
Abstract
It has been previously reported that 79.6% of adults in Malaysia are still unaware of the Malaysian Healthy Plate. Therefore, this study aims to assess changes in undergraduates’ knowledge of the Malaysian Healthy Plate following a peer-led educational intervention. Fifteen active Bachelor’s in Nutrition students, also known as nutrition buddies, were required to conduct a 30-minute workshop covering three topics: the key messages of the Malaysian Healthy Plate, practical guidelines for portioning food groups according to the Malaysian Healthy Plate, and estimating portion sizes using hand measures. A total of 194 undergraduates participated in this workshop. They were asked to self-report their gender, age, ethnicity, study stream, study year, and awareness of the Malaysian Healthy Plate before the workshop began. To assess the change in knowledge resulting from the peer-led educational intervention, all participants were asked to complete nine multiple-choice questions before (pre-intervention) and after (post-intervention) the intervention. The current findings indicate that the mean knowledge score on the Malaysian Healthy Plate significantly improved (t = −8.003, p < .001), rising from 5.25 ± 2.58 at pre-intervention to 6.75 ± 2.30 at post-intervention. It is also worth highlighting that pre-intervention knowledge scores differed significantly by gender, age, study stream, and awareness of the Malaysian Healthy Plate. In contrast, post-intervention knowledge scores showed significant differences only by gender and study stream. In conclusion, incorporating nutrition buddies into a peer-led educational intervention may be cost-effective in raising awareness and potentially fostering behavioral change related to nutrition-related issues among undergraduates.
Keywords
The recent joint statement by the Food and Agriculture Organization of the United Nations (FAO) and the World Health Organization (WHO) reiterates that healthy diets are vital for promoting growth and development, health, and well-being; supporting active lifestyles; as well as preventing foodborne diseases, malnutrition, and both communicable and non-communicable diseases. In line with the importance of healthy diets, they must meet four core principles: (a) provide
The Malaysian Healthy Plate was introduced by the Ministry of Health in 1996 as a visual guide to assist Malaysians in achieving a healthy and well-balanced diet. It incorporates the “quarter-quarter-half” (or suku-suku separuh in Malay) principle by dividing the plate into three sections: half of the plate should comprise fruits and vegetables; one-quarter should consist of carbohydrate-containing foods such as rice, noodles, bread, cereals, cereal-based products, and tubers; and the remaining quarter should include protein-rich food sources like fish, poultry, meat, and legumes. Moreover, the Malaysian Healthy Plate encourages Malaysians to choose plain water or unsweetened beverages with their meals (National Coordinating Committee on Food and Nutrition, 2021). There are five key messages to support meal planning according to the Malaysian Healthy Plate concept, including:
Key Message 1: Consume three regular healthy main meals daily.
Key Message 2: Take healthy snacks in between main meals if needed.
Key Message 3: Consume at least half of your grains from whole grains.
Key Message 4: Consume non-fried and coconut milk-free dishes daily.
Key Message 5: Consume home-cooked foods more often (Ministry of Health Malaysia, 2016).
According to the latest National Health and Morbidity Survey 2023 (NHMS 2023), over half a million Malaysian adults (or approximately 2.5%) are living with four non-communicable diseases: diabetes, hypertension, high cholesterol, and obesity (Institute for Public Health, 2024). Owing to the fact that the Malaysian Healthy Plate was introduced as a strategy to prevent non-communicable diseases (Mohamad Hasnan et al., 2023), it is essential for Malaysians to be aware of and understand how to incorporate this concept into their daily lives. Even though the Ministry of Health launched the Malaysian Healthy Plate some time ago, the NHMS 2019 revealed that 79.6% of adults in Malaysia are still unaware of it (Institute for Public Health, 2020). Therefore, there is an urgent need to promote the Malaysian Healthy Plate and its key messages to the public to encourage the adoption of a balanced and varied diet to curb the rising prevalence of non-communicable diseases.
Existing literature generally shows that peer-led nutritional interventions are effective in promoting the adoption of healthy eating behaviors. For example, a recent systematic review by Ekubagewargies et al. (2025) reported that interventions such as peer-led group discussions, poster making and practical demonstrations not only improved knowledge and attitudes toward healthy dietary behaviors among adolescents aged 10 to 19 years in low- and middle-income countries but also promoted greater intake of fruits and vegetables. Similarly, another systematic review by Yip et al. (2016) highlighted that peer-led nutrition education programs enhanced knowledge, self-efficacy, and attitudes toward healthy eating among school-aged children aged 5 to 18 years in Canada and the United States. In the tertiary education setting, Schroeter et al. (2021) conducted a 4-week pilot study to examine the effectiveness of peer-led nutrition education meetings in improving undergraduates’ knowledge and dietary behavior in accordance with the USDA MyPlate guidelines. Interestingly, undergraduates who participated in the peer-led nutrition education meetings were reported to have better nutrition knowledge and improved dietary behavior. They also showed higher intakes of whole grains, fruits, and vegetables compared to those in the control group. In short, these promising findings support the notion that peer-led nutrition education can significantly impact adolescents and young adults, as peer influence plays a critical role in shaping healthy eating behaviors. Despite those mentioned above, there remains a lack of peer-led nutrition education interventions focused on the Malaysian Healthy Plate. Therefore, this study aims to assess changes in undergraduates’ knowledge of the Malaysian Healthy Plate following a peer-led educational intervention conducted at Management and Science University, Malaysia.
Method
This peer-led educational intervention workshop on the Malaysian Healthy Plate was designed by a registered nutritionist (TST) who also trained the nutrition buddies. It was conducted in conjunction with Health Science Week, organized by Management and Science University. Fifteen Bachelor’s in Nutrition students (also known as nutrition buddies) were required to conduct a 30-minute workshop covering three topics: key messages of the Malaysian Healthy Plate, practical guides on portioning food groups according to the Malaysian Healthy Plate and estimating portion sizes using hand measures. Pamphlets and PowerPoint presentation slides were used during the workshop to educate undergraduates from other programs on these topics. The workshop materials were based on the Panduan Pinggan Sihat Malaysia (Guidelines on the Malaysian Healthy Plate) published by the Ministry of Health Malaysia (2016).
This study employed a quasi-experimental pretest-posttest design without a control group. Students at Management and Science University who were not enrolled in the Bachelor’s in Nutrition program and had never studied any nutrition-related subjects were invited to attend this workshop. They were required to pre-register their interest in attending this workshop by scanning the QR codes shared through WhatsApp groups or posted on the university notice boards. Due to the large number of pre-registrations (210 students signed up for this workshop), these students were randomly assigned to four sessions with approximately 50 students per session. All nutrition buddies were trained by a registered nutritionist (TST) to ensure consistent information delivery across different sessions. Informed consent was obtained from all participants, who were also required to confirm that they met the inclusion criteria before the workshop.
To assess the knowledge of all participants on the Malaysian Healthy Plate, the nutrition buddies developed nine multiple-choice questions, each with one correct answer (Supplemental Appendix 1). All questions were carefully reviewed and approved by registered nutritionists (TST, TSS, and TCX) before being uploaded to Google Forms. All participants were required to respond to the same set of questions twice: once before the workshop (pre-intervention) and once after the workshop (post-intervention). Changes in knowledge scores were then analyzed to assess whether there was an improvement following the peer-led educational intervention. In addition, all participants were also required to self-report their gender, age, ethnicity, study stream, study year, and awareness of the Malaysian Healthy Plate before the commencement of the workshop.
Data Analysis
Data were analyzed using IBM SPSS Statistics version 29.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics, including frequency, percentage, mean, and standard deviation, were used to describe the variables where applicable. For the nine multiple-choice questions intended to assess knowledge of the Malaysian Healthy Plate, each correct answer was coded as 1, while incorrect answers were coded as 0. Therefore, knowledge scores on the Malaysian Healthy Plate can range from 0 to 9 based on the scoring system mentioned earlier. The mean knowledge score was obtained by dividing the number of correct answers by the maximum possible score of 9. Differences in the knowledge scores before and after the peer-led educational intervention were tested using a paired samples t-test. At the same time, variations in knowledge scores across socio-demographics were assessed using either independent samples t-tests (for gender, age, study stream, and awareness of the Malaysian Healthy Plate before the workshop) or one-way ANOVA (for ethnicity and study year). In addition, the correlations between awareness and the knowledge scores attained by the undergraduates were also tested using Pearson’s correlation test. The current study analyzed data from 194 undergraduates who responded to all multiple-choice questions in pre-intervention and post-intervention. Statistical significance was set at a p-value of less than 0.05 (p< .05).
Results
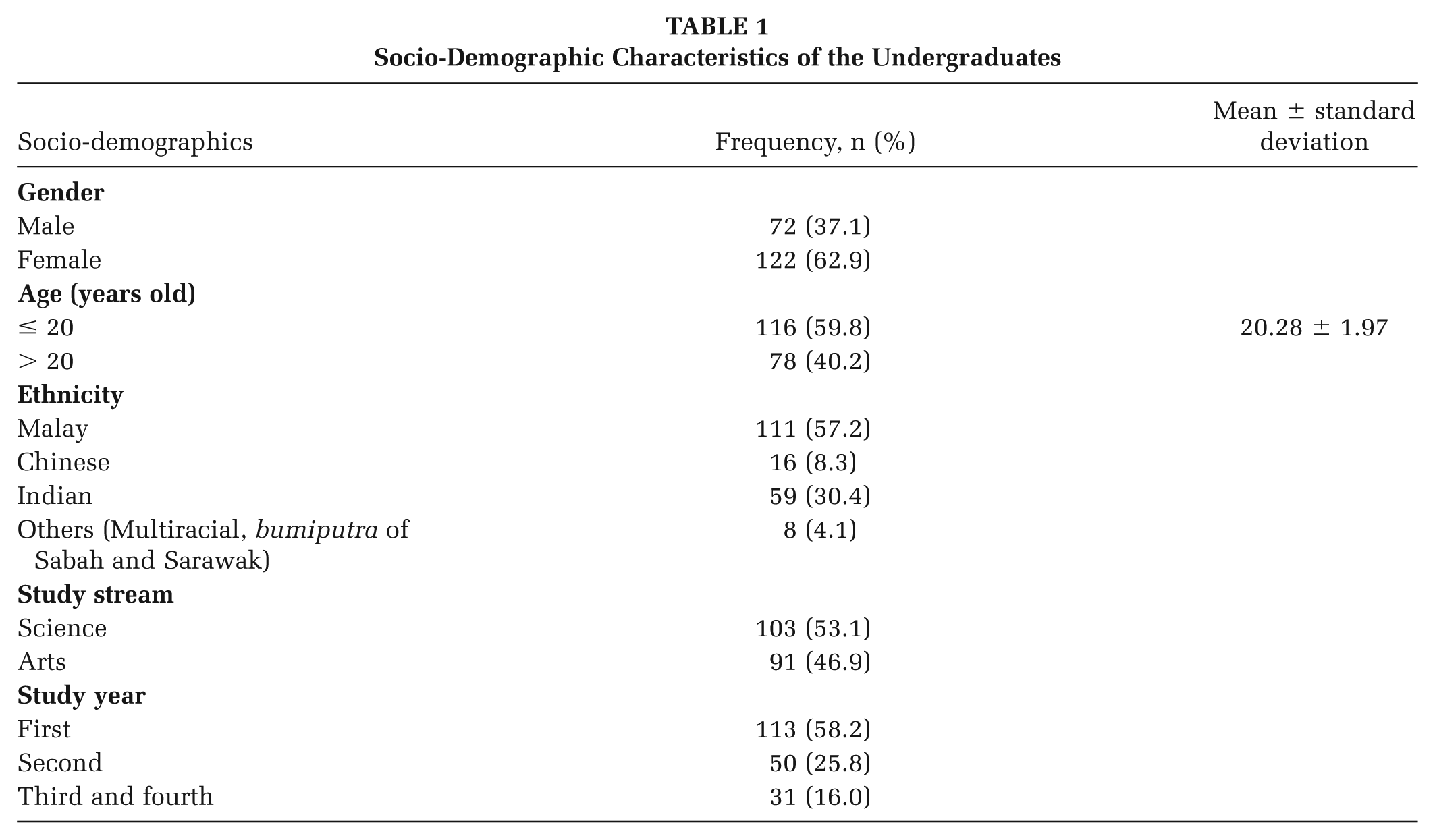
Table 1 shows the socio-demographic characteristics of the undergraduates. Of the 194 undergraduates who responded to all multiple-choice questions in both pre-intervention and post-intervention, the majority were female (n = 122, 62.9%), aged 20 years old or younger (n = 116, 59.8%), of Malay ethnicity (n = 111, 57.2%), studying in the science stream (n = 103, 53.1%), and first-year students (n = 113, 58.2%) at the time of data collection. Slightly more than four-fifths of the undergraduates (n = 160, 82.5%) were aware of the Malaysian Healthy Plate before the commencement of the peer-led educational intervention workshop.
Socio-Demographic Characteristics of the Undergraduates
The responses of all undergraduates to the nine multiple-choice questions at pre-intervention and post-intervention are tabulated in Table 2. It is worth noting that the top three most challenging questions at pre-intervention were: Question 2: “Which of the following measurements is the ideal plate size for portioning your food using the Quarter-Quarter Half (suku-suku separuh) concept?” (119 undergraduates or 61.3% answered incorrectly), Question 4: “What is the ideal portion of grains or starchy foods in the Malaysian Healthy Plate?” (96 undergraduates or 49.5% answered incorrectly), and Question 5: “What is the ideal portion of protein in the Malaysian Healthy Plate?” (89 undergraduates or 45.9% answered incorrectly). After attending the peer-led educational intervention workshop, it is notable that the proportion of undergraduates who answered these questions incorrectly reduced to 27.8% or 54 undergraduates for Question 2, 37.1% or 72 undergraduates for Question 4, and 33.0% or 64 undergraduates for Question 5. In general, the percentage of undergraduates who managed to answer each multiple-choice question correctly at post-intervention increased in the range of 8.2% (Question 1) to 33.5% (Question 2). It is also worth highlighting that the mean knowledge score was significantly improved (t = −8.003, p < .001) from 5.25 ± 2.58 at pre-intervention to 6.75 ± 2.30 at post-intervention (Figure 1).
The Responses From Undergraduates at Pre-Intervention and Post-Intervention

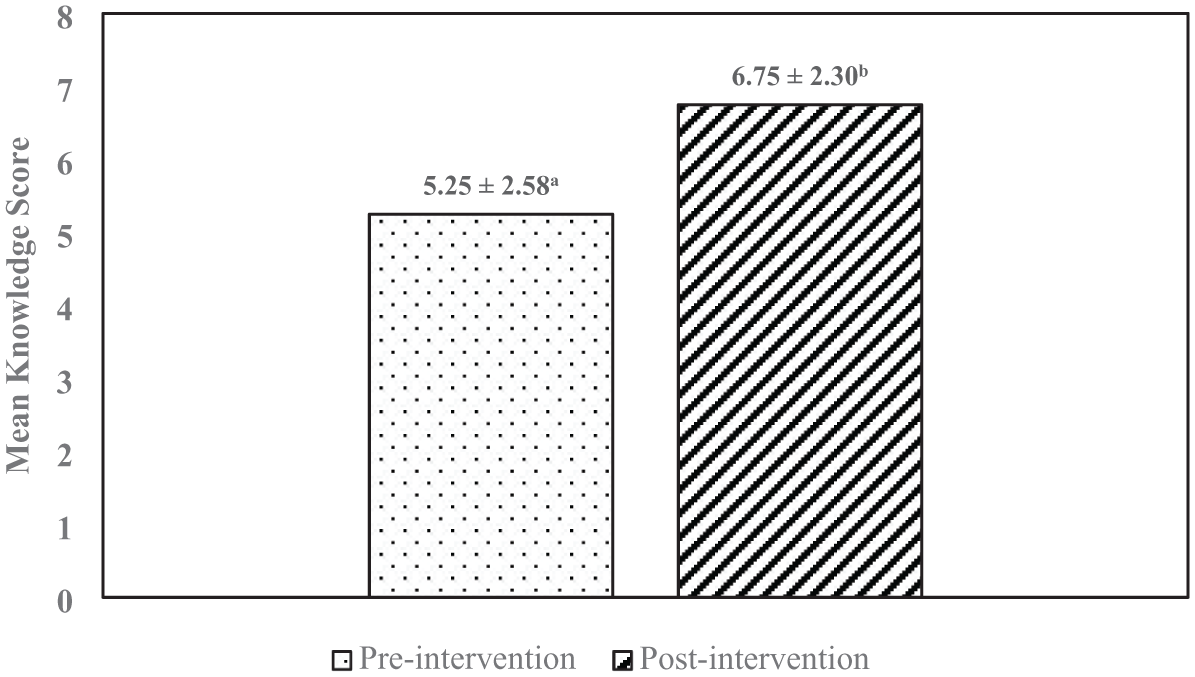
Comparison of the Mean Knowledge Scores at Pre-Intervention and Post-Intervention
Table 3 depicts the differences in the knowledge scores by socio-demographics and awareness of the Malaysian Healthy Plate before and after the intervention. Females (t = −2.256, p = .025), those studying in the science stream (t = 1.986, p = .049), and those aware of the Malaysian Healthy Plate (t = 2.297, p = .026) attained significantly higher knowledge scores compared to their respective counterparts at pre-intervention. Although the knowledge scores were still significantly higher among females (t = −2.567, p = .011) and those studying in the science stream (t = 2.434, p = .016), first-year students (F = 6.197, p = .005) recorded a significantly higher knowledge score compared to students in other study years at post-intervention.
Differences in the Knowledge Scores by Socio-Demographics and Awareness of the Malaysian Healthy Plate at Pre-Intervention and Post-Intervention

Significant difference was tested using a paired samples t-test.
Significant difference was tested using independent samples t-tests.
Significant difference was tested using one-way ANOVA.
Lower case denotes statistically significant at p < .05 within the same column.
Upper case denotes statistically significant at p < .05 within the same row.
Apart from those mentioned previously, the findings of the paired samples t-test revealed that the knowledge scores were significantly higher across gender (male: t = −4.825, p < .001, female: t = −6.359, p < .001), age (≤ 20 years old: t = −6.385, p < .001, > 20 years old: t = −4.804, p < .001), study stream (science: t = −5.953, p < .001, arts: t = −5.323, p < .001), and awareness of the Malaysian Healthy Plate (yes: t = −6.774, p < .001, no: t = −4.385, p < .001) at post-intervention compared to the pre-intervention. In terms of differences in the knowledge scores across ethnicity and study year, it is observed that Malays (t = −5.926, p < .001), Indians (t = −4.598, p < .001), first-year students (t = −6.536, p < .001), and third and fourth-year students (t = −5.658, p < .001) attained significantly higher scores at post-intervention compared to the pre-intervention. While there was a positive and significant correlation (r = 0.165, p = .021) between awareness and the mean knowledge score of the Malaysian Healthy Plate before the intervention, no significant correlation (r = 0.027, p = .708) was observed between awareness and the mean knowledge score of the Malaysian Healthy Plate after the intervention.
Discussion
The National Health and Morbidity Survey 2019 (NHMS 2019) previously uncovered that 79.6% of adults in Malaysia are unaware of the Malaysian Healthy Plate. Awareness of the Malaysian Healthy Plate appeared to be associated with the socio-demographic factors. Specifically, being female, belonging to the major ethnicities in Malaysia (Malay, Chinese, and Indian), having a tertiary education, and working in government sectors increased the likelihood of being aware of the Malaysian Healthy Plate (Mohamad Hasnan et al., 2023). In comparison to the statistics released by the NHMS 2019, only 17.5% or 34 undergraduates were reported to be unaware of the Malaysian Healthy Plate at pre-intervention. The high awareness of the Malaysian Healthy Plate (82.5% or 160 undergraduates) could be attributed to the fact that participants in the current study are active students at Management and Science University, where they can easily access information on the Malaysian Healthy Plate either within the institution or through browsing the internet.
The current findings indicate that slightly less than two-thirds (61.3%) of undergraduates were unaware of the recommended plate size, and nearly half incorrectly interpreted the ideal portion sizes for grains or starchy foods (49.5%) and protein (45.9%) as outlined in the Malaysian Healthy Plate concept before the commencement of the peer-led educational workshop. In Indonesia, a recent study by Jeslin and Astina (2023) indicated that 80% of young people aged 15 to 24 were unaware of the daily recommended portions of food and water, the guidelines for physical activity, and the consumption limits for sugar, salt, and fat. The proportion of undergraduates who misinterpreted portion sizes in this study is still lower than that of young people in Indonesia. Given that only 14.0% of adults in Malaysia are aware of and adhere to the Malaysian Healthy Plate concept daily (Institute for Public Health, 2020), it is not surprising that nearly half of the undergraduates in this study were unable to interpret portion sizes correctly.
Pre-intervention knowledge scores differed significantly by gender, age, study stream, and awareness of the Malaysian Healthy Plate. In contrast, post-intervention knowledge scores showed significant differences only by gender and study stream. Since females tend to have better nutrition knowledge, greater awareness of expert recommendations, are generally more health-conscious, and are more likely to engage in food-related decisions (Bärebring et al., 2020; Grunert et al., 2012; Loginova & Mann, 2024; Spronk et al., 2014), it is understandable that their mean knowledge scores were significantly higher than those of males. In addition, higher pre- and post-intervention knowledge scores among science stream undergraduates compared to those in the arts stream may be due to the inclusion of nutrition topics in the biology syllabus for science stream students during secondary school (Wan Mohamed Salleh et al., 2021). In general, these findings suggest that individuals with prior knowledge of nutrition (such as those studying in the science stream and being aware of the Malaysian Healthy Plate) attained significantly higher knowledge scores before and after the peer-led educational intervention.
A systematic review by St. Pierre et al. (2021) demonstrated that peer-led educational interventions are effective for improving nutrition-related behaviors (such as nutrition knowledge, knowledge of portion sizes, the adoption of healthy dietary patterns, fruit and vegetable consumption, and engagement in physical activity) in various settings. Overall, the findings of this study generally align with the literature mentioned above, in which the post-intervention knowledge score significantly increased by 28.6% compared to the pre-intervention knowledge score (Figure 1). Notably, undergraduates who were unaware of the Malaysian Healthy Plate prior to the peer-led educational intervention and those in their third and fourth years of study achieved more than a 50% increase in their knowledge scores at post-intervention (Table 3). The ability of undergraduates to answer each question correctly also improved by 8.2% for the question related to the key messages of the Malaysian Healthy Plate (Q1), by 12.4% to 33.5% for questions on portioning food groups (Q2–Q6), and by 13.4% to 23.8% for questions regarding portion sizes using hand measures (Q7–Q9; Table 2).
Several limitations need to be highlighted in the present study. First, the adoption of nutrition buddies or peer educators may result in variability in the quality of education provided. Although the nutrition buddies in the present study received training from the lead researcher (TST) before the educational intervention, it is worth noting that they are first-year nutrition students and may lack comprehensive knowledge of the Malaysian Healthy Plate. This could increase the risk of disseminating misleading information (Muddu et al., 2021). Second, as this study focuses only on the knowledge of the Malaysian Healthy Plate among undergraduates at one institution (Management and Science University), the findings may not be generalized to undergraduates in other Malaysian institutions. Third, the post-intervention knowledge assessment was conducted at only a single time point (specifically, immediately after the intervention). Therefore, this study does not provide insight into the long-term knowledge retention regarding the Malaysian Healthy Plate. Future research employing longitudinal designs with multiple follow-up assessments would be valuable in determining whether the knowledge gained is sustained over time. Despite those mentioned above, this study is still the first to adopt nutrition buddies or peer educators to improve the knowledge of the Malaysian Healthy Plate among undergraduates.
Conclusion
The findings of this study suggest that incorporating nutrition buddies into a peer-led educational intervention has significantly improved undergraduates’ knowledge of the Malaysian Healthy Plate. Despite the above-mentioned limitations, this approach may serve as a cost-effective way to raise awareness and potentially foster behavioral change in nutrition-related issues within educational institutions.
Implications for Practice
Health promotion practitioners should consider developing a mobile application to store all training materials and deliver ongoing reminders about the importance of practicing the Malaysian Healthy Plate. Such a platform can also share practical tips for healthy eating based on the Malaysian Healthy Plate, for instance, by including downloadable educational videos featuring cooking demonstrations that align with this concept. Furthermore, the above-mentioned mobile application could function as a test–retest tool by prompting participants to complete the same questionnaire at predetermined intervals (e.g., 1 month, 6 months, and 1 year) following the peer-led intervention, thereby allowing health promotion practitioners to assess knowledge retention over time.
Implications for Research
In addition to knowledge retention over time, future studies could explore whether the nutrition buddies enhances participants’ self-efficacy in applying the Malaysian Healthy Plate concept to daily meal planning. It is also equally important to assess whether improved knowledge and self-efficacy translate into actual and sustained dietary behavior changes, such as healthier food choices, accurate portioning, and consistent application of the Malaysian Healthy Plate in real-life settings. Assessing these outcomes may provide deeper insights into the program’s effectiveness in promoting long-term dietary behavior change.
The concept of nutrition buddies can be expanded by implementing a tiered system (or a “Train-the-Trainer” program), whereby senior nutrition buddies mentor and train their junior counterparts. This approach not only promotes the continuity and sustainability of the peer-led educational intervention but also fosters leadership skills among senior nutrition students. By adopting this tiered system, the intervention program could be scaled to various settings (such as among school-aged children and adolescents aged 7–17 years) to further disseminate knowledge of the Malaysian Healthy Plate.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399251382835 – Supplemental material for Incorporating the Concept of Nutrition Buddies to Improve the Knowledge of the Malaysian Healthy Plate: A Peer-Led Educational Intervention Approach
Supplemental material, sj-docx-1-hpp-10.1177_15248399251382835 for Incorporating the Concept of Nutrition Buddies to Improve the Knowledge of the Malaysian Healthy Plate: A Peer-Led Educational Intervention Approach by Seok Tyug Tan, Seok Shin Tan and Chin Xuan Tan in Health Promotion Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.