
Abstract
As calls for improved menstrual health management have gained momentum in sociopolitical contexts, period poverty and menstrual equity have gradually been established and recognized in the discipline of public health. These conversations typically take place in the context of low- and middle-income countries (LMICs) where donor-sponsored projects are already underway. Nevertheless, research on period poverty in high-income countries (HICs) is seldom performed. In addition, current literature on the topic tends to generalize HICs and LMICs, thereby ignoring crucial cultural and socioeconomic distinctions that necessitate a more detailed comparison of individual countries facing period poverty. This case examines the current body of research on period poverty in the United States and India, and compares the causes, effects, and approaches toward ameliorating this phenomenon. Through performing a scoping review of the current literature on period poverty, this case illustrates that—as opposed to the breadth of research available on period poverty in LMICs—research on period poverty in HICs is underrepresented. In addition, the findings demonstrate a stunning parallel between the contributing factors of period poverty in India and the United States, suggesting that the current approach to isolate conversations on the topic based on regional economic incongruencies is inappropriate. Finally, this case identifies dismantling the stigmatization of periods, investing in water or hygiene infrastructure, promoting the economic mobilization of females, and reforming menstrual health curricula in schools as essential to ending period poverty.
Keywords
Background
According to the World Bank (2022), approximately 500 million women and girls face period poverty due to a lack of menstrual products (MP) and proper water, sanitation, and hygiene (WASH) facilities. By definition, period poverty denotes a lack of appropriate menstrual health management (MHM) (Tull, 2019). As defined by the United Nations Children’s Fund (UNICEF), four elements are essential to ensuring satisfactory MHM: social support, knowledge and skills, facilities and services, access to absorbency materials, and provision of resources that address the side effects of periods, such as lower abdominal cramps. In addition, UNICEF underscores the necessity of sanitation, distinguishing as mandatory the following criteria: access to sanitary MP that can effectively absorb blood, private facilities conducive to changing MP, soap and water for cleaning the vaginal area, proper disposal for used MP, and educational resources that enable individuals to navigate menstruation comfortably and without fear (Tull, 2019).
In low- and middle-income countries (LMICs) and high-income countries (HICs), women and girls experience various setbacks due to menstruation. These limitations—extending from socioeconomic to educational barriers—collectively inhibit menstruators’ social, religious, cultural, and economic mobility (Hennegan et al., 2019). The high price tag on designated period products and lack of sociopolitical will to designate MP as free or discounted impose significant economic responsibility on menstruators (Weiss-Wolf, 2020). In addition, generational reluctance or refusal to educate boys and girls about menstruation has manifested in poor menstrual health (MH) knowledge and reinforced inaccurate social taboos that deem menstruators “dirty” and “impure” (Mohammed & Larsen-Reindorf, 2020). Finally, many public spaces, such as schools, lack proper WASH facilities. As a result, women in LMICs and HICs often experience poor MH, which contributes to urogenital infections, sentiments of shame and embarrassment toward menstruation, and unsatisfactory female education due to school absenteeism during menstruation (Hennegan et al., 2019). These negative consequences underscore the broader failure of politicians and academia to address period poverty as a public health crisis. A more critical approach toward ameliorating period poverty would promulgate female empowerment through forging economic and social advancements for women globally.
In India, adolescent girls ages 10–19 years compose an estimated 10% (120 million people) of the population, 52% of which were not aware of menstruation before menarche (Sivakami et al., 2019). Cultural taboos especially limit women’s ability to discuss menstruation openly and contribute to reports of women feeling anxious regarding the disposal of period products, experiencing pressure to conceal their menstrual status, and facing social regulations that deem them unfit to participate in various household and religious tasks (MacRae et al., 2019). As a result, 25% of adolescent girls in India skip school during their menstrual cycle (Sivakami et al., 2019).
In the United States, period poverty predominately affects lower-income individuals and is bolstered by the “tampon tax” in place in 21 states. The tampon tax refers to the imposition of sales tax on sanitary items; other items—deemed “necessary”—bear a smaller or non-existent sales tax (Alliance for Period Supplies, n.d.). The lack of coverage for period products by the Supplemental Nutrition Assistance Program, Medicaid, and health insurance presents another financial barrier for the 42 million impoverished women in the United States (Smith, 2019). Likewise, the 2023 State of Period—the only open access report on the scale and repercussions of period poverty among American teens—concluded that one in three adults and one in four teens surveyed struggled to purchase period products, which remains consistent with researchers’ findings in 2021. The study additionally found that—like their Indian counterparts—women in the United States face widespread discrimination due to their period. Finally, the study concluded that 58% of teens reported that “the world is not set up for them to manage their periods with full confidence,” while 60% of adults reported negative perceptions of their body as a result of the stigmatization of menstruation (Team Thinx, 2023).
The growing attention toward period poverty in academia has contributed to a breadth of research and fieldwork on the topic, specifically sponsored by donors such as UNICEF (United Nations, 2023). Nevertheless, there is a lack of attention toward period poverty’s role in HICs. In a review that cited literature on MHM from 35 countries, every country was an LMIC, and only one was in Europe (Hennegan, 2017). Similarly, Tull (2019) analyzed literature from countries where UNICEF-sponsored projects were underway; much like the article by Hennegan (2017), every participating country was an LMIC. Given the limited body of literature on period poverty in HICs, more research should be performed to assess the current state of MHM in each country to inform policy legislation. Considering the dearth of research available on MHM in HICs, public health leaders and policymakers should consider existing interventions when developing theoretical frameworks for eliminating menstrual inequality.
Through analyzing the state of period poverty in the United States and India, this scoping review aims to compare the experiences of women facing period poverty in the United States with women in India to (a) identify the leading contributors to period poverty in these distinct regions, (b) compare and contrast documented experiences of period poverty between high-income and low- and middle-income economies at both population and community levels, and (c) synthesize the findings to inform policy recommendations and interventions aimed at addressing period poverty. A scoping review has been deemed most appropriate in the context of these aims and the nature of the study, which is to determine and evaluate the current body of literature on period poverty in India and the United States.
Method
Search Strategy and Selection Criteria
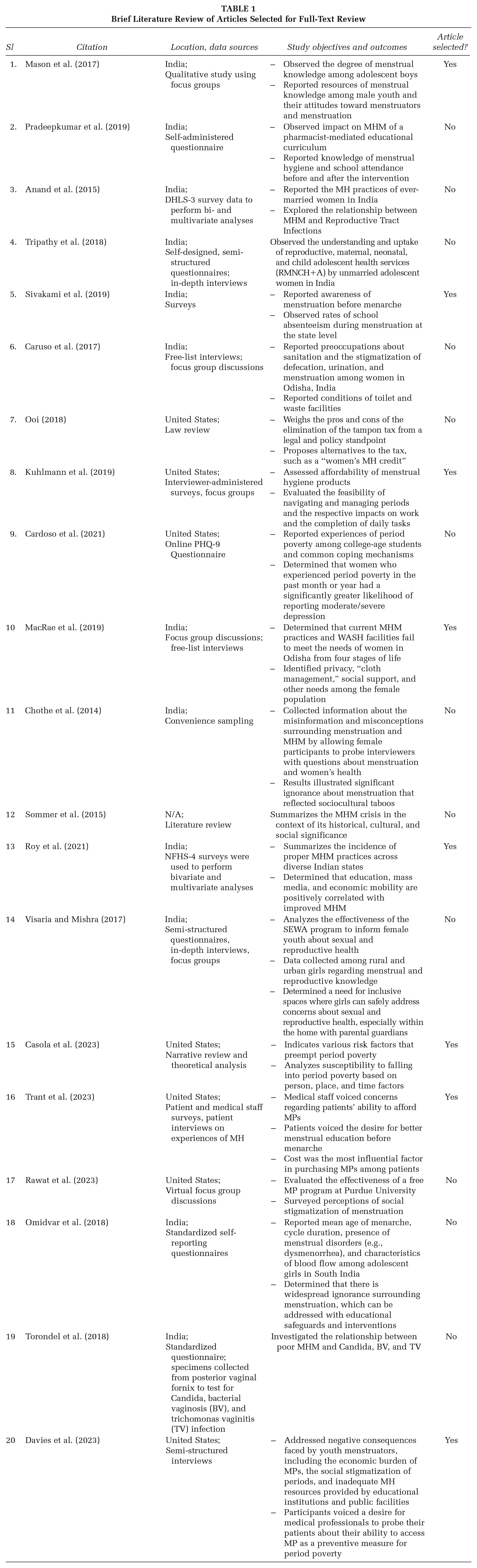
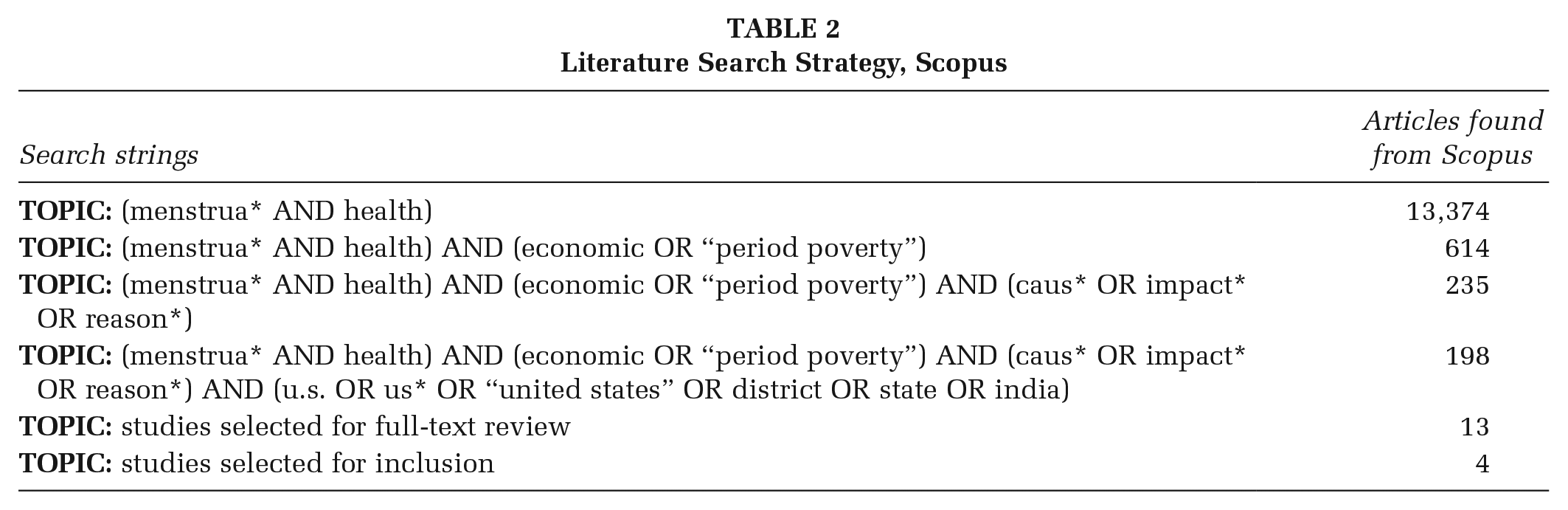
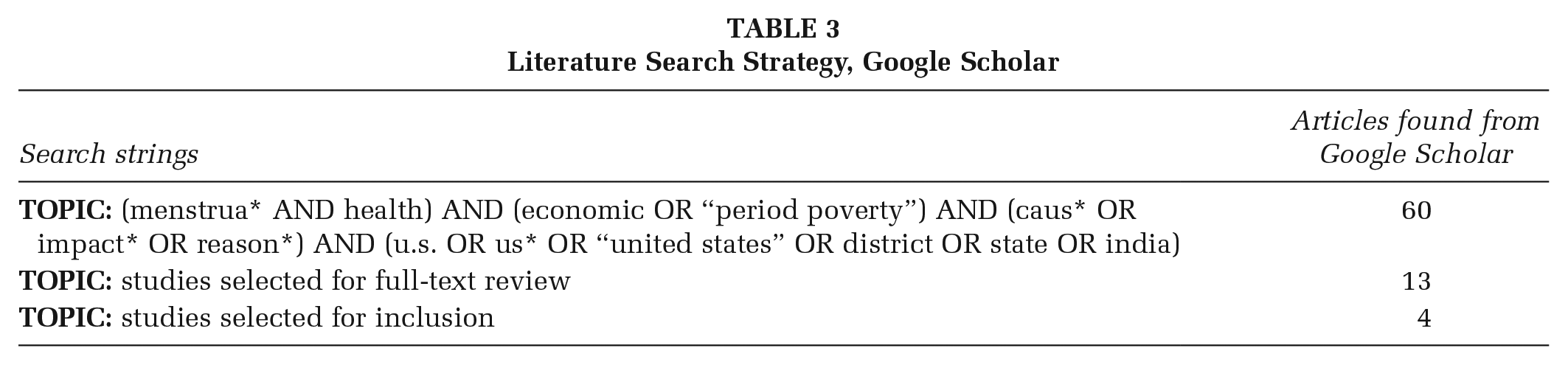
In this scoping review, Scopus was employed by one reviewer to search for peer-reviewed literature, while Google Scholar was used to extract gray literature between December 2023 and January 2024. To ensure thoroughness, the other author double-checked the screening process to confirm no relevant articles were missed. During the initial abstract and title screening phase, inclusion criteria included research articles that adhered to the following guidelines: written in or translated into English, relevant to the two countries of interest (i.e., India or the United States), identified or analyzed potential causes and effects of period poverty in the countries of interest, and published between January 2013 and December 2023. This timeframe was selected in light of the significant strides made to ameliorate period poverty in the past decade that would potentially deem older articles inappropriate for inclusion. Review articles were excluded in addition to research articles on the following topics: COVID-19’s impact on period poverty, the intersectionality between MHM and the feminist movement, and health-related topics irrelevant to the research question (e.g., menstrual disorders, abortion, etc.). There were no exclusion criteria for sample size. Relevant findings from each included study were summarized in a table in the full-text screening phase of the review (see Table 1). Data were imported, screened, and extracted using Covidence’s systematic review software (Veritas Health Innovation, 2014). The search strategy employed is detailed below in Tables 2 and 3 in addition to the PRISMA diagram (see Figure 1).
Brief Literature Review of Articles Selected for Full-Text Review
Literature Search Strategy, Scopus
Literature Search Strategy, Google Scholar
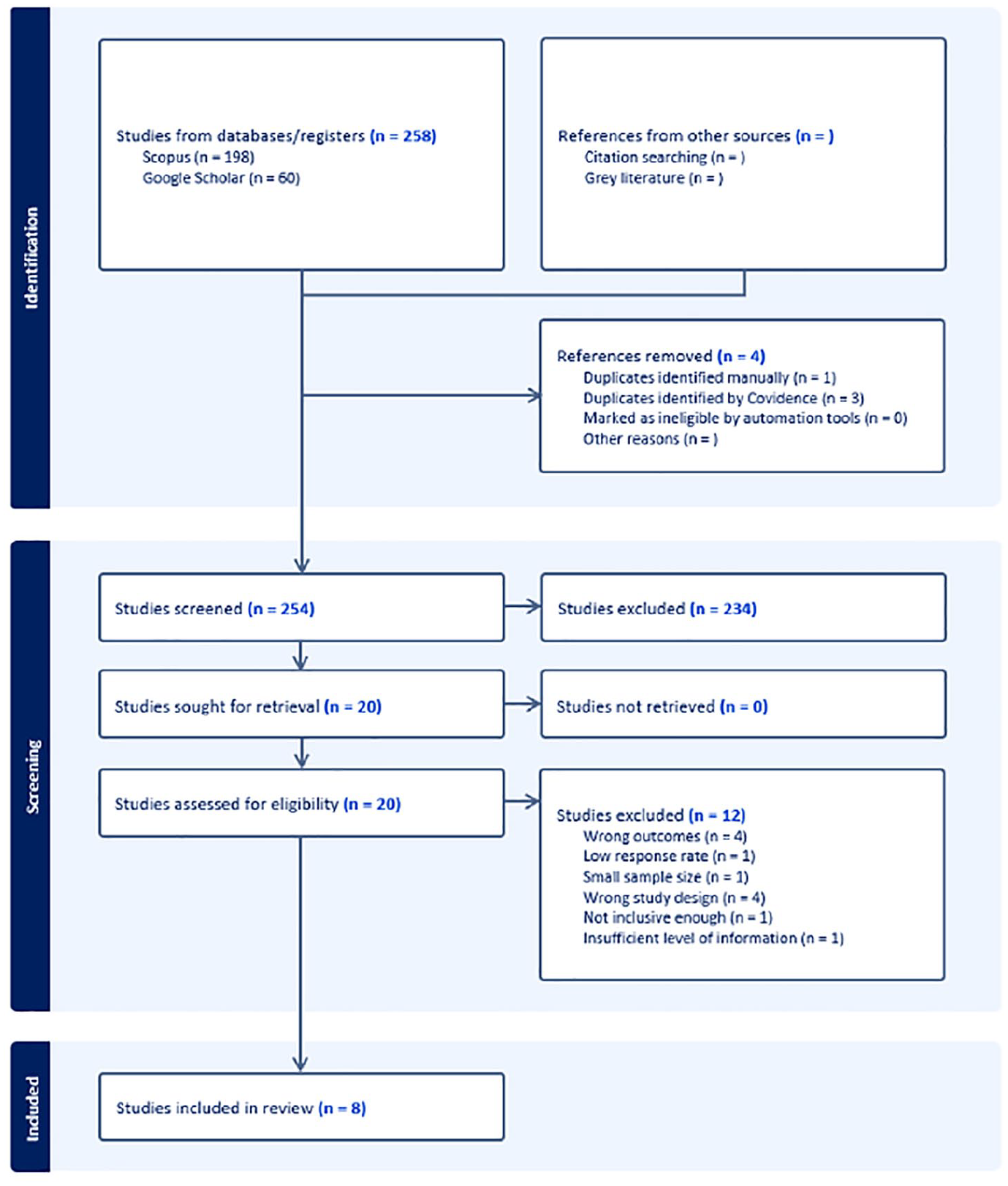
PRISMA Diagram
Deviations From the Protocol
Initially, the study aimed to assess the causes of period poverty among adolescent populations in the United States compared with India. On completing a preliminary search, however, there was a lack of scholarly work targeted toward youth populations suffering from period poverty and poor MHM in the United States. As a result, the scope of the review was expanded to include studies with participants of all ages, not explicitly adolescents.
Study Selection
The PRISMA diagram in Figure 1 details the three stages of selection: screening, eligibility assessment, and inclusion. The majority of studies screened and included were extracted from Scopus, while a minority were extracted from Google Scholar. The PRISMA diagram defends the exclusion of certain literature during the inclusion stage by drawing attention to relevant exclusion criteria.
Results
Selection Criteria
Of the 258 articles identified for screening, 198 were extracted from Scopus, and 60 were extracted from Google Scholar. Four of these articles were removed as duplicates, and the abstracts and titles of the remaining 254 articles were screened for selection. Notably, 20 articles were selected for full-text screening, 8 of which were included in this scoping review. The 12 excluded articles were deemed inappropriate for inclusion due to the following exclusion criteria: wrong setting, wrong outcomes, low response rate, wrong study design, not inclusive enough, and insufficient level of information.
Lack of Social Support
The needs of Indian women during menstruation are frequently dismissed due to social taboos that deem girls impure and, in some cases, temporarily bar them from certain activities. In a recent study, Roy et al. (2021) noted that the greatest factor influencing the MH practices of Indian women was the desire to avoid menstrual stains. Similarly, MacRae et al. (2019) found that the desire to conceal menstrual status predominated among participants of all four age groups included. Women also voiced concerns regarding the lack of privacy within their homes, limiting the ease at which they could change their MP. Accordingly, many women ventured outside of the house to change. Such was the case of one of the participants who went to a cow shed when she had nowhere else to change; another woman recounted that she hid a dirty MP in her underwear so people would not suspect her menstrual status on returning home. In addition, many women reportedly disposed of MP in “sludge,” ponds, or mud to prevent their family and community from determining their menstrual status. They similarly went to great lengths to hide stained clothes by throwing them in the dirt, bamboo sheds, or on the roof. Women stated that they preferred these practices over their own health, claiming that despite their knowledge that sunlight is necessary to kill harmful bacteria lingering on stained garments, they would prefer not to risk publicizing their menstrual status (MacRae et al., 2019).
Mason et al. (2017) cited a similar reaction of shame toward the topic of menstruation, explaining that most adolescent male participants initially answered incorrectly when probed about whether or not they knew what menstruation was, suggesting a perception of menstruation as embarrassing or shameful. In addition, some respondents shared views of menstruation as a “disease” representative of “uncleanliness,” although this was a minority opinion. As a result of the social, religious, and cultural stigmatization of periods, Indian women experienced various hindrances to their daily lives during menstruation. Many women were barred from cooking, entering certain spaces, handling food, and completing other household tasks. Likewise, many women felt like a burden when forced to ask neighbors or family members to complete tasks for them. Nevertheless, many women remained hesitant to do so, given their fear of disclosing their menstrual status.
A significant number of women in the United States face similar experiences of social stigmatization, albeit to a lesser degree. Casola et al. (2023) found that many girls shied away from asking questions and learning about menstruation, given the shame associated with the topic. Similarly, participants in a study by Trant et al. (2023) noted that the taboo nature of menstruation and fear of revealing an individual’s menstrual status prevented many women from going to school and other events. Not only did the participants lose out on an opportunity for social and educational engagement but the authors cited that many participants felt emotionally distressed by feelings of having “missed out.” Moreover, Indian and American menstruators voiced similar experiences of social isolation and exclusion as a result of the lack of social support for menstruation, which collectively pose dangerous implications for the mental and physical health of women in both countries.
Lack of Proper Sanitation and WASH Facilities
The lack of sufficient WASH facilities presents an additional barrier to menstrual equity in LMICs and HICs that warrants consideration. In a study by Sivakami et al. (2019), 45.7% of participants reported that their schools lacked enough toilets to address menstruation. This reality could be attributed to various factors. For example, when asked if they could wash themselves at school when leaking, only 51% said yes, 17.2% said sometimes, and 28.1% said never. In addition, the lack of an adequate number of toilets, clean water, and male- and female-segregated bathrooms—considering that 21.9% reported that their bathrooms were mixed-gendered—may contribute to the unsatisfactory state of school restrooms. Finally, the authors noted that long lines and a lack of clean restrooms negatively affected participants’ perceptions of bathroom facilities.
The presence of proper disposal facilities is an additional aspect of MHM. The findings by Sivakami et al. (2019) underscore the inadequacy of disposal services in the schools selected for the study. Likewise, merely 27% of respondents were satisfied with their school’s disposal facilities, while 21% of girls were forced to take their used MP home, 20% put them in burn pits, 17% in trash pits, 16% in trash cans, and 7% in incinerators. In the context of the stigmatization of periods, women were not only deprived of a remedy to dispose of soiled products but were also forced into a position where they could have been “outed” by having to carry these items to disposal areas outside of the bathroom.
In a study conducted among women and girls ages 13–24 years in the United States, one respondent reported that dispensers for pads and tampons “were empty” and “the trash cans didn’t have a bag in [them]” (Davies et al., 2023). Likewise, Casola et al. (2023) noted that 20% of female respondents living in the United States felt that schools did not do enough to promote MHM. Many girls surveyed were forbidden from leaving class to change their period products, forcing them to sit unhygienically in their own blood and develop stains on their clothing that ultimately promulgated sentiments of embarrassment. Some girls even reported being punished by professors or threatened with punishment (i.e., detention) after they missed the beginning of class because they were changing their MP. As a result, many American girls opted to skip school because of inadequate WASH facilities and access to MP. Schoolgirls in India reported comparable issues in the study by Sivakami et al. (2019), where 38% of respondents stated that there was not enough time during breaks to change period products, 30.4% said that they could not leave class if they were leaking, and 54% said that they could only go to the toilet during breaks. Overall, Indian and American schoolgirls demonstrated sizable dissatisfaction with public facilities’ ability to accommodate them during their menstrual periods.
Financial and Accessibility Barriers
The cost of MP presents a considerable challenge for many Indian menstruators, with women voicing concerns about the high price and distant location of stores that sell quality products (MacRae et al., 2019). As one participant explained: We are poor people. So father cannot provide pad. How can we say that we have to bring pad with father’s money? We can’t say. We bring occasionally during rainy season, other times we adjust. (Unmarried woman in the free-list interview)
Hygienic solutions are neither accessible for purchase nor available in local schools, considering that only 37% of participants could receive pads at school in a study by Sivakami et al. (2019). The financial barriers presented by maintaining proper MHM likely explain why 72.6% of participants in the study by Roy et al. (2021) used cloth—a material the authors deemed “unhygienic”—as opposed to tampons, locally prepared sanitary napkins, or generic sanitary napkins. The same study found that women from the highest quintile of household wealth were nearly nine times more prone to practicing good MHM than women from the lowest quintile.
In a study by Trant et al. (2023), female patients voiced similar concerns about the financial burden imposed by MP. However, 54% of women revealed that they were unable or were suspected of having been unable to afford sanitary products, while 22% of patients were classified as “MH insecure,” given that they could “sometimes” or “most of the time” not afford MP. Likewise, many participants reported having to use alternatives to designated MP; as one participant stated: I would have to use toilet paper and it sucked because it would always get stuck on me and I would have to take a shower and all that. Like not comfortable. (Participant 04)
Inadequate access to MP often forces women to use MP for a prolonged timespan or to use alternatives, such as cardboard or rags. Accordingly, many women develop urogenital infections and diseases, such as bacterial vaginosis and toxic shock syndrome, which propagate more expenses (Casola et al., 2023). A study conducted among a group of low-income women in St. Louis determined that 64% of participants could not afford MP at least once throughout the year prior, and 21% faced this challenge monthly. In addition, one third of participants resorted to using alternatives such as those mentioned above instead of proper MP (Kuhlmann et al., 2019). Likewise, the literature illustrates the immense economic burden of MP among both Indian and American menstruators, which ultimately impedes the feasibility of practicing satisfactory MHM.
Inadequate MH Education
The insufficient MH curricula and lack of credible resources provided to youth additionally contribute to period poverty in India and the United States. Poor MH education not only leaves women unprepared for menarche but also reinforces the social stigmatization of periods, particularly through the exclusion of males from the conversation. Sivakami et al. (2019) found that only 56% of girls in model schools and 36% of girls in regular schools knew about menstruation before menarche. Likewise, only 34% of girls reported obtaining MH education in school. Nevertheless, exposure to mass media, literacy, and higher education increased MH practices, the latter two by five times compared with illiterate individuals in their respective communities (Roy et al., 2021).
Despite poor MH curricula, the literature suggests an eagerness among male and female youth to obtain such education. In a study by Mason et al. (2017), boys voiced a desire to learn more about menstruation, often asking interviewers questions or voicing discontent with the current approach toward MH education. This response parallels the female participants’ response in the study by MacRae et al. (2019), in which women asked interviewers questions regarding menstruation, such as “if it does not happen on date, then is it a problem.”
Many women and girls in the United States also feel discontented by inadequate MH education. As is the case in India, most girls in the United States receive their menstrual education from their mothers, schoolteachers, or peers. Nevertheless, Trant et al. (2023) found that many participants felt that their menstrual education was sporadic and failed to prepare them for menarche. In addition, young women voiced a desire for males to receive MH education and thereby dismantle sentiments of “disgust” that circulate around menstruation (Davies et al., 2023). Low-income participants voiced similar concerns and stressed the importance of improved MH education and awareness (Kuhlmann et al., 2019). The strong desire for improved schooling designed to equip them with menstrual knowledge among Indian and American menstruators demonstrates a compelling need to reevaluate the current educational systems in place.
Discussion
This scoping review aimed to satisfy three objectives: (a) identify the leading contributors to period poverty in India and the United States, (b) compare and contrast documented experiences of period poverty between high-income and low- and middle-income economies at both population and community levels, and (c) synthesize the findings to inform policy recommendations and interventions aimed at addressing period poverty. Although India and the United States differ in per capita income, population, and health care systems, the results of this scoping review illustrate stunning parallels between the state of period poverty in both regions. Primarily, the literature indicates mutual factors correlated to period poverty in the respective countries. These include a lack of social support, a lack of proper sanitation, and WASH facilities—notably proper bathrooms in LMICs and access to disposal areas and hygiene products in both LMICs and HICs—financial and accessibility barriers, and inadequate MH education. Hennegan et al. (2019) corroborate these findings and underscore the necessity of addressing the social stigmatization of MHM, expanding MHM research beyond an adolescent demographic, and investing in research that identifies the biological consequences of period poverty (e.g., BV and various sexually transmitted infections [STIs]). The study additionally pinpoints the necessity of pursuing both an education- and products-centered (i.e., distributing free MP) approach to achieving sustainable developments in the areas of MHM and menstrual awareness. These findings provide depth to the second purpose of this scoping review, which is to examine the extent to which the economic status of a country can be treated as an appropriate predictor for period poverty.
Although the United States faces less per capita period poverty than India, this scoping review suggests that the relationship between economic growth and proper MHM is ambiguous. The results demonstrate that women in India and the United States face period poverty at significantly high rates, both of which can be attributed to inadequate policy measures. In India and the United States, period poverty is the direct product of the governments’ failure to prioritize MHM from a public policy standpoint by implementing social welfare and educational reform. Riley et al. (2020) found the following consistencies regarding the impediments to menstruation: the desire to conceal menstrual status, promotion of social taboos and stigmatizations, and finally, unsatisfactory MHM. Akin to the experiences faced by Indian menstruators, the study’s findings suggest that structural gender inequality—as opposed to gross domestic product (GDP)—is liable for the respective period poverty crises. Crawford et al. (2020) affirm this conclusion, citing the necessity of addressing structural gender inequalities rooted in the U.S. legal system. Nevertheless, the authors stress that judicial reform must be coopted by enforcement and the monitoring and evaluation of policy frameworks, including the provision of free MPs in New York, which, despite becoming legislation in 2019, failed to be implemented in 82% of facilities (Crawford et al., 2020). Similarly, a systematic review largely including LMICs cites the failure of public health officials to work alongside the legal system to ensure enforcement as a crucial hindrance to ameliorating period poverty (Valipour et al., 2023).
The literature additionally demonstrates that there is a dearth of literature on the topic of period poverty in the United States. Of the 254 articles screened for inclusion, only 15 discussed menstrual inequality in the United States. Nevertheless, nearly every other article examined period poverty focused on the context of LMICs. This gap in the literature underscores the U.S.’ complicity in relegating period poverty to the private—rather than public—sector. Despite the public appeal, the U.S. Congress insists on imposing the burden of menstruation entirely on women by rejecting legislation that allocates the provision of accessible period products. Crawford et al. (2020) attribute this failure to a narrow understanding by non-menstruators of the dynamic and unpredictable “nature” of periods that often leave women distressed if they cannot readily find MP. Likewise, the absence of health care and educational reform within the Indian government further emphasizes the necessity of both countries’ recognition of and response to period poverty as a public health crisis. By assigning the burden of ameliorating menstrual inequality to NGOs, governments have silently affirmed poor frameworks that champion shipping mass quantities of period products to LMICs and thereby neglect educational reform (Chandra-Mouli et al., 2019). Consequently, many schools are complicit in neglecting MHM guidelines, underscoring a need for comprehensive research in academic settings to inform future policy frameworks (Sharma et al., 2020). Governments, therefore, must work alongside NGOs to create solutions to period poverty that bolster sustainable and generational reform.
Overall, promising strides toward ameliorating period poverty have been made in recent years in LMICs and HICs. Nevertheless, significant work remains to be done from both a policy and socioeconomic standpoint that can only be accomplished through broader recognition of period poverty as a public health crisis. In addition, more time must be invested in ongoing R&D efforts centered around period poverty. Through fostering a community-based approach toward ameliorating period poverty, policymakers and public health officials can implement more demographic-specific reforms, eliminating some of the negative consequences of pursuing a universal approach (Khorsand et al., 2023). Promising research is already underway, including an intervention that found a positive correlation between the provision of MH products in the workplace and yearly revenue due to fewer absences by female employees (Eaton et al., 2023). In addition, the Indian company Jayaashree Industries has developed a low-cost machine that produces sanitary napkins with the objective of employing “bottom of the pyramid” women while simultaneously providing low-cost MP to rural areas (Goyal, 2016). Finally, studies on banana fiber pads have proven to be a viable solution to the environmental, financial, and health care consequences of period poverty (Achuthan et al., 2021). Nevertheless, compliance and uptake must be evaluated considering demographic distinctions among sample populations, given that the study mostly selected women with satisfactory MHM practices.
This scoping review has several limitations that warrant consideration. First, the inclusion criteria were restricted to articles published in English, which may exclude relevant studies conducted in other languages that could offer additional insights into the topic. Second, the study aimed to assess the causes of period poverty among adolescent populations in the United States compared with India. However, we deviated from this goal due to a dearth of scholarly work. Finally, due to the nature of scoping reviews, this study did not assess the quality of the included articles. The absence of quality appraisal means the findings are based on the available literature without evaluating the evidence’s strength or reliability. Despite these limitations, this review provides a comprehensive overview of the existing literature on period poverty in India and the United States.
Conclusions and Implications for Practice
The findings of this scoping review illustrate that by addressing the leading contributors to period poverty, India and the United States can benefit immensely on a socioeconomic scale. Given that improved female education is a cause and effect of good MHM, schooling should be at the forefront of public health approaches toward ameliorating period poverty. Moving forward, the nature of interventions geared toward addressing menstrual injustice must transition from reactive to proactive, starting with reevaluating hygiene curricula in schools. Based on our findings, the following health promotion policies or practices can be considered:
1. Curriculum Development:
– Develop, evaluate, and integrate comprehensive MH and hygiene education into the national curriculum, ensuring that it covers biological, social, and emotional aspects of MH.
– Train teachers and health educators on delivering MH education effectively, using culturally sensitive and age-appropriate materials.
– Collaborate with public health experts to enhance the quality and relevance of the curriculum and training content.
2. WASH Infrastructure Improvement:
– Mandate that all public buildings, especially schools, meet minimum standards for WASH facilities to support MH.
– Conduct regular assessments of WASH facilities in schools and public spaces, ensuring they are clean, safe, and equipped with necessary supplies for MHM.
3. Public Sentiment and Cultural Change:
– Develop national health promotion campaigns to educate the public about MH and reduce stigma, supported by government endorsements and media partnerships.
– As highlighted from the work by Casola et al. (2023), engage community leaders and influencers to advance evidence-based health promotion programming to shift societal perceptions and promote positive attitudes toward menstruation.
4. Research and Development:
– Increase funding for research on MH to identify effective interventions, understand the diverse needs of different populations, and fill the gap in the current body of research in this setting (Sommer et al., 2019).
– Partner schools and public health agencies with research institutions to pilot and evaluate new MHM interventions, using findings to inform policy adjustments and best practices.
Despite menstrual education’s current role in reinforcing period poverty, the reevaluation of MH curricula in schools forms the backbone of future policy aimed at addressing period inequality. Moving forward, the nature of interventions geared toward addressing menstrual injustice must transition from being reactive to proactive. Likewise, educational environments serve the purpose of shaping girls in regard to their personal, societal, and global perspectives. Nevertheless, investment in R&D efforts remains fickle in schools despite ongoing limitations in the current body of research in this setting (Sommer et al., 2019). Therefore, Public health officials must undertake efforts to target schools in both R&D and policy measures to foment sustained improvements to MHM in India and the United States.