
Abstract
Past Australian research has identified gaps in midwives’ knowledge, confidence and skills to incorporate oral health promotion within routine antenatal care. The Midwifery Initiated Oral Health (MIOH) evidence-based online training program is designed to provide midwives with practical skills required to promote oral health. The long-term effectiveness of the MIOH program on midwives’ oral health knowledge and confidence to incorporate oral health promotion into practice was assessed. A pre-post-test design was used with a convenience sample of midwives (pre vs. post and post versus long-term follow-up ≥12 month) participating in the program with questionnaires capturing self-reported oral health knowledge and confidence. Data was analyzed using descriptive and inferential statistics (McNemars test). Midwives (pre,
Keywords
During pregnancy, women are at higher risk of oral health complications such as gingivitis, periodontitis, and dental caries, which are linked to hormonal fluctuations, dietary changes, and increased vomiting (George et al., 2010; Hartnett et al., 2016). Oral diseases, such as periodontitis during pregnancy has been associated with complications such as premature and low-birth-weight babies and pre-eclampsia (Bendek et al., 2021; Hartnett et al., 2016). Women with periodontitis have been reported to be at heightened risk for developing Gestational Diabetes Mellitus (GDM) (Abariga & Whitcomb, 2016; Bunpeng et al., 2022), which is concerning as those who experience GDM have an increased risk of developing type 2 diabetes (Bellamy et al., 2009). Despite a higher incidence of oral health problems, many women in Australia and elsewhere do not access dental services during pregnancy due to factors such as lack of awareness of the importance of oral health in pregnancy, safety concerns of dental treatment, and barriers such as cost and accessibility (Al Agili & Khalaf, 2023; George, Johnson, Blinkhorn, Ajwani, Ellis, & Bhole, 2013; Kamalabadi et al., 2023). Globally, misconceptions about oral health issues resulting from pregnancy-related hormonal changes have been noted in several studies necessitating the need for oral health education during pregnancy (Ahmadi-Motamayel et al., 2023; Kamalabadi et al., 2023).
The importance of non-dental professionals promoting maternal oral health has only recently been explored (Bashirian et al., 2023; George et al., 2010). Previously, only oral health professionals received training on oral health during pregnancy (Boutigny et al., 2016). However, several studies have identified midwives to be well-placed to provide pregnant women with important oral health information, conduct oral health assessments and refer clients to dentists (Bagherzadeh et al., 2021; George, Villarosa, et al., 2019). Pregnancy is a time when women have higher engagement with health care services, more likely to trust and accept information (George, Johnson, Blinkhorn, Ajwani, Ellis, & Bhole, 2013; Olander et al., 2018) and adopt health supporting behaviors for the benefit of their unborn child (Bagherzadeh et al., 2021; Cagetti et al., 2024). In Australia, some essential dental services are subsidized for eligible populations under Medicare (Health Direct, 2021). In Victoria, priority access to subsidized public dental services is provided for pregnant women who have a concession card (Dental Health Services Victoria, 2021a); however, the proportion of pregnant women accessing dental services has been historically low (Lim et al., 2018).
In Australia, the majority (75%) of hospital-based births occur in public settings managed by midwives (Australian Institute of Health and Welfare, 2020). Midwives are generally the first point of contact for health care in pregnancy and are uniquely placed to promote oral health within their routine practice (Heilbrunn-Lang et al., 2015). Both Australian and international clinical guidelines for midwives stipulate the delivery of oral health promotion during pregnancy (Australian Living Evidence Collaboration, 2024; Oral Health Care During Pregnancy Expert Workgroup, 2012). Nevertheless, prior research (George et al., 2010; Heilbrunn-Lang et al., 2015) has identified gaps in midwives’ knowledge, confidence and skills to incorporate oral health promotion within routine antenatal care both in Australia (George et al., 2010; Heilbrunn-Lang et al., 2015) and in other countries. One German study found that about 50% of midwives recommended dental visits during pregnancy (Wagner, Heinrich-Weltzien, 2016). Bechina et al. (2023) identified that while midwives and gynecologists in France reported good oral health knowledge during pregnancy, there were knowledge gaps about the link between periodontal diseases and pregnancy complications. In both the United States and France, midwives reported a lack of adequate oral health training to inform their clinical practice, even though some continued to give oral health advice to clients (Bossouf et al., 2023; Naavaal & Claiborne, 2021). A recent systematic review exploring the oral health literacy levels of nursing professionals similarly found gaps in oral health knowledge and training (Albougami, 2023).
In recognition of these knowledge gaps and challenges, in 2012, Oral Health Victoria (OHV) (formerly Dental Health Services Victoria) implemented the Healthy Families, Healthy Smiles (HFHS) program (Dental Health Services Victoria, 2020). The objective of the HFHS program was to extend the oral health promotion capacity and skills of early childhood and health professionals who work with pregnant women and young children (0–3 years). This encompassed building the capacity of health and early childhood professionals, including midwives, to embed oral health promotion and prevention activities in their routine practice. The program aligned with the action areas of the Victorian Government’s Action Plan to Prevent Oral Disease (2020–2030; Department of Health and Human Services, 2020) and the National Oral Health Plan (2015–2024; Oral Health Monitoring Group, 2015) in engaging non-oral health sectors to reach pregnant women to improve their oral health.
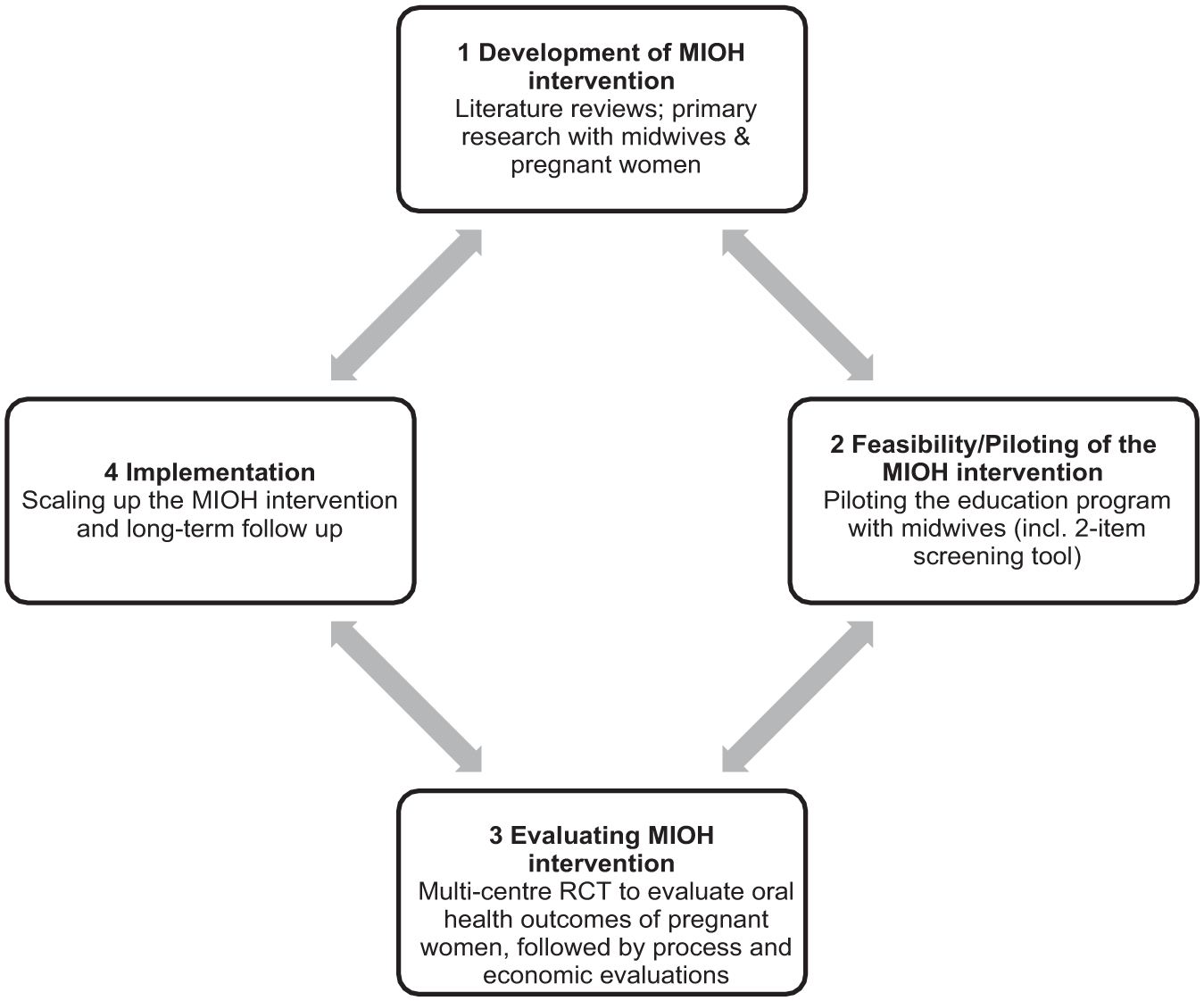
There has been a growing number of oral health promotion programs that encourage interdisciplinary collaboration among non-dental professionals, including doctors and pharmacists (Barnett et al., 2014). Nevertheless, the effective integration of oral health into the clinical practice of non-dental professionals requires comprehensive training, adequate incentives and the implementation of government policies that support integration (Christian et al., 2023). The Midwifery Initiated Oral Health (MIOH) education program, initially developed and piloted in New South Wales (NSW) in 2010 (George, Lang, et al., 2016; Heilbrunn-Lang et al., 2015), was a comprehensive evidence-based online training program which provides midwives with the practical skills required to promote oral health (George, Shamim, et al., 2012). It includes three self-paced modules focused on oral health screening, education, and referral of pregnant women to dental services and is accredited by the Australian College of Midwives as a formal continuing professional development activity (George, Duff, et al., 2012). The development of the MIOH intervention was guided by the Medical Research Council (MRC) framework (Shahsavari et al., 2020) for complex interventions (Figure 1). The framework outlines four non-linear steps: (1) Development; (2) Feasibility/Piloting; (3) Evaluation; and (4) Implementation.
MIOH Intervention Framework
Figure 1 illustrates how the MIOH intervention aligned with the four steps of the MRC framework. Step 1 focused on intervention development through literature reviews (George et al., 2010; George, Shamim, et al., 2012) and primary research with pregnant women (George, Johnson, Blinkhorn, Ajwani, Bhole, et al., 2013; George, Johnson, Blinkhorn, Ajwani, Ellis, & Bhole, 2013) and midwives (George et al., 2011). Step 2 involved piloting the intervention (George, Lang, et al., 2016) to assess feasibility. Combined evaluations across NSW and Victoria showed that training improved midwives’ oral health knowledge (21%; George, Lang, et al., 2016), confidence (82%), and referrals to dental services (78%; George, Lang, et al., 2016; Heilbrunn-Lang et al., 2015).Midwives also found the program suitable, appropriate, useful and feasible (Heilbrunn-Lang et al., 2015).
The third step, Evaluation, included a multicenter randomized controlled trial (RCT; George et al., 2018), and follow-up short-to-medium term process evaluations (Ajwani et al., 2019; Dahlen et al., 2019; George, Villarosa, et al., 2019; Heilbrunn-Lang et al., 2015). The economic evaluation by Tannous et al. (2021) found that the program was cost-effective compared with current practices. The World Health Organization endorsed the program as a case study for integrating oral health into primary health care (World Health Organization, 2023).
The fourth step involved further adaptation, evaluation, and dissemination as a subsidized course in Victoria through the HFHS program in 2012 (Dental Health Services Victoria, 2021b). Participation in the MIOH program in Victoria was fully subsidized by OHV through the HFHS program for midwives who pass the course within a set-time frame. Long-term follow-up assessed the program’s sustained impact in two populations. The first group comprised of children of women from the RCT and focused on evaluating maternal preventive oral health behaviors and child oral health outcomes (George et al., 2023). The second group included the midwives who received MIOH training, which forms the focus of the present study.
Aim and Purpose
Studies on health promotion programs have suggested that the retention of knowledge and confidence may wane over time following education and may require further training and education (Bardosono et al., 2018; Ferreira et al., 2016; Naeem, 2016). This has direct implications for the MIOH education program. Thus, the current study aimed to assess the short and long-term impact of the MIOH program by following up on a cohort of Victorian midwives who completed the training. Specifically, this study assessed the extent to which midwives retained knowledge and confidence on a range of oral health topics such as answering oral health related questions, referring pregnant women to dental services, conducting oral health assessments and introducing the topic of oral health over a period of at least 12 months. This study formed part of a broader evaluation (Dental Health Services Victoria, 2020) that also explored factors affecting the scalability of the MIOH program, the findings of which will be presented elsewhere.
Method
Study Design and Ethics
A pre-post quasi experimental design was used to evaluate the long-term impact of the MIOH program. Ethics approval was obtained from OHV (HREC #263) and the Department of Health and Human Services (Project no. 08/15) Human Research Ethics Committees.
Framework
The MIOH intervention employed the MRC framework for complex interventions to guide its development and evaluation (Shahsavari et al., 2020). As part of the fourth and final step of the MRC framework, evaluating intervention implementation, this present study followed midwives to assess the short term, long-term and sustained impact of the training. The process and economic evaluations of the short and medium-term effects of the MIOH intervention have been published elsewhere (Ajwani et al., 2019; Dahlen et al., 2019; George, Villarosa, et al., 2019; Tannous et al., 2021).
Recruitment and Participation
Study recruitment and data collection of pre-post questionnaires took place between 2014 and 2018.
Recruitment to the MIOH Program
Midwives were invited to participate in the MIOH education program through Victorian hospitals and maternity services. A purposive recruitment strategy was employed, and where possible, recruitment of clusters of midwives in larger maternity services was undertaken. Midwives were recruited to the program via telephone calls, email, and meetings with unit managers at targeted maternity services; presentation at staff meetings and professional development events; through the Australian College of Midwives; members of the broader program reference group and their contacts; promotional flyers; OHV website and newsletters distributed to maternity services. Midwives who were interested in the study could ask any additional questions about the study prior to participation. Participants could provide written consent, which was embedded in the training package.
Oral Health Victoria partners with the Victorian Aboriginal Community Controlled Health Organisation through which the program was promoted to midwives working within the Koorie Maternity Service. Midwifery course coordinators and teaching staff also promoted the course to their networks. Eligible midwives were those working in antenatal clinics and undertaking the first booking visit under midwifery care, general practitioner shared care or the caseload model; unit manager or assistant manager; midwifery clinical educator in Victorian setting; teaching staff working in midwifery courses offered by Victorian Universities; midwives working in the Koorie Maternity Service; childbirth and early parenting educators.
Recruitment to Evaluation
Before MIOH training commenced, all midwives were provided with information about the evaluation and those who were interested could ask any additional questions about the study prior to participation. All midwives were provided with a Participant Information Sheet and Consent Form. Participants could provide written consent (within the consent form), or completion of the questionnaire was also considered consent. Questionnaires were distributed at three time points:
Data Collection and Measures
Midwives completed a self-administered online questionnaire that included 25 items (adapted from the earlier evaluation study undertaken in NSW MIOH training program; George, Lang, et al., 2016) which took participants approximately 15 minutes to complete. The questionnaire explored midwives’ demographics, previous oral health training/education, self-reported oral health knowledge and confidence in promoting oral health, and current oral health promotion and referral practices. Demographic information collected included age, gender, professional training/current position, service type, and number of years practicing. The assessment of knowledge included multiple choice questions on a range of topics (response was noted as correct or incorrect), oral health knowledge statements, and perceptions of the participant’s oral health. Midwives’ level of oral health confidence was assessed on a range of oral health statements. Current professional practices were assessed as current practices regarding oral health referral to dental services and resources within their organization. Changes in knowledge and confidence were assessed across pre-, post-, and long-term follow-up questionnaires.
Data Analysis
Data collected between August 20, 2014, and September 24, 2018, from pre-, post-, and long-term follow-up questionnaires were analyzed using STATA Version 17.0. While this study draws on data collection that concluded in 2018, the paucity in data around long-term maternal oral health promotion interventions (Ghaffari et al., 2018) means that the results of this study are still relevant in the present-day context. Descriptive statistics are presented as frequencies (percentages) for categorical data and mean for continuous variables. The McNemars test was used to assess the significance of any changes in midwives’ knowledge and confidence in promoting oral health between pre- and post-training and post-training to long-term-follow-up. Categorical data were combined into two groups to perform McNemars test. Knowledge question responses were grouped for analysis as follows: correct and incorrect; confidence questions: somewhat confident/confident and not confident; and self-reporting of oral health knowledge: good/very good and average/poor/very poor. The level of significance was set at p < .001, and where significance is shown to p < .05 this is reported.
Results
Characteristic of Midwives
All midwives participating in the MIOH training (n = 179, 100%) completed a pre-training questionnaire, 97% (n = 173) of whom completed the post-training questionnaires. A sub-set of participants (12%, n = 22) completed the long-term follow-up questionnaire between 12 and 19 months (average 15 months) after completion of the post-questionnaire.
Most midwives were female (99%), aged ≥40 years (61%) and held an average of 13 years’ experience (Table 1). MIOH reached antenatal services across metropolitan (36%) and rural/regional (64%) Victoria. Most midwives worked in the public health sector (88%) and held a range of professional roles. Generally, midwives attained their qualifications via a university degree (38%), post-graduate studies (46%), or hospital-based training (10%; Table 1).
Characteristics of Midwives (n = 179)
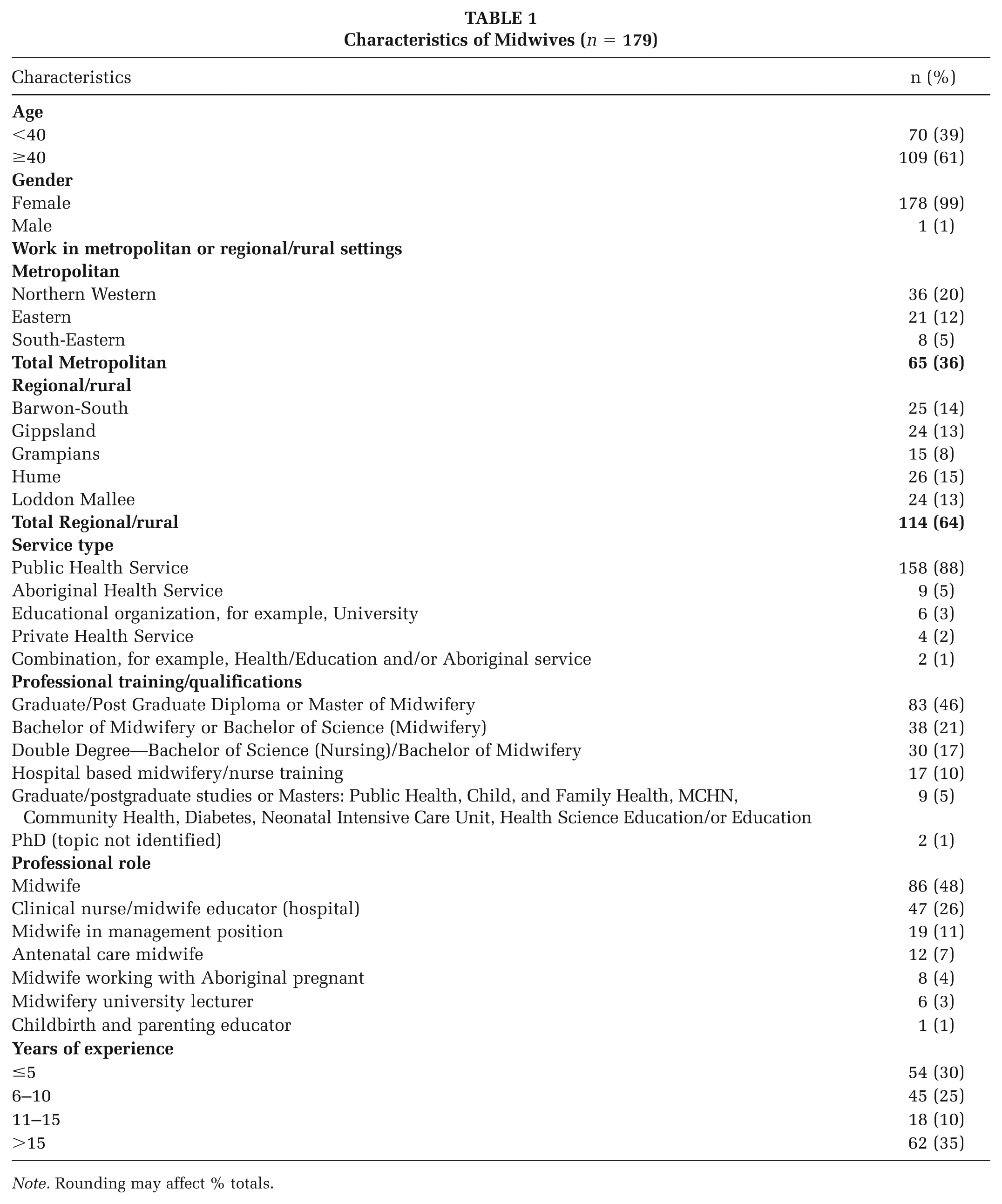
Note. Rounding may affect % totals.
Questionnaire Results
Prior to undertaking the training most midwives reported no previous oral health training (95%). Most midwives (86%) either never (41%) or sometimes (45%) discussed how to prevent tooth decay with their clients and more than a half (55%) did not refer clients to dental services (Table 2). Most (90%) midwives were aware of their organization’s information and resources regarding nutrition during pregnancy; however, few were aware of information or resources relating to the links between pregnant women’s oral health (38%) or child oral health (17%) and nutrition (31%; Table 2).
Current Oral Health Practices Pre-MIOH Participation
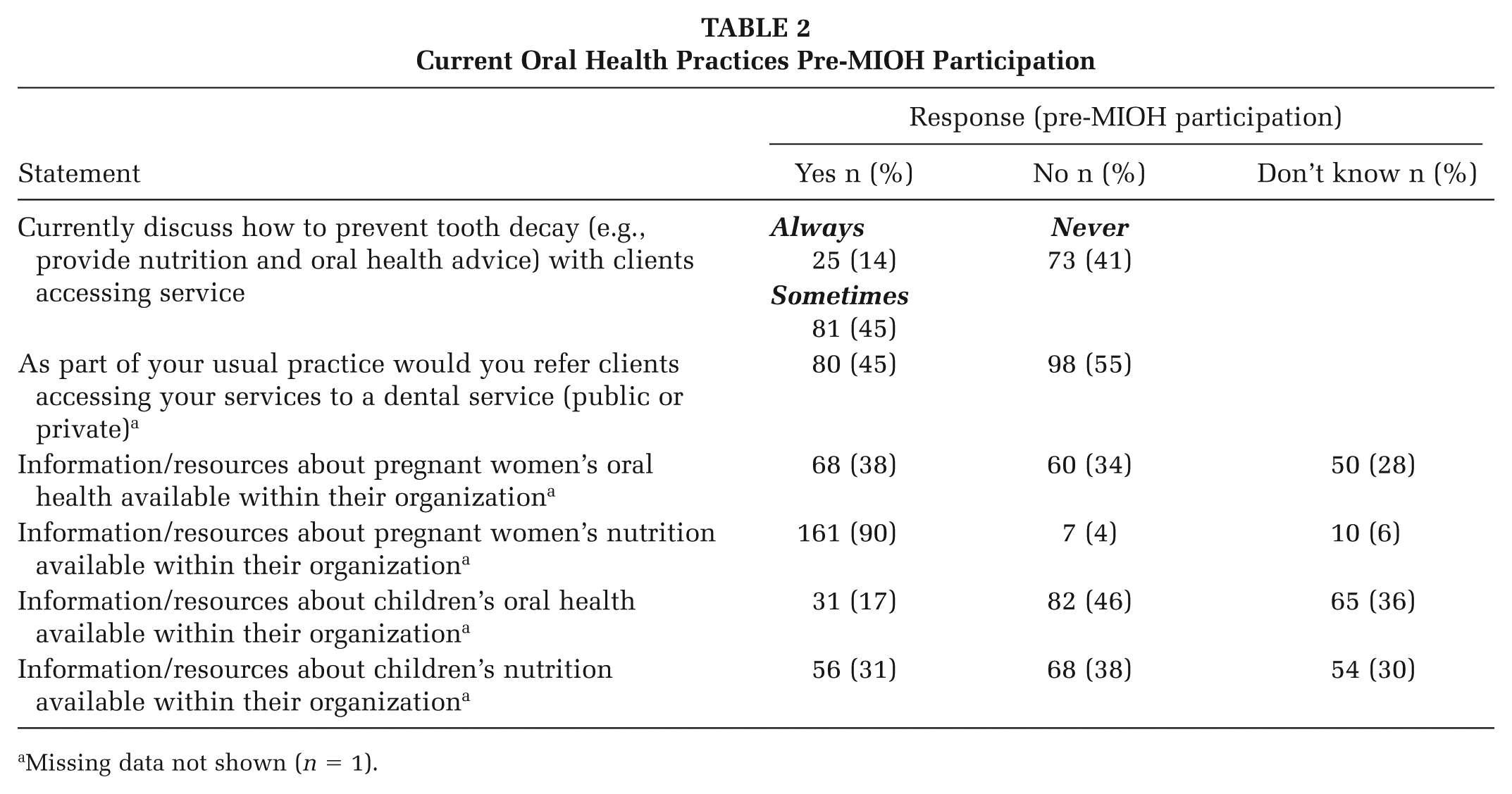
Missing data not shown (n = 1).
Oral Health Knowledge
The proportion of midwives self-reporting their oral health knowledge as good/very good significantly increased from pre- to post-training (19% vs. 94%, p < .001) and was sustained at long-term follow-up (95% vs. 86%, p = .317; Table 3).
Oral Health Promotion Knowledge at Pre-, Post- and Long-Term Follow-Up
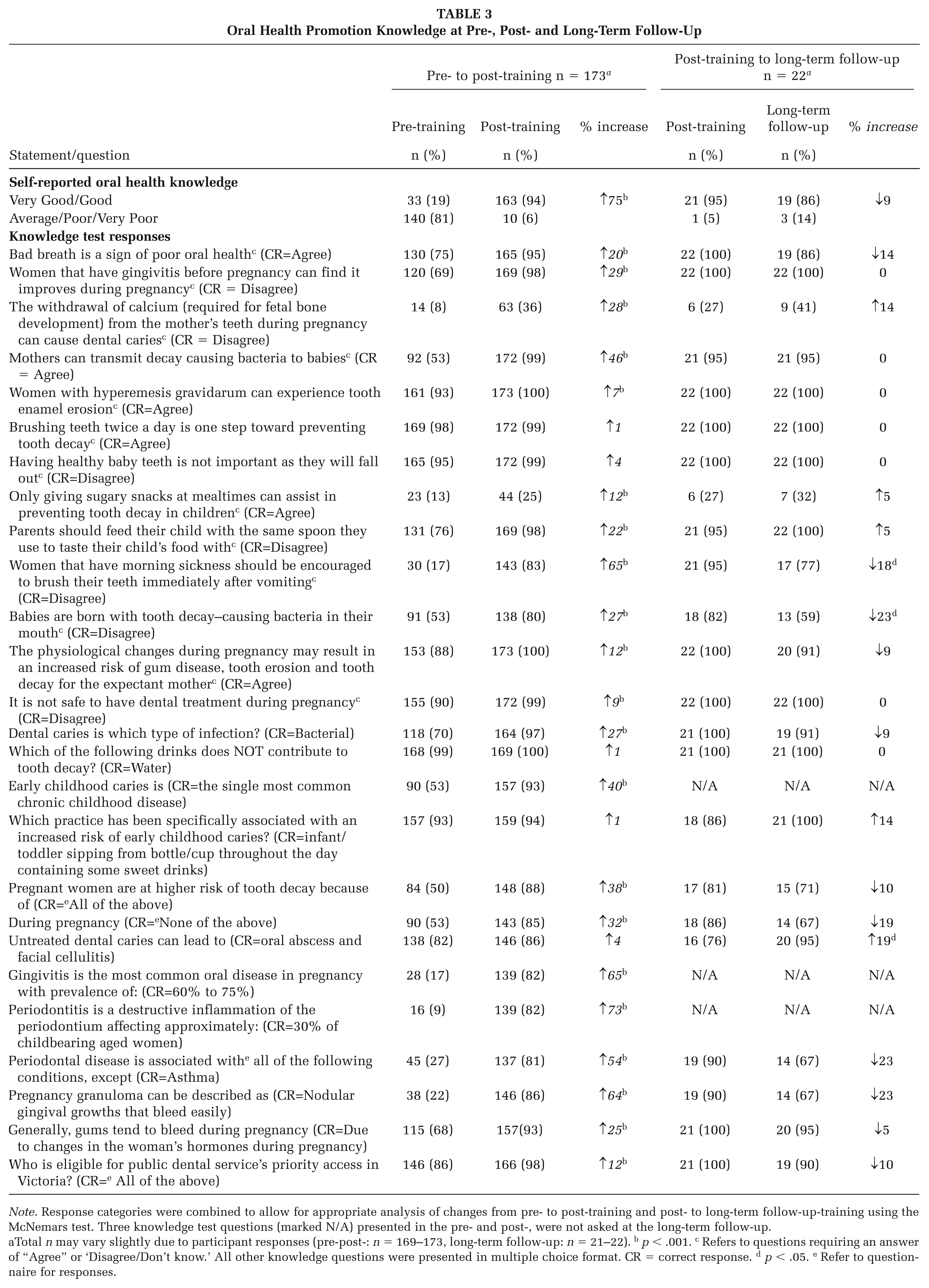
Note. Response categories were combined to allow for appropriate analysis of changes from pre- to post-training and post- to long-term follow-up-training using the McNemars test. Three knowledge test questions (marked N/A) presented in the pre- and post-, were not asked at the long-term follow-up.
Total n may vary slightly due to participant responses (pre-post-: n = 169–173, long-term follow-up: n = 21–22). b p < .001. c Refers to questions requiring an answer of “Agree” or ‘Disagree/Don’t know.’ All other knowledge questions were presented in multiple choice format. CR = correct response. d p < .05. e Refer to questionnaire for responses.
Overall, midwives received high scores on the oral health knowledge test pre-training with ≥70% responding correctly to 46% (n = 12) of the questions (Table 3). A significant increase (p < .001) in the proportion of midwives correctly responding from pre- to post- was shown for 81% (n = 21/26) of the oral health knowledge-based questions. The greatest knowledge gains from pre- to post- training included: understanding that pregnant women should avoid brushing teeth immediately after vomiting (↑65%), the meaning of pregnancy granuloma (↑64%), conditions associated with (↑54) and prevalence of (↑73%) periodontal disease and gingivitis (↑65%), that mothers can transmit decay causing bacteria to babies (↑46%), and ECC being the single most common chronic childhood disease (↑40%; Table 3).
Generally, knowledge test scores remained high at long-term follow-up (Table 3) with either no change or a slight increase in the percentage of correct responses shown for 52% (n = 12/23) of the questions. There was a small reduction in percentage of correct responses on some items, however no significant differences (p > .001) were observed between post- training and long-term follow-up for any of the questions. At long-term follow-up a significant increase at p < .05 in the proportion of midwives correctly responding (↑19%) was shown for understanding that untreated dental caries can lead to oral abscess and facial cellulitis. Significant reductions were shown to p < .05, for questions relating to babies not being born with tooth-decay causing bacteria in their mouth (↓23%) and management of oral health after vomiting in pregnancy (↓18%; Table 3).
Regardless of increases in knowledge between pre-, post- and long-term follow-up, midwives most frequently incorrectly responded to questions about the misconception that the withdrawal of calcium (required for fetal bone development) from the mother’s teeth during pregnancy can cause dental caries. The proportion of midwives responding correctly to this question increased from 8% pre- to 36% post-training (↑28%, p < .001) and from 27% (n = 6/22) to 41% at long-term follow-up (↑14%, p = .317; Table 3). Similarly, the proportion of correct responses for midwives understanding that only giving sugary snacks at mealtimes can assist in preventing tooth decay in children increased from 13% at pre to 25% to post-training (↑12%, p < .001) and from 27% (n = 6/22) post to 32% at long-term follow-up (↑5%, p = .564) but remained low overall.
Oral Health Confidence
The proportion of midwives self-reporting confidence to promote oral health within their practice significantly increased among midwives in most areas assessed (Table 4, p < .001), except in relation to answering questions about healthy eating where confidence remained high (97%–99%). Highest increases included the confidence of midwives to incorporate oral health assessments into consultations (↑59%); determine pregnant women’s eligibility for dental services (↑50%); refer women to dental services (↑40%); and answer questions about oral health (↑38%; Table 4, p < .001). Confidence (confident or somewhat confident) was largely sustained for all items between post- and long-term follow-up with slight changes in confidence that were not statistically significant (↓5–↑5%, p > .001; Table 4).
Oral Health Promotion Confidence at Pre-, Post- and Long-Term Follow-Up
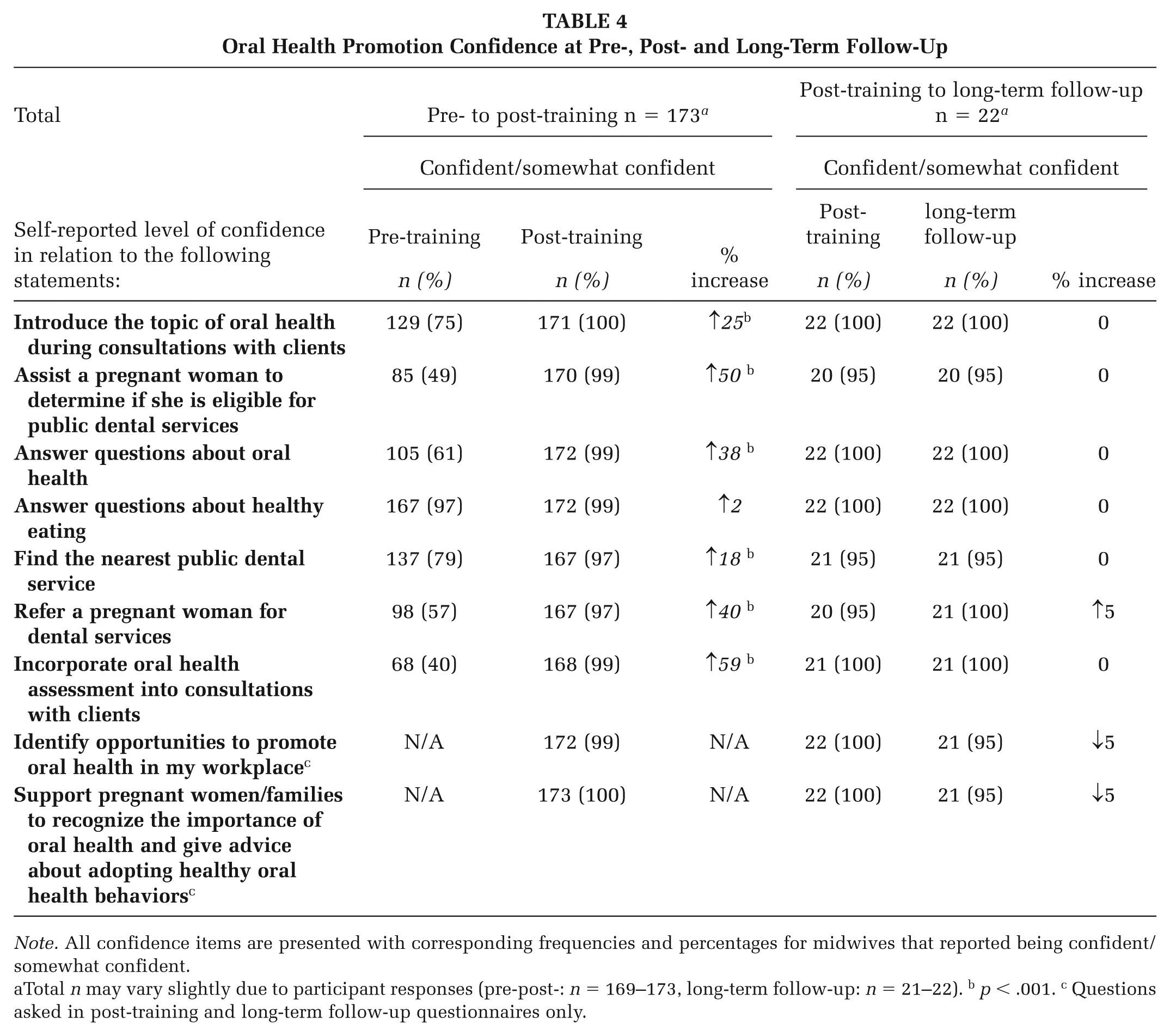
Note. All confidence items are presented with corresponding frequencies and percentages for midwives that reported being confident/somewhat confident.
Total n may vary slightly due to participant responses (pre-post-: n = 169–173, long-term follow-up: n = 21–22). b p < .001. c Questions asked in post-training and long-term follow-up questionnaires only.
Discussion
Our current study with Victorian midwives reaffirmed previous findings in NSW and Victoria, demonstrating that with almost no prior oral health education and varied oral health promotion implementation, the MIOH program can significantly improve midwives’ tested and self-reported knowledge and confidence on a range of oral health topics relevant to their clinical practice (George, Dahlen, et al., 2016; George, Lang, et al., 2016). Past qualitative evaluation findings of the MIOH program have shown the program was suitable, appropriate and feasible to incorporate into midwives’ practice (Heilbrunn-Lang et al., 2015) and that it was cost-effective for improving knowledge and self-reported oral health outcomes for pregnant women in Australia (Tannous et al., 2021). The study showed that many of these improvements can be largely sustained after 12 months, providing evidence of building midwives’ capacity to incorporate oral health promotion into their practice. However, the study experienced a high attrition rate (88%) at the 12-month follow-up. While not uncommon in longitudinal research, it warrants caution in interpreting the findings.
Gaps in Midwives’ Oral Health Knowledge, and Practice
It is important to address midwives’ oral health knowledge gaps as research has shown that midwives educated and trained in maternal oral health are more likely to engage in practices addressing the oral health of pregnant women (George, Dahlen, et al., 2016). Midwives’ sustained knowledge gains around the health implications of periodontal disease on the mother, as suggested in our study are important (George, Villarosa, et al., 2019), given the links between periodontitis and elevated risk for GDM, subsequent development of type 2 diabetes later in life (Abariga & Whitcomb, 2016). We also found potential sustained improvements in midwives’ knowledge around mothers transmitting decay causing bacteria to babies, and the risk factors for the child developing ECC. These results add validity to previous findings (George, Lang, et al., 2016), however past research did not test the improvement across time, which is an added strength of the current study. Xiao et al. (2019) found a reduced incidence of ECC and Streptococcus mutans presence in children whose mothers received prenatal oral health care. While oral health professionals play a significant role in this care, midwives are uniquely placed to complement oral health promotion (George, Sousa, et al. 2019). George, Sousa, et al. (2019) found that Australian midwives believed that they could support mothers by providing accurate and timely oral health information/screening and dental referrals, which is important given that pregnant women are unlikely to visit an oral health professional (Lim et al., 2018). While Spanish midwives acknowledged the importance of dental assessments during pregnancy, they did not have the knowledge to provide advice or conduct a dental assessment (Touriño et al., 2021). Wagner and Heinrich-Weltzien (2016) also observed that German midwives who received advanced oral health training were more likely to consult about the risk of periodontal disease during pregnancy and counsel pregnant women to see a dentist. Previous research indicates these interventions can also result in improved oral health outcomes for the child (George, Sousa, et al., 2019).
Midwives’ Role in Dispelling Misconceptions in Knowledge
Midwives can play a role in dispelling potential misconceptions pregnant women may hold regarding managing their oral health during pregnancy (George, Lang, et al., 2016). Most midwives in our study recognized that dental treatment during pregnancy was safe, and this persisted up to 12 months. Unlike previous findings (George, Lang, et al., 2016), a higher proportion responded correctly, though both studies showed significant improvements. In our study, the statement was presented in the negative (i.e., it is not safe—correct response: disagree), which may partly explain the higher pre-training results. In other studies, misconceptions regarding the safety of dental visiting during pregnancy are common among both women and health care providers, including midwives, obstetricians, and general practitioners (George, Dahlen, et al., 2016). Uncertainties around the safety of dental visits during pregnancy can be a barrier to attendance (Lim et al., 2018) and highlights the importance of midwives retaining knowledge on this topic to alleviate women’s fears with realistic and accurate information. George et al.’s (2017) findings showed a lack of consensus among dentists on how dental treatment should be managed during pregnancy. While the Australian pregnancy care guidelines recommend midwives advise pregnant women to receive a dental visit during pregnancy (Australian Living Evidence Collaboration, 2024), the lack of national evidence-based guidelines for the treatment of oral health during pregnancy, as available in America (Oral Health Care During Pregnancy Expert Workgroup, 2012), continues to be an area for advocacy and action in Australia (George et al., 2017) including in other countries like Spain (Touriño et al., 2021), Germany (Wagner, Heinrich-Weltzien, 2016), England, and Wales (Garry & Boran, 2017).
Confidence and Translation Into Practice
Prior to undertaking MIOH training most midwives in this study avoided discussion on tooth decay prevention with their patients. While developing oral health knowledge is important, it is imperative that midwives feel confident to discuss oral health with pregnant women and address their concerns to enable translation of the knowledge into practice. There was a marked increase in the level of confidence of midwives to carry out all, but one oral health promotion activity listed in the questionnaire and this was indicated at 12 months. Interestingly prior to completing the course, most midwives felt confident to answer questions about healthy eating and knew where to access information/resources regarding pregnant woman’s nutrition. In contrast, few knew where to access information/resources relating to oral health for the pregnant woman and/or child, or nutrition for the child. From a patient perspective, George, Johnson, Blinkhorn, Ajwani, Ellis, and Bhole (2013) found that only 10% of pregnant women received oral health promotion brochures/information during their pregnancy and that they were >3 times more likely to visit a dentist if they had received such information. This is important finding as past NSW research has also shown that antenatal care providers (including midwives) were more likely to discuss the importance of oral health with pregnant women if they themselves had access to oral health information/brochures thereby increasing access for women (George, Dahlen, et al., 2016). Findings relating to midwives’ reporting their awareness of oral health information/resources for pregnant women pre- training were slightly better (38%) in our study compared with previous findings (25%; George, Dahlen et al., 2016; George, Lang, et al., 2016). This may indicate the impact of previous awareness raising and educational efforts of the MIOH program, while also highlighting additional room for improvement.
Prior to MIOH participation, less than half the midwives reported feeling confident to assess women’s oral health or refer clients to dental services as recommended in Australian pregnancy care guidelines (Australian Living Evidence Collaboration, 2024). This lack of confidence was similarly reported in studies across other countries where few midwives would conduct a dental assessment with pregnant women (Naavaal & Claiborne, 2021; Touriño et al., 2021). Past qualitative research has found midwives lacked knowledge about the dental referral processes and felt if it was provided this would improve their confidence and ability to refer (Lim et al., 2018). In Australia, most dentists felt that pregnant women were more likely to seek out their services if encouraged to do so by their antenatal care providers, including midwives (George et al., 2017). Building on previous findings on the MIOH program, our study suggests that it is likely that providing midwives with this information helped to build and could sustain their confidence and ability to fulfill their role in assessing oral health and referring to dental services (George, Lang, et al., 2016).
Strengths and Limitations
A strength of the current study is the assessment of oral health knowledge and confidence retention over the longer term which addresses a common limitation highlighted in previous research (George, Lang, et al., 2016). This study has some limitations, with the use of self-reported knowledge and confidence ratings. However, the inclusion of the knowledge test component to the questionnaire helps to strengthen confidence in the self-reported findings. Combining the somewhat confident and the confident responses to allow for the McNemars analysis may have resulted in an overestimation of participants confidence levels. The program included a higher proportion of participants from regional areas, and this would affect generalizability of the study results to the whole of Victoria.
Another limitation of this study was the high attrition rate (88%) at the long-term follow-up, resulting in a small sample size (n = 12). As such, these findings should be interpreted with some caution. High attrition rates among nurses and midwives in research may be attributed to factors such as heavy workloads, staff shortages, high turnover, and shift patterns (Donnelly et al., 2024; Small et al., 2025). In this study, participants were recruited from a range of high demand antenatal public health settings across the state. Participants included a workforce with demanding workload, competing priorities, and high turnover rates; this introduced additional logistical and ongoing participation challenges for follow-up.
Implications for Antenatal Research
While past evaluations have shown that the MIOH education program significantly improved midwives’ oral health knowledge and confidence, this study adds to the research by showing that these improvements were sustained 12 months after training. Although the intervention was delivered through initial training, there was little incentive for midwives to participate in the 12-month follow-up to measure long-term outcomes. This includes not only follow-up of midwives’ knowledge and confidence but also assessing sustained changes in midwifery practice and oral health behaviors among pregnant women. Given the loss to follow-up experienced in this study, future research should incorporate strategies to mitigate the potential challenges with study retention in this population, such as including monetary incentives (Brueton et al., 2013) and collaborating with the health service to allocate time for midwives to participate in follow up to reduce participant burden (Teague et al., 2018). Future research should also qualitatively explore how the translation of knowledge and confidence gained impacts midwives’ practice and how the midwife’s new learnings might affect organizational oral health policy and procedures and the sustainability of knowledge in practice.
Conclusion—Implications for Policy and Practice
With the relevance and success of this program at upskilling midwives and improving their confidence (George, Lang, et al., 2016; Heilbrunn-Lang et al., 2015), as well as its sustained long-term impact, widening the scope of oral health promotion within antenatal care is warranted. Expanding the role of oral health promotion in routine antenatal care may contribute to improved maternal oral health outcomes, particularly among populations where there is a higher risk of oral health problems. Policymakers should consider mandating oral health promotion modules within undergraduate and postgraduate midwifery education nationally and provide clearer guidance regarding oral health treatment recommendations during pregnancy. Professional organizations could also recommend ongoing oral health training as part of CPD requirements for midwives to maintain competence and knowledge in this area. To implement these changes, however, would require addressing barriers such as resource allocation so midwives have access to the training. To support clinical practice, collaboration with antenatal, public health and dental health services to develop an integrated model for routine preventive oral health care and streamlined referral pathways is a logical next step.
Footnotes
Authors’ Note:
The evaluation was funded by the Victorian Department of Health as a part of the Healthy Families, Healthy Smiles program evaluation.
Data availability statement
While the questions asked within our questionnaire were not sensitive in nature, our survey respondents were assured their raw data would remain confidential and therefore will not be shared. Data not available/the data that has been used is confidential.