
Abstract
Offering group-based sexual health education online can expand access to information for youth. However, few studies have examined how student perceptions and outcomes may vary by teaching modality, particularly in sexual health education. This study compared the perceptions and short-term outcomes of participants completing In the Know, a comprehensive sexual health curriculum, in-person versus online. A total of 528 youth aged 13–19 were recruited through schools and community-based organizations in Fresno County, California. In-person participants (n = 359) were enrolled from December 2018 to February 2020 and online participants (n = 169) from August 2020 to August 2021, during the COVID-19 pandemic. We surveyed all participants at program entry and exit to measure changes in sexual health knowledge, attitudes, confidence in life skills, and program perceptions, which we compared between in-person and online participants. In-person and online participants had similar age and racial/ethnic characteristics, but online participants were less likely to live in rural areas or in settings such as group homes. Participants in both delivery modes showed statistically significant improvements in their sexual health knowledge and attitudes as well as life skills confidence. More than 80% participants were interested in the material and felt it was clear, regardless of delivery mode. With sufficient planning and health educator training, online sexual health education can be a feasible and appropriate alternative to in-person programming. When considering online implementation, programs should adopt approaches to minimize inequities in participation, maintain participant confidentiality, and promote engagement.
Sexual and reproductive health (SRH) interventions increasingly use technology to expand access to services and information. Research has shown these interventions can improve youth sexual health outcomes, including condom use, abstinence, and reproductive health knowledge (Wadham et al., 2019; Widman et al., 2018). One systematic review found that 75% of digital adolescent sexual health interventions led to positive sexual health behavior and cognitive changes (Sewak et al., 2023). However, most of these interventions were implemented individually and did not include group-based or synchronous components. Fewer interventions have been developed and tested offering online implementation of group-based SRH education (Faccio et al., 2023; Guilamo-Ramos et al., 2015; Patel et al., 2022). While these studies demonstrated the feasibility and acceptability of online SRH education for youth and educators, they did not assess changes in knowledge or other outcomes. Some studies of blended learning—combining asynchronous online education with in-person sessions—have shown increased sexual health knowledge and safer sex behaviors, but evidence on effectiveness remains inconclusive (Coyle et al., 2019).
The COVID-19 pandemic prompted a sudden, large-scale transition to online learning for most schools. In the United States, 93% of households with school-aged children engaged in online learning during the pandemic’s first year (McElrath, 2020). Since that time, online learning has remained above prepandemic levels, with the U.S. e-learning market projected to grow by US$56.44 billion between 2023 and 2028 (ConsumerAffairs, 2025). Enrollment in K–12 virtual schools also increased by more than 350,000 students between 2013 to 2014 and 2022 to 2023, reflecting the ongoing growth in online education beyond the pandemic (ConsumerAffairs, 2025).
Online education has the potential to expand access to information in rural and low-resource settings, reach populations that may face barriers to in-person education, provide more scheduling and administrative flexibility, and reduce the costs associated with in-person instruction, among other benefits. Given that many adolescents do not receive comprehensive sex education in school or other community settings (Lindberg et al., 2022), online education may offer an alternative to help fill gaps left by limited in-person instruction.
While extensive research has documented positive outcomes for online education at the university level, studies comparing the impact of in-person versus online education at the K–12 level remain limited (Barbour, 2019; Martin et al., 2022). Within the United States, recent studies have found more positive academic and socioemotional outcomes for in-person compared with online teaching. One national survey found most adolescents preferred in-person learning, and a third felt less connected to classmates and teachers while learning online (Anderson et al., 2022). Other studies reported higher academic achievement, greater connection to classmates and teachers, and greater social and emotional well-being for in-person students compared with online students (Duckworth et al., 2021; McKellar & Wang, 2023).
Few studies have compared in-person and online sexual health education. Three small qualitative studies examined the challenges of online sexual health education implementation, all from the health educators’ perspective (Cahalan & Carpenter, 2023; Rolleri Insignares et al., 2021; Scriver, 2023). Key considerations for the health educators included the importance of youth comfort and supporting their ability to participate fully. One evaluation of a sexual health program adapted for virtual delivery found lower attendance and greater recruitment challenges than in-person implementation, although facilitator quality and student satisfaction remained high (Faccio et al., 2023). Online formats may reduce embarrassment by allowing anonymous questions (Pound et al., 2016), but they can also increase discomfort if home environments lack safety or privacy (Lindberg et al., 2020; Rolleri Insignares et al., 2021).
The COVID-19 pandemic provided a natural experiment to compare the implementation and effects of a sexual education curriculum, In the Know (ITK), by delivery mode. The program shifted from in-person to fully online implementation after the March 2020 shelter-in-place order. This study compares participants’ perceptions and short-term outcomes—including sexual health knowledge, attitudes, and confidence in life skills and activities—by delivery, providing new insights into the effectiveness and acceptability of group-based online sexual health programming.
Methods
Intervention Overview
ITK was originally designed as an in-person sexual health education program that integrated digital technology to improve the sexual health and overall well-being of adolescents in Fresno County, California (Yarger et al., 2024). ITK was specifically developed for adolescents ages 13–19 who were underserved by existing programming including unstably housed youth, youth of color, and LGBTQ+ youth. Using a youth-centered design process (Fakoya et al., 2022), a group of adolescents representing priority populations participated in workshops with the design team to co-develop content, design a mobile app, create rapid prototypes, and provide feedback on multiple design and content iterations.
The curriculum had three modules: (1) sexual health and contraceptive use, (2) healthy relationships, and (3) educational and career success. Each module lasted approximately 2 hours and was taught by trained health educators in a group setting. In addition, participants could download the app on their phones to use during and outside of the sessions. The app included digital activities and resources that reinforced key information presented in the group instruction, including videos, quizzes, articles, a goal-setting activity, and a resource for local services with geo-location features.
Conceptual Framework
ITK was developed using a positive youth development framework that cultivates adolescent assets for reaching their full potential (Damon, 2004). Positive youth development is empirically supported in improving health outcomes and reducing youth susceptibility to engage in risky behaviors by promoting personal strengths and healthy development through supportive opportunities and experiences (Gavin et al., 2010). Examples of this approach within ITK include promoting healthy relationships, building skills to obtain jobs and educational opportunities, and providing a platform for goal setting. This approach parallels constructivist learning theory, which emphasizes the importance of a learner-centered approach as well as a collaborative environment. Constructivism and advances in technology provide new opportunities for creating supportive learning environments both online and in person (Tam, 2000).
Program Modifications for Online Delivery
The project team spent 2 months updating and adapting the curriculum for fully online implementation. While the content of the modules remained the same, several modifications were made.
Engagement Strategies
Some activities, such as discussions and role plays, were modified to engage participants in an online format. Activities were modified to use the digital interactive message board Jamboard, Zoom annotations, Zoom polls, and group chat features. The team prioritized flexibility to accommodate various online learning platforms and the technology available in participants’ homes.
Asynchronous Learning
To limit the time spent as a group online and “Zoom fatigue,” several activities were modified for asynchronous completion. This included activities and mini-lessons completed before or after synchronous sessions. For example, health educators prerecorded videos for participants to watch beforehand and discuss during the live sessions.
Privacy and Confidentiality
Strategies were implemented to maintain privacy and online confidentiality. Only registered participants and authorized staff with unique assigned usernames and passwords could join the meeting. A digital whiteboard was used for sharing ideas anonymously, while private chatting in Zoom was limited to messaging hosts.
Health Educator Roles and Responsibilities
To successfully handle these changes, health educator roles and responsibilities were restructured. Two health educators were assigned to each online cohort regardless of size, with one health educator responsible for providing curriculum instruction, while the other managed the technology, such as breakout rooms and links, and responded to chat messages.
Setting
ITK was implemented in partnership with local schools, afterschool programs, community-based organizations, and shelters throughout Fresno County, California. In-person sessions were conducted at partner sites, while participants receiving the intervention online typically joined sessions from their homes.
Participants
We recruited participants from youth-serving sites throughout Fresno County between December 2018 and August 2021 (N = 528). Individuals were eligible if they were 13 to 19 years, English- or Spanish-speaking, and living within Fresno County. In-person participants (n = 359) were enrolled between December 2018 and February 2020 across 34 cohorts as part of a larger randomized control study (Yarger et al., 2024). We enrolled 12 cohorts of online participants (n = 169) between August 2020 and August 2021.
Data Collection
The institutional review board of the University of California, San Francisco approved the study protocol (#17-22381). Following state guidelines for sexual health education, passive parental or guardian consent was used, meaning parents or guardians needed to sign and return a consent form for refusal. Participants completed a consent/assent form at recruitment.
Participants completed an entry survey before the program and an exit survey immediately upon completion via Qualtrics. In-person participants had the option of completing surveys on paper if needed. Health educators administered entry surveys, while the evaluation team sent participants a link to the exit survey via email or text message.
Measures
The surveys assessed program perceptions, sexual health knowledge and attitudes, confidence in life skills, and participant characteristics. Measures were selected based on federal grant requirements or developed in alignment with the learning objectives and delivery format of the intervention.
Program Perceptions
We assessed participants’ perceptions of the program, including their level of interest in program sessions, clarity of the material presented, helpfulness of activities and discussions for learning, sense of personal respect, and opportunities to ask questions, using a 5-point Likert-type scale at program exit. Responses to perception questions were dichotomized into the categories: 1 = “all of the time” or “most of the time”; and 0 = “some of the time,” “a little of the time,” or “none of the time.”
Online participants answered additional questions about their perceptions of receiving the program online: “What did you like about taking the class online?” and “What did you NOT like about taking the class online?” with prepopulated response options. In addition, one open-ended survey question asked, “What is your opinion of taking this class online instead of in-person?”
Sexual Health Knowledge and Attitudes
We assessed three measures of sexual health knowledge and attitudes at entry and exit. To measure participants’ knowledge of where to access sexual health services (SHS), they were asked, “Do you know where a clinic or doctor in your community is where teens can get sexual health information and services such as condoms, birth control, pregnancy tests, STI tests/treatment, and/or HIV tests?” Responses were dichotomized as 1 = “yes” and 0 = “no” or “not sure.” The second measure assessed participants’ comfort with sexual refusal. They were asked, “Suppose someone you liked wanted to have sex with you, and you did not want to have sex. How comfortable would you be telling that person you do not want to have sex/you do not consent?” Responses were dichotomized as 1 = “very comfortable” or “kind of comfortable” and 0 = “kind of uncomfortable” or “very uncomfortable.” A third measure assessed their likelihood of seeking SHS by asking “How likely is it that you would go to a clinic or to a health care provider for sexual health services if you needed them?” Responses were dichotomized as 1 = “very likely” or “somewhat likely” and 0 = “somewhat unlikely” or “very unlikely.”
Confidence
We measured confidence in life skills and abilities at entry and exit with a 4-point Likert-type scale. Responses to survey questions about how confident participants felt writing a resume, writing a cover letter, making a budget, and doing an interview were dichotomized (1 = “very” or “moderately”; and 0 = “slightly” and “not at all”).
Participant Characteristics
Questions in the entry survey measured demographic and socioeconomic characteristics, including age, sexual orientation, geographic location (rural, urban), race/ethnicity, and vulnerable living situation, such as foster care or shelters. Gender identity was assessed using a multiple-response item, with options including female, male, transgender, gender queer/nonbinary, and other (with a write-in option). The survey also included questions about technology ownership (owned a smartphone, iPad/tablet, or laptop/desktop computer) and access to the Internet at home.
Analyses
We used independent sample t-tests and chi-square tests to compare characteristics of the online and in-person program participants. Next, we used multivariable logistic regression to compare perceptions of the program by delivery mode. Finally, we used multivariable logistic regression to compare sexual health knowledge and life skills confidence between program entry and exit, estimating separate models for the online and in-person participants. We also estimated a model for the full sample, which included a generalized estimating equation with interaction between program completion and delivery mode.
Given that many outcomes were based on Likert-type scales, we dichotomized responses before modeling. We chose this approach for two key reasons: (1) to improve clarity and interpretability when comparing the proportion of participants who achieved the desired outcome across multiple measures and (2) due to distributional challenges. Responses were often skewed, with few or no participants selecting the lowest response categories, particularly in the online program group. All models adjusted for age, gender, sexual orientation, vulnerable living situation, Hispanic ethnicity, and rural location. All quantitative analyses were conducted using Stata 16.1.
Qualitative responses to the open-ended question were individually coded in Excel by two researchers, while a third researcher resolved any discrepancies in coding assignment. Coded results were then analyzed for key themes.
Analytic Sample
From the total sample of 528 participants, we excluded 10 participants who did not complete the entry survey from the first analysis comparing characteristics of online and in-person participants, for an analytical sample of 518 participants (in-person, n = 349; online, n = 169). For the analysis of program perceptions and outcomes, we further excluded 94 participants who did not complete exit surveys, 27 participants who did not have matched entry/exit surveys, and 33 participants with missing demographic or outcome data. Our final analytic sample included 364 participants with complete entry/exit survey data (in-person, n = 281; online, n = 83). Participants in the final analytic sample were slightly older and more likely to live in rural areas than those who were excluded. Online participants were more likely to be excluded (51% vs. 19%), primarily due to exit survey nonresponse. We conducted sensitivity analyses, comparing the entry outcome measure scores between participants included and excluded from the analysis and found no significant differences, suggesting the groups were comparable.
All online participants completing an exit survey (n = 114) were included in the qualitative analysis of perceptions of online programming.
Results
The average age of the sample was 15.3 years (Table 1). Most participants identified as female (66%) and Hispanic (76%). Nearly all reported smartphone ownership (89%) and home Internet access (90%). About 24% identified as LGBTQ+, and 19% lived in a vulnerable setting. Compared with in-person participants, the online sample included more females and LGBTQ+ youth but fewer from vulnerable settings or rural areas. Online participants were also more likely to own an iPad/tablet (60%) and computer (65%).
Baseline Characteristics and Outcome Measures of In-Person and Online ITK Participants
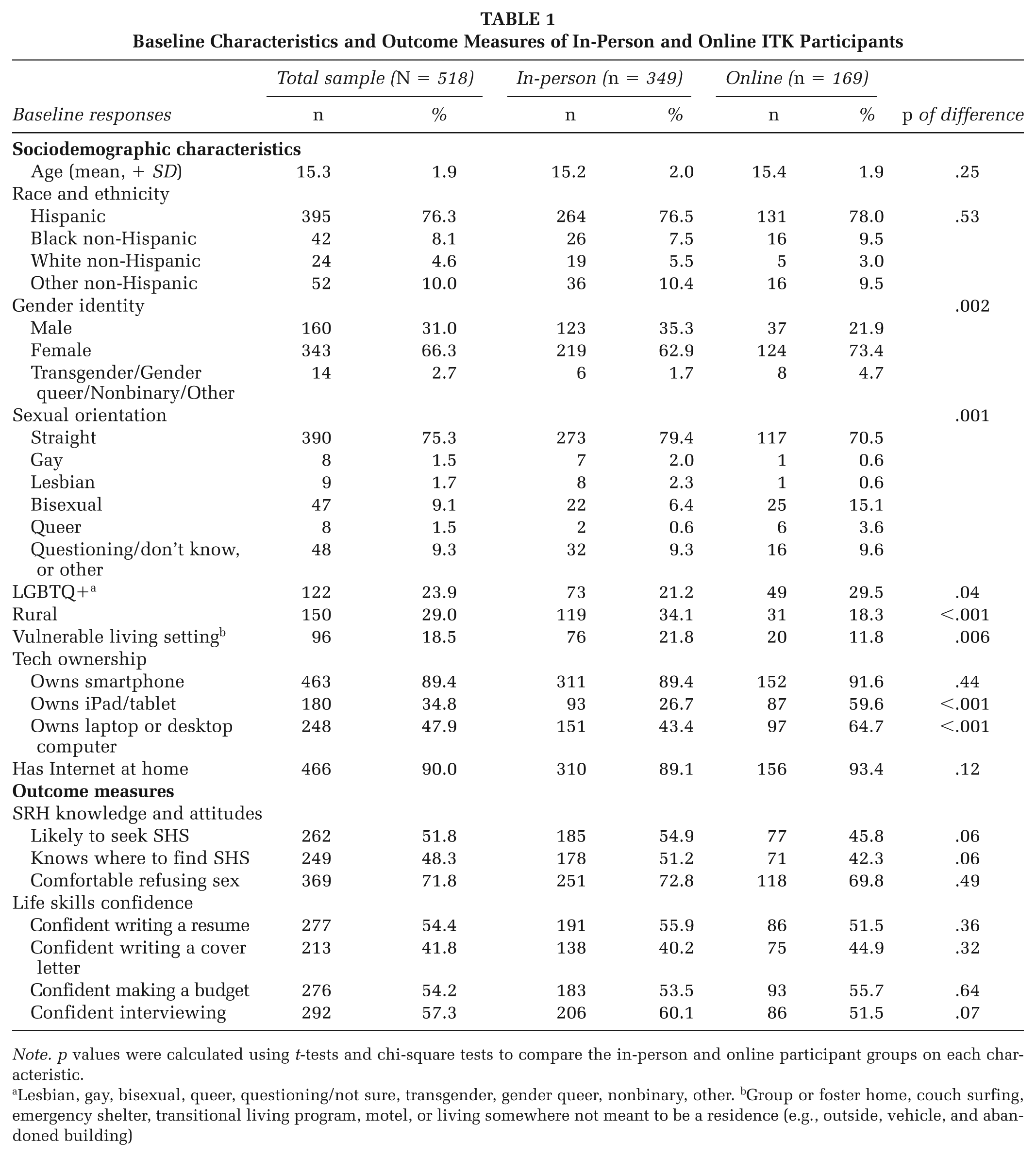
Note. p values were calculated using t-tests and chi-square tests to compare the in-person and online participant groups on each characteristic.
Lesbian, gay, bisexual, queer, questioning/not sure, transgender, gender queer, nonbinary, other. bGroup or foster home, couch surfing, emergency shelter, transitional living program, motel, or living somewhere not meant to be a residence (e.g., outside, vehicle, and abandoned building)
Participant Perceptions of the Program
Most participants, regardless of delivery mode, shared positive reviews of the program (Table 2). More than 80% of all participants responded “all of the time” or “most of the time” to four of five survey measures (clarity of program material; helpfulness of discussions or activities; opportunity to ask questions; and interest in program sessions), with no significant differences by delivery mode. However, significantly fewer online participants reported feeling respected compared with in-person (78% vs. 89%, respectively; adjusted odds ratio [aOR] = 0.31, 95% confidence interval [CI]: 0.15–0.61).
Participant Perceptions of ITK by Method of Program Delivery
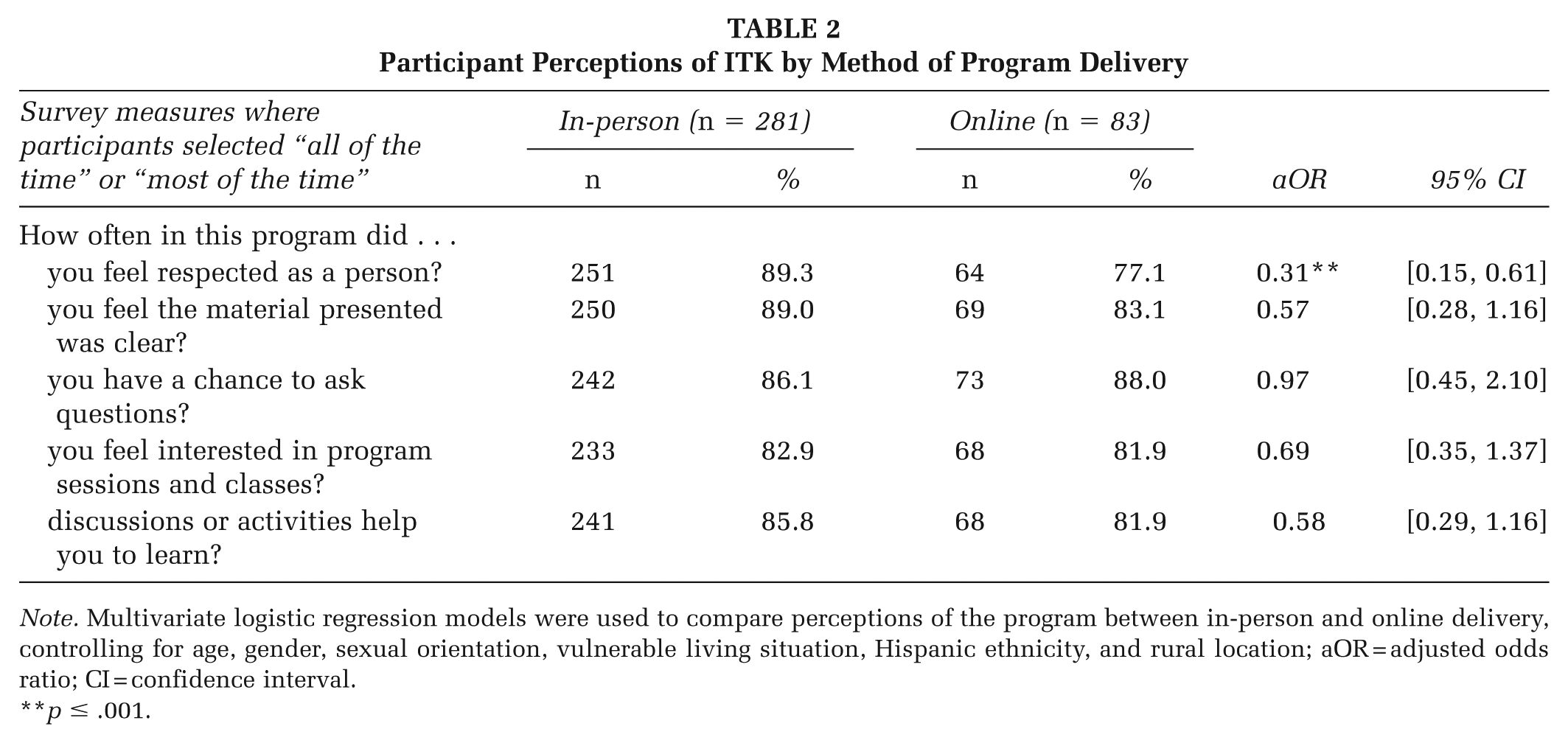
Note. Multivariate logistic regression models were used to compare perceptions of the program between in-person and online delivery, controlling for age, gender, sexual orientation, vulnerable living situation, Hispanic ethnicity, and rural location; aOR = adjusted odds ratio; CI = confidence interval.
p ≤ .001.
Online participants were asked to share what they did and did not like about the format (Table 3). Most appreciated being able to work at their own pace (62%) and ask questions privately (61%). However, 37% reported issues with unreliable Internet connections, such as the video freezing or sound problems.
Participant Perceptions of Taking ITK Online
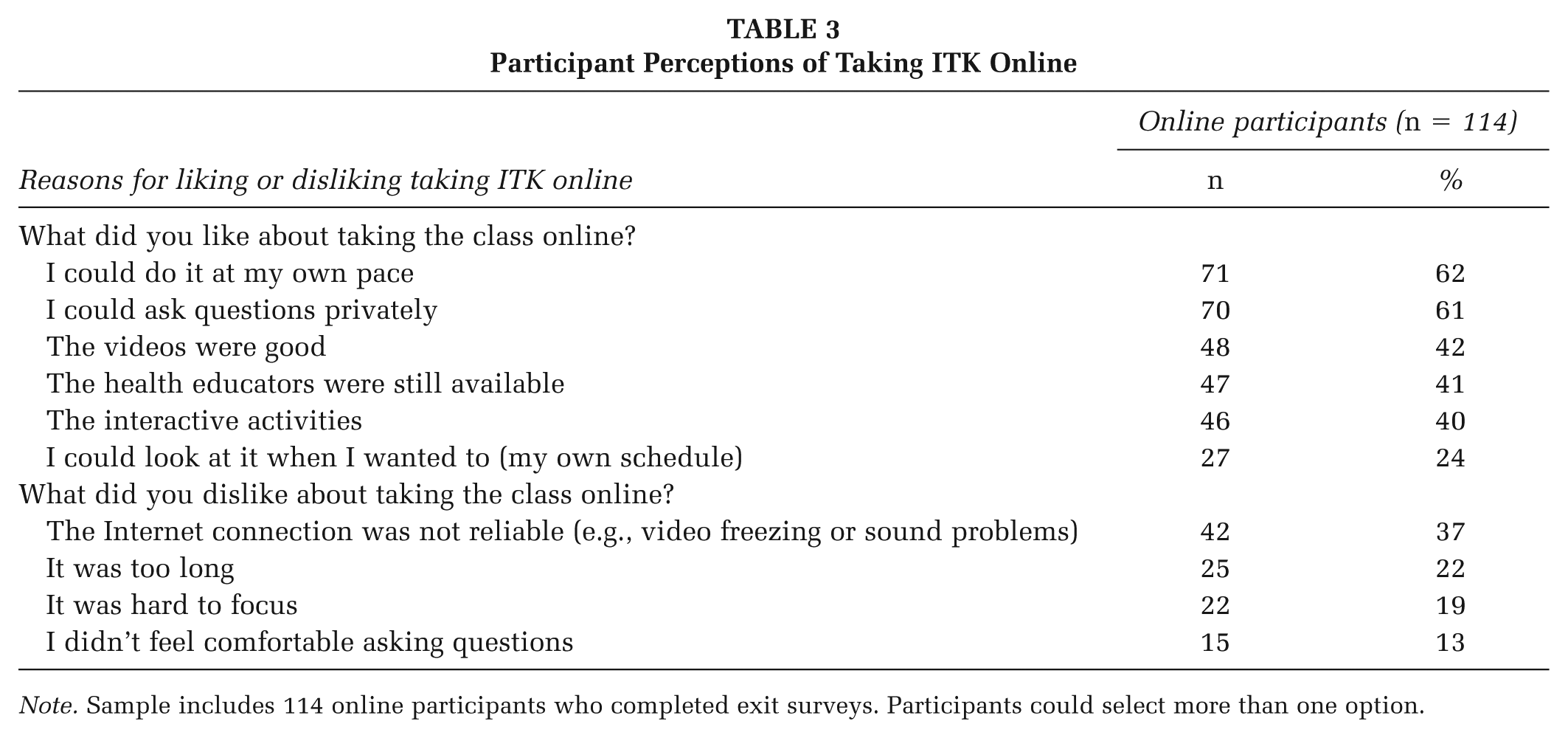
Note. Sample includes 114 online participants who completed exit surveys. Participants could select more than one option.
In open-ended responses, most reacted positively to the online format. The most common reason was that online delivery was more convenient or easier, which often related to enjoyment and comfort. One shared, “I believe it was easier and more fun than in-person classes,” and another wrote, “I felt more comfortable with the topics and was able to answer the questions a bit easier.” A few people mentioned the anonymity or confidentiality that online delivery provides. One stated, “I’m fine with online because I’m very shy,” and another noted, “It was very great because you feel safe and comfortable since it’s online.” Others appreciated the engaging format that promoted learning. One stated, “I enjoyed taking this class online; it was something different and fun. I was able to learn a lot of things that I didn’t really know.”
However, a small number of participants noted challenges with the online format or preferred in-person delivery. One commented, “I would prefer to take it in class because it’s more hands on and engageable.” Another stated, “I think it was good, but it would have been funner to do it in-person to meet everyone.”
Change in SRH Knowledge and Attitudes
There were statistically significant improvements among in-person participants for all the SRH knowledge and attitudes measures (Table 4). Online participants also showed significant increases for all measures, except for feeling comfortable refusing sex. We also used generalized estimating equations of the program effect with interactions by delivery mode and found no differences in program impact by delivery mode (see Supplemental Appendix).
Change in Sexual Health Knowledge and Attitudes and Life Skills Confidence Before and After ITK Program, by Program Delivery Method
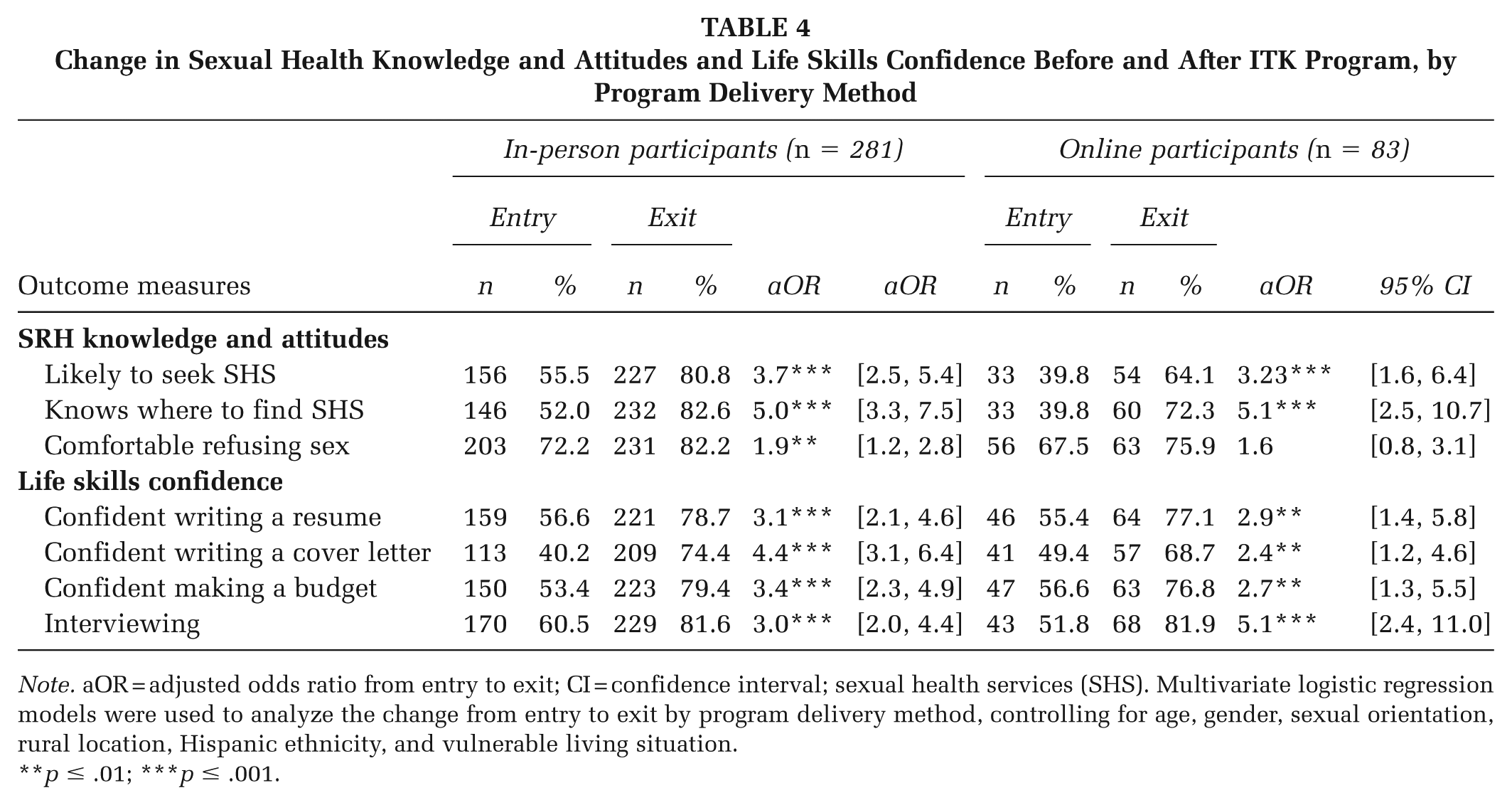
Note. aOR = adjusted odds ratio from entry to exit; CI = confidence interval; sexual health services (SHS). Multivariate logistic regression models were used to analyze the change from entry to exit by program delivery method, controlling for age, gender, sexual orientation, rural location, Hispanic ethnicity, and vulnerable living situation.
p ≤ .01; ***p ≤ .001.
Change in Life Skills Confidence
Participants showed similar improvements in life skills confidence. Both groups showed significant improvements in confidence in writing a resume, cover letter, budgeting, and interview skills. Generalized estimating equations showed a greater increase in cover letter confidence for in-person participants, with no other differences by delivery mode (see Supplemental Appendix).
Discussion
Regardless of modality, ITK participants showed significant increases in SRH knowledge, attitudes, and confidence in life skills. In addition, most participants in both groups had positive opinions of the program, which was similar to the acceptability of other online SRH programs (Faccio et al., 2023; Patel et al., 2022). These findings show the potential for online delivery of sexual health education to achieve short-term outcomes and be well-received by youth.
Other studies conducted during the pandemic found more positive outcomes for in-person compared with virtual learning (Duckworth et al., 2021). Because education had to shift rapidly to online formats during that period, the quality of virtual instruction may have been compromised. In contrast, key ITK content was preserved, and the curriculum was carefully adapted for online delivery, which may explain why outcomes were comparable across delivery modes. These results align with prior literature that suggests a well-designed online program should have similar outcomes to a well-designed classroom-environment (Barbour 2019). Scriver (2023) identified common challenges in online sexual health instruction, including low engagement, technology issues, insufficient activity time, difficulty responding to nonverbal cues, and lack of privacy. ITK redesigned activities and trained the health educators to help overcome these challenges, particularly around youth engagement and skill building. For example, Kahoot—used in the in-person version as an interactive quiz tool—was less effective in the online course due to challenges switching between platforms and holding students’ attention. Instead, game elements were directly embedded into Zoom using polls, annotations, and whiteboards to maintain student engagement. Successful online programs require flexibility and opportunities for pilot testing to refine instructional and engagement strategies. Because the in-person ITK program already used technology and interactive activities, its transition online may have been easier than for other programs’ instructors (Decker et al., 2022).
One notable difference was that online participants did not show significant improvement in comfort refusing sex, unlike in-person participants. This skill-based outcome may be better supported in in-person settings that allow for interactive feedback and real-time discussion of sensitive topics. However, one study of an asynchronous online intervention for LGBT youth found significant improvements in safer sex outcomes, including sexual assertiveness, suggesting online programs can successfully support behavioral competencies (Mustanski et al., 2015). Relatedly, a systematic review of online education and training programs found that active learning approaches, which include discussions and simulations, can lead to improved knowledge and skill development (Wittayakom et al., 2024). Because skill acquisition is often a precursor to behavior change, further research is needed on how to best adapt skill-building components to online sexual health education.
Another consideration is that underserved youth may have less access to online sexual education. Although online and in-person participants were similar in age and race and ethnicity, fewer youth in rural areas and vulnerable living settings participated online. While smartphone ownership was similar, more online participants reported owning a laptop or computer, which may reflect ongoing tech access disparities (Golden et al., 2023). Low-income families and communities of color often face limited access due to shared devices and unreliable or slow Internet (Haderlein et al., 2021). As online education and virtual schooling continue to grow, developers and educators must thoughtfully address how to use technology to expand access rather than exacerbating disparities (Zervos et al., 2023).
Limitations
The rapid pivot to online implementation presented data-collection challenges. It was more difficult to collect surveys and assign and track unique identification numbers, resulting in lower survey response rates and fewer matched entry/exit surveys in the online group. Given the relatively small sample size, particularly for the online group, nonsignificant findings should be interpreted with caution. In addition, the pandemic may have positively impacted participants’ perceptions compared with less engaging school programming. Finally, the single gender question did not distinguish between cisgender and transgender youth.
Reflexivity Statement
The authors represent a diverse, multidisciplinary group, including two doctoral researchers in public health (MJD and JY), three with graduate public health degrees (AG-G, NB, and JR), and three from the study community with extensive experience as sexual health educators (SH, JR, and KA). We collaborated with community partners, youth, and health educators to design the intervention, refine the survey, and interpret results. Including community partners helped the research team examine how our backgrounds influenced data collection and interpretation and ensured their perspectives and expertise informed every stage of the research.
Implications for Practice
Quality sexual health education can be delivered in-person or online with positive short-term outcomes and participant perceptions. Participants in both modalities demonstrated improvements in SRH knowledge, attitudes, and life skills confidence and reported positive program perceptions. These findings support offering SRH education virtually. However, transitioning to an online format requires a thoughtful redesign of curriculum content and activities to accommodate the modality’s strengths and challenges. Program developers and facilitators should develop strategies to ensure that online implementation maintains participant confidentiality, promotes engagement, and avoids exacerbating inequities in access. In addition, developers must ensure that online content remains medically accurate and inclusive to provide youth with the knowledge they need to make informed decisions about their health. Online sexual health education offers an opportunity to reach youth in areas lacking comprehensive sexual health education due to limited resources or restrictive policies.
Implications for Research
Future research should examine the impacts of online instruction on access to information, participant outcomes, and program costs beyond the unique circumstances of the COVID-19 pandemic. In addition, future research should compare the differences in program acceptability and effectiveness between individual, group-based, asynchronous, synchronous, and blended learning models. Further studies are needed to assess the relationship between delivery mode, skill-building strategies, and behavior change. In particular, rigorous research is needed to assess intermediate and long-term outcomes at the K–12 level.
Supplemental Material
sj-xlsx-1-hpp-10.1177_15248399251411256 – Supplemental material for Comparing In-Person and Online Sexual Health Education Program Delivery: Youth Perspectives and Short-Term Outcomes
Supplemental material, sj-xlsx-1-hpp-10.1177_15248399251411256 for Comparing In-Person and Online Sexual Health Education Program Delivery: Youth Perspectives and Short-Term Outcomes by Martha J. Decker, Abigail Gutmann-Gonzalez, Natasha Borgen, Salish Harrison, Julio Romero, Kayla Angeles and Jennifer Yarger in Health Promotion Practice
Footnotes
Authors’ Note:
The authors are grateful to Bhupendra Sheoran and our other partners at the Youth+Tech+Health initiative of ETR, the staff at Fresno Economic Opportunities Commission, and the study sites, as well as the youth who participated in this study. This study was funded by the Department of Health and Human Services, Family and Youth Services Bureau, and Personal Responsibility Education Program Innovative Strategies (Grant No. 90AP2688-01-00). Dr. Yarger received support from the National Institute of Diabetes and Digestive and Kidney Diseases through grant K12DK111028. The sponsors were not involved in the writing of the article or the decision to submit the article for publication.
ORCID iDs
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.