
Abstract
Efforts to effect racial health disparity (RHD) policy change are urgent, necessary, and subject to a key barrier: defensiveness among White privileged audiences. Within the literature to date, such defensiveness is under-investigated, and when examined, is typically conceived of as an individual cognitive outcome—a message effect—rather than a communication interaction. Yet policy change advocacy efforts, ranging from community organizing to change campaigns, necessitate communication interactions between advocates and privileged policy change audiences, such as neighborhood groups or policymakers themselves. This defensiveness conceptualization, focused on individual cognitions, therefore limits our understanding of interactive communication barriers in RHD policy advocacy processes. To address this limitation, our research conceives of defensiveness using the privileged identity exploration (PIE) model, developed by Watt in 2007, which posits that defensiveness strategies are used as part of an interactive communication process when people are asked to reflect on their own privilege. Defensiveness strategies, as described by Watt and colleagues in 2021 and 2023, are normal communicative reactions to protect one’s self-identity from threatening information; the PIE models eight such strategies. RHD information invokes racial privilege, therefore eliciting defensiveness. Using a thematic analysis of semi-structured qualitative interviews with White young adults from the Chicago (U.S.) area (N = 27), we identify defensiveness strategies relative to COVID-19 RHDs. Using the PIE as a lens to understand the data, we find some strategies lacking, some similar but differently nuanced, and identify a novel strategy among our participants, suggesting message tailoring opportunities. We describe implications for future research and practice.
Keywords
Racial inequities cannot be adequately understood without accounting for Whites’ perceptions of, and reactions to, their race and privileged position in the social order
Racial health disparities (RHD) inequitably harm communities and need addressing to support better health for everyone (WHO, 2021). RHD policy advocacy seeks to persuade stakeholders like policy makers and publics of the importance of RHD to enact new policies that substantively address the issue and repeal harmful policies (Niederdeppe et al., 2023). (Publics are groups differentiated by factors ranging from socio-demographics to behaviors (Hallahan, 2000; Slater, 1996)). RHD policy change advocacy efforts, ranging from partnership building to campaign development, are therefore communicative processes (Snyder & Iton, 2020). However, these efforts face a troubling catch-22: communication about RHD elicits cognitive dissonance and defensiveness among those with White racial privilege (Gollust and Cappella, 2013; Winett et al., 2021). This is because, as a system, RHD is upheld by both disadvantage and privilege (Jones, 2000); in the United States, RHD privilege is experienced by Whites (Knowles et al., 2014). Privileged identities are “ . . . socially constructed . . . [and] linked historically to aspects of social or political advantages in a society, such as a racial (White) identity” (Watt et al., 2021, p. 5).
Considering one’s White privilege threatens one’s self-image, with threats ranging from not seeing oneself positively (an innocence threat) to not seeing one’s accomplishments as fully earned (a meritocratic threat) (Knowles et al., 2014; Phillips & Lowery, 2018). Associated defensiveness can act as a barrier to RHD policy change advocacy efforts for those audiences (Calloway et al., 2022; Dupree & Kraus, 2022). Extant research has presented this defensiveness as an individual cognitive reaction to messaging—that is, as an outcome, rather than as a communicative process between parties (Watt, 2023). But as RHD information in policy advocacy is communicated with others, as in face-to-face meetings with policy makers or during community engagement events (Calloway et al., 2022; Parvanta et al., 2018), this narrow conceptualization limits our understanding of defensiveness as a communication process and as a barrier to policy change advocacy.
For researchers to better understand White defensiveness strategies in relation to RHD and for policy change advocacy practitioners to effectively mitigate and respond to them, we must begin identifying them. We analyzed qualitative interviews with White young adults in the Chicago (United States) area to understand how these individuals’ defensiveness strategies may exemplify—or depart from—existing research using the privileged identity exploration (PIE) model (Watt, 2023). Below we review current research on White defensiveness in relation to RHD policy change advocacy and detail the PIE model (Watt, 2023).
Literature Review
Encountering White Defensiveness Strategies During RHD Policy Change Advocacy
RHD policy change advocacy efforts developed and implemented by health promotion practitioners are designed to effect policy change both directly and indirectly. In indirect models, communication diffuses through a social system, which in turn is understood to indirectly pressure policy makers (Hornick, 2002). White adults act as key publics in indirect approaches in the United States, by virtue of their majority status and their inequitable White privilege (Knowles et al., 2014). In contrast, direct approaches work to persuade policymakers and staff, most of whom are White, to action policy change (Brenson and Victor, 2023; Snyder and Iton, 2020; Winett et al., 2021).
Communication is a key component of such advocacy (Snyder & Iton, 2020), regardless of its direct or indirect approach (see Figure 1). In turn, communication audiences undertake their own interactive communication activities to process such advocacy (see Figure 2).
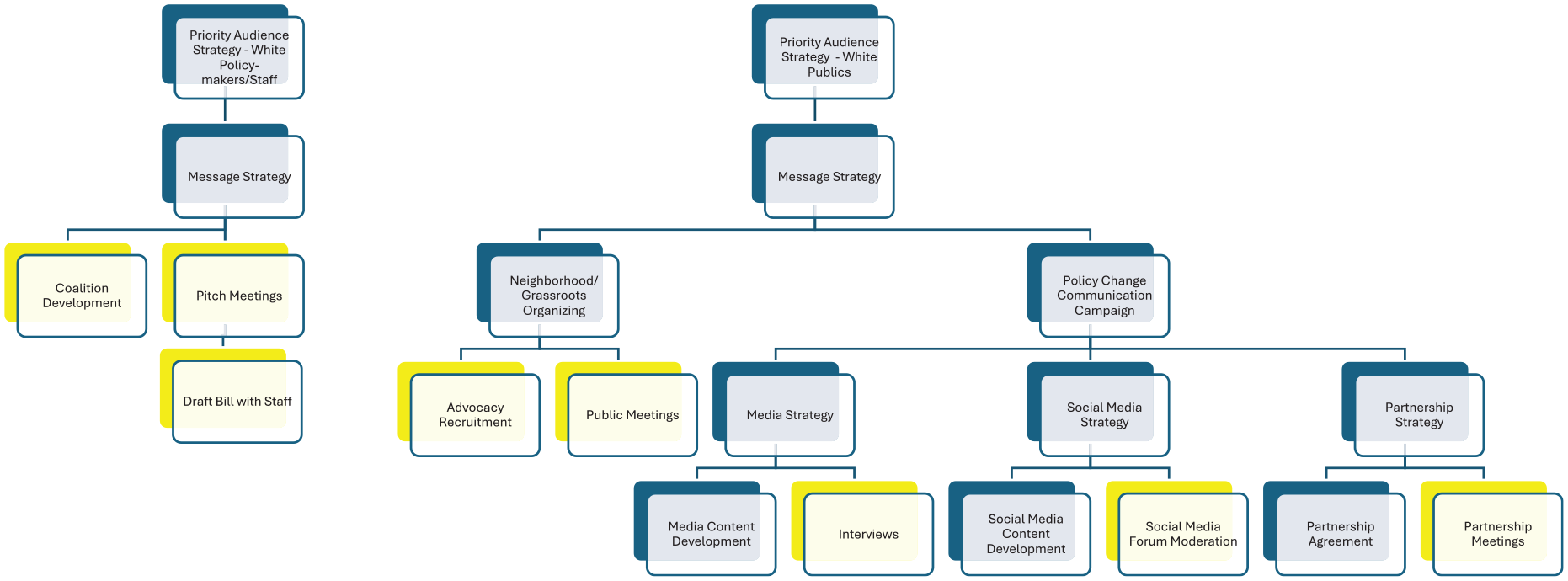
Communication Activities Associated With Policy Advocacy Change Efforts
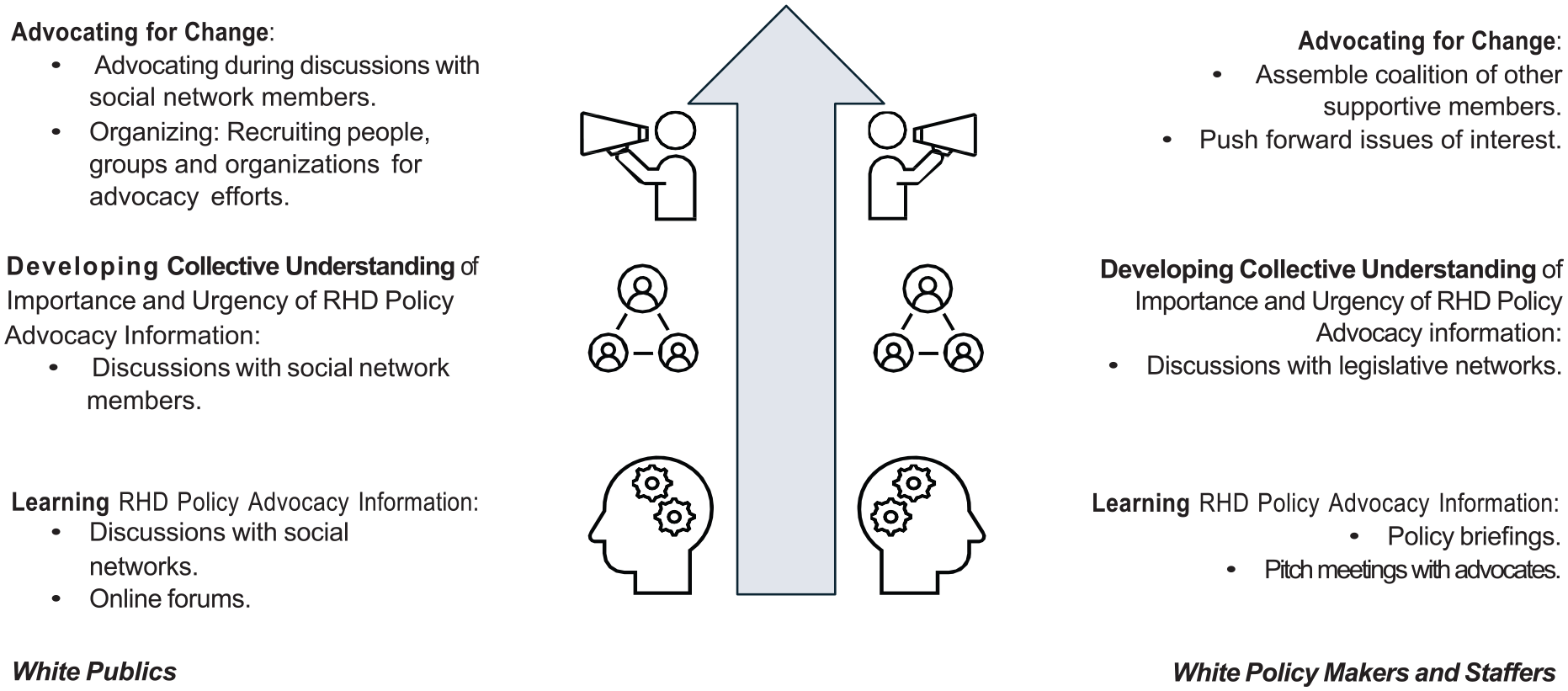
Opportunities for Communication Interactions Relative to RHD Policy Change Advocacy Efforts
Therefore, practitioners planning and undertaking advocacy for RHD policy change necessarily need to understand audience receptivity to such efforts. We contend that the outsize influence of White audiences, such as publics or policy makers, means that White defensiveness strategies represent a significant barrier to RHD policy change efforts. We further suggest that this barrier might contribute to the consistently low levels of public awareness of RHD (Gollust et al., 2020), as well as the low priority given to RHD by policy makers (Michener, 2022) by inhibiting communication interactions that lead to advocacy support.
Existing RHD health communication research lacks an appropriate understanding of audience receptivity processes; unfortunately, we know little about White defensiveness relative to RHD policy change advocacy efforts. In considering how to design such strategies, communication research has largely limited itself to focusing on message effects and consequently conceived of defensive reactions as individual cognitive outcomes (Niederdeppe et al., 2023; Peinado et al., 2020). Most of these studies feature survey or experimental designs with a majority of White audiences (Niederdeppe et al., 2023) and variously describe outcomes as ranging from motivated reasoning, when individuals selectively attend more to evidence confirming their existing opinion than disconfirming evidence (Taber & Lodge, 2006), to counterarguing, when generated thoughts counter a message’s attempted persuasive focus (Gollust & Cappella, 2014).
Yet developing effective communication relative to RHD policy change advocacy requires research that extends beyond examining cognitive message level effects. Understanding interactive audience behaviors—what defensiveness strategies White audiences enact in concert with others when faced with RHD information—can inform our knowledge of a barrier to White audience receptivity to policy advocacy change efforts. To begin identifying defensiveness strategies, we turn to the PIE model.
The PIE
The PIE is based on cognitive dissonance, an uncomfortable feeling induced by inconsistencies between one’s attitudes and behaviors, or new information and existing knowledge. It motivates attempts to reduce dissonance, from behavior change to rationalization (Festinger, 1954). The PIE was developed through analysis of reactions to dialogues during an ongoing multiculturalism course with masters students; dialogues ranged in topic from racism to homophobia (Watt, 2007). The PIE states this dissonance results in eight defensive strategies to defend against considering one’s own privileged identity (Watt, 2023). As a model, the PIE argues that different defensive stages occur dependent on information being processed at unconscious, preconscious, or conscious levels of awareness and appear linked to information familiarity (Watt, 2023). These three stages, respectively, are the recognizing (unconscious), contemplating (preconscious), and addressing privileged identity (conscious) stages in the model.
Each stage contains discrete strategies. The recognizing stage contains two strategies: denial and deflection. For example, Watt (2007) describes a denial strategy as stating that something, such as racism, does not exist. The contemplating stage contains three strategies: the first, minimization, distances participants from the issue by reducing its importance. The second, rationalization, occurs when people provide alternative explanations to justify the issue, and the third, intellectualization occurs when the issue is explained using scientific or academic theories (Watt, 2023; Watt et al., 2021). Finally, the addressing stage contains three strategies: false envy, principium, and benevolence. False envy expresses affection or envy regarding the issue or a person who exemplifies it; principium uses values to avoid further examination of the issue, while benevolence uses charity to defend against the issue (Watt, 2023; Watt et al., 2021).
Considering White defensive strategies in relation to RHD, we therefore ask:
We report on qualitative interview data collected as part of a larger exploratory project. That study investigated COVID-19 risk perceptions and information behaviors among White young adults in a high-risk setting for Black and Hispanic communities: Chicago and its suburbs (Chicagoland). This study analyzes the defensive strategies participants employed during our interviews regarding considerations of their COVID-19 experiences as White individuals and COVID-19 RHD information.
Method
Reflexivity
The impetus for this study began when a confluence of events occurred in 2020 for the first author (M.B.D.): in addition to the racial justice protests under the Black Lives Matter banner that swept the United States and identified as one of the largest mass mobilizations on any issue in its history (Shuman et al., 2022), many of my students from Black and Hispanic communities in Chicago were experiencing inequitable COVID-19 impacts. I am an immigrant, and Chicago’s history of redlined segregation and its resultant COVID-19 RHD startled me. 1 I decided to use my power, as a White researcher, to investigate how White young adults might understand their contributions to these inequitable COVID-19 risks and recruited interested collaborators.
This study uses several lenses: systemic racism (Jones, 2002), intersectionality theory (Crenshaw, 1989), and an interpretive approach (Tracy, 2019). Intersectionality theory refers to how multiple identities co-exist together, granting different knowledge, opportunities, and barriers (Crenshaw, 1989), while an interpretive approach assumes that we symbolically and socially co-construct our social reality (Tracy, 2019).
In applying these lenses, team members recognize we are ensnarled within systemic racism and that we necessarily hold White privilege. All of us live in the United States and range from identifying as White to White passing, mixed race, with various intersectionalities from age to ethnicity to expertise. Because of our interpretive approach, we consider our interviews to be co-constructed with our participants, and we recognize that we are, in part, writing about ourselves and our own White privilege (Tracy, 2019).
To address these perspectives, we undertook project reflexivity throughout the project as a key practice of ongoing researcher responsiveness to White privilege (Morse et al., 2002). This reflexivity included ongoing interrogation of our own White privilege and intersectionalities in activities ranging from consulting with experts during research design, to regular team meetings during interviews, thematic analysis, and the review process. We provide an example of such reflection below regarding interviewer and participant racial concordance considerations.
Setting, Sampling, Recruitment, and Interviewing
We chose to focus on Chicagoland because it had the second-highest COVID-19 rate in the United States at the beginning of the pandemic, which disproportionately impacted Black and Hispanic communities (Pierce et al., 2021). We recruited White young adults (18–30) who considered Chicagoland home and who had lived there for at least a month since March 2020. Recruitment tools included our personal networks, Craigslist and Facebook advertisements, a departmental research pool, and alumni list-servs at a medium-sized Midwestern university. Interviews were recruited, conducted and recorded with permission from October 2020 to May 2021, occurring over Zoom or the phone, ranging from 24 minutes to an hour and 40 minutes. Seven interviews were removed as it was discovered during the interviews that those participants did not meet study parameters, resulting in a total of 27 interviews. Pre-testing of the interview guide for clarity and comprehension occurred with graduate students.
Interview topics ranged from COVID-19 information behaviors to risk perceptions. The interview protocol did not ask participants explicitly about their defensive strategies; instead, it asked about inequitable COVID-19 risk burdens. That section of the guide contained questions regarding perceptions of participants’ COVID-19 experiences as White people, as adapted from and in consultation with Raby (2004). For example, one question asked, “What has your experience as a White person been in your community during COVID?,” while another relatedly asked “What about someone who’s Black/Latinx/Indigenous, how do you think they’ve experienced COVID in your community?.” Disparities were also the subject of questions, as exemplified here: “Research shows that Black/Latinx/Indigenous folks have been affected by COVID at higher rates than Whites. What do you remember about learning about this, if at all?”
Because both the interviewers (M.B.D. and E.M.) and our participants classified themselves as White, and many of our interviews were conducted on Zoom, at first glance this study might be presumed to represent White racial concordance. Positivist studies define such concordance as “racial matching” and typically study discordance, that is, what effects interviewers of one race have on interviewees of another racial category; however, researchers from interpretive traditions instead suggest that racial categories are necessarily negotiated and co-constructed during interactions like our interviews (Marcucci, 2024). Given that our study accords with the interpretive tradition, we consider that racial concordance was both afforded and complicated throughout our interviews, by virtue of interview design and our academic intersectionalities.
Specifically, participants exhibited notable tone shifts when we began our last interview section about inequitable COVID experiences. Tone is one of several vocal non-verbal signals of relational communication (Burgoon et al., 2011). We attribute these shifts to how our questions about White privilege foregrounded our academic identities as experts, and also challenged White invisibility norms (Tracy, 2019). White privilege is often experienced as invisible and uninterrogated by those who have it, making White invisibility socially normative in the United States (Phillips & Lowery, 2018). Therefore, consistent with interpretive concordance perspectives (Marcucci, 2024), we suggest that our interviews were sites where racial identity was both co-constructed and negotiated.
Analysis
Using an inductive approach, we applied reflexive thematic analysis to interview transcripts (Braun & Clarke, 2006). Specifically, rather than applying a pre-established set of categories, we searched for patterned meaning in the data via our analysis question: “If participants are defensive about their Whiteness in relation to their COVID experience, what defensive strategy is being used? In other words, how are they being defensive?” (Braun & Clarke, 2006).
Three authors (M.B.D., M.K., and E.G.) acting as coders immersed themselves in the data through activities such as memo writing and open coding (Braun & Clarke, 2006; Strauss & Corbin, 1998). After developing an open codebook, we coded the data and used those coded transcripts to develop initial themes. Specifically, themes were developed by a recursive process of reading through the coded excerpts, interpreting common meaning patterns across codes (Braun & Clarke, 2006). All transcripts were reviewed by two different authors to strengthen the credibility of our analysis (Lincoln & Guba, 1985). Applying accepted standards of trustworthiness in qualitative research, we ensured that our resulting themes were distinct and discrete. The initial list of defensiveness strategies was then refined (by M.B.D. and M.K.) using Owen’s (1984) criteria of “recurrence, repetition and forcefulness”; these criteria help to indicate what participants themselves considered important by emphasizing or repeating aspects of the discussion. Responses were then coded according to the themes, and disagreements were settled by discussion. Upon identifying these defensive strategies, we compared them with the PIE.
Results
We asked what defensive strategies our participants exhibited and identified three major strategies: negation, distancing, and racist intellectualization. The negation strategy had three sub-strategies: direct disregard, equality, and deflection. Below we describe each strategy and orient it to the PIE.
Negation
Negation occurred when participants denied, directly or indirectly, that race was a factor in their COVID-19 experiences. This happened in three major ways.
Direct Disregard
Participants who used this strategy stated race was not pertinent to their COVID-19 experiences. One way they did so was by indicating that they didn’t “see” color: This is going to sound super White of me to say. I never really thought of people based on their skin color or their race. I just see them as a person. If someone who’s Black or Latinx were a good person, that’s all right by my book. But if they make remarks that I don’t like . . . I’m not going to respond to that differently than I would say like a White person that I know who also makes those similar remarks. (Participant 55)
2
This appears representative of colorblindness—a belief that avoiding considerations of race, and associated racial privilege, ensures equality (Hartmann et al., 2017). Participants also denied that their experience of COVID-19 was informed by race, as exemplified by this participant reflecting on being White in relation to their COVID-19 experience: “I think being White, I don’t know. I don’t really know if that has anything to do with it to me” (Participant 115). These approaches seem similar to the PIE’s denial strategy, where the dissonance-evoking issue is explicitly denied (Watt, 2007).
Equality
In this strategy, participants indicated that race did not matter because humans were equally susceptible to COVID-19 infection: “I don’t know if there’s anything that’s going to set me apart, because I’m White when it regards COVID. Because COVID is just a sickness that affects anybody and everybody” (Participant 111). As opposed to focusing on the equality of individuals, participants also noted equality in relation to a larger level of analysis, the community; here a participant discusses equal access to PPE: Well, I don’t think in my community it affects most because I would say my community is pretty equal . . . Even if you can’t purchase those items on your own, there’s other environments that will allow that for you . . . (Participant 112)
We did not find strategies similar to this in the PIE and reflect further on this in our discussion.
Deflection
In this defense strategy, participants conversationally shifted focus from their racial COVID-19 experiences to other types of COVID-19 experiences in two major ways. First, they indicated COVID-19 experiences were not about race but other factors ranging from class to individual decision-making. For example, as a common occurrence, here a participant deflects the issue from race to class when discussing COVID-19 RHD: “So I know low-income areas have been hit hard, but I don’t know who’s in those areas, I don’t know how those kinds of people have been affected, so” (Participant 99). Participants also deflected discussion from their own racial COVID-19 experiences to their knowledge of others’ racism. For example, here a participant deflects from considering her own racial experience of COVID-19 to her inequity literacy relative to her community: . . . I think that the people in this community have never been oppressed before or they don’t realize the kind of things that are actually oppression, like voter suppression, or not getting the same funding that rich towns get or redlining and stuff like that . . . (Participant 114)
These strategies appear similar to the PIE’s deflection strategies, focused on examining another cause for the issue at hand.
Distancing
In this strategy, participants acknowledged that even if RHD existed, they did not affect them and therefore weren’t considered important—in this way, distancing themselves from the issue. Participants often noted community or neighborhood racial structure as central to this experience: So the demographic of my community is mainly Caucasians. So I never really experienced anything regarding the race in COVID. The two never correlated, at least in my community or my world, necessarily not that it wasn’t going on, but I don’t have any specific instances in my life where those two paths crossed. (Participant 125)
These structures led to a lack of diversity among social networks, leading to distance, as noted by this participant discussing their lack of knowledge about Black or Hispanic experiences of COVID-19 in their community: “. . . the area that I live in is predominantly White. And so I’m not sure that I’m informed enough to give a good answer on that” (Participant 127). This subsequently contributed to a perceived lack of salience regarding the issue, as this participant noted when discussing their COVID experience as a White person: “. . . in my neighborhood, White people, there aren’t a lot of diversity . . . so I feel like it hasn’t really affected me as much” (Participant 11). This strategy appears similar to what Watt and colleagues (2009, 2021) call minimization, where facts are used to downplay the importance of the information.
Racist Intellectualizing
In this strategy, participants attempted to explain racial COVID-19 disparities using “facts” or “data” rooted in racist “biological” tropes. As an example, one participant pointed to differences in immune systems: I’m not a doctor, so I don’t really know too much about it . . . I don’t know if it’s just they have the different immune system that makes it harder for them to fight COVID than other races, I guess. (Participant 131)
Another participant explicitly pointed to racial “biology” as a key issue: “I think there’s a lot of factors . . . it might have to do with biological, for all we know” (Participant 128). This seems similar to the PIE’s intellectualization strategy, where scientific theory suppresses emotionally relating to the issue (Watt et al., 2021); in this case, pseudo-scientific theories were used.
Discussion
Using the PIE as a lens to understand our results, our interviews yielded three findings. First, we identified a defense strategy the PIE has seemingly not considered: equality. We also found similarities between some of our strategies and the PIE’s, strengthening their validity across contexts (Strauss & Corbin, 1998). In addition, we identified nuances in our strategies not yet noted in the PIE literature, that might be specific to RHD contexts. Finally, we did not identify any strategies indicative of the PIE’s addressing the privileged identity stage, suggesting our findings may be most applicable for those newly considering their racial privilege in relation to RHD information.
Strategy the PIE Should Add: Equality
We identified a defensive strategy, equality, that psychological and sociological literature notes as key for Whites relative to White privilege (Bonilla-Silva, 2010; Knowles et al., 2014) but is not yet noted in the PIE literature. Participants invoking an equality strategy did so in line with its conceptualization as a moral value (Feinberg & Willer, 2019), which researchers have shown supports White merit myths: where social standing is attributed to hard work and abilities, rather than inequitable social stratification (Phillips & Lowery, 2018). We suggest RHD researchers include this strategy in an expanded PIE model moving forward.
Similar Strategies, Different Nuances
Similar to the PIE, we found strategies of denial and deflection, representing the PIE’s negation stage, as well as strategies of minimization (which we call distancing) and intellectualization, representative of the contemplating privilege stage. Each strategy has nuances not noted in the PIE literature, which may be specific to RHD contexts. Here, we briefly describe these distinctions.
Negation: Direct Disregard Through Colorblindness
Our participants employed colorblindness, consistent with the 72% of White Americans who identify as colorblind (Hartmann et al., 2017)—yet colorblindness is not yet noted in the PIE literature. We suggest future research should assess colorblindness’ prevalence as a negation strategy, while practitioners could prepare themselves to encounter colorblind negation strategies.
Distancing Through Social Structure: Redlining
Participants used the distancing strategy to downplay the importance of RHD information, similar to the PIE’s minimization strategy (Watt, 2023). Instead of focusing on a variety of facts for such a strategy, our participants largely focused on structural facts—how neighborhoods, communities, and social networks distanced them from engaging with COVID-19 RHD information. This resigned distancing appears to be the legacy of generations of segregated redlining in Chicago (Pierce et al., 2021), and future PIE research should consider how participants’ experiences with structural segregation affect their distancing strategies.
Intellectualizing Through Racist “Scientific” Tropes
Intellectualization strategies, as described by the PIE, use scientific evidence; in contrast, our participants used pseudo-scientific racist tropes. Our findings are in line with research showing that RHD structural attributions are often discounted in favor of biological or genetic ones (Gollust et al., 2020), making this a likely type of intellectualization strategy in the face of RHD information.
What Was Not Found—Addressing Privilege Strategies
We did not identify any strategies representative of the PIE’s addressing privileged identity stage. Upon reflection, we suggest this may be because compared to Watts’ original participants, on whom the model was based and who were consciously wrestling with privilege over a semester in a multicultural classroom, many of our participants hadn’t heard about COVID-19 RHD information. Therefore, for some, their defensive strategies seemingly occurred in the context of unfamiliar information, which the PIE suggests invokes unconscious and preconscious information processing and related strategies. To our knowledge, no research has yet examined this PIE claim, providing a future avenue for investigations.
Limitations
While our findings suggest that information (un)familiarity may be associated with the PIE’s unconscious and preconscious stage strategies, we did not design the study to investigate strategies in relation to information processing stages, and we acknowledge this as a limitation. Further studies that investigate the relationships between information processing, familiarity, and strategy types are needed. Second, our sample represented young adults, and different strategies may be employed by differently aged people; however, we note that a key factor in the policy space—staffers—are often White young adults (Brenson & Victor, 2023; Federal Managers Association, 2024), and these strategies may therefore be employed by them. Further research is needed to tease out whether strategies differ by age, and if so, how.
Implications for Practice
Health promotion practitioners in the RHD policy change advocacy space want their advocacy efforts to be successful, and White defensiveness strategies represent a potential barrier to such efforts. We have therefore chosen to focus on how practitioners can use our findings in the service of key elements of policy change advocacy communication: segmentation, messaging, and strategy stages.
Segmentation
First, practitioners can use our findings to develop segmentation strategies, which differentiate groups and customize communication efforts so that they resonate with that specific audience, or avoid activating a particular defensive strategy (Slater, 1996). One method of segmentation uses audience behaviors, which these defensiveness strategies represent. Practitioners could therefore segment White audiences based on, for example, whether they are more likely to deflect or use colorblindness when learning RHD information. In the service of such detailed segmentation by practitioners, future research could investigate the importance and relevance of these strategies to different White audiences.
Such segmentation offers practitioners opportunities to consider both how to mitigate such defensiveness strategies and how to respond. For example, practitioners developing a recruitment strategy for grassroots advocacy in a neighborhood and expecting high deflection levels from White community members could train recruiters to expect deflection strategies. Another way to respond is to reframe messages, which we turn to next.
Message (Re)framing
Reframing messages entails changing a message’s values to more closely align with its intended audience(s)’ values (Feinberg & Willer, 2019). When practitioners encounter value-based defensive strategies among White audiences, we suggest this may be a useful practice. For example, to reframe equality strategies, advocates could discuss harms caused to communities of color by inequities, and a commitment to care about these harms through policy change efforts, evoking a harm/care moral frame (Feinberg & Willer, 2019). Current research offers clues that reframing could be an effective practice: for example, a recent meta-analysis of RHD messaging studies found that messaging that describes the harms current policies enacted on Black people, along with a commitment to address racial discrimination (seemingly a harm/care frame) were associated with policy change support (Niederdeppe et al., 2023). To assist with this work by practitioners, future research could investigate which value-based defensive strategies are most open to reframing efforts.
Strategy Stages
Finally, our findings suggest practitioners should consider how familiar their White advocacy audiences are with RHD information to plan for the defensive strategies they are likely to encounter. We did not identify strategies associated with the addressing privilege stage, likely because compared to Watts’ original participants, many of our participants seemingly experienced COVID-19 RHD information as unfamiliar. Unfortunately, we do not yet have research confirming that the PIE’s information stages are associated with specific defensiveness strategies. In the absence of such knowledge, we recommend practitioners undertake formative research on RHD knowledge familiarity among different White audiences to forecast strategies they are likely to use, per the PIE. For example, initial community engagement efforts with White publics where RHD information is unfamiliar will likely manifest strategies associated with unconscious processing, compared to meetings with White policy makers familiar with the topic and more likely to use conscious processing strategies. These considerations can inform advocate training about defensive strategies likely to be encountered during communication interactions.
Conclusion
Overall, this study identified and detailed White defensiveness strategies relative to RHD. As a theoretical contribution, our findings suggest these strategies occur in ways both predicted by the PIE and that also inform nuanced exploration and testing moving forward. Practically, our findings show promise for informing practitioner efforts to address White defensiveness as a communication barrier in policy change advocacy efforts. We hope researchers will view this study and its implications for RHD policy change advocacy as encouragement for future work in this area.
Footnotes
Authors’ Note:
We would like to thank Dr. Rebecca Raby for consulting with us regarding interview questions.
Ethical Approval
The study was approved by the Illinois State University IRB as exempt; consent was obtained from all study participants.