
Abstract
Child care programs can be one setting for promoting physical activity (PA). To support technical assistance providers in promoting PA best practices, Nemours Children’s Health with the Centers for Disease Control and Prevention developed a set of trainings known as Physical Activity Learning Sessions (PALS). PALS centers on PA best practices, and state partners are encouraged to embed the program into early care and education (ECE) systems, such as training and TA networks. From 2019 to 2023, 22 states and 802 individuals completed a PALS train-the-trainer (TTT) course. This brief highlights findings from the 2022–2023 PALS evaluation, examining the extent to which PALS provided ECE trainers with effective training materials, affected trainer confidence in providing PA trainings to ECE providers, and was integrated into state systems. The PALS evaluation included a mixed-methods design consisting of pre-, post-, and 6-month post-TTT surveys of trainers. Among trainers, 87% of 125 respondents said they were confident training ECE providers on PA practices after completing the PALS TTT. Nearly 67% of participants planned to deliver a PALS training to ECE providers within 6 months of completing the TTT. Surveys from 16 of 18 PALS state leads suggested PALS has been embedded in state ECE systems. PALS counts for training credit of some type in 10 states, including licensing, provider credentials, and Quality Rating and Improvement Systems. Additional evaluation efforts could determine the impact of PALS on PA practices and policies among ECE providers and programs.
Keywords
In the United States, 74% of children aged 3–5 years are cared for by someone other than a parent each week, with most children (83%) attending center-based early care and education (ECE) programs (The National Center for Education Statistics, 2021). A recent nationally representative survey found that over a third of children in this age group (37%) play outdoors for 1 hr or less per weekday and nearly a quarter (24%) play outdoors for 1 hr or less per weekend day, suggesting a need for more supports for outdoor play and physical activity (Dahl et al., 2023). Physical activity (PA) has been shown to enhance cognitive development, gross motor skills, and social emotional learning in children (Khan & Hillman, 2014; Yogman et al., 2018). Being active at a young age is also associated with improved bone health and weight status (Centers for Disease Control and Prevention, 2024). Despite the known benefits of PA, studies from the United States and Canada have found that young children in ECE spend 50%–94% of their time being sedentary (Alhassan et al., 2012; Pate et al., 2008; Statler et al., 2019). ECE providers report barriers to embedding more PA in their programs, including lack of space and time (Dinkel et al., 2017).
To address some of these challenges, Nemours Children’s Health (Nemours), with the support of the Centers for Disease Control and Prevention (CDC), designed a set of PA trainings using a train-the-trainer model (TTT). Nemours created the Physical Activity Learning Sessions (PALS) program in 2019 and disseminated to 22 states from 2019 to 2023. The goal of PALS was to develop trainings centered on PA best practices to support state trainers and technical assistance (T/TA) providers to train ECE providers statewide. PALS emphasizes embedding the trainings into existing state ECE systems to ensure sustainability.
This brief highlights findings from the 2022–2023 PALS evaluation, which examined the extent to which PALS provided T/TA providers effective training materials, affected trainer confidence in delivering PA trainings to ECE providers and was integrated into state ECE systems.
Program Description
PALS covers eight areas of PA best practices: time, space, type, daily activities, provider’s role, family engagement, training and resources, and policy. Best practices are taken from Caring for Our Children Health and Safety Performance Standards; Guidelines for Early Care and Education Programs (American Public Health Association et al., 2019) and include 11 High-Impact Obesity Prevention Standards relating to PA. PALS aims to address the challenges faced by ECE providers supporting active play for young children.
The PALS package was shared through a TTT approach for T/TA providers. First, Nemours’ staff trained T/TA trainers virtually on PA for young children and the 8 recommended PA content areas. Trainers participated in 6 hr of training. They received slide decks with speaker notes (in English and Spanish), handouts, and sample training activities. A resource kit with equipment was also provided for demonstrations. After completing the TTT, T/TA providers could deliver PALS to ECE providers in their community in-person, virtually, or via hybrid approaches. All PALS materials were provided at no cost to T/TA providers and are available for free download at https://healthykidshealthyfuture.org/.
Program Dissemination
PALS was piloted as an in-person training in 2019 in three states. Due to the COVID-19 pandemic, Nemours modified PALS for virtual delivery in 2021. They translated it into Spanish in 2022. From 2020 to 2023, Nemours annually selected additional states to expand the use of PALS. Once a state was identified, a program manager from the health department or child care resource and referral agency would serve as that state’s PALS lead responsible for the program. The PALS state lead along with key state partners recruited trainers to attend the PALS TTT. T/TA providers who participated in the TTT came from child care resource and referral agencies, child care health consultation, cooperative extension, infant toddler networks, state or local health departments, and child and adult care food program organizations.
PALS state leads and T/TA providers were offered quarterly calls to support peer learning and networking across states. As shown in Table 1, 22 states and 802 individuals completed a PALS TTT from 2019 to 2023. States trained an average of 36 trainers, ranging from 3 in Massachusetts to 173 in Tennessee.
Number of Trainers Receiving PALS Training by State, 2019–2023 a

Note. PALS = Physical Activity Learning Sessions.
Nemours Children’s Health administrative data. bLocal initiative by Boston Public Health Commission.
Program Evaluation
An external evaluator was contracted for PALS evaluation. The evaluation assessed (a) the impact of PALS on T/TA provider experience and confidence in delivering PA trainings; and (b) integration of PALS into state ECE systems.
Methods and Data Collection
The PALS evaluation included a mixed-methods design consisting of pre-, post-, and 6-month post-TTT surveys of trainers that participated in a TTT session from February 2022 to July 2023. Information on T/TA provider experience with PA training in general (pre-test), how well PALS prepared them to deliver PA training to ECE providers (post-test), and the extent to which trainers used PALS (6-month post-training) was solicited through optional web-based surveys. Pre-surveys were sent to the 276 T/TA providers who registered to attend a TTT session from February 2022 to July 2023. A post-survey was administered immediately following the PALS TTT and a final survey was sent 6 months later. To explore the extent to which PALS contributed to ECE systems change, a state lead survey was fielded from May to June 2023 to the 18 PALS state leads.
Data Analysis
For the trainer and state lead surveys, descriptive statistics were generated for all close-ended questions. Responses to open-ended questions were analyzed for common themes. Completion rates varied by trainer questionnaire: 163 TTT participants (66%) completed the pre-survey, 125 individuals (45%) completed the post-survey, and 85 (31%) returned a 6-month follow-up survey. Completion of state lead survey was 16 of 18 states with an 89% response rate.
Results
Trainer Survey Finding
Table 2 summarizes the survey results. In the pre-test (n = 163), 49% of trainers reported they had never received training on PA in ECE settings, and 11% reported they did not know or remember if they had previous PA training. However, 48% of respondents reported they were “somewhat prepared” to lead a PA training for ECE providers while another 14% said they were “between not prepared and somewhat prepared” and 9% said they were “not prepared at all.” Only 10% said they were “extremely prepared.” Among the 153 respondents who stated they provided training to ECE providers annually, 38% reported carrying out 1 to 5 trainings per year, and 23% reported providing up to 10 trainings per year.
Summary of Participant Agreement Before and After PALS TTT Course
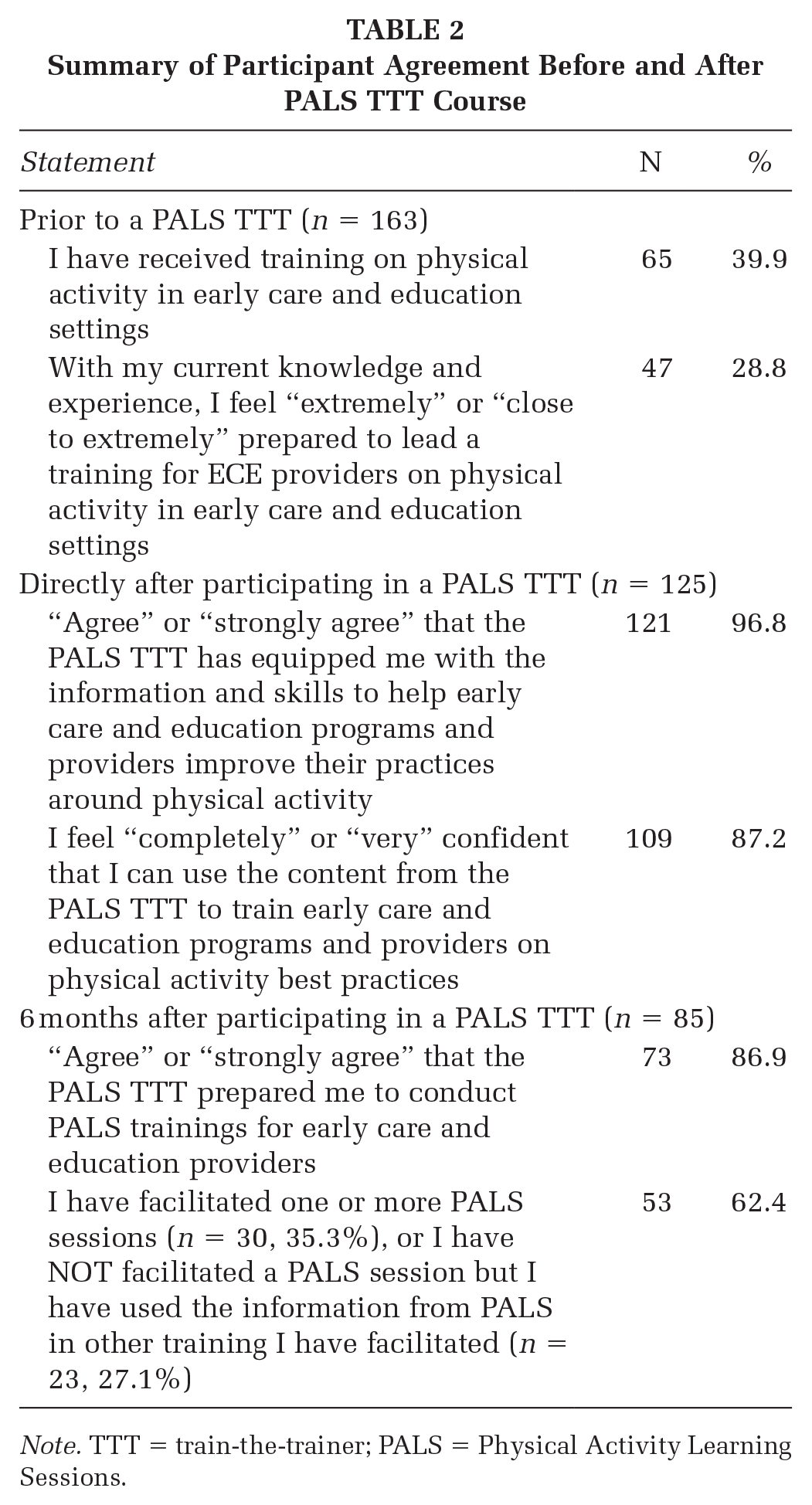
Note. TTT = train-the-trainer; PALS = Physical Activity Learning Sessions.
In the post-survey (n = 125), nearly all respondents agreed (121/125) (60% “strongly agreed” and 37% “agreed”) that the PALS TTT equipped them with information and skills to help ECE programs and providers improve their PA practices. When asked about their confidence to train ECE providers using PALS, 87% said they were “completely or very confident” after the TTT. After completing the TTT, nearly 67% of participants planned to deliver a PALS training within 3–6 months.
Among respondents to the 6-month survey (n = 85), 35% had facilitated one or more training sessions with ECE providers using PALS materials. Another 27% reported they had not facilitated a training but had used PALS content in other ECE provider trainings they delivered. Respondents who had delivered a training over the last 6 months (n = 30) reached a total of 823 ECE providers. Notably, 6 months after participating in a PALS TTT, 87% of respondents agreed or strongly agreed they were prepared to conduct an ECE provider PALS training. In addition, 81% of respondents agreed or strongly agreed they would use the PALS materials when working with ECE providers.
PALS State Lead Survey Findings
In the PALS state lead survey, 6 of 16 states (38%) reported they had made PALS trainings available to all ECE providers in their state by recruiting T/TA providers from all geographic regions of the state or promoting virtual trainings. In addition, one state reported that PALS is available for most ECE providers, six states have made the trainings available for some ECE providers, and three states indicated that although it is currently unavailable, they plan to make it available once state training calendars open for new trainings. One important state strategy for sustainability was offering professional development training credit to ECE providers who take a PALS training. PALS counts for training credit in 10 states, with 3 states recognizing PALS for licensing training credits, provider credentials, and training credits for Quality Rating and Improvement System (QRIS). Two states indicated PALS had not yet been embedded for state training credit, and one state reported no training credit for PALS within their systems and no plans to integrate it.
Information on the number of ECE providers trained by PALS trainers is limited, but the state lead and 6-month trainer surveys provide some insights on the extent to which PALS has reached ECE providers. Seven state leads reported the number of ECE providers who participated in PALS trainings. Then, 844 total individuals are known to have participated in a PALS training. Six states provided data on the number of ECE facilities reached, with numbers ranging from 5 to 389. In total, at least 606 ECE facilities completed the training.
Data from the 6-month follow-up survey of PALS trainers (n = 85) also provide some indication of the spread of PALS. Among these respondents, 35% reported they had conducted one or more training sessions with ECE providers using the PALS materials. Another 27% reported they had not facilitated a training but had incorporated PALS content into other trainings for ECE providers.
Discussion
This evaluation suggests that PALS increased trainer confidence to deliver evidence-informed trainings on PA to ECE providers. The state lead survey highlighted the extent to which PALS has been embedded in state systems, which has not typically been examined in studies of PA training approaches (Messing et al., 2019). There is demand for PA training, as shown in the number of states (n = 22) that requested a PALS TTT session and in responses to the PALS state lead survey. T/TA providers have put PALS concepts into practice and are conducting PALS sessions in at least 14 of the 22 states that held TTT. States have taken steps to institutionalize PALS by including it as an option for licensing, provider credentialing, and QRIS. PALS is currently available to ECE providers in 14 states, with 6 states having statewide access, which increases access to training opportunities for ECE providers. Comprehensive reach data are unavailable because of challenges in tracking training data, especially given that PALS was disseminated through a TTT model. However, trainer and state lead data indicate that PALS is reaching ECE providers. Even when these trainers are not delivering dedicated PALS sessions, they are applying the knowledge they gained in the PALS TTT to their broader TA provision.
Limitations
The PALS evaluation had three limitations. First, all survey data were self-reported, and it was not possible or feasible to verify the number of ECE providers trained by PALS T/TA providers. Second, questions on the pre- and post-surveys were not identical, and so a matched analysis of participant responses before and after the PALS TTT was not possible. Finally, response rates varied across the three TTT survey timepoints, with the largest number of respondents for the TTT pre-test (n = 163 respondents) and the smallest number at the 6-month post-survey (n = 85).
Implications for Practice
This evaluation suggests that PALS increased trainer confidence to deliver PA trainings and that the program was embedded in several state ECE systems. However, it is unknown that the extent to which PALS improved ECE provider’s PA practices in the classroom and overall program. This is an important topic for future evaluation. PALS seems acceptable to states, as evidenced by awarding training credits in many participating states and use by 22 states to date. Future efforts include continuing to scale and spread PALS by offering PALS TTT to more locations while continuing to offer refresher trainings for states already participating in PALS.
Footnotes
Authors’ Note:
The authors thank and recognize contributions made in the creation and development of the PALS program by Dr. Diane Craft, Ms. Allison Nihiser, and Mr. Michael Waldmiller. Nemours Children’s Health would like to acknowledge the funding received from the Centers for Disease Control and Prevention (CDC) through Cooperative Agreement (6 NU38OT000304-04) to support the design, delivery, and evaluation of the Physical Activity Learning Sessions (PALS). The findings and conclusions of this report are those of the authors and do not necessarily represent the official position of the CDC.