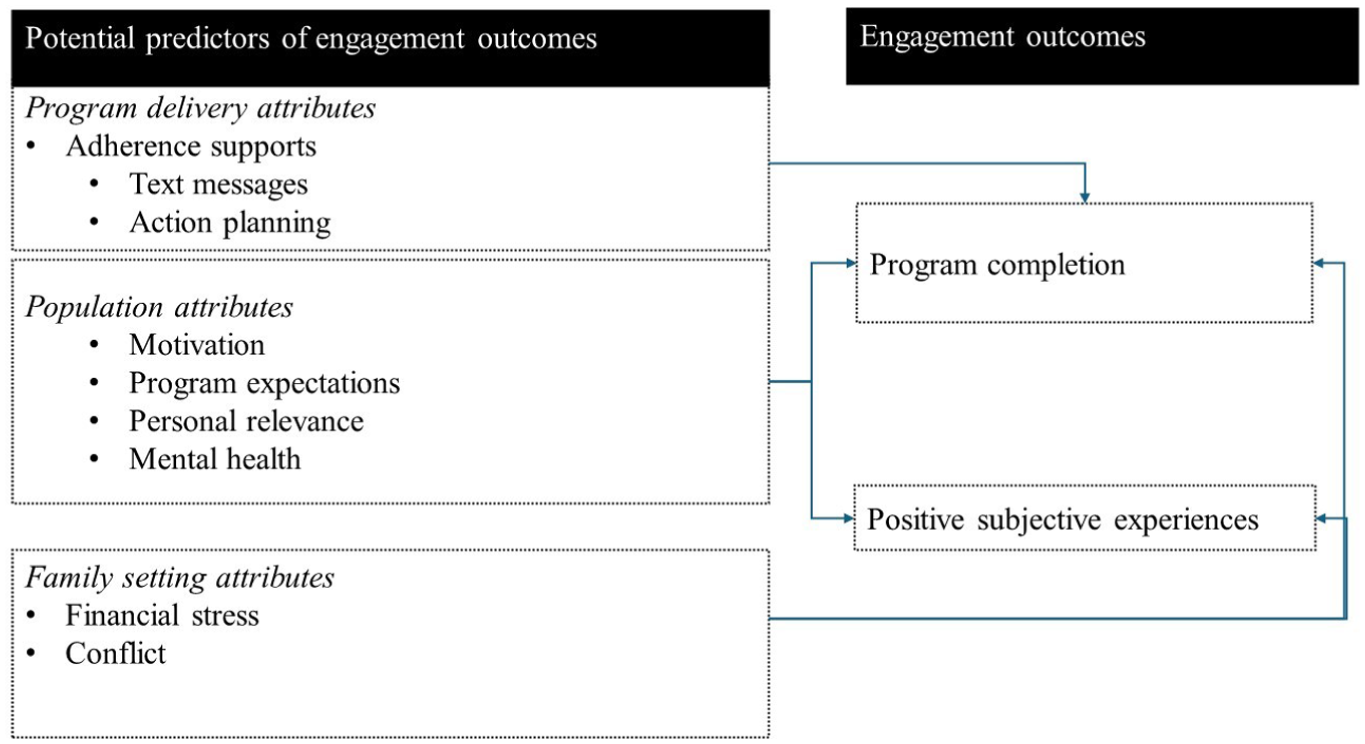
Perski and colleagues’ (2017) conceptual framework of engagement with digital behavioral change interventions (DBCIs) informed both the measurement of engagement outcomes and identification of predictors (depicted visually in Figure 1). According to this framework, engagement with DBCIs can be conceptualized both as (1) a subjective experience characterized by attention, interest, and positive affect when interacting with a DBCI and (2) a behavior characterized by the usage of the DBCI over time. Consistent with this two-part definition, we operationalized engagement outcomes as (1) program completion level and (2) subjective experiences with program modules. The framework also identifies distinct influences on engagement with DBCIs, including attributes of the program itself or its delivery, as well as characteristics of the population using the DBCI and the setting of use. Thus, guided by the framework, we examined the influence of two randomly assigned program delivery attributes—action planning and text message reminders—that were conceptualized as potentially encouraging program use by helping caregivers set goals before initiating the program (action planning) and cueing them to engage (text message reminders). We also examined several population and family attributes that were hypothesized to influence engagement outcomes, including motivation for doing the program, expectations about the program’s effectiveness, perceived program relevance, participant mental health, family conflict, and family financial stress. Associations between demographic variables and engagement outcomes were also assessed. However, because the program was designed to appeal universally to families from diverse demographic groups, we had no a priori expectations regarding these associations.
Study Conceptual Model
Method
Participants
Data are from a pilot study of eMTSD, a self-directed web-based program designed to be completed by maternal caregivers who have been exposed to IPV and their 12- to 16-year-old adolescents that comprises six brief (15–25 minute) modules that can be completed on any device with internet access (Reyes et al., 2022, 2023). Details on study procedures and results related to feasibility and acceptability outcomes have been reported elsewhere (Reyes et al., 2022, 2023). Briefly, study participants were mother–adolescent dyads recruited via social media posting and information dissemination through agencies that work with or provide services to mothers or IPV survivors. Mothers or maternal caregivers residing in the United States were eligible to participate if they: (1) had at least one 12- to 16-year-old child who lived with them at least part of the time, (2) had experienced IPV at some point in their lives after at least one of their 12- to16-year-old children was born, (3) were not currently living with an abusive partner, (4) were able to read and speak English, (5) had access to an internet-enabled device, and (6) were able to receive text messages. Mother participants were nearly all adolescents’ biological or adoptive mothers (97%). The institutional review board at UNC Chapel Hill approved the study.
Procedures
All mother–adolescent dyads who enrolled in the study (n = 106) completed a baseline survey and were randomized to one of four adherence support groups—text reminders (TR), action planning (AP), text reminders plus action planning (TRAP), or low adherence support (LA)—using a factorial design. After randomization, five dyads withdrew from the study due to health reasons (n = 3) or were found ineligible (n = 2). All mothers who enrolled were directed to complete the program modules together with their adolescents over 6 weeks, with a 2-week grace period allowed for families unable to comply. All mothers, regardless of group assignment, received up to three TR if they had not logged in to the program in the first 10 days after enrollment, and one reminder 7 days before their program access would end if they had not completed the program. Mothers in the TR and TRAP conditions received up to eight additional text reminders at fixed intervals. Mothers assigned to the AP and TRAP conditions were asked to complete a brief electronic form before logging into the program. The form prompted them to create an “action plan” outlining how they would complete the program and overcome any engagement barriers.
Measures
Engagement Outcomes
Program completion was coded as 0 if the dyad did not complete the first caregiver-teen module, 1 if the dyad completed the first caregiver-teen module but did not complete the entire program, and 2 if the dyad completed the entire program. Indicators of mother and adolescent positive subjective experiences with each of the five mother–adolescent eMTSD modules were created using responses to three questions that asked how strongly they agreed or disagreed that: (1) they enjoyed doing the module, (2) the module kept their attention, and (3) they learned useful information from the module. Responses were averaged across the three indicators and scaled to denote the percentage of the maximum possible (POMP) score, interpreted as the percentage of a measure’s total that a specific score represents. Separate POMP indicators were created for both mothers and adolescents, as well as for each of the five modules. The supplemental appendix includes further details on each of the engagement outcomes.
Predictors of Engagement
Demographic Covariates
Adolescent demographic covariates included age, sex at birth, sexual or gender minority status, race, and exposure to abuse by a caregiver. The demographic covariates for mothers were age, current partner status, education, and domestic violence protective order status. For details on measures and coding, see the supplementary appendix.
Program Delivery Attributes
The text message reminder was coded as 1 if the dyad was assigned to the TR or TRAP conditions and 0 otherwise. Action planning was coded as 1 if the dyad was assigned to the AP or TRAP conditions and 0 otherwise.
Population and Family Attributes
Population and family attribute variables were coded such that higher levels indicated greater maternal motivation, more positive maternal program efficacy expectations, greater relevance of the program to both mothers and adolescents, higher levels of maternal and adolescent psychological distress, increased family conflict, and greater family financial stress. All variables were scaled using POMP scores except for adolescent program relevance, which was assessed using an indicator of prior involvement in DV victimization, and was coded as 0 (no acts reported), 1 (one act reported), 2 (2–4 acts reported), or 3 (5 or more acts reported). The supplementary appendix provides details on the measures, coding, and psychometrics of the variables.
Analytic Strategy
Program Completion
We used ordered logistic regression models to examine predictors of program completion for all enrolled participants who did not withdraw from the study (n = 101). First, we examined the main and interaction effects of TR and AP in predicting program completion. Second, we examined associations between each demographic covariate and program completion. Because we had no a priori hypotheses regarding these associations, we treated these analyses as exploratory and used the Benjamini–Hochberg adjustment to retain an overall false discovery rate (FDR) of 5%. Third, we estimated a multivariable model that included all the hypothesized population and family attributes as predictors plus demographic covariates that were significantly associated with the program completion after adjustment for FDR.
Positive Subjective Experiences
Reports of positive subjective experiences with each module (n = 5) were reported separately by mothers and adolescents and were nested (repeated) within participants. We analyzed the data separately for mothers and adolescents using a mixed-modeling approach to account for the nested data structure. For these models, we did not examine the program delivery attributes as predictors, as these factors were intended to prompt program completion but were not intended to impact subjective experiences of the program. We first estimated a “base” model that included only module number as a categorical predictor. Second, we estimated models for each demographic covariate with adjustment for FDR. Third, we estimated a multivariable mixed model that included module number, each of the hypothesized predictors, and demographic covariates that were statistically significantly associated with subjective experiences after FDR adjustment.
Across models for both outcomes, multiple imputation (MI) was used to deal with missing data on covariates (n = 4) and subjective experiences outcomes (n = 28). Specifically, using StataNow/SE 18.5, we created 10 imputed datasets using the multivariate normal method. All covariates and outcomes with missing data were included in the imputation equation, and estimates were pooled across datasets. Robust standard errors were used across all models.
Results
Participant Characteristics
Table 1 reports descriptive statistics for demographic, predictor, and program completion outcome variables. Figure 2 illustrates caregiver and adolescent POMP scores for positive subjective experiences with the eMTSD program, categorized by module. Notably, across all modules, mothers reported more positive subjective ratings of their experiences than adolescents.
Descriptive Statistics for Study Variables (n = 101)
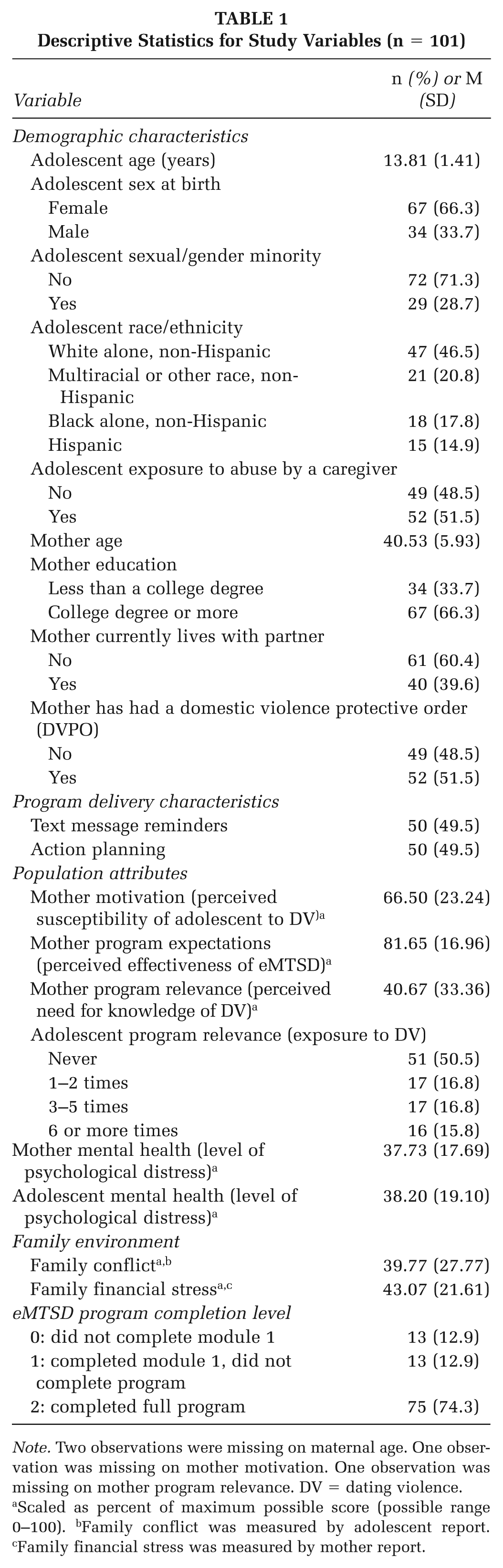
Note. Two observations were missing on maternal age. One observation was missing on mother motivation. One observation was missing on mother program relevance. DV = dating violence.
Scaled as percent of maximum possible score (possible range 0–100). bFamily conflict was measured by adolescent report. cFamily financial stress was measured by mother report.
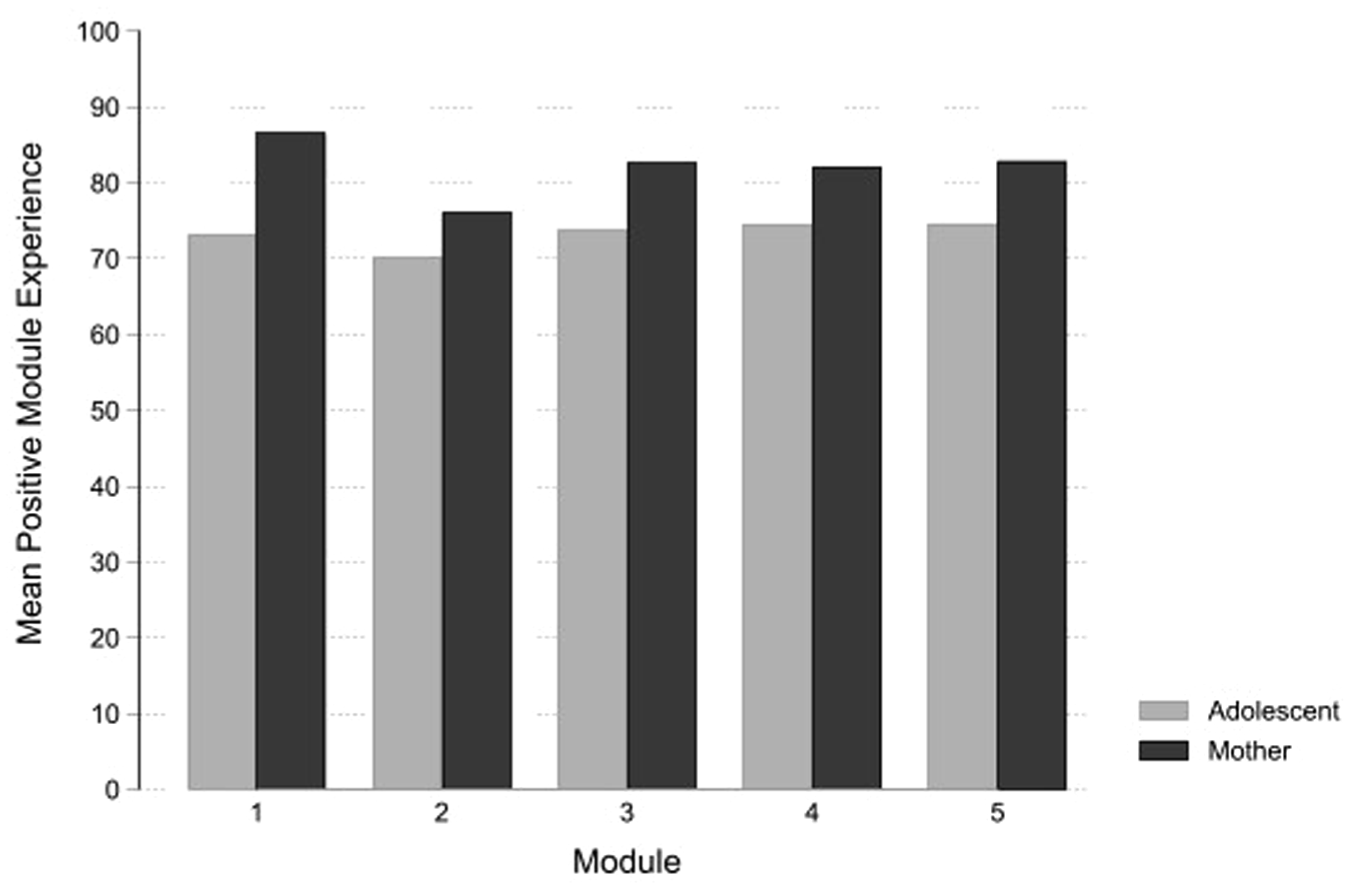
Mother and Adolescent Positive Experiences With the eMTSD Program by Module
Predictors of Engagement
Program Completion
The interaction between text message reminders and AP was not statistically significant (p =.19). Further, in the model that included the main effects of each factor but no interaction, neither TR (OR = 1.24, 95% CI = [.50, 3.04]) nor AP (OR = 1.34, 95% CI = [.53, 3.35]) were significant predictors of completion. In models examining demographic covariates, adolescent exposure to abuse by a caregiver (OR = .22, 95% CI = [.08, .59, p = .003) and maternal age (OR = .91, 95% CI [.85, .98, p = .008) were each negatively associated with program completion after adjustment for FDR (see Supplemental Table 1a for all FDR-adjusted hypothesis tests). The results of the multivariable model that included all hypothesized population and family attributes are presented in Table 2 (for bivariate associations, see Supplemental Table 2). Consistent with expectations, greater mother program relevance was associated with increased odds of program completion (AOR = 1.04, 95% CI = [1.02, 1.06], p < .001) and worse adolescent mental health was associated with lower odds of completion (AOR = .96, 95% CI = [.93, .99], p = .02). There were no other statistically significant associations between population or family attributes and program completion.
Adjusted Odds Ratios and 95% Confidence Intervals From Ordered Logistic Regression Models Assessing Associations Between Population and Family Setting Attributes and Program Completion
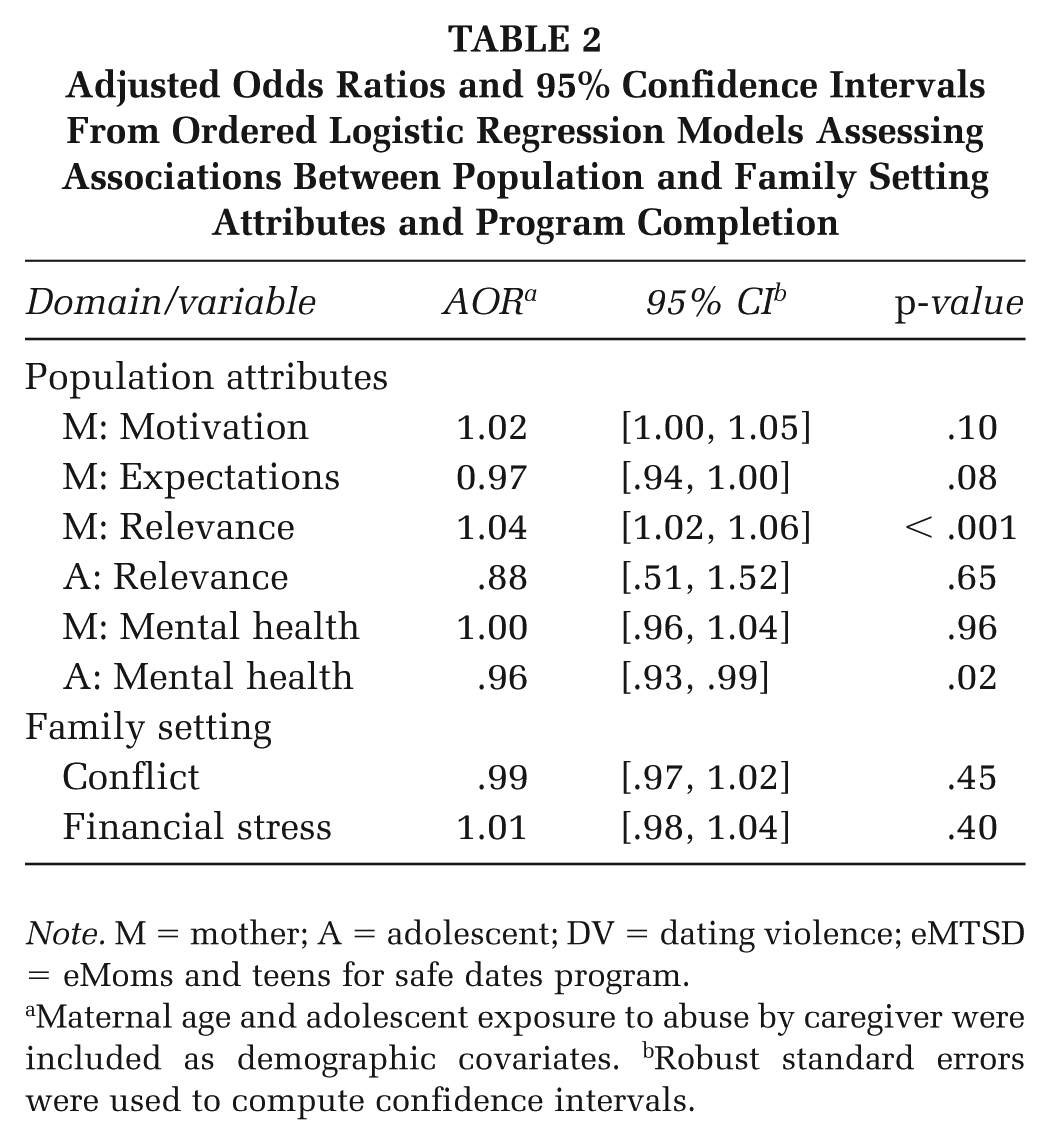
Note. M = mother; A = adolescent; DV = dating violence; eMTSD = eMoms and teens for safe dates program.
Maternal age and adolescent exposure to abuse by caregiver were included as demographic covariates. bRobust standard errors were used to compute confidence intervals.
Subjective Experiences
Results of the mixed model assessing the effects of module number on subjective experiences suggest that, among mothers, reports of positive subjective experiences were significantly lower for Module 2 than for Modules 1 (p < .001) and 3 (p = .01). No other pairwise differences were statistically significant for mothers or adolescents. Models examining associations between demographic factors and subjective experiences found no statistically significant associations (Supplemental Tables 1b–c). Table 3 presents the results of the multivariable models examining the effects of population and family attributes on subjective experiences (for bivariate associations, see Supplemental Table 3). Consistent with expectations, among both mothers (p = .007) and adolescents (p = .006), poorer maternal mental health was associated with less positive subjective experiences with eMTSD. Contrary to expectations, among both mothers (p = .004) and adolescents (p = .004), higher levels of family financial stress were associated with more positive subjective experiences with eMTSD. As expected, among mothers, higher program effectiveness expectations were associated with more positive subjective experiences with eMTSD (p = .02). Also, as expected, among adolescents, higher program relevance, as measured through exposure to DV victimization, was associated with more positive subjective experiences (p = .004).
Regression Coefficients and Robust Standard Errors From Mixed Effects Regression Models Assessing Associations Between Population and Family Setting Attributes and Reports of Positive Subjective Experiences with eMTSD Program Modules
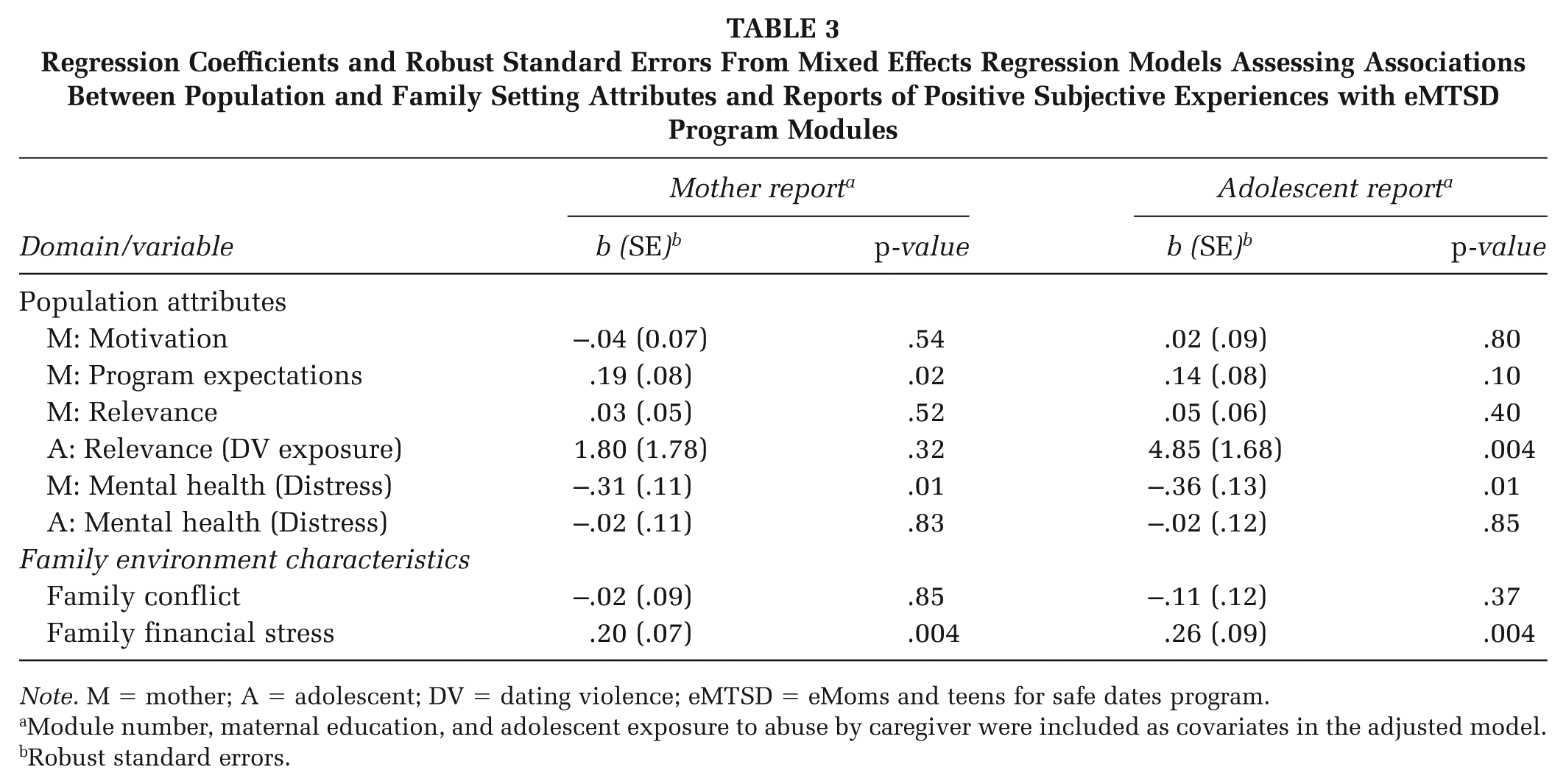
Note. M = mother; A = adolescent; DV = dating violence; eMTSD = eMoms and teens for safe dates program.
Module number, maternal education, and adolescent exposure to abuse by caregiver were included as covariates in the adjusted model. bRobust standard errors.
Discussion
Our findings support the hypotheses that personal program relevance, expectations of effectiveness, and participant mental health predict engagement. Specifically, personal relevance —the connection between program content and participants’ situations—was critical to engagement (Perski et al., 2017). Among mothers, personal relevance was measured as the extent to which mothers indicated they needed more information to communicate with their adolescents about DV. Personal relevance can derive from the perception that a program can be used to fulfill a goal (Priniski et al., 2018). Mothers who perceived that they needed more knowledge to communicate with their adolescent about DV may have seen the program as particularly useful for achieving this goal, resulting in them being more likely to complete the program. Among adolescents, personal relevance was measured as the extent to which they had experienced DV. Personal relevance occurs when content resonates with memory or identity (Priniski et al., 2018). Thus, adolescents with greater DV exposure may have perceived the program content as particularly meaningful or consonant with their own experiences as survivors, leading them to report more positive experiences with the program.
Mothers who expected the eMTSD program would protect their child from experiencing DV reported more positive subjective experiences. Caregiver expectations may “prime” them to view program content positively. Indeed, qualitative research suggests that the expectation of benefits for one child is among the most important factors influencing parents’ willingness to engage with digital programs (Broomfield et al., 2021). Also, consistent with the theory of self-fulfilling prophecy, the expectation that eMTSD will be effective may lead participants to adapt ratings to match expectations (Raita & Oulasvirta, 2011).
Higher psychological distress was linked to lower engagement. Specifically, greater adolescent distress was associated with lower odds of program completion. Greater mother distress was negatively associated with both mothers’ and adolescents’ subjective experiences of the program. Both findings align with research, showing that participant mental health problems are negatively associated with digital intervention engagement (Borghouts et al., 2021), although such findings for family-based prevention programs are mixed (Chacko et al., 2016; Finan et al., 2018; Haine-Schlagel et al., 2022). Mothers of adolescents experiencing psychological distress may have perceived that the emotional costs of completing the program outweighed its benefits. High levels of maternal distress may have hindered mothers’ ability to engage, leading them and their adolescents to report lower positive program experiences.
Contrary to expectations, program delivery attributes, maternal motivation, and family conflict were not associated with engagement. Any effects of program delivery attributes (TR and AP) were likely small because all participants received initial TR and offers of technical support. Thus, the differences between conditions may have been dampened and therefore difficult to detect, given the study’s sample size. More intensive support, such as coaching or health educator calls, may be necessary to facilitate engagement in self-directed digital programs for some participants (Morrison, 2015). The relationship between maternal motivation—measured by perceived adolescent susceptibility to DV—and program engagement may depend on other factors, such as adolescent traits. For example, motivation may not be linked to engagement among mothers whose adolescents are highly psychologically distressed, as distress may interfere with participants’ ability to attend to intervention content and thus motivation to program engagement. Finally, research examining associations between program engagement and aspects of the family relational environment, such as conflict, is mixed (Haine-Schlagel et al., 2022). Accordingly, there may be a nonlinear relationship between family conflict and engagement, such that conflict beyond a certain threshold interferes with engagement.
Unexpectedly, higher levels of family financial stress were associated with more positive subjective experiences with the eMTSD program for both mothers and adolescents. Study participation incentives, tied to research activities, may have been perceived as supportive by families facing economic challenges, positively influencing their subjective experiences of the program. Further research is needed to explore the impacts of monetary incentives—whether tied to research activities or behavior adoption—on engagement in DBCIs.
Families of adolescents who reported having directly experienced caregiver abuse were less likely to complete the program. The traumatic effects of such abuse could hinder teens’ ability to engage in the program with their mother. Further research is needed to understand this finding, as youth who have experienced caregiver abuse and who witness IPV may be particularly at risk for becoming involved in DV and may need additional support to participate in and complete violence prevention programs (Herrenkohl et al., 2020).
Implications for Practice
Health promotion practitioners should ensure that digital family-based interventions integrate tools to address mental health concerns and provide referral pathways. Embedded screeners can identify distressed families and trigger referral messages with support links. Practitioners should also prioritize tailoring content and delivery to maximize personal relevance. For example, incorporating adaptive features, such as algorithms that match knowledge and skill-building content to participants’ needs, may enhance engagement and attention.
Implications for Research
Mothers reported more positive experiences than adolescents, possibly due to greater perceived relevance given their experience as IPV survivors or their caregiving role and desire to protect their children from harm, factors that may increase investment. Prior research suggests that caregivers may rate prevention programs more favorably than adolescents (Rizzo et al., 2021), underscoring the importance of measuring subjective experiences separately among family members. Because noncompleters tended to disengage early, future research should also examine first impressions of DBCIs and identify strategies to foster engagement among those at risk for dropout. Finally, while eMTSD was developed with input from a diverse group of IPV-exposed families (Foshee et al., 2015; Reyes et al., 2022), program content and delivery attributes were not explicitly tailored to participants’ identities or cultural backgrounds. Research is needed to assess whether the influence of engagement strategies and family-level behavior drivers varies across subgroups, to inform whether and how to tailor program content and delivery (Griffith et al., 2024).
Limitations
This study has several important limitations. Use of a convenience sample restricts generalizability to the broader population of IPV-exposed mothers and adolescents. The small sample size limited the statistical power to detect effects and perform subgroup analyses, so null findings should be interpreted cautiously. Reliance on self-reported measures introduces potential biases, including social desirability and recall inaccuracy. The study did not assess all potential predictors of engagement and may have missed key constructs. In addition, the study lacked a qualitative component to provide deeper insight into engagement. Finally, due to funding limitations, eMTSD was developed for delivery in English only; therefore, findings may not generalize to non-English-speaking or English-limited populations.
Conclusions
Findings suggest that personal relevance and participant mental health impact mother and adolescent engagement in digital family-based DV prevention programs. To enhance effectiveness, such programs should prioritize content and delivery strategies that increase personal relevance and address users’ mental health challenges. Future research should explore predictors of engagement using multiple measures and collect data from caregivers and adolescents.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399261419090 – Supplemental material for Predictors of Engagement With a Digital Family-Based Dating Violence Prevention Program for Adolescents Exposed to Intimate Partner Violence
Supplemental material, sj-docx-1-hpp-10.1177_15248399261419090 for Predictors of Engagement With a Digital Family-Based Dating Violence Prevention Program for Adolescents Exposed to Intimate Partner Violence by H. L. M. Reyes, E. G. Armora Langoni, L. A. Sharpless, R. J. Macy, K. E. Moracco and V. A. Foshee in Health Promotion Practice
Footnotes
Authors’ Note:
The authors would like to thank the Connected Health for Applications and Interventions core team at the University of North Carolina at Chapel Hill for their work in developing the web-based program, community-based organizations for helping with recruitment for this study, and the mothers and teenagers who will participate in this study. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported in this publication was fully supported by an Injury Control Research Center award (R49-CE003092) from the Centers for Disease Control and Prevention and National Center for Injury Prevention and Control. The findings and conclusions of this publication are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.