
Abstract
Expanding access to pre-exposure prophylaxis (PrEP) is crucial for ending the HIV epidemic in the United States and reducing disparities in HIV incidence among marginalized populations. Telehealth models for the delivery of PrEP have the potential to improve access, acceptability, and adherence. In 2022, Philadelphia established the Philadelphia TelePrEP Program to deliver HIV prevention services through telehealth. This qualitative descriptive study aims to identify implementation determinants for telehealth PrEP services in Philadelphia. We completed nine in-depth interviews with staff at the Philadelphia TelePrEP Program (n = 5) and external stakeholders in the HIV prevention workforce (n = 4) using a semi-structured interview guide based on the Consolidated Framework for Implementation Research (CFIR). Thematic analysis was used to identify key facilitators and barriers to implementation. Interviews revealed that telePrEP improved convenience and flexibility in accessing PrEP, but online marketing may exclude certain populations with limited digital presence. Dedicated patient navigators and ongoing staff training were key facilitators, whereas limited provider capacity was a challenge. Sustainable funding through grants and 340B revenue enabled the Philadelphia TelePrEP Program to serve uninsured patients. The digital divide, lack of PrEP awareness, and competition from commercial telePrEP providers were identified as potential barriers to engaging priority populations. TelePrEP has the potential to expand the availability of PrEP services and reach communities that currently face barriers to access. However, overcoming key structural and social barriers around public awareness, technology access, and organizational capacity will be critical for successful implementation.
Nationally, progress toward the goal of reducing HIV incidence set out in the plan to end the HIV Epidemic in the United States has been slower than expected (Centers for Disease Control and Prevention, 2022, 2023). Pre-exposure prophylaxis (PrEP) is a highly efficacious tool for HIV prevention that is a key pillar of the national plan given its effectiveness in reducing HIV incidence at the population level (Smith et al., 2020; Sullivan et al., 2024). Although PrEP was approved for use in the United States in 2012, only recently have a significant portion of those indicated for PrEP gained access to the medication, with 36% of eligible individuals being prescribed PrEP in 2022, up from 18% in 2018 (Centers for Disease Control and Prevention, 2020, 2022). Despite this progress, substantial disparities in PrEP access by race, gender, and region have persisted due to a mire of structural and social barriers (Pinto et al., 2018). Specifically, Black and Latinx individuals experience a disproportionate burden of HIV, yet have accessed PrEP at lower rates than White individuals (AIDSVu, 2023). To address these persistent disparities, it is crucial to understand and address the various barriers that hinder PrEP uptake among underserved communities.
Structural and health systems-level barriers have hindered access to PrEP, including limited appointments with PrEP providers (Laborde et al., 2020), discrimination within health care systems (Quinn et al., 2019), and logistical challenges related to transportation and scheduling (Rice et al., 2019). These obstacles disproportionately affect marginalized populations, particularly racial and ethnic minority communities, who have fewer clinics offering PrEP services in their areas and may face concerns about confidentiality, stigma, and potential discrimination in health care settings (Kimball et al., 2020; Ojikutu et al., 2018; Siegler et al., 2018; Watson et al., 2022; Wood et al., 2019). The limited geographical availability of PrEP providers, with nearly 20% of PrEP-eligible men who have sex with men living at least 30 minutes away from the nearest provider, has posed significant challenges (Siegler et al., 2019). Telehealth delivery of PrEP services represents a promising strategy to expand PrEP availability and address access barriers by mitigating transportation, scheduling, and availability constraints while addressing concerns related to stigma and confidentiality (Bonett, Li, et al., 2024; Giorlando et al., 2023; Patel et al., 2022).
In 2022, the City of Philadelphia launched the Philadelphia TelePrEP Program (PTP), a telehealth model for HIV prevention that aims to improve access and adherence to PrEP in Philadelphia, especially among marginalized communities facing barriers to PrEP access. Through a partnership between the Philadelphia Department of Public Health (PDPH) and Albert Einstein Medical Center (AEMC), the PTP was designed to bolster access by providing PrEP services in a flexible and convenient online format that eliminates the need for patients to travel to a physical clinic for PrEP care. Patients enroll through the Philly Keep on Loving website (Philadelphia Department of Public Health, 2024), where they can chat with a navigator or directly schedule an appointment with a PrEP provider. Nursing staff at the PTP coordinate laboratory specimen collection using at-home testing kits or local lab options before the telehealth consultation with a PrEP provider. After the appointment, PrEP medication is prescribed and delivered to the patient, with ongoing support and follow-up provided by the PTP team.
As telePrEP programs like the PTP are considered and implemented across jurisdictions in the United States, there is a need for research to understand the factors influencing their implementation, reach, and impact among key populations. To date, several studies have found telePrEP to be a feasible and acceptable strategy (Chasco, Shafer, et al., 2021; Player et al., 2022; Refugio et al., 2019), and limited evidence suggests that these programs are effective at linking clients to PrEP at rates similar to in-person PrEP programs (Bonett, Li, et al., 2024; Chasco, Shafer, et al., 2021; Meyer et al., 2022). While telePrEP has shown promise, research on contextual determinants influencing implementation is limited. Understanding these factors is crucial for adapting and scaling up programs to serve priority populations and promote health equity (Tapia et al., 2024). To address this need, we conducted a qualitative descriptive study aimed at identifying the systems-level facilitators and barriers to the equitable implementation of telehealth-delivered PrEP services in Philadelphia through the PTP.
Method
Interviews With Staff and Stakeholders
We conducted in-depth individual interviews with PTP staff working at AEMC (i.e., providers, patient navigators, and program managers). The telePrEP clinic at AEMC is affiliated with their Immunodeficiency Clinic, which offers health and social services for people living with HIV, and their Pride Clinic, which specializes in serving the LGBTQ community. We used total population sampling for program staff by sending interview invitations to all clinical and non-clinical staff members directly involved in the telePrEP program (n = 12). In addition, we used purposive sampling to identify and recruit several community stakeholders that worked in other health service and community organizations providing HIV related services. We worked with our research team members and partners at PDPH and AEMC to identify key leaders in the local HIV prevention and care workforce. We deliberately selected potential participants who represented diverse clinical and community settings to ensure a range of perspectives on program implementation and community needs. These stakeholders were included to provide a broader perspective on how the PTP fits into the larger HIV prevention landscape, offering insights on community needs, potential barriers, and opportunities for collaboration that might not be apparent to those directly involved in the program.
Using a semi-structured interview guide based on Consolidated Framework for Implementation Research (CFIR), interviews explored facilitators and barriers to the implementation of the PTP. The CFIR is organized into five key domains: innovation characteristics, outer setting, inner setting, characteristics of individuals, and implementation process. These domains include a range of constructs that represent specific barriers and facilitators to implementation success, such as the complexity and adaptability of the intervention itself, external policies and incentives, organizational culture and readiness for change, and individual knowledge and beliefs (Damschroder et al., 2022). The CFIR provides a structured approach for identifying determinants of implementation and informing the development of implementation strategies tailored to specific contexts and has been applied across a wide range of settings to evaluate the implementation of health interventions, including HIV prevention programs and telehealth initiatives (Li et al., 2022; Rangachari et al., 2022). Our interview guides were tailored to the participant’s role (staff or stakeholder), and were focused primarily on constructs in the Innovation, Inner Setting, and Outer Setting Domains (see Supplemental Material for full interview guides). The interviews were conducted through video conferencing between May and September 2023, which corresponds to a period approximately 9 to 12 months after the PTP started accepting patients. All interviews were recorded and lasted 30 to 60 minutes. Before starting, each interviewee underwent an informed consent process and verbally agreed to being recorded. After the interview, participants completed a brief survey where they provided self-reported demographic information including race/ethnicity, gender, sexual orientation, educational background, and professional role.
Data Analysis
The interviews were transcribed verbatim by research staff and a third-party transcription agency. Three authors (AS, QL, SB) used deductive qualitative methods to analyze the transcripts using the Dedoose software platform (Version 9.0.90, Los Angeles, CA). Prior to analysis, the team created a codebook containing 45 codes based on the CFIR framework, selected for their relevance to the interview guide questions. To ensure systematic application of CFIR constructs, each code was clearly defined and included example applications specific to telePrEP implementation.
To establish initial coding consensus and calibrate the team’s approach (Cascio et al., 2019; Giesen & Roeser, 2020), the first interview was coded independently by three authors (AS, QL, SB) and any discrepancies were resolved through discussion. These initial coding discussions helped identify potential sources of interpretive bias and established shared understanding of code applications. The eight remaining interviews were coded independently by two of the authors, with regular team meetings to resolve any coding disagreements. No measures of inter-rater reliability were used, as the two coders discussed each code until full consensus was achieved. To ensure comprehensive and consistent coding throughout the analysis process, codes were updated iteratively as interviews were completed, with clear documentation of any modifications. After each update to the codebook, the team reviewed previously coded transcripts to ensure consistent application of new or modified codes.
Deductive thematic analysis was conducted based on the CFIR to identify the most salient determinants of implementation. The research team collectively reviewed coded excerpts within each CFIR construct to identify patterns and assess the valence of each implementation determinant. These determinants were then classified as either facilitators or barriers to implementation.
We continued recruitment until all staff had been invited, and until we observed substantial thematic redundancy in our interviews with stakeholders, with later interviews largely confirming patterns identified in earlier ones rather than generating new insights about implementation barriers and facilitators.
Results
We interviewed nine participants, including five staff members at the PTP (two providers, two patient navigators, and one program manager) and four community stakeholders. The demographic characteristics of interview participants are shown in Table 1. Results from the thematic analysis are presented here, organized by CFIR domain. Additional illustrative quotes as well as the CFIR constructs associated with each theme can be found in Table 2.
Demographic Characteristics of Participating Staff and Stakeholders Related to the Philadelphia TelePrEP Program (PTP), n = 9

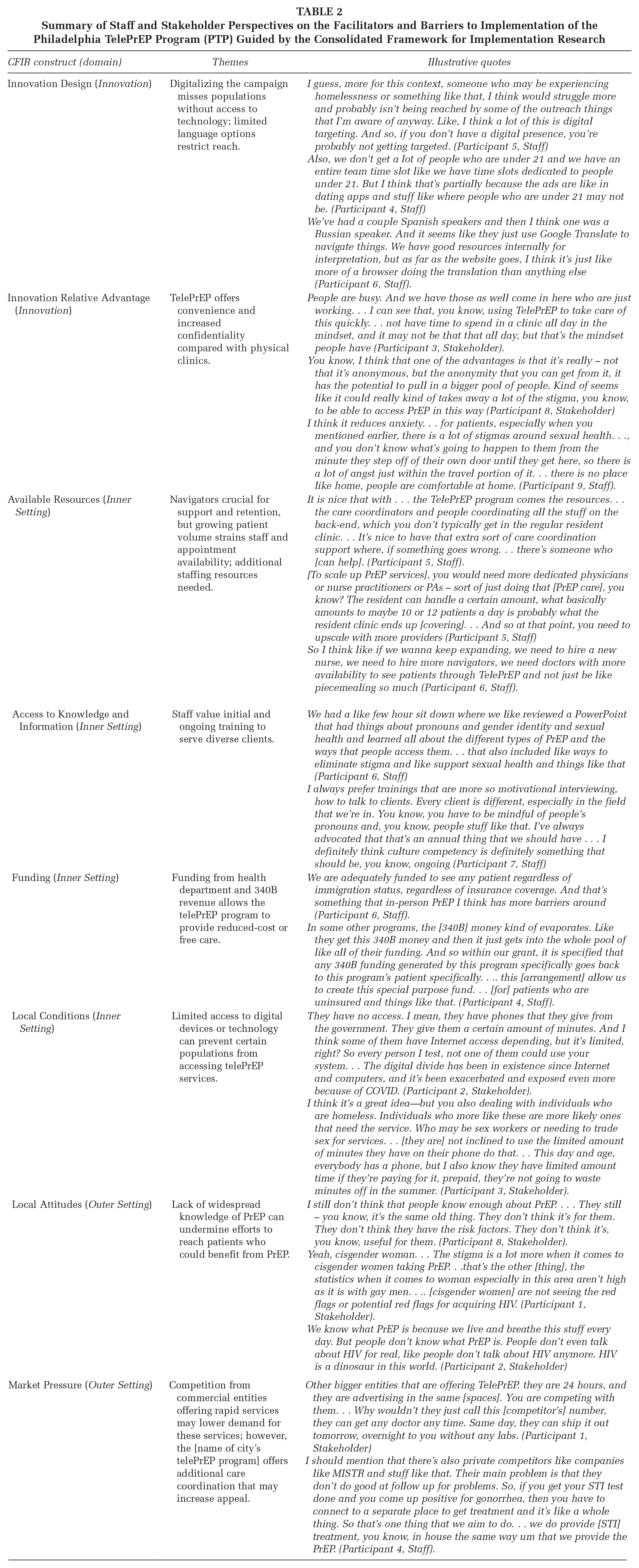
Summary of Staff and Stakeholder Perspectives on the Facilitators and Barriers to Implementation of the Philadelphia TelePrEP Program (PTP) Guided by the Consolidated Framework for Implementation Research
Convenience and Online Marketing (CFIR Innovation Domain)
The online format of telePrEP was seen as an asset, meeting client needs for convenience and flexibility in accessing PrEP services. Staff from the PTP perceived that their clients valued the convenience and ease of not having to go into a physical location for care (CFIR: Relative Advantage). According to these staff members, the telePrEP model appeared to meet client needs for flexibility in accessing PrEP services by allowing clients to have their video consultation with a provider anywhere, without navigating travel and transportation to a clinic. Staff members also reported that some clients may have faced barriers to seeking in-person PrEP services due to medical mistrust and stereotypes regarding PrEP, and the telePrEP model helped to overcome these barriers (CFIR: Relative Advantage). One staff member described how the telehealth format could help overcome hesitancy around seeking sexual health care, and address barriers related to travel:
I think it reduces anxiety. . . for patients, especially when you mentioned earlier, there is a lot of stigmas around sexual health. . ., and you don’t know what’s going to happen to them from the minute they step off of their own door until they get here, so there is a lot of angst just within the travel portion of it. . . there is no place like home, people are comfortable at home. (Participant 9, Staff).
However, the telePrEP model presents potential barriers related to marketing and accessibility of the online platform. Advertising and marketing for the PTP was conducted exclusively through online channels, and some participants have expressed concerns that this might exclude certain populations that do not have a strong presence in the digital space (CFIR: Innovation Design). In addition, while the online platform is now available in both English and Spanish, it was initially available only in English, which limited accessibility to individuals who spoke other languages. Several participants highlighted these barriers:
Like, I think a lot of this is digital targeting. And so, if you don’t have a digital presence, you’re probably not getting targeted (Participant 5, Staff).
We’ve had a couple Spanish speakers and then I think one was a Russian speaker. And it seems like they just use Google Translate to navigate things. We have good resources internally for interpretation, but as far as the website goes, I think it’s just like more of a browser doing the translation than anything else (Participant 6, Staff).
Staffing Resources, Training, and Funding (CFIR Inner Setting Domain)
Participants expressed that having dedicated patient navigators has been an integral part of ensuring client satisfaction with the program. Navigators were able to provide on-demand troubleshooting and care coordination, making it easier to resolve participant issues in a timely manner (CFIR: Available Resources). In addition, having local navigators who are familiar with the landscape of resources in Philadelphia is an additional benefit of this model.
It is nice that with . . . the TelePrEP program comes the resources. . . the care coordinators and people coordinating all the stuff on the back-end, which you don’t typically get in the regular resident clinic. . . It’s nice to have that extra sort of care coordination support where, if something goes wrong. . . there’s someone who [can help]. (Participant 5, Staff).
As the patient volume at the PTP grew from about 10 enrollments per month during the first 6 months of implementation to about 20 enrollments per month during the subsequent 6 months, the availability of appointment slots with providers became more limited (CFIR: Available Resources). Participants noted that in order for the program to continue to scale-up, additional staffing resources were needed, including more providers.
[To scale up PrEP services], you would need more dedicated physicians or nurse practitioners or PAs – sort of just doing that [PrEP care], you know? The resident can handle a certain amount, what basically amounts to maybe 10 or 12 patients a day is probably what the resident clinic ends up [covering]. . . And so at that point, you need to upscale with more providers (Participant 5, Staff)
Training and education for staff members has played a pivotal role in ensuring that the staff are competent in providing care to marginalized communities (CFIR: Access to Knowledge and Information). Staff reported that their team placed a strong emphasis on providing ongoing training to keep up-to-date with important information and innovations that can support the staff and their clients:
We had a like few hour sit down where we like reviewed a PowerPoint that had things about pronouns and gender identity and sexual health and learned all about the different types of PrEP and the ways that people access them. . . that also included like ways to eliminate stigma and like support sexual health and things like that (Participant 6, Staff)
Sustainable funding for this model of telePrEP service delivery was discussed by several of our participants. One participant highlighted the key role of the PDPH in creating a sustainable funding model. The PDPH designed the telePrEP program and selected AEMC as the implementing partner through a competitive process. As the selected partner, AEMC now receives grant funding to implement the program. This funding, in combination with revenue from the federal 340B drug pricing program, allows the telePrEP provider to cover the cost of providing care to patients without insurance (CFIR: Funding).
In some other programs, the [340B] money kind of evaporates. Like they get this 340B money and then it just gets into the whole pool of like all of their funding. And so within our grant, it is specified that any 340B funding generated by this program specifically goes back to this program’s patient specifically. . .. this [arrangement] allow us to create this special purpose fund. . . [for] patients who are uninsured and things like that. (Participant 4, Staff).
Digital Divide, Lack of PrEP Awareness, and Market Competition (CFIR Outer Setting Domain)
While telehealth offered the potential for expanded access to PrEP, several participants noted that limited access to technology (i.e., access to computer or smartphone to use the telePrEP platform) could pose a barrier to engaging with this model. This raised concerns about potential limitations of the model to reach populations with multiple intersecting social needs, including those with limited internet access, as well as those facing housing instability, food insecurity, and unemployment (CFIR: Local Conditions). One stakeholder in an HIV service organization spoke about the clients their organization serves:
They have no access. I mean, they have phones that they give from the government. They give them a certain amount of minutes. And I think some of them have Internet access depending, but it’s limited, right? So every person I test, not one of them could use your system. . . The digital divide has been an existence since Internet and computers, and it’s been exacerbated and exposed even more because of COVID. . .” (Participant 2, Stakeholder).
Furthermore, some stakeholders have noted that the clients they serve may have limited awareness of PrEP or may misunderstand who is eligible for PrEP. A common misconception that participants noted was that PrEP is primarily a tool for men who have sex with men, and that cisgender women are not candidates for PrEP. Participants discussed how this lack of awareness and knowledge related to PrEP could hamper the efforts of the PTP to expand access, and suggested that additional emphasis on PrEP education is needed in public health messaging (CFIR: Local Attitudes).
I still don’t think that people know enough about PrEP. . . . They still – you know, it’s the same old thing. They don’t think it’s for them. They don’t think they have the risk factors. They don’t think it’s, you know, useful for them. (Participant 8, Stakeholder).
In addition, participants noted that competition from commercial telePrEP providers may serve as an organizational barrier to this model of telePrEP (CFIR: Market Pressure). These commercial entities offer round-the-clock services and aggressive advertising, posing significant competition to local telePrEP programs. The convenience and rapid services offered by these commercial providers can be attractive to potential clients, who may opt for their services over local telePrEP programs. Speaking about a commercial telePrEP service, one stakeholder who worked for a local organization piloting a similar telePrEP program noted:
Other bigger entities that are offering TelePrEP, they are 24 hours, and they are advertising in the same [spaces]. You are competing with them. . . Why wouldn’t they just call this [competitor’s] number, they can get any doctor any time. Same day, they can ship it out tomorrow, overnight to you without any labs. (Participant 1, Stakeholder)
Discussion
This qualitative study identified systems-level facilitators and barriers to implementing the PTP. Key facilitators included: (1) the convenience and flexibility of the telehealth format, which eliminated travel barriers; (2) dedicated patient navigators who provided support for troubleshooting and care coordination; (3) comprehensive staff training in cultural humility and LGBTQ+ competent care; and (4) sustainable funding through health department support and 340B revenue. Primary barriers included: (1) limited provider availability as patient volume increased; (2) digital marketing strategies that potentially missed populations without strong online presence; (3) the digital divide preventing access among those with limited technology resources; (4) insufficient public awareness and knowledge about PrEP; and (5) potential competition from commercial telePrEP providers.
Participants in this study highlighted key strengths of the telehealth model used by the PTP, including its ability to provide convenient, flexible, and locally operated services. Beyond the flexibility inherent to the telehealth model of PrEP delivery, which has been highlighted across a variety of contexts (Giorlando et al., 2023; Hughes et al., 2021; Refugio et al., 2019; Tapia et al., 2024), having telePrEP program run by a local health department and implemented by a large health care organization allows for additional adaptability. For instance, the PTP offers flexibility in lab specimen collection, overcoming barriers identified in previous research (Chasco, Hoth, et al., 2021; Sharma et al., 2023). The PTP is uniquely positioned to serve marginalized populations by offering no-cost services regardless of insurance status. In addition, the PTP has the ability to leverage local referrals to connect clients with co-occurring medical and social needs to appropriate and accessible resources. Furthermore, the PTP can provide long-acting injectable PrEP, a recently developed PrEP modality that is highly efficacious and may be more acceptable than oral formulations among some patient populations (Delany-Moretlwe et al., 2022; Landovitz et al., 2021; Sued et al., 2022), as an option for patients in their in-person clinic.
A key barrier to implementation identified in our study was related to public awareness and knowledge of PrEP. In alignment with existing literature (Kalwicz et al., 2023; Kudrati et al., 2021), we found that both staff in the PTP and stakeholders in the wider HIV service workforce were concerned about the reach of marketing and advertising materials to the diverse communities that could benefit from PrEP. Specifically, there were concerns about low HIV risk perception and low PrEP awareness among cisgender women, as well as missed opportunities for outreach to populations with limited access to technology or who are not present on digital platforms commonly used for PrEP marketing (e.g., dating apps tailored to men who have sex with men). The PTP has adapted its marketing strategy, focusing recent campaigns on increasing PrEP awareness among Black and Latino sexual minority men and cisgender women who are at elevated risk for HIV due to poverty and other structural risk factors. As part of this strategy, digital ads are featured across various online platforms including search engines, social media sites, and dating apps.
While participants identified competition from commercial telePrEP providers as a barrier to implementation, the expanding landscape of telehealth providers for PrEP services also presents key opportunities to reach marginalized communities and promote equity in access to PrEP. Large commercial telePrEP providers have expanded the reach of PrEP services and offer a fast and convenient avenue to services (Dawson et al., 2022). However, these platforms may have limited reach to marginalized communities, especially those without health insurance and low-income populations where cost is a major barrier to PrEP access (Wong et al., 2020).
The importance of cultural humility and the integration of community experience into staff resources were also highlighted by participants in this study. Staff working at the PTP described how ongoing training and education around delivering non-stigmatizing sexual health services helped to facilitate implementation of this model and could promote client retention for these remotely delivered PrEP services. These findings align with recent research in both telePrEP programs and in-person sexual health clinics that emphasized the significance of prioritizing cultural humility, as well as hiring staff with lived experience relevant to the clients they serve (Bonett, Mahajan, et al., 2024; Tapia et al., 2024). It’s worth noting that the PTP’s clinical partner is AEMC’s Pride Clinic, which likely resulted in an environment with greater resources and expertise around providing culturally responsive care to sexual and gender minority populations.
Limitations
This study has several limitations that should be considered. First, our data were limited to the perspectives of staff and stakeholders; additional insights from patients and potential patients who have used or considered using the PTP would be valuable to better understand barriers and facilitators at the patient level. Future research should prioritize gathering patient perspectives, with particular attention to reaching individuals who attempted but did not complete enrollment in telePrEP services.
Second, our study had a small sample size and potential for selection bias. While our sample included a majority of the permanent staff working for this program, additional staff members who did not participate in interviews could offer valuable narratives that were not captured in our data. Staff who chose not to participate may have had different perspectives on implementation challenges, potentially leading to underrepresentation of certain viewpoints. While we took several steps to encourage candid responses from staff who did participate– including emphasizing the confidential nature of the interviews, removing all identifiers from the data, and explicitly stating that responses would not impact employment—staff members may still have felt some pressure to present the program in a positive light or downplay implementation challenges.
Third, it’s important to note that a small portion of the PTP’s clinical care is provided by family medicine residents, who are supervised by the attending physician. This incorporation of resident physicians served as an additional staffing resource to some degree, but also highlights the focus on medical training and education within the program. This dynamic would not be present in non-teaching settings, which has implications for how these findings translate to those settings. Comparative studies of telePrEP implementation across teaching and non-teaching settings could help clarify how staffing models influence program outcomes.
Finally, our study focused on a single telePrEP program in one large metropolitan area, which may limit the generalizability of our findings to other settings. The barriers and facilitators identified in this study may be specific to the unique characteristics and resources of the PTP and the Philadelphia context. Multi-site implementation studies across different geographic and organizational contexts would help identify which implementation factors are context-specific versus broadly applicable.
Implications for Practice
The findings of this study offer several important implications for the implementation and improvement of telePrEP programs. Strategic use of local resources and collaborations could allow telePrEP programs to bridge the digital divide. The digital divide, characterized by the gap between those who have access to digital technologies and those who do not, has been recognized as a significant barrier to health equity in the context of digital health interventions (Kincaid et al., 2023; Mitchell et al., 2019; Ramsetty & Adams, 2020). To address this barrier, partnerships with community-based organizations could help to facilitate access to the technology and internet services needed to engage with telePrEP, while also providing opportunities for more targeted outreach and education to raise awareness of PrEP among communities with low PrEP knowledge.
In addition, future telePrEP programs should also prioritize targeted, culturally relevant marketing strategies to reach diverse populations who are vulnerable to HIV, rather than broad social media advertising to the general population. Ongoing evaluation of these campaigns can inform adaptations to improve PrEP awareness and uptake among priority groups.
Implications for Policy
Integration with local health departments should be seen as a major asset for future telePrEP programs. Leadership and investment from the local health department can create opportunities to leverage existing public health resources, improve referral pathways across services, and enhance community trust. These partnerships can also aid in addressing insurance barriers by connecting health care providers to city-wide efforts to provide no-cost or low-cost services to uninsured and underinsured populations, promoting equitable PrEP access.
Implications for Research
Future research should examine patient perspectives on telePrEP implementation, particularly among populations facing technological barriers or with limited PrEP awareness. In addition, implementation studies are needed to test strategies for bridging the digital divide in telePrEP delivery. This could include evaluating hybrid models that combine telehealth with community-based services, or examining the effectiveness of providing technology support and resources to potential users of telePrEP programs. Finally, research should examine the cost-effectiveness and sustainability of different funding models for telePrEP programs, including the role of 340B revenue and public health department support in promoting equitable access, and the comparative costs and impact of various strategies for advertising and outreach. Such economic analyses could inform policy decisions about sustainable scaling of telePrEP services.
Conclusion
Telehealth represents an innovative approach to expanding PrEP access, offering a convenient and flexible path to services that can help overcome traditional barriers to care. Our study of a local telePrEP program demonstrates both the promise and challenges of this service delivery model. The program’s strengths—including its ability to provide tailored local resources, integrate with existing HIV prevention services, and offer navigation support—highlight how telehealth can enhance rather than simply digitize PrEP delivery.
However, realizing the full potential of telePrEP requires addressing critical implementation challenges. The digital divide and low public awareness of PrEP continues to limit access for marginalized populations. Success in scaling up telePrEP programs will depend on fostering robust partnerships with community organizations and local health departments, prioritizing cultural humility and community representation among staff, and developing targeted marketing strategies that resonate with diverse populations.
As telehealth becomes increasingly important to HIV prevention efforts, careful attention to equity in implementation will be crucial. Future telePrEP programs should build on lessons learned about the importance of local context, community partnerships, and comprehensive support services in creating accessible and effective PrEP delivery systems.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399251347253 – Supplemental material for Facilitators and Barriers to Equitable Implementation of Telehealth PrEP Delivery: A Qualitative Descriptive Study of Program Staff and Stakeholders
Supplemental material, sj-docx-1-hpp-10.1177_15248399251347253 for Facilitators and Barriers to Equitable Implementation of Telehealth PrEP Delivery: A Qualitative Descriptive Study of Program Staff and Stakeholders by Stephen Bonett, Anna Sweeney, Qian Li, Dovie L. Watson, José Bauermeister, Brian Hernandez, Javontae Williams and Kathleen A. Brady in Health Promotion Practice
Footnotes
Authors’ Note:
This work was supported by a National Institutes of Health supplement award to the Penn Center for AIDS Research (P30AI045008; Parent PI: Collman, Supplement PI: Bonett),
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.