
Abstract
After the fall of Saigon in 1975, waves of Vietnamese refugees and immigrants migrated to the United States. Currently, 2.3 million Vietnamese live in the United States. Many arrived with adverse conditions; however, their health data is scarce. After 50 years, many are aged and may have unmet health needs. To fill this gap, we developed the Vietnamese Aging and Care Survey (VACS) and collected their comprehensive health data in Houston, Texas (N = 402). It revealed a high prevalence of physical, mental, and cognitive disabilities. Using the university–community partnerships, we developed a linguistically and culturally tailored dementia one-pager, formed the Cognitive Health Initiative (CHAIN), and offered complimentary memory tests to monolingual Vietnamese refugees and immigrants. This study reported how CHAIN has operated for the past 2 years. Using the Cultural Exchange Model, we trained bilingual/bicultural Vietnamese university students (Cohort 1) and conducted cognitive assessments, the Vietnamese Montreal Cognitive Assessment (MoCA-V), in 2023. In 2024, when Cohort 2 students joined, we formed mentor (Cohort 1)-mentee (Cohort 2) dyads. Cohort 1 demonstrated the assessment, whereas Cohort 2 observed their mentors perform assessments. After several demonstrations, Cohort 2 tried the assessments supervised by Cohort 1. They repeated this sequence until Cohort 2 felt comfortable conducting the assessments independently. During 2023–2024, we recruited 52 students, attended 16 Vietnamese health fairs, and offered 406 MoCA-V assessments. Through the mentor–mentee relationships, CHAIN promoted teamwork, accountability, ethics, and responsibility to the community and demonstrated successful university–community partnerships.
Following the fall of Saigon in 1975, three waves of Vietnamese refugees and immigrants migrated to the United States, primarily settling in California and Texas. In 2020, they reached 2.3 million, becoming the fourth largest Asian subgroup in the United States (Rico et al., 2023). Many endured life-threatening conditions, war-time traumas, re-education camps, and harrowing migration journeys accompanied by physical and emotional torture. Many lost their professional positions, faced low socioeconomic status, and experienced linguistic barriers, with much of their health data unknown. This year marks the 50th anniversary of the fall of Saigon. Many are aged and may require health care assistance.
To fill this gap, we developed the Vietnamese Aging and Care Survey (VACS) and collected health data of older Vietnamese (≥65 years) in Houston, Texas in 2018 and 2021 (200+ surveys each). Although Houston is the second largest Vietnamese-populated metropolitan area in the United States (Pew Research Center, 2021), no health data on older Vietnamese-origin refugees and immigrants were available. The VACS data showed a high prevalence of physical (activities of daily living [ADLs], instrumental ADL), mental (depressive symptoms), and cognitive (dementia) disabilities (Miyawaki et al., 2020a, 2020b, 2022a, 2022b). The high prevalence of mild cognitive impairment (82%) and dementia (40%) was alarming. Because of their cultural belief that memory loss is part of aging, action to address cognitive issues of older family members was rarely taken, revealing low health literacy within the Vietnamese community (Miyawaki et al., 2024).
In cooperation with 14 Vietnamese key informants, we developed a linguistically and culturally tailored dementia one-pager (Miyawaki et al., 2024, Online Supplemental File) to improve the community’s health (dementia) literacy in 2022. In 2023, we formed the
Method
Study Design and Conceptual Framework
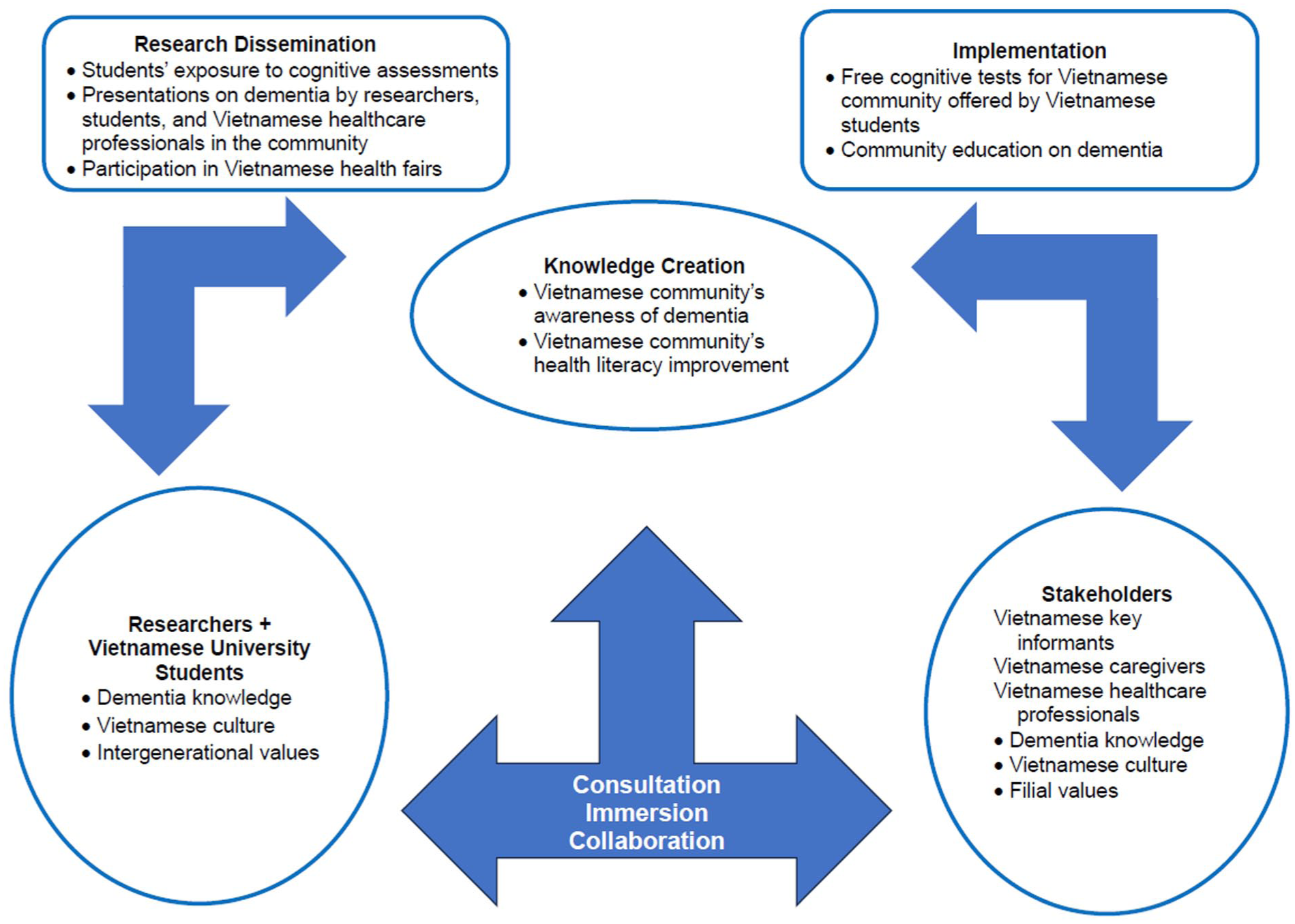
This article reports on the second year implementation stage of the Community-Engaged Dementia Education Program (CEDEP) one-pager (Miyawaki et al., 2024). We modified Haralambous et al.’s (2018) Cultural Exchange Model and tailored it to fit our new project, CHAIN. CHAIN is built on collaborative work between (a) Researchers/Vietnamese university students and (b) Vietnamese Community Stakeholders (Figure 1), aims to establish university–community partnerships, and improve dementia literacy of the Houston Vietnamese American community.
Modified Cultural Exchange Model
To implement the dementia one-pager and to initiate CHAIN, we recruited bilingual/bicultural Vietnamese students, taught them cognitive assessments, and offered memory tests to the Vietnamese community. Then, we distributed the dementia one-pager to Vietnamese physicians, nurses, and pharmacists and asked them to place it in their offices and discuss the importance of cognitive health with their patients during their visits.
Student Volunteer Recruitment
We recruited university student volunteers who were (a) bilingual/bicultural Vietnamese pre-health students; (b) could participate in a minimum of two health fairs per semester for one academic year; and (c) could complete training and maintain good standing in our team requirements. We recruited 20 students (Cohort 1) in the Spring 2023 semester and added nine students (Cohort 2) in Fall 2023. In Fall 2024, we recruited 15 (Cohort 3) students and in Spring 2025, 14 students (Cohort 4). Although students graduate every year, we aimed to maintain 29 to 30 students to cover the requests for our service in the community throughout the year.
Student Volunteer Training
We held training sessions following the orientation meetings for student volunteers and taught the Montreal Cognitive Assessment (MoCA) in English and Vietnamese (MoCA-V) (Appendix 2, Online Supplemental File). The Principal Investigator (PI) and her research assistants gave advice and evaluated each student’s assessment skills until they gained confidence performing the MoCA-V independently. When Cohort 2 students joined CHAIN (Fall 2023), we utilized Cohort 1 students’ help and formed a mentor (Cohort 1)–mentee (Cohort 2) relationship. Cohort 1 demonstrated the MoCA-V, whereas Cohort 2 observed their mentors perform. After several demonstrations, Cohort 2 tried the MoCA-V supervised by Cohort 1. They repeated this sequence until Cohort 2 felt comfortable with the MoCA-V solo performance. For the CHAIN second year (Spring and Fall 2024), Cohort 1 and 2 students became the mentors for Cohort 3 students. For this academic year (CHAIN third year, Spring 2025), Cohorts 1, 2, and 3 have been training Cohort 4 students. This builds teamwork, accountability, ethics, and responsibility to the community among the CHAIN team.
Cognitive Assessment
The MoCA assesses global cognitive function, including executive function, semantic memory, short-term delayed verbal memory, attention, language, abstraction, and spatial and temporal orientation with a score ranging from 0 (low) to 30 (high cognition). We set up a “memory booth” during health fairs, offered several tables with one student and one participant, obtained participants’ written consent, collected their demographic data, and conducted the MoCA in Vietnamese or English. After the test, participants received a copy of their results along with the dementia one-pager. The PI explained the results to participants individually and advised them to take the MoCA-V result and dementia one-pager to their next doctor’s appointment. This study was approved by the University of Houston (UH) Institutional Review Board (STUDY00004044). This article reports on all MoCA-V assessments that took place between the first and second year activities (April 2023 through November 2024).
Study Participants
Study participants were (a) 65 years and older, (b) community-dwelling, (c) Vietnamese, (d) could consent to the study by themselves, and (e) health fair participants. Some participants were younger than 65 years old; however, we kept them because we discovered their age after consenting to the study.
Data Analysis
We used descriptive statistics for participants’ demographic characteristics using SPSS version 30. The PI calculated the MoCA-V score, and students who conducted the assessments verified the score.
Results
Sample Characteristics
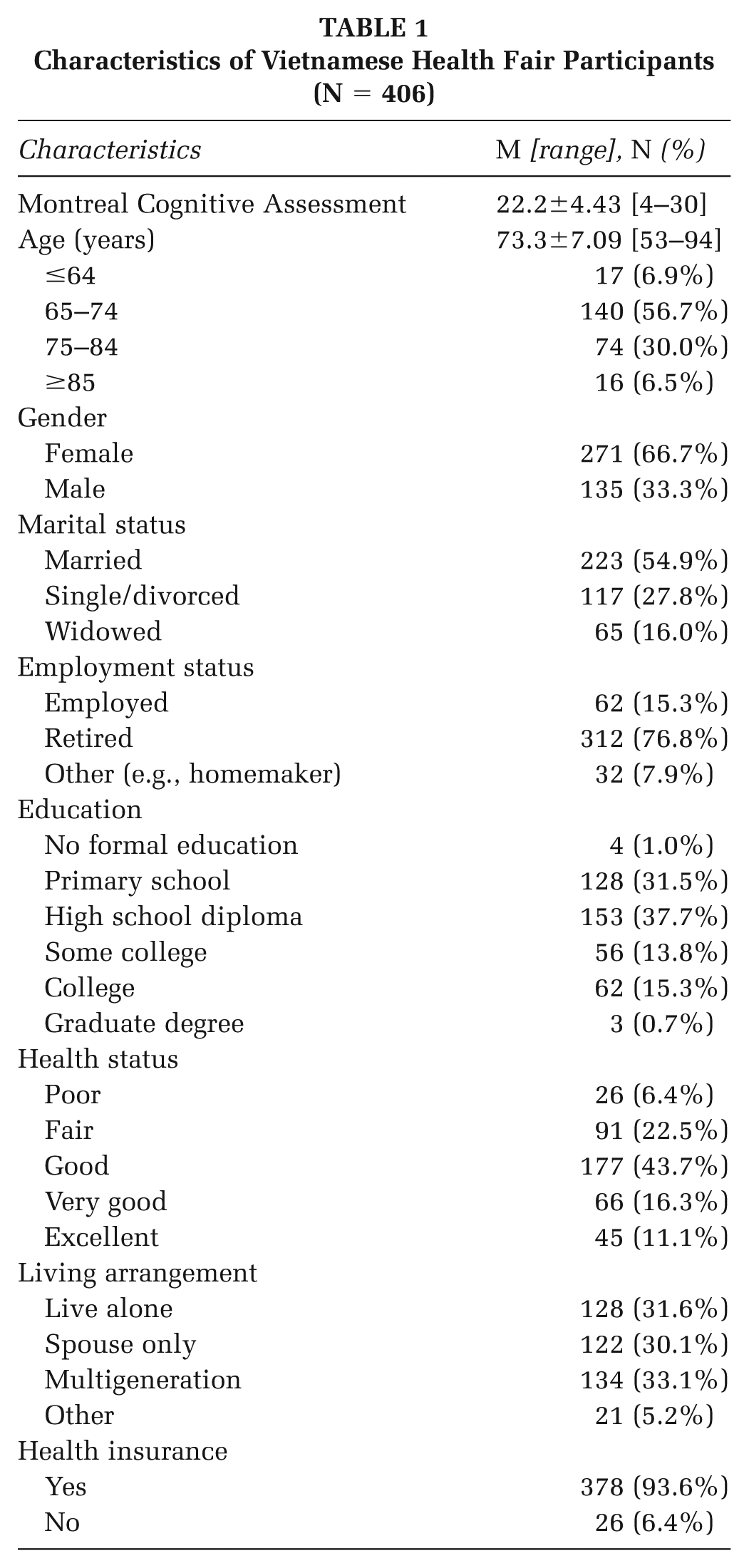
During the 2 years, we participated in 16 health fairs and assessed 406 Vietnamese participants (Table 1). Participants were 73 years old on average (age range: 53–94 years old). Many were married (55%), retired (77%), and female (67%) with between primary (32%) and high school (38%) education, and in good/very good/excellent self-reported health (70%). They lived alone (32%), with spouses only (30%), and in multi-generation households living with their adult children and grandchildren (33%). MoCA-V scores averaged 22.2 out of 30 (score range: 4–30).
Characteristics of Vietnamese Health Fair Participants (N = 406)
Discussion
The VACS revealed the high prevalence of physical, mental, and cognitive disabilities in older Vietnamese immigrants in Houston (Miyawaki et al., 2020a, 2020b; 2022a, 2022b). Based on the insights from 14 Vietnamese key informants, we (PI, her research team, and the Vietnamese community) developed a culturally and linguistically tailored dementia one-pager (Miyawaki et al., 2024). As the next step, the research team and bilingual/bicultural Vietnamese students started implementing the one-pager in 2023 in collaboration with Vietnamese health care professionals and community agencies, following the modified Cultural Exchange Model (Miyawaki et al., 2024), building the university–community partnerships. Our memory booth was overwhelmingly popular with long lines of participants waiting for their assessments. While in line, participants often shared their concerns with the students, such as their forgetfulness or having known someone who had dementia. During health fairs, other Vietnamese physicians, nurses, dentists, and pharmacists guided attendees to our memory booth to explore a new aspect of health. This sequence made a nice introduction to our “new” booth.
The Origin of the Houston Vietnamese American Community’s Partnerships
In 2000, the Vietnamese American Medical Association and the Vietnamese American Nurses Association were founded and started a Vietnamese local health fair, which expanded to become an annual event, attracting more than 600 Vietnamese families each year. Prior to CHAIN, Vietnamese optometry and pharmacy university students began volunteering, encouraged by the UH Vietnamese alumni health care professionals who were already involved. Therefore, the educational component of the fair is strongly emphasized. At the beginning of the health fair, all participants are to attend a lecture on a disease topic prior to receiving health care services.
Fostering Intergenerational Connections
The average MoCA score was 22.4 in the first year and 22.2 in the second year out of a score of 30, indicating the level of mild cognitive impairment by an education-adjusted threshold of ≥23 to be no sign of cognitive impairment (Quang et al., 2023). We held more health fairs in the second year to maintain outreach efforts. Having learned about the memory test, we expect to have more participants exploring the cognitive assessments in the third year. Some of our CHAIN students were their own or their peers’ grandchildren, which encouraged participation and excitement about the project. Older Vietnamese enjoyed observing their grandchildren or friends contributing to their community and forging intergenerational relationships.
Implications for Practice
Headed by Vietnamese health care professionals, the Houston Vietnamese American community has provided culturally and linguistically relevant health fairs to their older monolingual immigrants for the past 18 years. The sizes of health fairs vary from small fairs that serve a handful of participants to large fairs that attract hundreds. These fairs primarily address physical health, but for the past 2 years, CHAIN has joined and provided a new aspect of health care, cognitive health. For the Vietnamese community, this approach was new but piqued their interest, and thus, appeared to have benefited the participants. The students were able to engage with older adults in a real-world setting, enhance their Vietnamese communication skills, and reinforce proper cultural interactions. Volunteering was especially attractive for pre-health major students because they earned volunteer and clinical hours, as well as networking and internship opportunities, while working alongside Vietnamese health care professionals. Students found the experience personally enriching because CHAIN offered a chance to reconnect with their cultural roots, whether by rediscovering aspects of their identity that may have faded through assimilation or by exploring a heritage they had limited exposure to growing up. These opportunities also helped students strengthen their Vietnamese language skills and build deeper connections within the community. Furthermore, with the help of the PI, they participated in the university’s undergraduate research day and presented the results based on the collected data.
Although our project was conducted in Vietnamese, the training can be done in any of the other languages in which the MoCA has been translated and validated. When we served in the community, leaders of other racial and ethnic groups expressed interest and asked us to serve in their communities. However, any assessments, including the MoCA, are supposed to be conducted in the participants’ native languages. Our CHAIN students were limited to performing the MoCA in English and Vietnamese. With appropriate training, students who are fluent in other languages could adopt the same structure to conduct MoCA in ways that are culturally and linguistically appropriate for a broader range of communities. This practice of cognitive assessments in various languages can benefit not only the participants and their ethnic communities but also their health care professionals for exposure and preventive care.
The popularity of the memory booth was a pleasant surprise. However, we need to reduce the amount of time participants stand in line. First, we can recruit more volunteer students and train them to man more tables. Second, we can offer some age-appropriate educational games to entertain them while they are waiting. Third, we can offer other assessments such as the short physical performance battery (SPPB; Guralnik et al., 1994) for a change. The SPPB is an objective physical performance test that assesses the participant’s current physical functional status and predicts the risk of future adverse health events, including frailty, disability, cognitive impairment, and hospitalization. We could combine the data with the MoCA-V results and assess the participants from more angles to learn about their health.
Improving the community’s health literacy is a big goal and requires long-term commitment from all parties involved. This is the beginning of the university–community partnerships in collaboration with Vietnamese health care professionals. The Houston Vietnamese community has a long history of volunteer health care professionals, and the university is raising new generations of future health care professionals. The CHAIN program needs to continue this collaboration among researchers, university students, and health care professionals to serve a common goal of improving older Vietnamese immigrants’ health literacy.
Supplemental Material
sj-pdf-1-hpp-10.1177_15248399261419085 – Supplemental material for Improving Vietnamese Immigrants’ Cognitive Health Literacy Through University–Community Partnerships
Supplemental material, sj-pdf-1-hpp-10.1177_15248399261419085 for Improving Vietnamese Immigrants’ Cognitive Health Literacy Through University–Community Partnerships by Christina E. Miyawaki, Nguyen T. K. Nguyen, Tuong-Vi Ho, Angela McClellan, Jannette Diep and Thien-An Nguyen in Health Promotion Practice
Footnotes
Authors’ Note:
The authors appreciate the enthusiasm of the University of Houston undergraduate pre-health students. Without their efforts, flexibility, and willingness to accommodate the needs of participants, we could not offer cognitive assessments and complete the study. We appreciate all the participants who waited for a long time to take their memory tests. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Co-Curricular Learning Engagement, Office of the Provost at the University of Houston to CEM.
Ethics Approval Statement
This study was approved by the University of Houston Institutional Review Board (STUDY00004044).
Study Participant Consent Statement
Written consent was obtained from all participants before the assessments.
Data Availability Statement
Data is available from the first author upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.