
Abstract
Chronic diseases are prevalent in Canada’s aging population (≥65 years), which makes practicing positive health behaviors (e.g., physical activity and healthy diet) critical for the management of chronic diseases (e.g., stroke and heart disease). However, novel coronavirus (COVID-19) prevention strategies of quarantining, social isolation, and physical distancing may compromise one’s ability to manage health and engage in daily activities, possibly increasing the risk of adverse health events. The Community Outreach teleheAlth program for Covid education and Health promotion (COACH) program has demonstrated an increase in health-promoting behaviors, but little is known about participants’ experiences in participating in the program. The program entailed six telehealth sessions over 2 months that focused on health coaching, behavior change, and COVID education. This study aims to qualitatively describe older adult (≥65 years of age) participants’ experiences in the student-delivered COACH program. Twenty-four (n = 24) COACH participants were interviewed one-on-one in 30- to 45-minute audio-recorded, semi-structured interviews through Zoom videoconferencing. Interview recordings were transcribed verbatim and analyzed thematically. The sample’s mean age was 73.4 years (58% female) with 75% reporting two or more chronic conditions. Two major themes were identified that described participants’ experiences in COACH: (a) “Knowledge: Gaining New and Reinforcing Old” and (b) “Coach: Provider of Motivational Support.” COACH supported participants’ self-management knowledge, healthy behavior skills, and motivation during COVID-19. COACH acted as an external support strategy for chronic disease management and prevention practices during COVID-19, where student coaches provided motivation and knowledge to support self-management in older adult participants. (ClinicalTrials.gov ID: NCT04492527).
Keywords
Background
Aging populations experience an increased risk of developing chronic diseases (e.g., stroke, cardiovascular diseases, and diabetes), with over one third of older adults (≥65 years) in Canada (Government of Canada, 2021) and two thirds in the United States (Fong, 2019) reporting having two or more chronic diseases. As a result, demands on health systems related to sequelae of such chronic diseases and supporting older individuals in chronic disease management and prevention are increasing (Fong, 2019; Levine et al., 2019). Chronic disease self-management and prevention became especially apparent during the COVID-19 pandemic. Public health restrictions to reduce viral spread (i.e., quarantine, physical distancing, and closure of public facilities) also presented challenges to managing health behaviors, such as physical activity, eating healthy, and stress management (Darmon & Drewnowski, 2008; Diamond & Willan, 2020; Murphy et al., 2021; Park et al., 2022). Research indicates that social isolation and distancing have negative implications on mental health, stress, and anxiety, which in turn are associated with increased risk of heart disease and stroke onset (Darmon & Drewnowski, 2008; Lebrasseur et al., 2021; Mellor & Rehr, 2005; Murphy et al., 2021). Furthermore, closures of public areas affect exercise and dietary quality by limiting the options of when and where people may obtain physical activity, leave their homes, and access health care needs (Beltrán-Sánchez et al., 2015; Henning-Smith, 2020; Lebrasseur et al., 2021; Wister, 2005). Those at high risk of COVID-19 with poor outcomes are older adults and those with existing chronic diseases, relative to younger individuals and those without disease or disability (Beltrán-Sánchez et al., 2015; Shahid et al., 2020; Wister, 2005). Overall, support is required for older adults’ management and prevention of chronic diseases during public health situations that require physical distancing.
In response, we developed the student-delivered Community Outreach telehealth program for COVID-19 education and Health promotion (COACH). COACH is a 2-month program in which participants (aged ≥65 years) receive six 30- to 45-minute virtual health coaching sessions from a trained medical student, delivered using videoconferencing technologies (Yang et al., 2023). The primary foci are to (a) empower older adults to better manage health behaviors (e.g., physical activity, diet, sleep) as a means for chronic disease prevention and management during COVID-19; and (b) provide education and updates about COVID-19 (Yang et al., 2023). In COACH, participants self-identified important health-related behaviors for improvement and worked collaboratively with their student coach to develop action plans to reach their health-related goals (Yang et al., 2023). Participants completed six sessions of the COACH program, where they were paired with trained student coaches. These coaches were medical students from the University of British Columbia’s (UBC) medical doctor (MD) program. They were trained in areas of chronic disease management and prevention, motivational interviewing and brief action planning in preparation for leading the coaching sessions. During program sessions, coaches empowered and supported participants through education and motivation to self-manage their behaviors, while adhering to COVID-19 prevention guidelines (Yang et al., 2023). A “Healthy Living” booklet was also provided to participants that contained supplementary reading material on chronic disease management and prevention strategies and COVID-19 prevention (Yang et al., 2023).
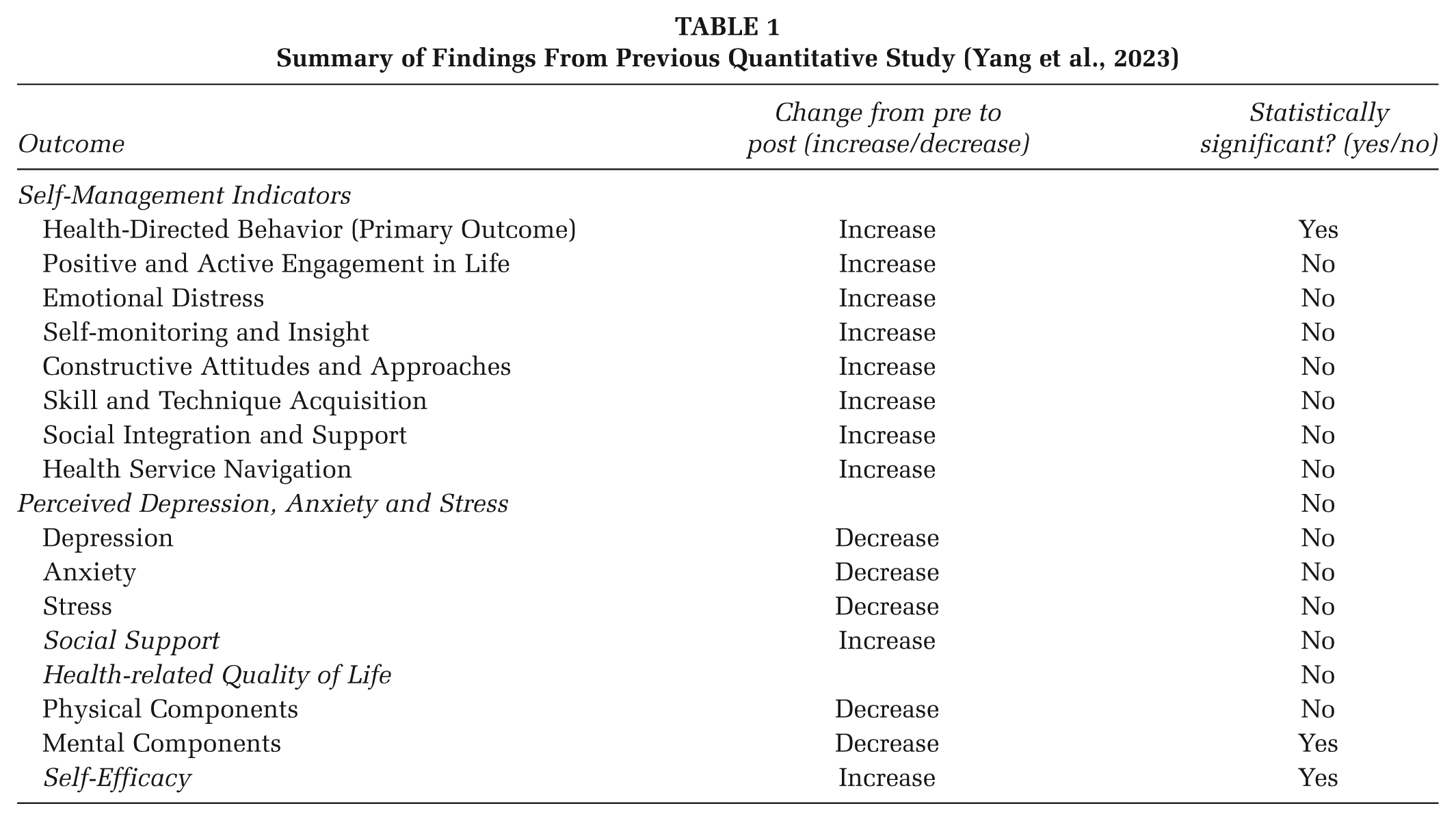
COACH was previously evaluated using a single group, pre–post quantitative study design (Yang et al., 2023). The primary objective of the previous evaluation was to evaluate the program’s effects on health-directed behavior (i.e., a self-management domain) on older adults (Yang et al., 2023). Secondary objectives included evaluating the program’s effects on perceived depression, anxiety, and stress; social support; health-related quality of life; health promotion self-efficacy; and other self-management domains (Yang et al., 2023). Results (n = 75) indicated statistically significant increases in health-directed behavior and self-efficacy, and statistically significant decreases in mental health (Yang et al., 2023; Table 1). These findings suggested that COACH was able to improve self-management behaviors and health promotion self-efficacy, despite diminishing mental health arising due to COVID-19 requirements for physical distancing, quarantining, and social isolation (Yang et al., 2023). However, the subjective program experience of participants was not described.
Summary of Findings From Previous Quantitative Study (Yang et al., 2023)
Objective
In this qualitative descriptive study, we aimed to develop an understanding of older adult (≥65 years) experiences participating in COACH (Sandelowski, 2000, 2010; Yang et al., 2023). The COREQ (COnsolidated criteria for REporting Qualitative research) was used to ensure comprehensive reporting of methodologies and findings (Tong et al., 2007; Supplementary Material 1). Ethical approval was obtained from UBC’s Behavioral Research Ethics Board (H20-01368).
Method
Participants
Participants in the larger quantitative investigation of COACH: (a) were 65 years or older, (b) had access to a telephone or videoconferencing program, and (c) had no previous COVID-19 diagnosis by health professionals. Individuals were excluded if they (a) were not medically stable (e.g., symptoms/conditions not being treated), (b) were participating in another health promotion program, and/or (c) had severe hearing loss that could not be corrected with a hearing aid (Yang et al., 2023). All participants in the larger sample (n = 75) of convenience were eligible to participate in this qualitative study, where we used stratified purposive sampling to ensure representation of both male and female sexes, and individuals residing in different geographical locations (e.g., urban, rural/suburban; Mathew et al., 2012; Palinkas et al., 2015; Sav et al., 2015; Suri, 2011). Participants were recruited until the research team determined that data sufficiency had been reached (Francis et al., 2010; Vasileiou et al., 2018). In total, 24 community-dwelling individuals were recruited with no dropouts or refusals.
Data Collection
Two weeks after completing quantitative data collection, participants were scheduled for a 30- to 45-minute semi-structured interview via Zoom videoconferencing. Interviews were conducted on a one-on-one basis by the primary author. The interviewer had no personal relationships with any of the participants. At the time of data collection, the interviewer was a 24-year-old rehabilitation sciences graduate student who had the privilege of receiving the training and education to prepare for their role as an interviewer and researcher for this project. The primary author was previously trained by the principal investigator and their lab research coordinator to conduct the interviews. Open-ended questions and probing were used during interviews to limit both subjectivity and bias that may arise from the interviewer’s experience researching this field. This was so that both positive and negative comments were obtained during interviews.
Interviews were conducted using an open-ended semi-structured interview guide developed by the primary author and principal investigator. The interview guide consisted of questions related to COACH (e.g., relationship with student coaches, using COACH resources, etc.). The interview guide was further refined throughout the data collection process to include any emerging topics. Interviews were audio-recorded using Zoom videoconferencing recording options, and supplementary field notes were written throughout the interview process.
Analysis
We conducted a codebook thematic analysis to create straightforward interpretations for our evaluation (Braun & Clarke, 2021). This analysis adapts an iterative process alongside a structured coding approach (Braun & Clarke, 2021). Analysis was broken up into three steps: (a) transcribing and initial reading, (b) coding, and (c) theme development. The first two steps of analysis were conducted by the primary author and a research assistant. The research assistant was an undergraduate student with a background in psychology and an interest in topics of chronic care, telehealth, and self-management.
During the first step, the primary author transcribed interview audio-recordings verbatim. Transcripts were read multiple times in detail to increase validity (Nowell et al., 2017). Reflexivity denotes the process of examining one’s own beliefs, judgments and practices during the research process. To monitor the interviewer’s positions, values, beliefs or biases that may have influenced the interpretation of data, documentation of theoretical and reflective thoughts was recorded into notes during each analysis process (Koch, 1994). This also supported the qualitative analysis process of data immersion that led to deeper understanding of the data (Braun & Clarke, 2021; Koch, 1994). All records of raw data, field notes, and transcripts were kept for researchers to clearly systemize, relate, and cross-reference data (Halpren, 1983).
After transcribing, the same two researchers began to identify, categorize, and sort important sections of text into codes using NVivo-12 (Braun & Clarke, 2021). Codes were not drawn from pre-existing ideas developed prior to analysis. The same five transcripts were initially coded by both researchers independently, after which the researchers met to discuss and establish any similar thoughts and findings. A coding guide was developed and subsequently modified throughout the coding process of other interviews when additional key elements were identified in the data. The remaining transcripts were then divided and coded separately by the two researchers. Regular meetings were held to continue discussion of findings throughout the analysis. Any discrepancies that arose between findings from the primary author and the research assistant were reconciled by the second author. They were a third year MD student at the time of the study with previous experience in delivering coaching interventions using skills in chronic disease management and prevention, motivational interviewing and brief action planning.
Finally, codes were sorted into themes through a collaborative process with the primary author, research assistant, and the principal investigator. By the end of analysis, themes that brought meaning and identity to a recurrent experience and posed as relevant to the research objectives were created, named, and defined (Braun & Clarke, 2006; DeSantis & Ugarriza, 2000). Participants were also emailed a one-page summary of the findings and requested to comment or clarify any thoughts. There were no significant edits made on our findings based upon the participants’ feedback.
Findings
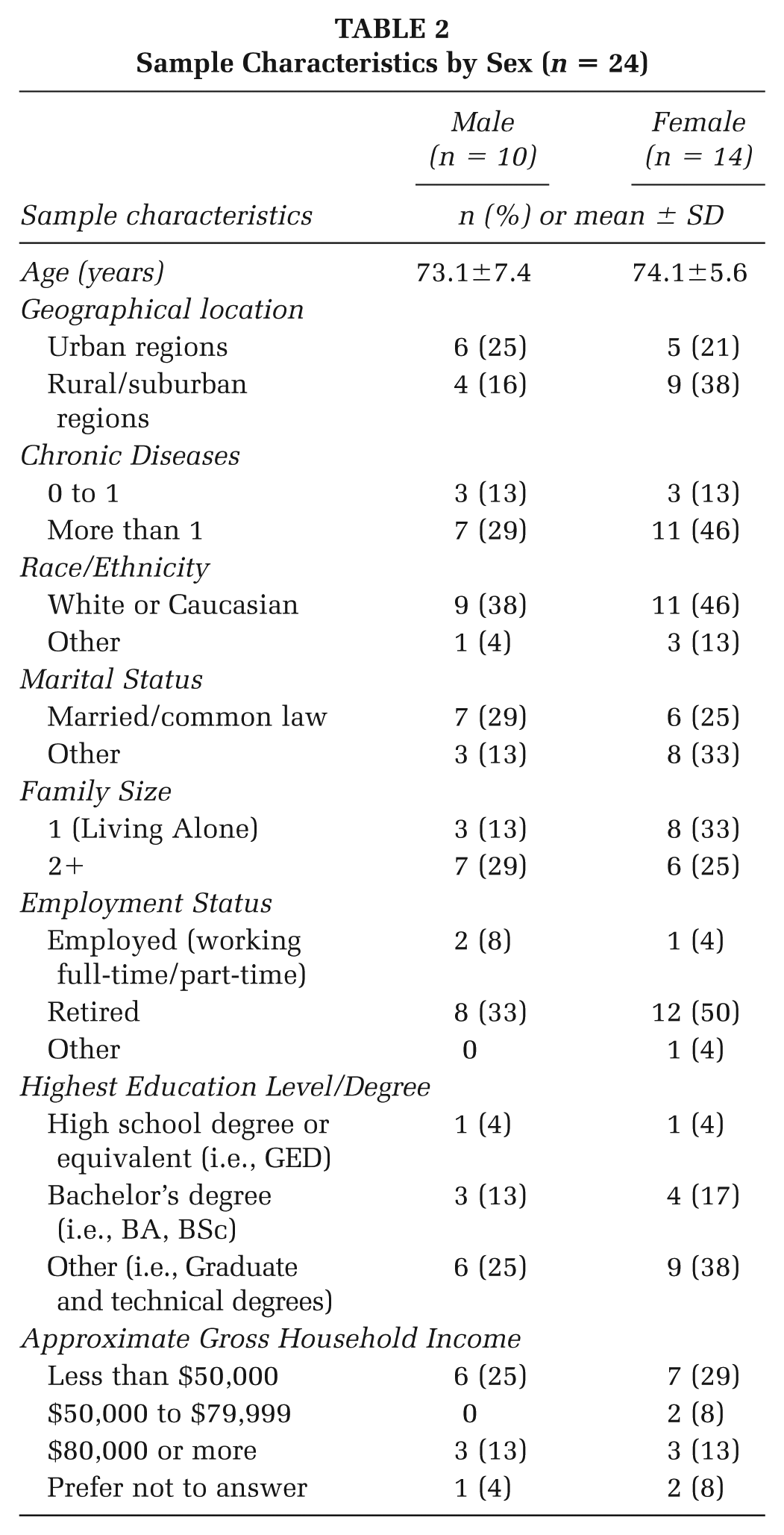
Ten male (mean [SD] age: 73.1 [7.4] years) and 14 female participants (mean [SD] age: 74.1 [5.6] years) participated in this study. Among the total sample, 20 (83.3%) of them identified as Caucasian. No participants were diagnosed with COVID-19 during participation in the larger quantitative study or this qualitative study. Table 2 further details the sample characteristics.
Sample Characteristics by Sex (n = 24)
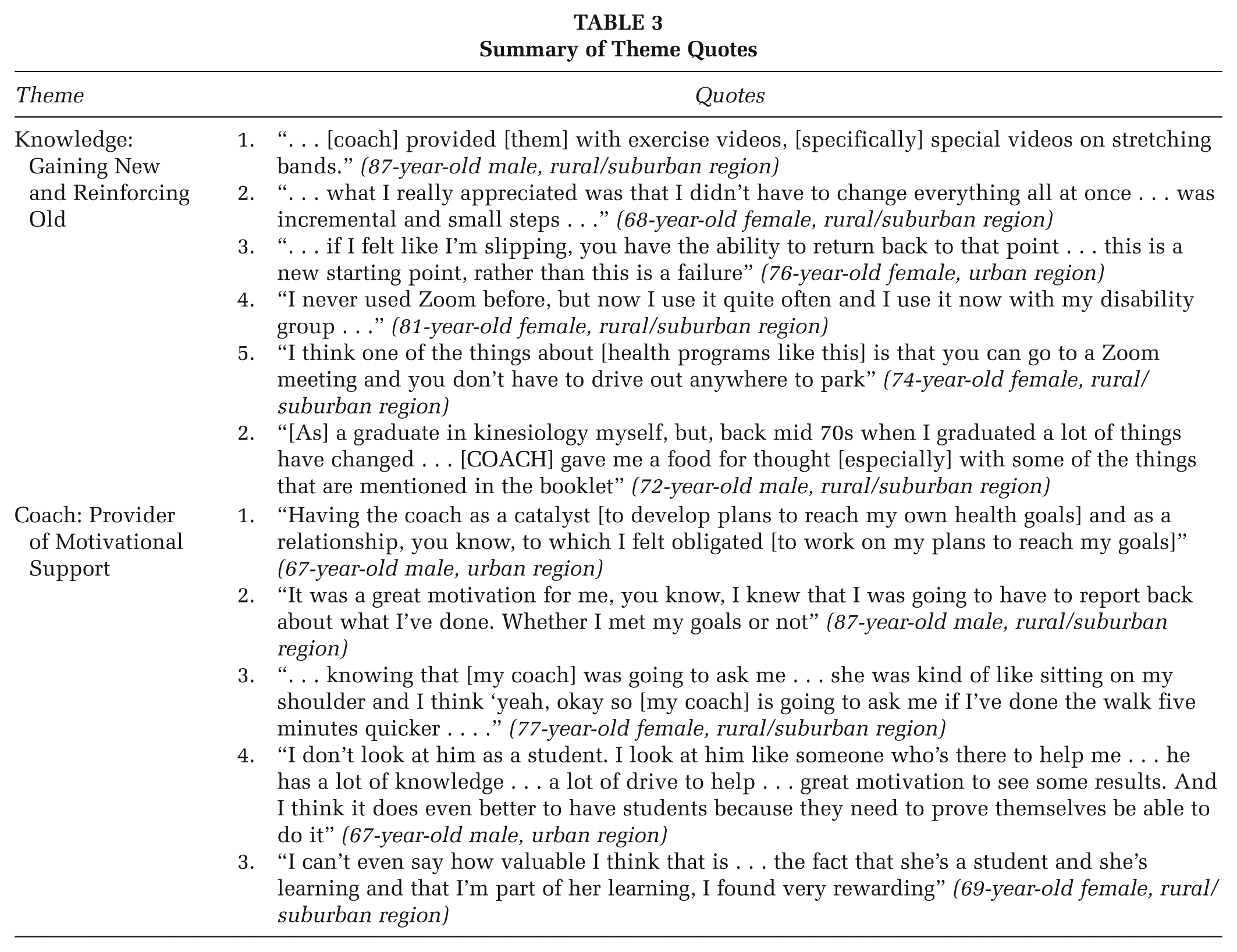
Overall, participants reported the program as being supportive of their adherence to practicing positive strategies for chronic disease management and prevention during COVID-19. Two themes were identified: “Knowledge: Gaining New and Reinforcing Old”; and “Coach: Provider of Motivational Support.” Details about each theme are described below and summarized in Table 3.
Summary of Theme Quotes
Knowledge: Gaining New and Reinforcing Old
Participants discussed both the development of new knowledge and the reinforcement of their existing knowledge related to their chronic disease management and prevention efforts. New knowledge was gained through interactions with their student coach, where the coach provided information to help reach their desired health goals. Participants described how their coach was a helpful resource when learning new self-management techniques or strategies. For example, new techniques or resources participants obtained from their coaches included online exercise videos, local online social groups (e.g., for mental health/social support), and learning behavior change strategies, such as action planning and modifying their environment to be more supportive of their health behavior goals (e.g., having a full, large-sized water bottle next to them as a reminder to drink water). An 87-year-old male from a rural/suburban region expressed how their coach “. . .provided [them] with exercise videos, [specifically] special videos on stretching bands.”
Participants also discussed learning about different self-management skills, such as goal setting, action planning, and changing their perspectives for accomplishing goals. A 68-year-old female from a rural/suburban region reported focusing on creating smaller, attainable action plans to better reach their longer-term health goals “. . .what I really appreciated was that I didn’t have to change everything all at once . . . was incremental and small steps . . .” In addition, other participants reported learning new strategies to cope with the lack of success in realizing their health goals. For example, one 76-year-old female participant from an urban region reported realizing that if they did not accomplish their goal 1 day, it is not a failure; rather, the next day can be a new starting point: “. . .if I felt like I’m slipping, you have the ability to return back to that point . . . this is a new starting point, rather than this is a failure.” Thus, findings expressed how COACH allowed participants to change the way they set health goals and shift participants’ outlook on goal accomplishments and failures to better support their chronic disease management and prevention practices.
Gaining new knowledge about the use of technology to deliver health-related services like COACH was also a common topic discussed about during interviews. One 81-year-old female participant from a rural/suburban region discussed learning how to use videoconferencing technology through the program: “I never used Zoom before, but now I use it quite often and I use it now with my disability group . . .” By the end of COACH, some participants commented on how they learned to see the benefits of using technology to get health-related support. In particular, a 74-year-old female from a rural/suburban region commented the following: “I think one of the things about [health programs like this] is that you can go to a Zoom meeting and you don’t have to drive out anywhere to park.”
In terms of reinforcing existing knowledge, participants found value in COACH reinforcing existing knowledge about chronic disease management and prevention strategies. In this case, COACH helped to validate participants’ perspectives. For example, participants commented about how some of the suggested chronic disease management and prevention strategies in the “Healthy Living” booklets were not new to them. However, they still appreciated having the resources to remind them of the information and to refer to when needed. Particularly, one 72-year-old male participant from a rural/suburban region expressed how information obtained from COACH gave him an opportunity to reinforce and build upon old knowledge they gained as a kinesiology graduate: “[As] a graduate in kinesiology myself, but, back mid 70s when I graduated a lot of things have changed . . . [COACH] gave me a food for thought [especially] with some of the things that are mentioned in the booklet.” COACH served as a valuable program for participants’ own knowledge about chronic disease management, whether it pertained to gaining new information or furthering knowledge that participants already had.
Coach: Provider of Motivational Support
In COACH, participants were paired with a trained student coach with whom they collaborated to manage their health and well-being in the context of COVID-19 restrictions. Motivational support was reported as a key element that participants appreciated from their coach. Participants discussed how coaches provided motivation by holding them accountable. For example, participants discussed about how coaches collaboratively developed health behavior action plans of which participants could work between coaching sessions: “Having the coach as a catalyst [to develop plans to reach my own health goals] and as a relationship, you know, to which I felt obligated [to work on my plans to reach my goals]” (67-year-old male, urban region). The coaches would then follow up with participants on how successful they were at following their action plans in subsequent sessions: “It was a great motivation for me, you know, I knew that I was going to have to report back about what I’ve done. Whether I met my goals or not.” (87-year-old male, rural/suburban region). One 77-year-old female participant from rural/suburban regions reported thinking of their student coach while attempting to practice their COACH plans to reach their health goals in between their scheduled coaching sessions: “. . .knowing that [my coach] was going to ask me . . . she was kind of like sitting on my shoulder and I think ‘yeah, okay so [my coach] is going to ask me if I’ve done the walk five minutes quicker . . . .” Thus, participants expressed feeling a sense of accountability to work on their action plans and report back on progress.
When asked about having a medical student (as opposed to a licensed health professional) as their coach, participants described the value in getting health promotion information from a student. Participants reported their assigned student coach as being a knowledgeable source with a lot of motivation to perform their best as student coaches: “I don’t look at him as a student. I look at him like someone who’s there to help me . . . he has a lot of knowledge . . . a lot of drive to help . . . great motivation to see some results. And I think it does even better to have students because they need to prove themselves be able to do it” (67-year-old male, urban region). Participants noted how they were aware that their coaches were limited in the medical advice they could share. However, many expressed seeing the value in working with students for both their own health development, as well as students’ own professional learning and development: “I can’t even say how valuable I think that is . . . the fact that she’s a student and she’s learning and that I’m part of her learning, I found very rewarding” (69-year-old female, rural/suburban region). Many participants reported on how interacting with medical student coaches was beneficial for both developing their own knowledge of health and helping the students with their own experiential learning. Overall, participants reported positive interactions with their coaches, as the coach’s knowledge and desire to help motivated participants to want to achieve their health goals.
Discussion
In this study, we qualitatively investigated the experiences of 24 older adults participating in COACH. COACH was a chronic disease management and prevention support program delivered by medical undergraduate students to help individuals manage their health and wellness during COVID-19. Our analyses revealed two overarching themes revolving around knowledge of health management and motivation to act.
“Knowledge: Gaining New and Reinforcing Old” summarized participants’ development of knowledge and reinforcing existing beliefs during COACH. Much of the knowledge highlighted by participants is aligned with existing literature reporting on self-management support strategies (Lorig & Holman, 2003; Rotheram-Borus et al., 2012). Decision-making and goal setting, resource utilization, formation of a patient/provider partnership, and action planning are common evidence-based self-management support strategies used in chronic disease prevention and management interventions (Lorig & Holman, 2003; Rotheram-Borus et al., 2012); these strategies were also used in the program sessions. Generally, individuals need to make decisions in response to ongoing changes to their health (Lorig & Holman, 2003). To support the decision-making process, people may seek external resources to develop further knowledge on how to respond to ongoing changes (Lorig & Holman, 2003). In COACH, the program sessions, program materials, and student coaches all helped to support and guide participants in making their own decisions to manage their health. These may have come as new resources to utilize (e.g., exercise videos and COACH’s Health Living booklet) or new perspectives on how to approach practicing self-management (e.g., creating smaller and attainable goals). Some participants also commented about learning how to use Zoom videoconferencing and how it benefited their experience receiving self-management support. This contributes to growing telehealth literature that emphasizes how technology use can have potential to strengthen and improve health-related services such as health coaching (Bouabida et al., 2022). Overall, COACH gave participants the opportunity to obtain resources to support knowledge of overall health, self-management, and technology, which all contributed to their efforts to practice self-management strategies at home.
Participants reported that motivational support provided by coaches was important in their chronic disease self-management and prevention efforts. Motivation has been previously identified as a key construct to drive individuals to effectively practice chronic disease self-management (Hadi et al., 2020). Different types and levels of motivation can affect an individual’s ability to self-manage their health (Hadi et al., 2020). Some motivators can come in the form of individuals obtaining aid from people in their social circles, which creates opportunities to increase individuals’ will to grow and reach any of their personal behavior goals (i.e., motivational social support; Feeney & Collins, 2015). Strong social support networks tend to be associated with increased health and wellness in previous literature; similarly, lower levels of social activity are implicated in lower perceived health among older adults with chronic disease (Garnett et al., 2018). Similarly, our findings highlight how motivational support from coaches gave participants confidence to pursue behavior changes. These align with previous findings that show student-led interventions have overall satisfaction and comparable results to professional-led interventions (Suen et al., 2020). They also align with exit satisfaction survey responses we reported in our previous preliminary evaluations; participants reported overall positive opinions about their assigned student coach (Yang et al., 2023). Many participants expanded upon these responses during these qualitative interviews by highlighting their coaches’ abilities to connect with participants. Coaches created a positive environment for participants to gain the willingness to practice self-management to reach their health goals. Thus, having this positive and supportive coach-participant relationship allowed participants to feel more motivated to reach their health goals.
Limitations
There are several limitations to this study. First, social desirability bias is possible due to participants’ knowing that their responses were being audio-recorded and the interviewer’s presence. Second, while perspectives that we gathered are reflective of the older adult COACH participants, we cannot guarantee that these experiences reflect what the entire older adult population experienced before and during COVID-19. Much of our findings also focuses on areas of health behavior change regarding chronic disease management and prevention. Self-selection bias is also possible due to participants originally having been part of COACH via voluntary participation. Participants selected for this qualitative evaluation were from a convenience sample that all willingly chose to participate in the original quantitative study. These limit the transferability of findings, biasing toward people who may be more motivated or active in practicing chronic disease management and prevention. The majority of the sample for this qualitative study was also predominantly Caucasian (83.3%), which also limits the transferability of findings. Further research may investigate how similar interventions can be best transferred to a broader population of older adults with chronic diseases and target other domains of chronic disease management and prevention. Finally, findings suggest that the sample group may have mostly focused on sharing more positive comments about the program. Similar future studies should consider how to best obtain representation of both positive and negative comments about similar future programs.
Implications for Practice
Our findings suggest that the student-run COACH program can effectively provide older adults with knowledge and motivation for chronic disease management and prevention. Particularly, our findings indicate that motivational support can be a strong component of active health management. The use of students and technology represents a low-cost, accessible, and sustainable strategy for the delivery of chronic disease management and prevention support programs.
Implications for Research
Future research could explore how interventions like COACH can be adapted to support a broader range of older adults. Specifically, further work is needed to understand how such programs can address the needs of diverse ethnic backgrounds and aspects of chronic disease management and prevention not captured in this study. Future studies could also consider how to obtain a wider range of participant perspectives (i.e., both positive and negative intervention feedback) to better inform program refinement. These efforts, combined with our findings, may lead to better insights into how to better support older adults in the ongoing management of their health.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399251414647 – Supplemental material for Qualitative Experiences of Older Adults Participating in a Student-Delivered Community Outreach TeleheAlth Program for COVID Education and Health Promotion
Supplemental material, sj-docx-1-hpp-10.1177_15248399251414647 for Qualitative Experiences of Older Adults Participating in a Student-Delivered Community Outreach TeleheAlth Program for COVID Education and Health Promotion by Michelle C. Yang, Cam Clayton, Devin Harris, Chelsea Pelletier, Julia Schmidt, Jill G. Zwicker and Brodie M. Sakakibara in Health Promotion Practice
Footnotes
Authors’ Note:
We acknowledge the following students from University of British Columbia’s Doctor of Medicine (MD) program for dedicating their time and efforts to delivering the intervention presented in this study: Annie Walters-Shumka, Alicia Liang, Caroline Guinard, Chris Lanz, Hanna Ellis, Imelda Suen, Jaspirit Nijjar, Jenny Zhang, Keegan Marchand, Lauren Hughes, Mariam Manna, Martin Cheung, Megan Chan, Mirna Hennawy, Robert McDermit, Stellar Lim, Tomas Rapaport, Vanessa Wildeman, and Valeriya Zaborska. We also acknowledge the Centre for Collaboration, Motivation, and Innovation for their contribution to the coaches’ training. This study was approved by the Behavioural Research Ethics Board (H20-01368) at the University of British Columbia (UBC). This study was not preregistered. The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Interior Universities Research Coalition (IURC) for BC Interior Region Seed Grant Health Research Fund, the Michael Smith Foundation for Health Research Scholar Award (to BMS and JS), and the Canada Research Chair (Tier 2) in Pediatric Brain Development and Rehabilitation (to JGZ).
Ethical Approval
Ethical approval was obtained from the University of British Columbia’s Behavioral Research Ethics Board (H20-01368).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.