
Abstract
Training is a commonly used implementation strategy to prepare organizational change agents in a variety of settings. Online training has the potential for more efficient and cost-effective scale-up of evidence-based interventions, but in-depth analysis of training engagement, especially in settings such as churches, is lacking. This study reported engagement with and evaluation of an online training for churches in the national implementation study of Faith, Activity, and Nutrition (FAN), an evidence-based program that targets church practices. Churches (N = 107) from 23 U.S. states (74.8% predominantly African American) and 442 committee members enrolled. Church committees, led by FAN coordinators, registered for the eight-lesson online training. Regarding training engagement, committee members completed 4.8±3.7 of eight lessons, and most who started the training finished it. They posted 1.8±3.0 times on the discussion board. Lesson completion and discussion board posts were higher among FAN coordinators and women and those older and not employed (p <.05). Just below half (42%) of churches submitted a FAN program plan, with submission more likely when the FAN coordinator completed the training or when the pastor completed at least one lesson (p <.05). Furthermore, quantitative and qualitative data showed favorable evaluations of the online training. The absence of differences in training engagement by education and race and the more favorable associations with increased age are highly promising indicators that this training can be scaled up to reach diverse learners. FAN coordinators, however, may need strategies to engage other committee members to initiate training.
Keywords
In dissemination and implementation (D&I) research, engagement with implementation strategies is critical because these strategies influence implementation outcomes, which ultimately impact individual and population health outcomes (Bauer et al., 2015). Training is an implementation strategy often used to prepare practitioners within organizations (organizational change agents) to implement evidence-based interventions (Balis et al., 2022; Wandersman et al., 2008). Despite evidence supporting the effectiveness of this implementation strategy, in-person training can be resource-intensive and is often limited by geography (Ballew et al., 2013). Thus, to scale up evidence-based interventions, more flexible and cost-effective training formats are needed, such as online training (Ballew et al., 2013). Although studies have examined the impact of online training programs for organizational change agents in diverse settings (Florindo et al., 2018; Holt et al., 2019; Saunders et al., 2019; Schachtner-Appel et al., 2024; Yeary et al., 2021), detailed analyses are lacking regarding engagement and satisfaction with online training and associated factors. Furthermore, very little is known regarding engagement with online training in settings where health-related mandates generally do not exist, such as churches (Mazzucca et al., 2021).
Our study addresses significant gaps identified in reviews of D&I research (Larsson, 2024; Mazzucca et al., 2021). Recommendations based on these gaps include focusing on health equity, identifying ways to shorten the uptake of research into practice, providing diverse training formats to enhance professional development and capacity building, using pragmatic methods, and conducting research in community settings where the primary mission is not health services delivery, including faith-based organizations. We have focused on training churches to create healthier church environments. Churches are present in nearly all communities and offer ways to reach populations with high risk of chronic disease and high rates of religious participation, including African Americans and older adults (Pew Research Center, 2015). There is also a long history of public health partnerships with Black churches for community-level health promotion (Brewer & Williams, 2019). Yet, evidence-based interventions with potential for scale-up in the faith-based setting are lacking. For example, a recent review of evidence-based interventions identified only six interventions that met various criteria, including being able to address health disparities and being easily accessible to churches, yet none included online training (Jones et al., 2025). It is also unclear whether online training for church-level health promotion would be well-received by potential change agents in this setting, most of whom are lay leaders. Our team engaged in a systematic process to convert an in-person training for the evidence-based Faith, Activity, and Nutrition (FAN) program to an online format, with high levels of training completion and favorable rating observed in our small pilot study (n = 9) (Wilcox et al., 2023). This preliminary work laid the foundation for conducting a national implementation study.
Purpose
This paper provides an in-depth analysis of engagement with the key implementation strategy of FAN, namely the online training of church committees. The goals of the current paper were to (1) report church committee engagement with the training, defined as completing lessons, posting on the online discussion board, and submitting a 12-month implementation program plan; (2) examine factors associated with training engagement; and (3) report how church committees evaluated the training program, using quantitative and qualitative data. Strengths and innovations of the study include the large sample and diversity of churches and the focus on organizational practices (vs. individual behaviors). Findings have great potential for informing training in evidence-based health promotion programs in the faith-based setting.
Method
Procedures
This national implementation study used a quasi-experimental design in which churches were recruited to take part in the online training to prepare them to implement the FAN program. The University of South Carolina Institutional Review Board reviewed and approved the study protocol and deemed it exempt. As reported in more detail elsewhere (Wilcox et al., 2024), we formed a Community Advisory Board of faith, health, academic, and economic development representatives who helped guide all study activities. We also formed a group of translation partners, comprised of faith and health representatives, who provided ideas for reaching churches and shared recruitment materials through their networks. Recruitment strategies included flyers, brochures, and a website shared with partners; emails to partners; cold contact emails to other faith-based networks or health-related organizations with ties to churches; telephone contacts; study presentations; social media and e-media stories and advertisement; and word of mouth.
Interested churches completed an online interest form, and in response, the study project coordinator emailed additional information about FAN and study participation. Research staff communicated via email and telephone to ensure churches understood what participation entailed and to assist them in identifying their FAN coordinator (i.e., the person who served as liaison with the research team and coordinated training and implementation efforts in their church). While we prioritized churches with predominantly African American congregations, participation was open to any U.S. church if the pastor provided approval and support to participate, if the pastor and FAN coordinator agreed to complete evaluation surveys at baseline and 12 months, and if they agreed to form a church committee.
Once a church indicated its intention to enroll in the study, and 5 weeks before we released the first online training lesson to the cohort, we initiated online baseline surveys. Baseline surveys occurred between August 2020 (Cohort 1) and December 2022 (Cohort 10). When the pastor and FAN coordinator completed their surveys, we shared a link to a brief online survey for the remaining church committee members. Baseline data are reported in this paper.
Intervention
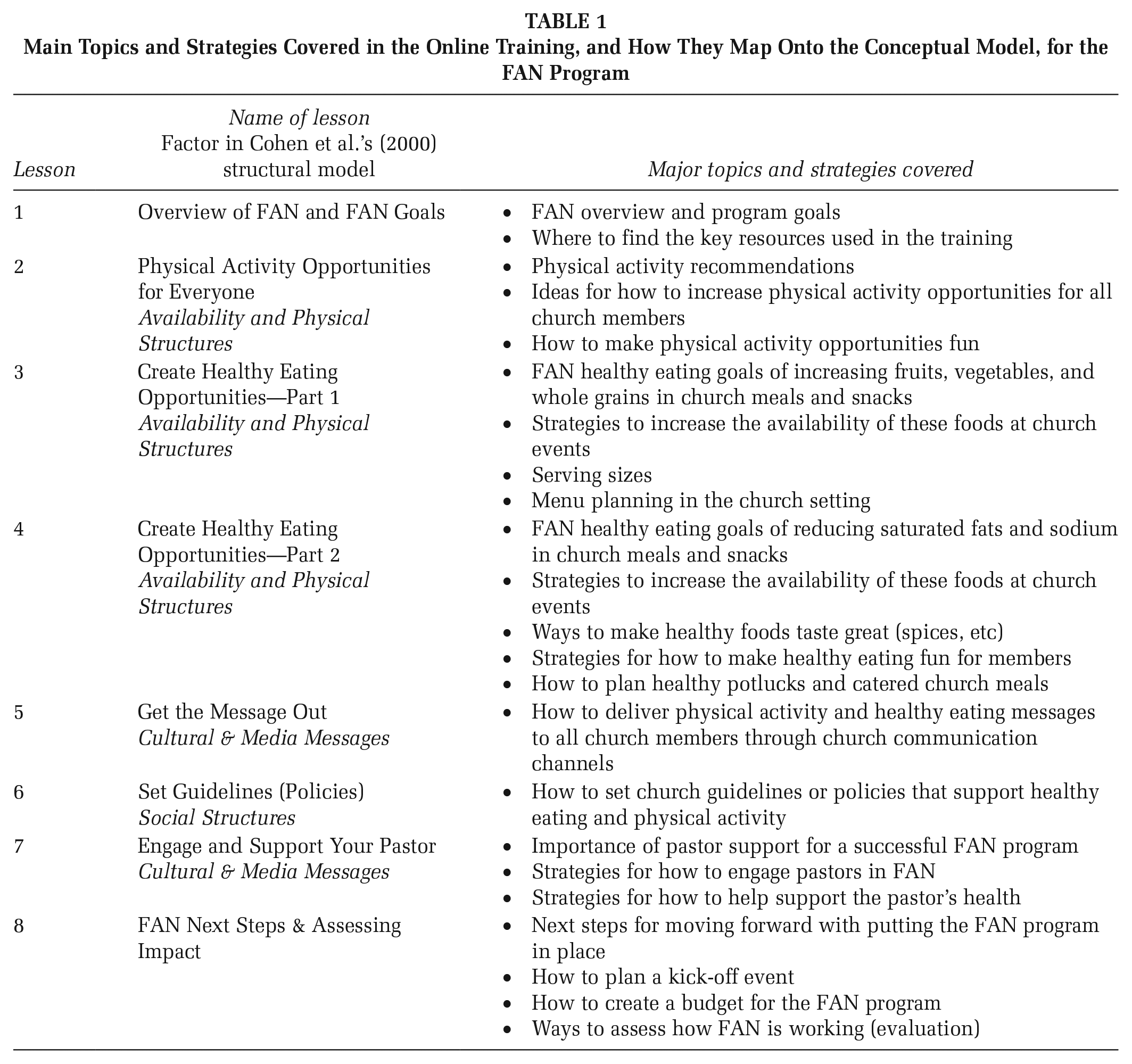
The FAN program was developed using a community-based participatory research process (Wilcox et al., 2010). The program training covered physical activity and healthy eating basics and recommendations, and church committees were trained to implement four core components related to physical activity and healthy eating based on factors from a structural model of health behavior (Cohen et al., 2000): (1) increase opportunities, (2) set policies, (3) share messages, and (4) enlist pastor support. In previous studies (Wilcox et al., 2010, 2018, 2021), church committees attended an in-person training. To increase the intervention’s reach, we converted the training to an online format in an iterative process (Wilcox et al., 2023). The content of the training and how the intervention components map onto factors from the structural model are shown in Table 1.
Main Topics and Strategies Covered in the Online Training, and How They Map Onto the Conceptual Model, for the FAN Program
We used the online learning management system Moodle to house the online training. The training site included the eight lessons; a knowledge check (10 items), feedback survey, and resources for each lesson; 12 months of materials to support implementation (monthly newsletter, bulletin insert, and resources related to physical activity, diet, and behavior change); and an online discussion board. Because recruitment began during the COVID-19 pandemic, we developed a guide with examples of activities that could be done if churches were meeting virtually. Access to the first online training lesson required watching two brief orientation videos and posting an introduction on the discussion board. We released one lesson each week with learner access restricted pending completion of the prior week’s lesson, receipt of a satisfactory score on the knowledge check (≥80% with opportunities to retake), and completion of the lesson feedback survey (used for formative purposes). Learners could not advance through the lesson without completing all lesson activities. The final slide in each lesson included an internal trigger that recorded lesson completion and returned the learner to the knowledge check and feedback survey.
Each lesson encouraged committee members to collaborate to draft portions of a program plan that outlined their plans for implementing the core intervention components over the next 12 months. The plan used simple and customizable templates that enabled them to choose or create activities best suited to their congregation. After training, research staff prompted churches to finalize the program plan and upload it to Moodle or email it to the study coordinator, who provided feedback.
Over the next 12 months, the study coordinator moderated the discussion board by posting reminders to review and utilize the monthly materials, sharing holiday greetings, and replying with encouragement or technical assistance. At Month 11, we encouraged churches to create a revised program plan for the next 12 months.
Study Measures
Training Engagement
Training engagement was operationalized as lesson completion, discussion board posts, and submission of a 12-month program plan. We calculated the number of lessons completed out of eight. Lesson completion was defined as completing seven or eight lessons because all core components of FAN were covered in the first seven lessons. All posts to the discussion board were downloaded, and the number of posts for each committee member was tallied. Because learners were required to post an introduction on the discussion board to get access to the first lesson, we focused on those who posted two or more times. Finally, the study coordinator documented the submission of the church’s program plan.
Influences on Training Engagement
We used the Consolidated Framework for Implementation Research (CFIR) (Damschroder et al., 2009) to guide our examination of influences on FAN adoption (Wilcox et al., 2024) and implementation fidelity (Wilcox et al., 2025). The CFIR, one of the most widely used implementation science frameworks, is well-suited to our study goal of examining multilevel influences on implementation outcomes in the church setting. The five CFIR domains are characteristics of the intervention, inner setting, outer setting, characteristics of the implementers, and implementation process. We examined a small number of constructs from two CFIR domains for their association with training engagement.
Church characteristics mapped onto the “structural characteristics” construct from the CFIR’s inner setting domain. Variables from this construct were faith tradition, geographical region, predominant race of congregation, congregation size, and presence of a health ministry. We categorized denominations into faith traditions based on responses to online interest forms (e.g., African Methodist Episcopal [AME] and United Methodist Church [UMC] were classified as “Methodist”). We categorized churches into geographical regions of the U.S. (Southeast, Northeast, Midwest, Southwest, West). Churches with ≥80% of the congregation reported as a given race/ethnicity were categorized as that race/ethnicity; otherwise, the church was classified as multiracial. Respondents reported how many people attended worship service(s) each week: 1–19, 20–99, 100–499, or 500+. Finally, respondents reported whether their church had an active health ministry, defined as “a recognized team of people who sponsor regular educational events and experiences that promote well-being.”
Church committee member characteristics mapped onto the “other personal attributes” constructs from the CFIR’s characteristics of the implementers domain. Variables from this construct were age, gender identity, race, ethnicity, level of education, and employment status; whether the FAN coordinators had a degree or certificate in a health-related field; and whether FAN coordinators led or co-led health promotion efforts in their church or elsewhere in the past 12 months.
Training Evaluation
At the end of the final lesson, participants evaluated the training with 10 items, including three open-ended questions (see Supplemental Material). We used two comprehensive models of online training evaluation to develop these items. First, Ballew et al.’s (2013) model has two main categories (and recommended criteria within each) for evaluating online trainings. Second, the Multidimensional Conceptual Model for Evaluating E-learning System Success (Al-Fraihat et al., 2020) consists of seven independent and four dependent constructs. The study team identified a pool of items used in other studies or recommended for evaluating online trainings and e-learning. We categorized each item according to the criteria for evaluating web-based training effectiveness from Ballew et al. (2013) and the construct(s) from Al-Fraihat et al. (2020). We reworded items as needed to match our study context or to provide uniformity and solicited input on items from our Community Advisory Board.
Analyses
Quantitative Analyses
We used means and frequencies to describe training engagement. We examined committee member characteristics that predicted lesson completion and discussion board posts as well as church and FAN coordinator characteristics that predicted program plan submission with multivariate simultaneous logistic regression models. Finally, we reported means for the training feedback items and, using analysis of variance (ANOVA), whether means differed by committee role.
Qualitative Analyses
We used content analysis to identify categories and patterns (Strauss & Corbin, 1998). Three team members read the committee members’ open-ended comments for the training and generated question-specific codes to capture the range of responses. Two of these team members and the study PI developed a codebook with definitions. Two team members independently coded all responses and met to reach consensus where there were disagreements.
Results
Church and Committee Member Characteristics
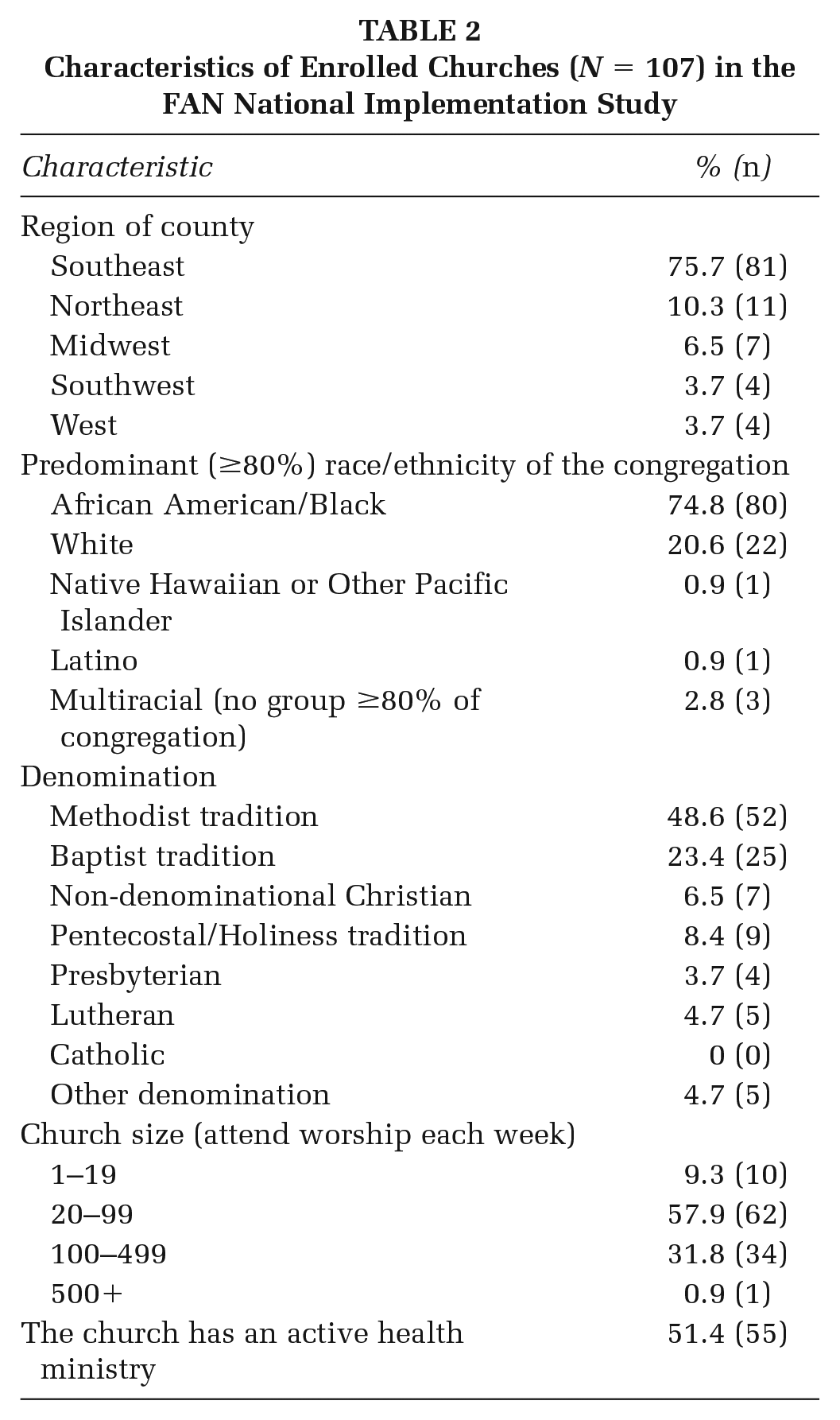
Churches (N = 107) from 23 U.S. states enrolled in the study. Church characteristics, as reported previously (Wilcox et al., 2024), are shown in Table 2. Two churches in the sample were served by the same pastor. In addition, in four churches, the pastor served as the FAN coordinator (they were classified as FAN coordinators in all analyses).
Characteristics of Enrolled Churches (N = 107) in the FAN National Implementation Study
A total of 442 committee members from these churches registered for the online training, with an average committee size of 4.1±2.0 members. Of these committee members, 107 were FAN coordinators, 80 were pastors (excluding 4 pastors who were also FAN coordinators), and 255 were other committee members (see Table 3).
Characteristics of Committee Members Who Registered for the Online Training, Overall and by Committee Role
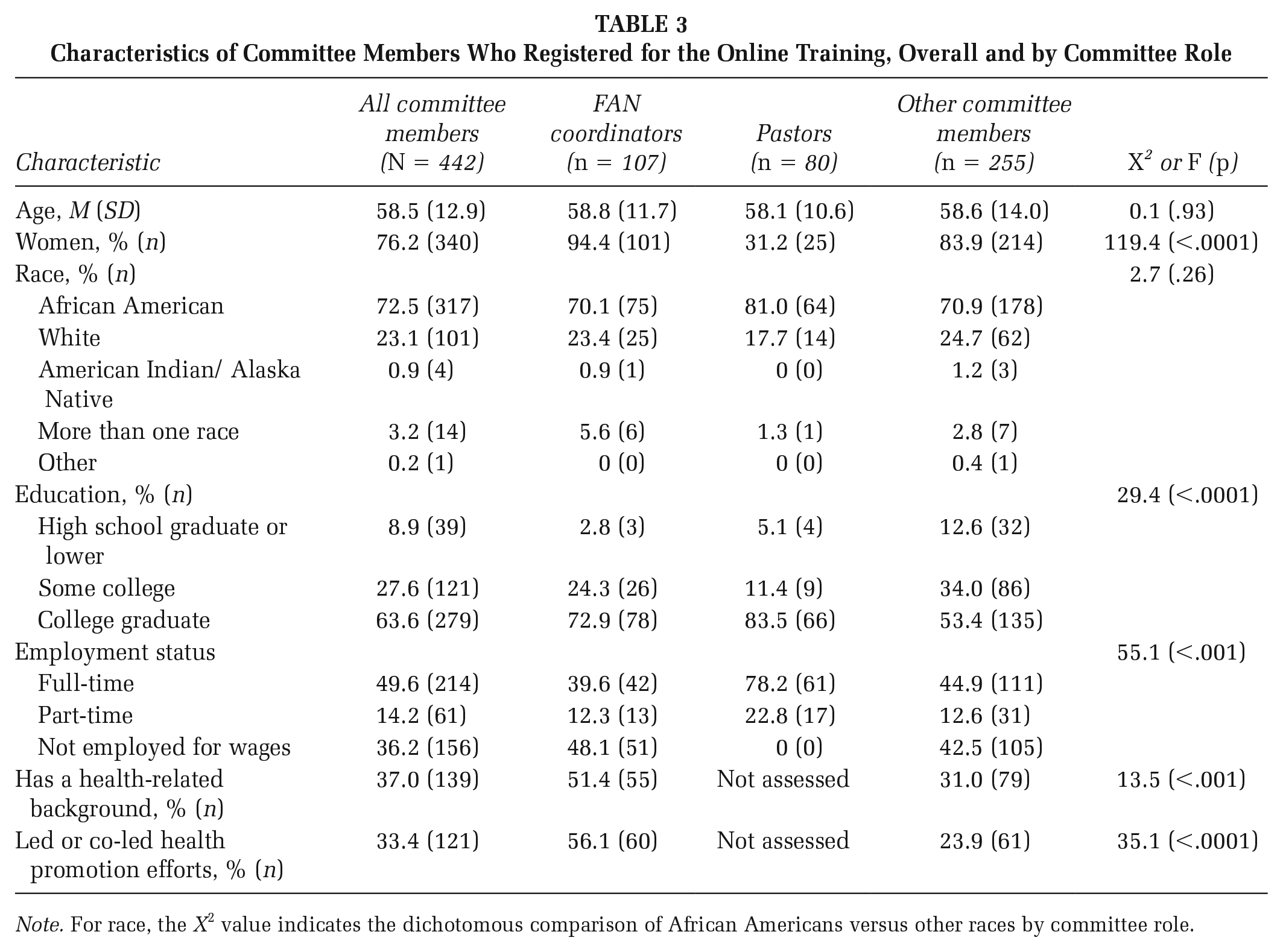
Note. For race, the X2 value indicates the dichotomous comparison of African Americans versus other races by committee role.
Training Engagement
Lesson Completion
Committee members completed 4.8±3.7 of eight training lessons (6.6±2.8 for FAN coordinators, 2.3±3.4 for pastors, 4.8±3.7 for other committee members; see Table 4). Close to one-third completed zero lessons, whereas just over half completed seven or eight lessons (79.5% of FAN coordinators, 25.0% of pastors, 56.5% of other committee members). The simultaneous logistic regression model (see Table 5) predicting lesson completion from committee member characteristics was statistically significant, χ2(6, N = 423) = 77.80, p <.0001. Lesson completion was greater in FAN coordinators versus other committee members (p <.0001) and in women versus men (p <.01), and was lower in pastors versus other committee members (p <.0001). Age was positively associated with lesson completion (p <.01). Education and race were not associated with lesson completion. Due to the collinearity between employment status and age, we excluded employment status in the simultaneous model.
Training Engagement and Lesson Completion, Overall and by Committee Role
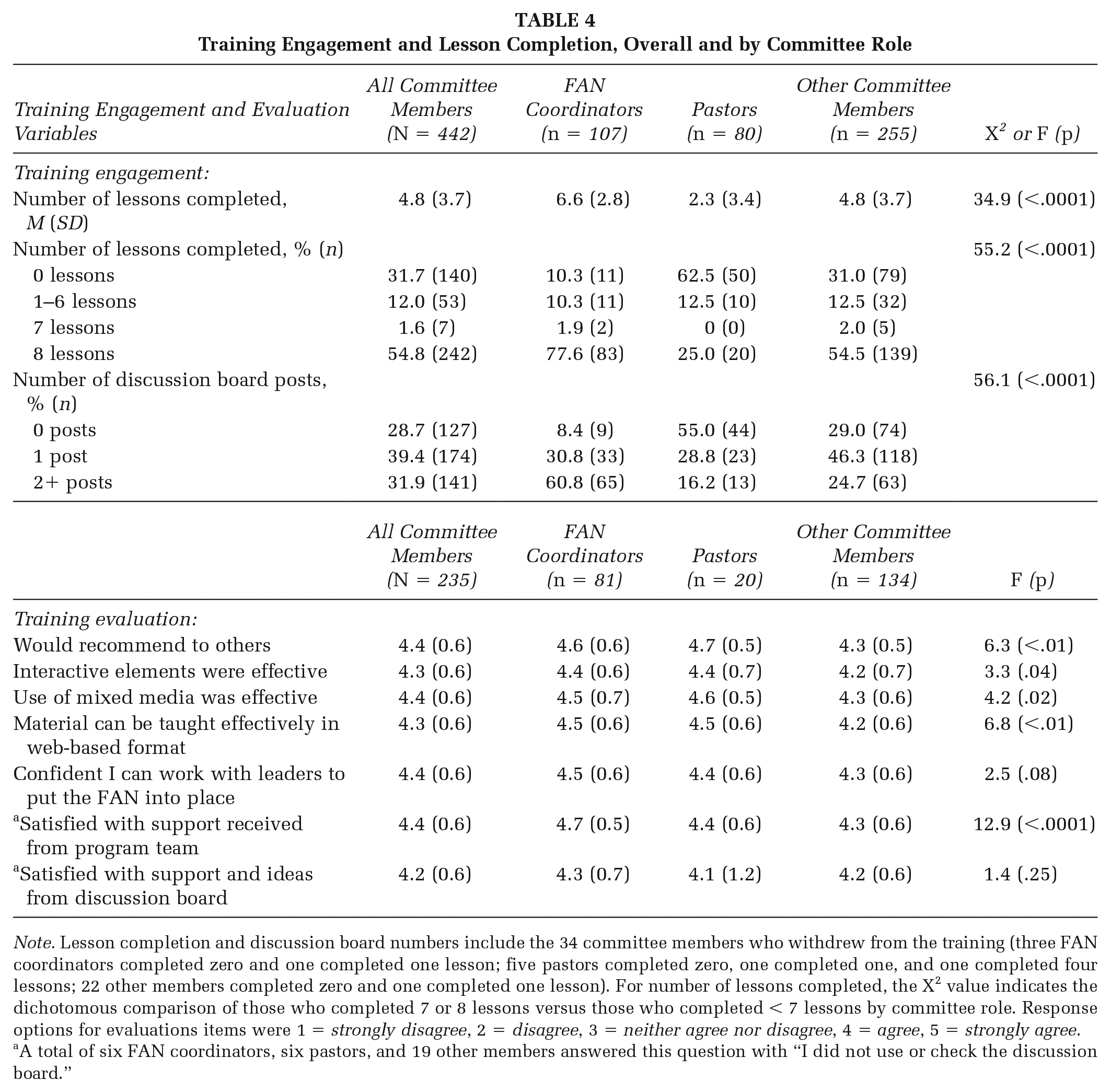
Note. Lesson completion and discussion board numbers include the 34 committee members who withdrew from the training (three FAN coordinators completed zero and one completed one lesson; five pastors completed zero, one completed one, and one completed four lessons; 22 other members completed zero and one completed one lesson). For number of lessons completed, the X2 value indicates the dichotomous comparison of those who completed 7 or 8 lessons versus those who completed < 7 lessons by committee role. Response options for evaluations items were 1 = strongly disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, 5 = strongly agree.
A total of six FAN coordinators, six pastors, and 19 other members answered this question with “I did not use or check the discussion board.”
Results of Simultaneous Logistic Regression Models Predicting Training Engagement Outcomes
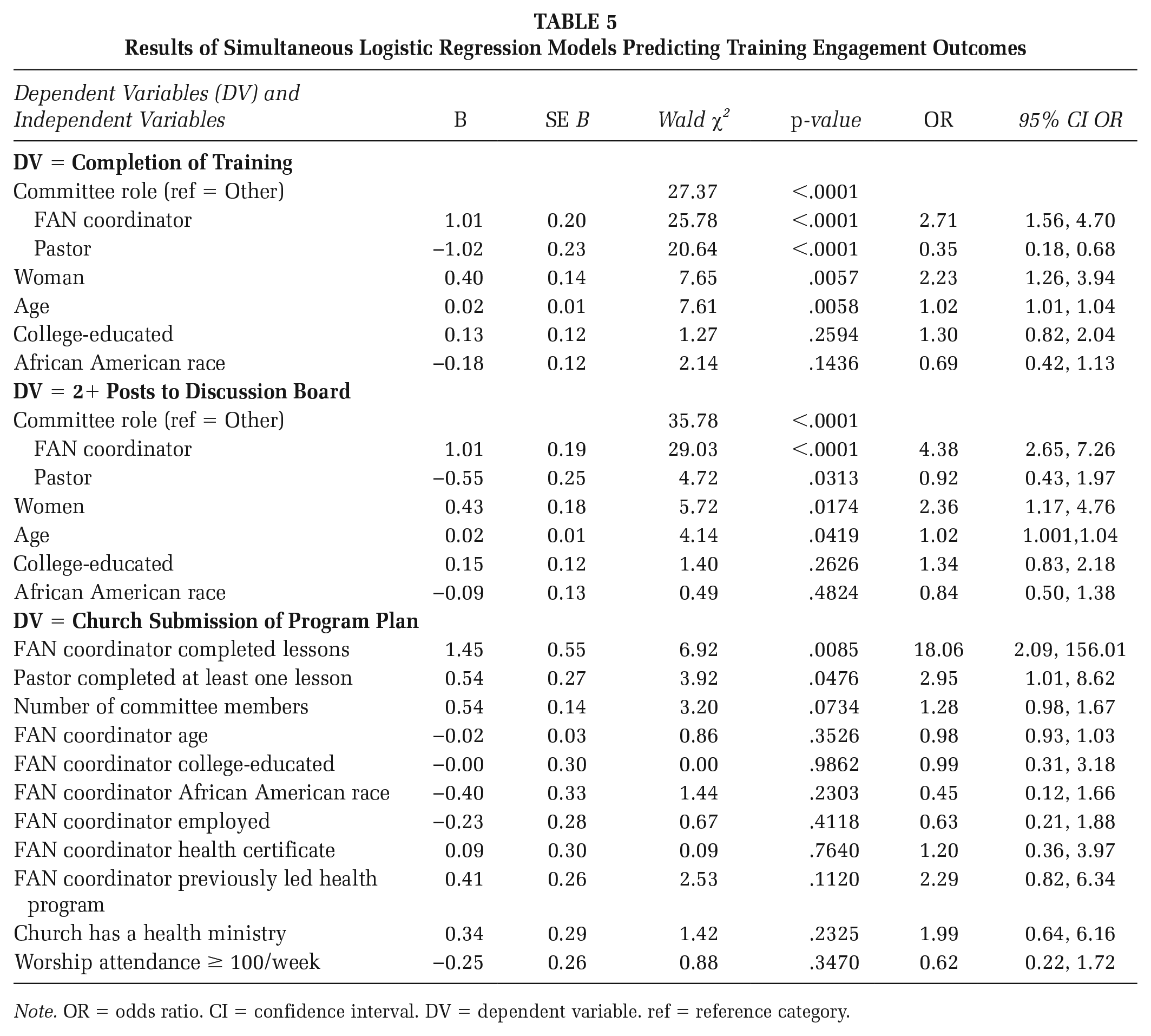
Note. OR = odds ratio. CI = confidence interval. DV = dependent variable. ref = reference category.
Discussion Board Posts
The average number of discussion board posts was 1.8±3.0 (range: 0–31), with 28.7% having 0 posts, 39.4% having 1 post, and 31.9% having 2 or more posts (Table 4). The simultaneous logistic regression model (see Table 5) predicting discussion board posts from committee member characteristics was statistically significant, χ2(6, N = 423) = 64.94, p <.0001. Posting 2+ times was greater among FAN coordinators versus other committee members (p <.0001) and in women versus men (p <.05), and was lower in pastors versus other committee members (p <.05). Age was positively associated with posting 2+ times (p <.05). Education and race were not associated with discussion board posts.
Program Plan Submission
FAN coordinators from 45 of the 107 churches (42%) submitted a FAN program plan. The simultaneous logistic regression model (see Table 5) predicting program plan submission from church and FAN coordinator characteristics was statistically significant, χ2(11, N = 104) = 36.4, p <.0001. FAN coordinator completion of training (p <.01) and pastor completion of at least one lesson (p <.05) were significantly associated with submitting a program plan. Because FAN coordinator training completion was highly related to the average number of lessons completed by the committee members (r = .69, p <.0001), we only used FAN coordinator training completion in the regression model. FAN coordinator age, race, employment status, education level, having a health-related background, having previously led or co-led a health promotion program, presence of a health ministry in the church, and church size were unrelated to program plan submission.
Training Evaluation
Quantitative Data
Committee members’ ratings of the training items ranged from 4.2±0.6 to 4.4±0.6 out of 5 (Table 4). FAN coordinators and pastors were significantly more likely to agree that they would recommend the training to others than other committee members. FAN coordinators were more likely than other committee members to agree that the interactive elements of the lessons were effective and that the training material could be taught effectively in a web-based format. Finally, FAN coordinators were more likely than both pastors and other committee members to agree that they were satisfied with the support they received from the FAN program team.
Qualitative Data
Committee members frequently noted that they liked the online format that made the training convenient and flexible, the clear and organized way the information was presented, how later lessons built on previous lessons, how lessons could be completed in a relatively short period of time, and the ability to go back and replay content. They also liked the information and ideas presented, described the training as very informative and helpful, and appreciated the many suggestions and ideas as well as practical examples from previous FAN churches. The program resources and materials were cited by many as very helpful and easy to access and use. Committee members enjoyed the physical activity videos, found the church videos and testimonials helpful and encouraging, described the potential that the training had for promoting health in their congregations (e.g., oh the possibilities for a healthier church), and shared that the training was easy to use and easy to follow.
The most common response to what committee members liked least was either nothing or they made a positive comment (e.g., it is all good). Training format and technical difficulties were cited by some. Regarding format, some committee members would prefer to complete the lessons all at once (i.e., not one per week), and others did not like that they could not skip content or videos. Some found the training pace to be too slow or a little repetitive, and others found some lessons too lengthy. Regarding technical difficulties, some committee members found the lessons confusing to navigate or the training site confusing, although this challenge decreased over time. Others described video glitches, or they had difficulty advancing in a lesson. They spoke positively about the support received by the research team to help them with challenges.
The most common response to the final open-ended question, whether they had anything else they wished to share about the FAN online training program, was a positive statement such as expressing gratitude for the program (e.g., thank you for this wonderful ministry!), making global statements about the program being excellent or great, or expressing excitement for bringing FAN to their congregation.
Discussion
A key finding from this unique national implementation study was that the FAN online training program was positively received, and most committee members who started the training completed it. FAN coordinators, who served as liaisons to the study team and oversaw their church committees, had the highest rates of training engagement—they were the most likely to complete the training lessons and post to the discussion board, and rate the training most favorably. We also found that churches most likely to submit a program plan were those in which the FAN coordinator completed the training and the pastor completed at least one lesson.
Despite their promise to promote health equity and broad reach, evidence-based programs that can be scaled up in faith-based settings are rare (Jones et al., 2025). We identified two studies that used web-based/online training to prepare community health workers to implement health promotion activities in the faith-based setting. Yeary et al. (2021) found that those trained online (n = 9 participants) to deliver the Diabetes Prevention Program had comparable satisfaction and knowledge scores as those trained in-person (n = 10 participants). In a series of studies for Project HEAL (Holt et al., 2015, 2019; Santos et al., 2014, 2017), the authors reported comparable implementation outcomes for cancer prevention workshops from their web-based training (n = 6 churches) as compared with their traditional in-person training (n = 8 churches). Our national implementation study reached a large and diverse sample of churches from 23 states across the United States. We used an online learning management system to house the training, which allowed us to collect objective measures of training engagement for each committee member.
Completion of online training for practitioners has been reported in other settings, including early childhood education (63%–68% completed the course) (Bruijns et al., 2022), preschools (73% of teachers who began the training completed it) (Kennedy et al., 2017), and health care (22.6% accessed the final module) (Florindo et al., 2018). Our training completion (78% of FAN coordinators, 25% of pastors, and 54% of other committee members) appears to fall within this range. This finding is important because church committees do not have professional mandates for continuing education. FAN coordinators, women, and older committee members were significantly more likely to complete the online training and post 2+ times to the discussion board than their counterparts. The higher level of engagement among FAN coordinators is consistent with research in other settings that demonstrates the importance of a champion for implementation success (Miech et al., 2018; Santos et al., 2022). The positive association between committee member age and both training completion and discussion posts suggests that age is not a limiting factor in online training programs, even among a sample with a mean age of just below 60 years. Similarly, the lack of associations between both education and race with training engagement indicates that the online format was not necessarily a barrier for subgroups with sociodemographic risk factors. In this study, pastor participation in training was encouraged but optional. While 80 of the 103 pastors expressed an interest in completing the training, very few did, likely due to time constraints, especially for bi-vocational pastors (Corbie-Smith et al., 2010).
We also examined church and FAN coordinator characteristics that predicted the submission of a program plan, an activity shown to predict greater implementation of several of the key intervention components in an earlier study (Saunders et al., 2022). In this study, 57% of churches submitted a program plan (Saunders et al., 2022), higher than in the present study (42%). Churches were more likely to submit a plan when the FAN coordinator completed the training and the pastor completed at least one lesson. Neither the characteristics of the FAN coordinator nor of the church were related to plan submission. Training engagement may reflect church dynamics, committee functioning, mission alignment, and/or church capacity.
Finally, the highly favorable quantitative and qualitative evaluations of the online training were consistent with our small pilot study (Wilcox et al., 2023). The qualitative responses to open-ended questions were heavily weighted toward positive training evaluations, including its format, information, and resources provided, use of videos and testimonials, the potential for improving the health of their congregation, and ease of use. A few committee members noted aspects of the training they did not like or made suggestions, which is valuable feedback for future program modifications.
Limitations
This study has several limitations. First, churches from the Southeast and those with Methodist and Baptist traditions were disproportionately represented. Results may not generalize as well to churches from other geographical areas of the United States or to all denominations. Our existing partnerships (many in the Southeast) were most fruitful in recruiting churches. We did not have an adequate sample size to examine regional, denominational, or cultural differences in training. In addition, nearly one-third of participants completed no training lessons. The lesson and training evaluation data are likely biased toward more favorable ratings as they were completed by committee members who completed the entire training and thus may have been more interested and engaged. Furthermore, we assessed training engagement through metrics such as lesson completion. Although participants had to pass a knowledge test to proceed to the next lesson, we do not have other comprehension data to indicate skill acquisition or other markers that could impact implementation fidelity. Finally, the lack of in-depth qualitative data was a study limitation. Although we collected open-ended data regarding participants’ responses to the lessons, the study would have benefited from a richer insight into barriers and facilitators to training completion, comprehension, and ultimately implementation.
Implications for Practice
Our findings indicate that carefully developed online training for evidence-based health promotion programs can engage faith-based committees, and participation does not appear to be limited by age, race, or education. Training engagement, especially by FAN coordinators, was high, and the training was rated favorably. Most committee members who started the training completed it. Nonetheless, a sizable proportion of committee members completed no lessons. It might be helpful to train FAN coordinators, who serve as organizational change agents, in the importance of and strategies to engage, encourage, and motivate other committee members to complete the training. For example, completing the training as a team, incentivizing lesson completion, and scheduling meetings to discuss each week’s training lesson might facilitate training completion. The inclusion of interviews and qualitative analyses in future research might also inform barriers to lesson completion and supports needed by committee members. Finally, although this study was conducted in churches, FAN’s intervention framework and the online training were based, in part, on an online training for preschool teachers (Saunders et al., 2019), suggesting that online training for organizational change agents is likely feasible in a wide range of organizational settings.
Implications for Policy
To scale up evidence-based interventions in the faith-based and other community sectors, infrastructure and incentives are necessary. Although most of the costs associated with implementing FAN are related to human resources at the church (i.e., time), typically provided by church volunteers with an interest in health, infrastructure is needed to house and offer the training, as well as provide any necessary assistance in accessing it. Furthermore, incentives to complete training could be useful to encourage participation in community settings.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399251362162 – Supplemental material for Church Committee Engagement in and Evaluation of an Online Faith-Based Training in a National Implementation Study
Supplemental material, sj-docx-1-hpp-10.1177_15248399251362162 for Church Committee Engagement in and Evaluation of an Online Faith-Based Training in a National Implementation Study by Sara Wilcox, Ruth P. Saunders, Jasmin Parker-Brown, Andrew T. Kaczynski, Jessica Stucker, Deborah Kinnard, Kelsey R. Day and Caroline Rudisill in Health Promotion Practice
Footnotes
Authors’ Note:
We thank our Community Advisory Board and translation partners for their support in recruiting churches and guiding study activities. We are grateful to all the churches for their participation. We also thank Brent Hutto for his statistical support and guidance and Jenna Dzwierzynski for her assistance in coding open-ended responses. This work was supported by Cooperative Agreement Number U48DP006401 from the Centers for Disease Control and Prevention. Its contents are solely the authors’ responsibility and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.