
Abstract
HIV disproportionately affects adolescent girls and young women living in Southern Africa. Rates of perinatal HIV transmission are high in this population, emphasizing the need for targeted health promotion and public health programming to improve the health of young mothers living with HIV. Zvandiri, a non-profit organization in Zimbabwe, created the Young Mentor Mother (YMM) program in response to this issue. This health promotion program uses peer-led service delivery conducted by trained young mothers living with HIV, called YMMs. We conducted semi-structured virtual interviews (N = 29) among Zvandiri staff and YMMs to identify benefits and challenges, and to inform future program scaling. We applied thematic analyses to the transcriptions. Participant narratives revealed several themes, including three key benefits from the YMM program: (1) peer support, (2) holistic care, and (3) women’s empowerment. Participants also shared barriers to the success of the program, reflecting two overarching dimensions: (1) barriers related to scaling up the YMM program and (2) challenges related to addressing socio-structural factors. Barriers to scale-up included limited funds and resources, and food insecurity. Socio-structural challenges included HIV-related stigma, cultural and geographic differences, and intimate partner violence (IPV). These challenges align with the social-ecological model, whereby structural factors (lack of funding, food insecurity), community factors (HIV-related stigma, socio-cultural differences in accepting HIV care), and interpersonal factors (IPV) affect the implementation and scale-up of the program. We recommend future adopters of the YMM program to tailor the model for their community, prioritize peer supporter’s well-being, foster women’s empowerment, and adopt a holistic care approach.
Keywords
Introduction
Two thirds of people living with HIV (25.6 million) live in Africa (UNAIDS, 2021; World Health Organization, 2022). One population disproportionately affected by HIV is adolescent girls and young women (15–24 years), largely due to reduced social power and protections (Karim & Baxter, 2019; UNAIDS, 2018, 2022). One woman aged 15–24 years is infected with HIV every 3 minutes, and this population is three times more likely to be infected than men of the same age in Africa (UNAIDS, 2022). In Zimbabwe, for example, recent estimates suggested that the prevalence of HIV was 7.5% and 14.8% among adolescent (15–19 years) and young (20–24 years) mothers, which is substantially higher than the national average estimates of 3.9% and 8.1% for individuals in these age groups (Burrage et al., 2020). This is a global and public health concern because many young women living with HIV must manage their own health and well-being in addition to that of their children, highlighting the need for increased public health promotion (Toska et al., 2020; Yakubu & Salisu, 2018).
Adolescent birth rates are high in HIV-endemic communities, and adolescent mothers are more likely to be of low socioeconomic status (Ng’eno et al., 2020; Toska et al., 2020; Yakubu & Salisu, 2018). Southern African–based research suggests that young mothers living with HIV have significantly lower rates of HIV treatment access and adherence compared with adults living with HIV (Ronen et al., 2017; Toska et al., 2020). In addition, young mothers with HIV have higher rates of perinatal, previously referred to as mother-to-child, HIV transmission than adult women with HIV, and lower perinatal transmission prevention services uptake (Burrage et al., 2020; Ng’eno et al., 2020; Tapera et al., 2019). Young women and girls living with HIV often also face financial and housing challenges, stigma, and abuse from family and communities, which can lead to HIV status concealment and reduced care retention (Kimera et al., 2019; Ng’eno et al., 2020; Tapera et al., 2019; Toska et al., 2020; Yakubu & Salisu, 2018).
In response, Zvandiri, a Zimbabwean non-profit organization, created the Young Mentor Mother (YMM) health promotion program in partnership with Zimbabwe’s Ministry of Health and Child Care (MoHCC) and UNICEF (Tapera et al., 2019; Zvandiri, 2021). The program uses peer-led service delivery conducted by trained young mother counselors living with HIV (18–24 years), called YMMs, recruited with assistance from the MoHCC (Tatenda, 2018; Zvandiri, 2020, 2021). With support from Zvandiri staff, YMMs optimize HIV testing, treatment, counseling, psychosocial support, and service access for other young mothers living with HIV, and their infants and partners, during pregnancy and breastfeeding through home, group, virtual, and clinic consults, which last for 1–2 years. In addition to regular adherence check-ins by YMMs, the program connects young mothers to services for mental health, HIV care, sexual and reproductive health (SRH), IPV, antenatal care, early infant diagnosis (EID), and economic strengthening via income/savings/loans training (Zvandiri, 2021).
Peer-led HIV care is a unique approach that incorporates shared experiences and trust (Mark et al., 2019). Peer support can be particularly useful for youth to reduce stigma and isolation, while improving their physical and mental health (East et al., 1987; Mark et al., 2019; Meng et al., 2023). Zvandiri’s peer-led HIV service delivery has proven to be effective, with improved testing, treatment, and viral suppression rates among youth living with HIV in Zimbabwe (Tapera et al., 2019). In 2020, 94.6% of young mothers living with HIV in the YMM program received valid viral load results, and 97.1% of those mothers achieved viral suppression (Zvandiri, 2021). This is substantially higher when compared to Zimbabwe’s national statistics of that same year, which indicate viral suppression among only 66.2% of women aged 15–24 years living with HIV (ZIMPHIA, 2020). In addition, the rate of perinatal transmission among women in the YMM program was only 2%, as 98% of infants were HIV-negative at breastfeeding completion (ZIMPHIA, 2020; Zvandiri, 2021).
Zvandiri operates in 11 African countries and is piloting an extension of the YMM program for young fathers. Zvandiri is planning the implementation of similar programs in Tanzania, Mozambique, and Eswatini. However, the YMM program has only been established in Zimbabwe thus far. As such, we aimed to (1) explore how the YMM program bridges health care service delivery for young mothers living with HIV and (2) examine key benefits and challenges of the program identified by Zvandiri’s staff and volunteers (e.g., YMMs) using the social-ecological framework. This information can inform the scaling and establishment of future health promotion programs to support the well-being of young mothers living with HIV in other regions.
Methods
This study was conducted in partnership with Zvandiri and University of Toronto’s Reach Alliance. Created in 2015 at the University of Toronto, the Reach Alliance is a student-driven, faculty-mentored, research and leadership initiative, whereby student researchers lead research to examine how critical interventions and innovations target hard-to-reach populations (Roll et al., 2024). Ethical approval was obtained from Research Ethics Boards at the University of Toronto (REB#: 00042111) and the Medical Research Council of Zimbabwe (REB#: MRCZ/B/2319).
Conceptual Framework
When exploring potential barriers and facilitators to scaling a peer-mentored program for young mothers living with HIV in Southern Africa, it is important to contextualize the interplay and overlap between societal, community, and individual-level variables, which can be modeled through the social-ecological model. We employed the social-ecological model to organize and explain findings identified through participant interviews into structural, community-level, and interpersonal dimensions (Baral et al., 2013; McLeroy et al., 1988). For example, quotations related to resources or access to care would be considered structural, while information on cultural or social interactions would be grouped at the community level, and findings related to social support would be at the interpersonal level (Baral et al., 2013; McLeroy et al., 1988). In addition, the social-ecological framework allows for the identification of overlap between dimensions and suggests that simultaneous action across all levels may promote population-level impacts (CDC, 2022). We can therefore use this framework to identify implications for future practice and research.
Participants
Participants were eligible if they were English-speaking Zvandiri volunteers (e.g., YMMs) or staff to ensure a variety of perspectives were included. As peer mentors, YMMs are young volunteers (aged 18–24 years) with lived experience of HIV during motherhood. Zvandiri’s staff, including health care providers, work closely with the YMM volunteers to optimize care and create tailored programs for young mothers living with HIV. Health care staff and YMMs are client-facing members of the program who work directly with patients. Other interviewed staff, including former YMMs and higher-level administrative staff, are directly involved in the creation of the YMM program, meaning they train YMMs and make organizational decisions in collaboration with government officials and sponsor agencies. Since the aim was to identify the benefits and challenges of the YMM program to help scale the model, we ensured that the perspectives of YMMs and staff were equally considered. Participants were identified through referrals from Zvandiri’s coordinating staff and were invited by the University of Toronto student researchers (under the mentorship of C.H.L.) to participate via email or WhatsApp messaging. The information on who participated/did not participate was not shared with Zvandiri, and researchers unaffiliated with Zvandiri led the recruitment and data collection to mitigate the risk of participants feeling pressured to participate.
Procedures
Students (L.S.T., J.A., S.H., and S.L.) trained in research methods and ethics conducted a series of semi-structured, confidential, virtual interviews with Zvandiri staff and YMMs via Zoom and WhatsApp. Interview questions were developed by these four researchers through literature reviews and verified by a third party from the University of Toronto and Zvandiri staff.
Signed consent forms were obtained prior to interviews in addition to verbal consent at interview commencement. Participants were explicitly informed of their right to skip questions or withdraw consent and contribution at any point. All records of communication, including audio files, were stored on a secure server. Eligible participants received unique identification numbers to link interview responses. All identifiable information was de-identified and removed from databases and transcriptions. The master list of identification numbers was destroyed prior to publication. Participants received reimbursement for mobile data purchases of US$5 and were informed that responses would inform the scalability of the program.
Measures
The interview guide (Table 1) included questions about participants’ experiences with Zvandiri and the YMM model. For example, participants were asked, “What does the YMM program give to participants that other HIV prevention/treatment programs do not provide?” To explore the possibility of scaling, participants were asked questions including, “What are the steps for bringing YMMs to a new community?” and “What challenges do you think the YMM program might encounter with expanding to other countries?” We adapted our guide to expand on topics that emerged repeatedly, such as gender-based violence. Finally, we investigated the perceptions of the role of Zimbabwe’s MoHCC in the YMM program.
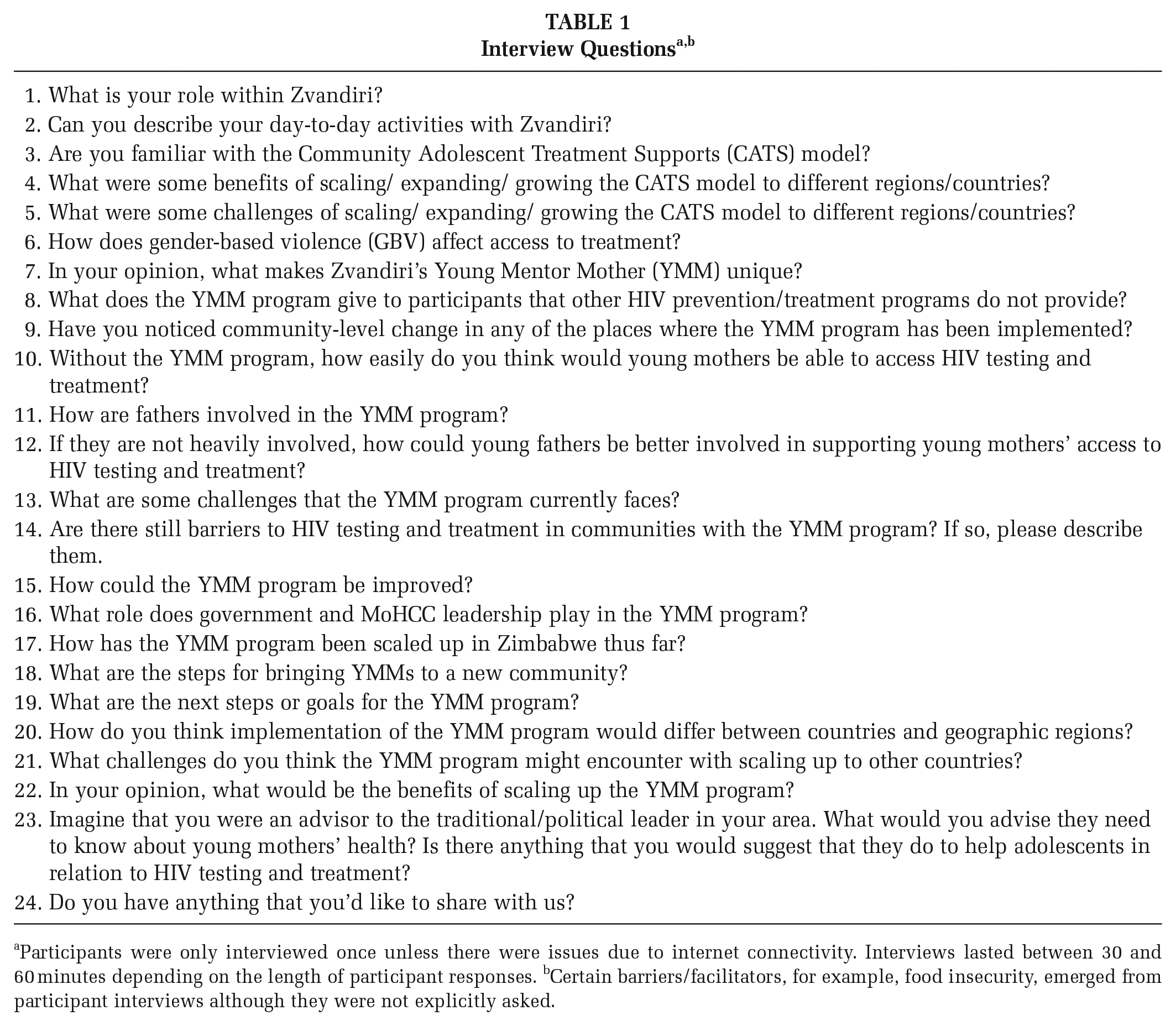
Participants were only interviewed once unless there were issues due to internet connectivity. Interviews lasted between 30 and 60 minutes depending on the length of participant responses. bCertain barriers/facilitators, for example, food insecurity, emerged from participant interviews although they were not explicitly asked.
Data Analysis
All interviews were recorded and transcribed verbatim, in English. All personal identifying information was removed from interview transcripts, which were then cleaned and uploaded into Dedoose 9.0.62 software for analysis (Dedoose Version 9.0.17, 2023). Demographic characteristics, such as education level and employment status, were summarized with descriptive statistics.
To analyze the data, we (L.S.T., J.A., S.H., and S.L.) employed Attride-Stirling’s thematic network approach and identified shared themes throughout participant interview transcriptions (Attride-Stirling, 2001). Two independent researchers reviewed each transcript line-by-line in Dedoose and created a coding framework based on reoccurring themes in the texts (Attride-Stirling, 2001). These themes were then abstracted, refined, and arranged into major and sub-themes (Attride-Stirling, 2001). Disagreements were resolved by a third independent reviewer when needed. We used a reflexive analysis to explore deductive and inductive themes shared across multiple transcripts (Braun & Clarke, 2006). Thematic analysis is theoretically flexible and includes both deductive and inductive analyses; we used deductive analyses to identify the unique benefits and challenges of the peer-led YMM program (e.g., a priori coding for general barriers, such as limited funding) and applied inductive analyses to elucidate emerging themes (e.g., the impact of intimate partner violence [IPV] on access to care), following Braun and Clarke’s data analysis process (Braun & Clarke, 2006; Clarke & Braun, 2013). We used the social-ecological model (Baral et al., 2013; McLeroy et al., 1988) as a conceptual framework for benefits/barriers to the program, independently compiled a list of key themes and situated these themes with existing literature. As previously mentioned, the social-ecological model was employed to describe and contextualize complexities between structural, community-level, and interpersonal factors posing as benefits or barriers to scaling the YMM model (Baral et al., 2013; McLeroy et al., 1988).
Results
Demographic Results
We conducted interviews with n = 29 Zvandiri staff and YMMs: 79.3% were Zvandiri staff, and 20.7% consisted of YMMs, health care providers, or counselors. We aimed to recruit n = 20 participants to learn from a diversity of perspectives while reaching saturation (Hennink & Kaiser, 2022), although required sample sizes are contested in qualitative research (Vasileiou et al., 2018) and increased this sample due to the high interest from staff and YMMs. We distributed n = 110 invitations to participate and received n = 29 responses; all interested respondents were invited to participate. To protect confidentiality, we did not collect information on respondents versus non-respondents.
The mean age of participants was 30.2 (7.07) years. Most interviewees identified as women (89.7%) with full-time employment (75.9%), as demonstrated in Table 2
Socio-Demographic Characteristics of Participants Sampled From Zvandiri (N = 29)
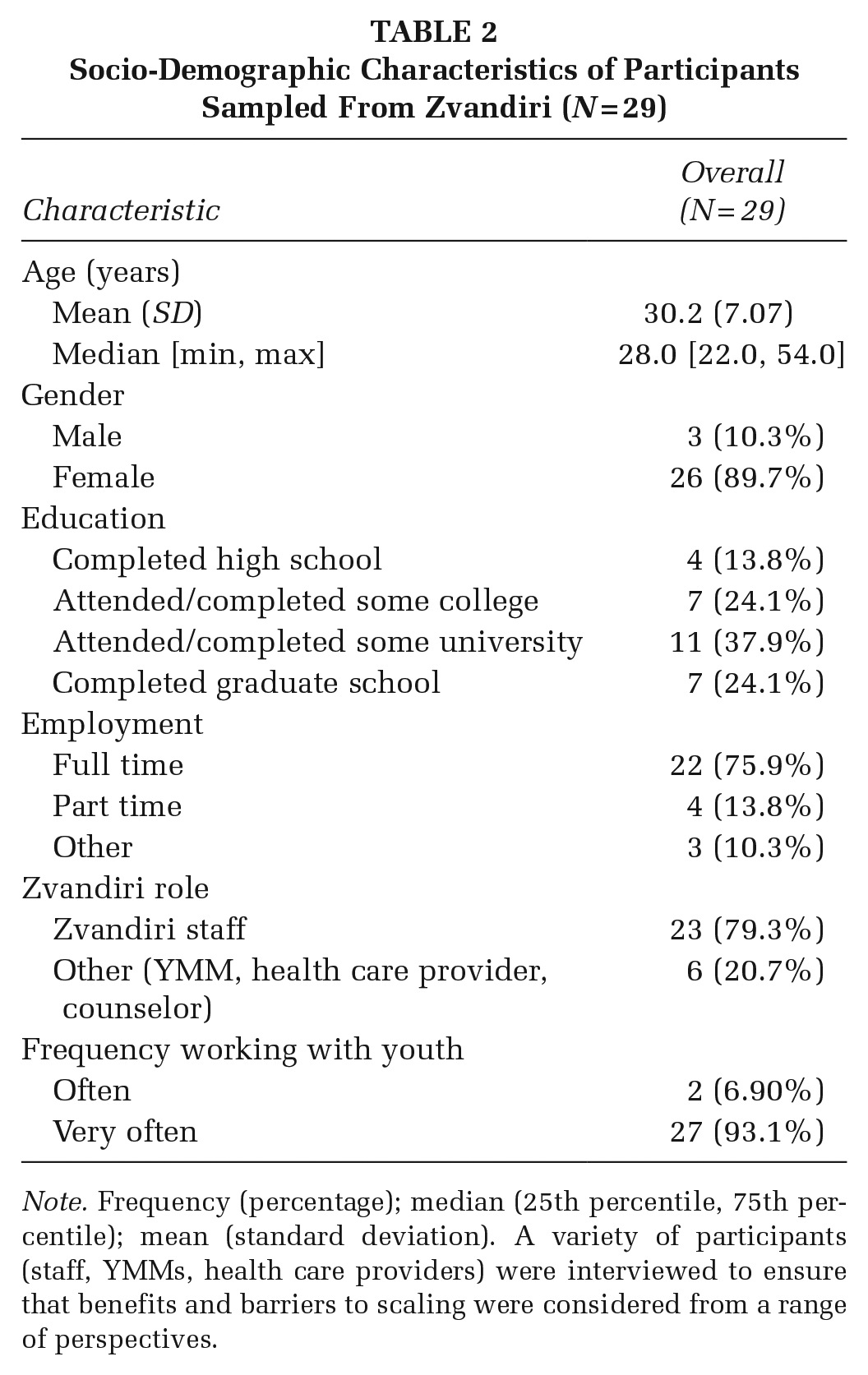
Note. Frequency (percentage); median (25th percentile, 75th percentile); mean (standard deviation). A variety of participants (staff, YMMs, health care providers) were interviewed to ensure that benefits and barriers to scaling were considered from a range of perspectives.
Thematic Analyses
Participant narratives revealed several benefits and challenges of the YMM program, with key quotations highlighted in Table 3.
Themes and Subthemes With Illustrative Quotes
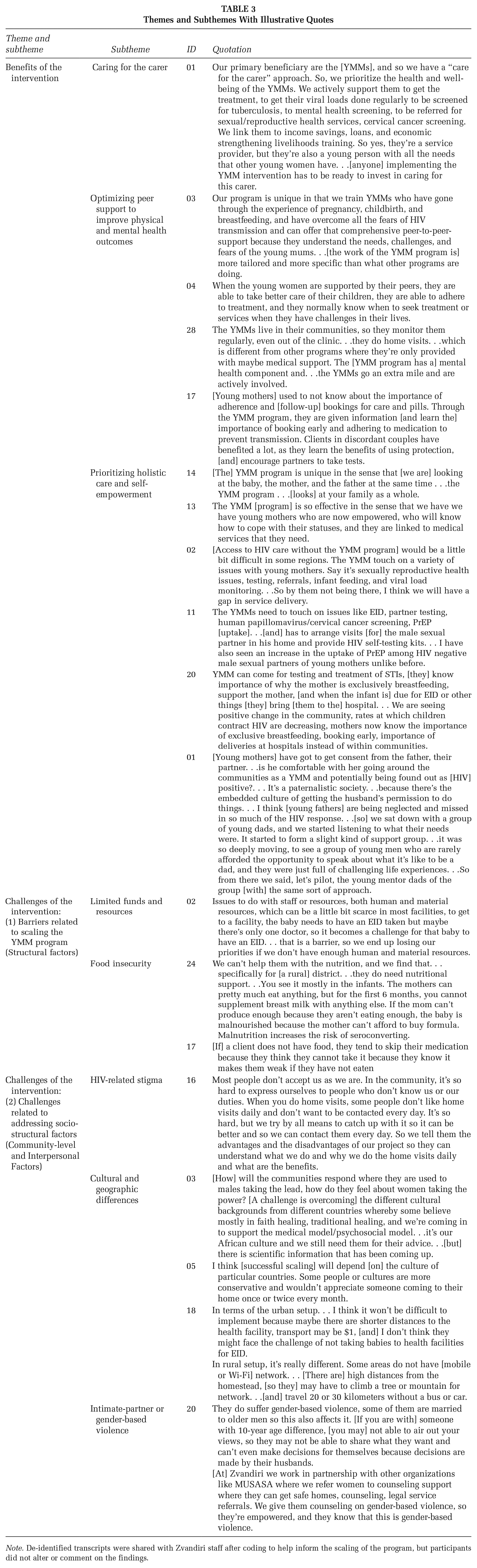
Note. De-identified transcripts were shared with Zvandiri staff after coding to help inform the scaling of the program, but participants did not alter or comment on the findings.
Benefits and Facilitators of the Intervention
Structural factors
(i) Caring for the Carer. The importance of considering the needs of the YMMs emerged in interviews since YMMs are also young mothers living with HIV with the same needs as their clients. Described as “caring for the carer” by Interviewee 01, this aspect of the YMM program focuses on supporting the YMMs outside of their volunteer work through counseling and support for their own health and well-being, and linkage to external health services (e.g., mental health., tuberculosis, cervical cancer, and sexually transmitted infections [STIs]). In addition, economic strengthening and livelihood training, alongside YMM role-specific training, were flagged as necessary to help YMMs thrive. This is being implemented in select districts but needs scaling up.
Community-level factors
(i) Optimizing Peer Support to Improve Physical and Mental Health Outcomes. The value of the peer-based YMM model was emphasized throughout most interviews. Participants attributed increased medication uptake and improved health service access to support and guidance from the YMMs. The YMMs share personal experiences with their clients, making it “easier for [YMMs] to identify the challenges that these mothers are facing, and then show them where to go, how to cope, how to live with HIV” (Interviewee 10). As such, receiving support from YMMs is “like having a friend to confide in” (Interviewee 04). According to Interviewee 28, the YMMs are “more approachable than the other staff” in health facilities due to their young age and relatable backgrounds.
YMMs provide personalized reminders and advice to encourage and promote the engagement of young mothers in their own health care. Participants expressed that these reminders help improve medication adherence, trust in health care providers, and self-confidence. As indicated in Table 3, we learned that the peer-based program bolstered physical and mental health through individualized care. Interviewees noted that peer-based trust allows YMMs to assess patient’s well-being and identify red flags (e.g., medication nonadherence, lack of support, malnourishment of the mother or infant). YMMs encourage clients to attend enhanced adherence sessions and receive blood tests to assess viral load counts, improve viral load suppression, and reduce the risk of viral transmission to children or partners.
(ii) Better Informed Community. Participants expressed that the YMM program had a positive community-level change since “people in the community are now equipped with information [on HIV]” (Interviewee 17).
Interpersonal factors
(i) Prioritizing Holistic Care and Self-Empowerment. Participant narratives highlighted that the program emphasizes holistic care for young mothers and their families, including future work targeting young fathers. Participants emphasized the importance of providing support for infants, partners, and family members of clients to minimize HIV transmission, improve treatment adherence, and reduce stigma from family.
Participants commented on unique programs offered by the YMMs, including sexual and reproductive health counseling and infant care resources tailored for young mothers with HIV. Participants noted that collaboration with Zimbabwe’s MoHCC allows for referral to appropriate services (e.g., contraceptives, STI management, and cervical cancer screening) to optimize care. They stressed the need for government collaboration when scaling the program to a new country. For instance, Interviewee 02 detailed, “The program doesn’t work in isolation—it works in collaboration with the ministry. . . So, there is a very close relationship between the YMM and the ministry. . .they work together.”
Support groups co-facilitated by YMMs and the ministry teach young mothers about the importance of medication adherence, family planning, STI prevention, responses to stigma and violence, and mental health coping strategies. Interviewees also noted that this holistic approach to care empowers young mothers living with HIV through health education.
Challenges of and Barriers to the Intervention
Identified from interview findings, barriers to success map onto the social-ecological model (Baral et al., 2013; McLeroy et al., 1988) and can be divided into two key dimensions: (1) barriers related to scaling the YMM program and (2) challenges related to addressing socio-structural factors (Figures 1 and 2).
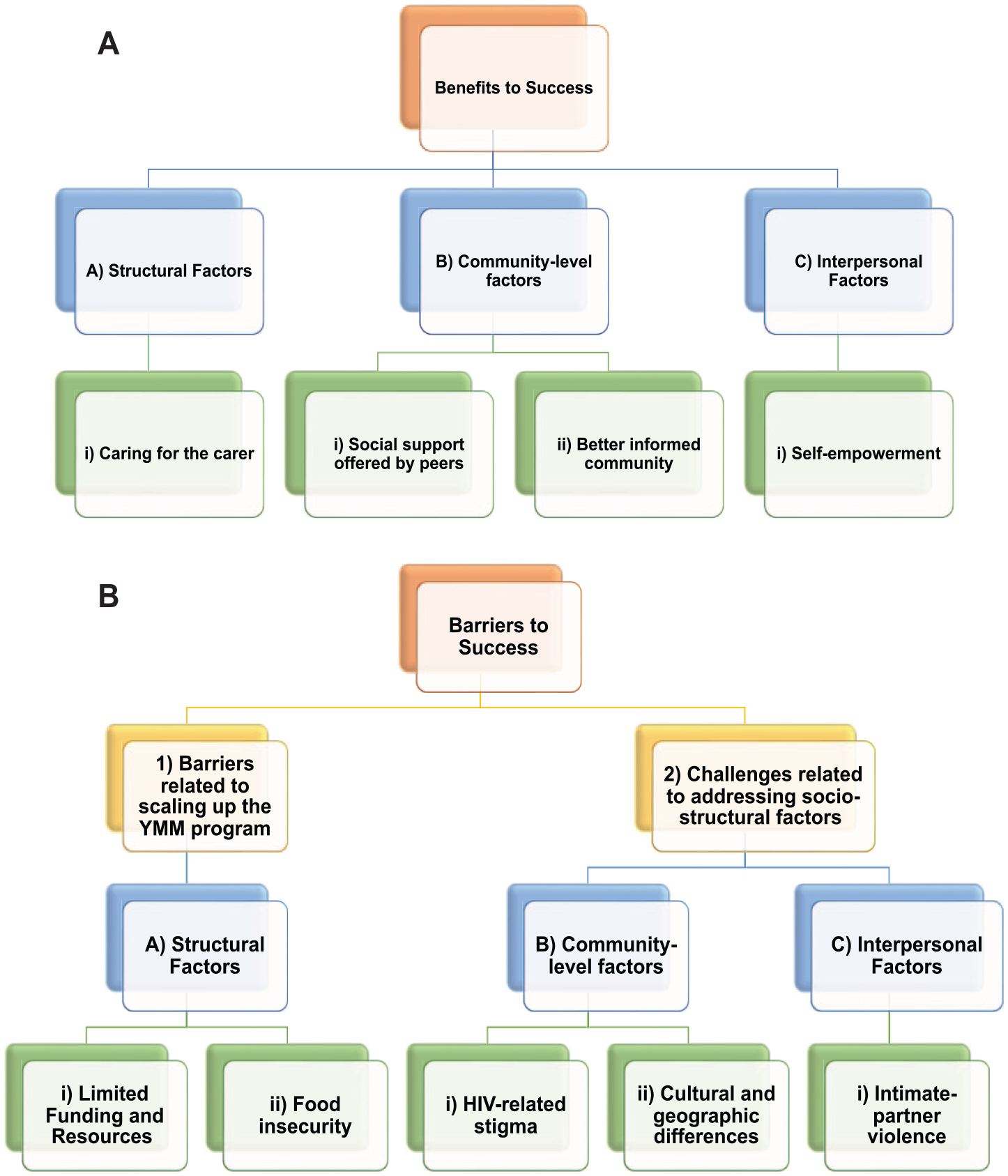
Benefits and Barriers to Success: Benefits and Barriers to Success can be Mapped Onto the Social-Ecological Model: (A) Benefits to Success and (B) Barriers to Success can be Divided Into Two Key Dimensions—(1) Barriers Related to Scaling Up the YMM Program and (2) Challenges Related to Addressing Socio-Structural Factors
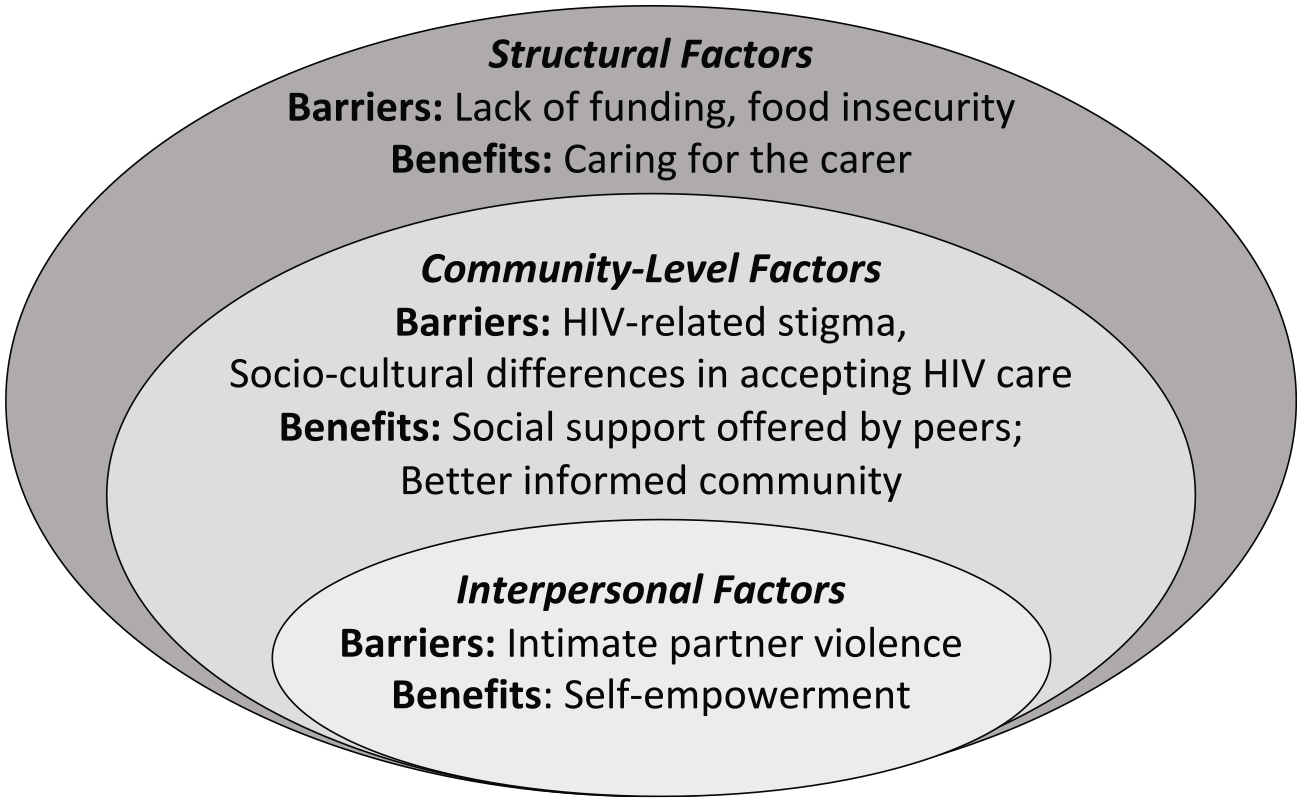
Barriers to and Benefits of the YMM Program Mapped to the Social-Ecological Model. Barriers: Structural Factors (Lack of Funding, Food Insecurity), Community-Level Factors (HIV-Related Stigma, Socio-Cultural Differences in Accepting HIV Care), and Interpersonal Factors (IPV). Benefits: Structural Factors (Caring for the Carer), Community-Level Factors (Social Support, Educating the Community), and Interpersonal Factors (Self-Empowerment)
Barriers related to scaling the YMM program
(A) Structural Factors. (i) Limited Access to Funds and Resources were identified as key barriers to the success, scale-up, and sustainability of the YMM program. Interviewees noted that lack of funding and staffing restricts the ability to incentivize and support new YMMs. YMM volunteers receive a monthly allowance to help support their work and living. However, some participants expressed that, insufficient resources (e.g., test supplies, vehicles) are barriers to service delivery that increase wait times. Participants suggested limiting the number of clients under a YMM’s care to avoid burnout and maintain program success.
(ii) Food Insecurity emerged as a client medication adherence barrier and a potential enhancer of perinatal transmission based on participant conversations. According to interviewees, many clients who lack adequate nutrition also have reduced medication adherence and insufficient breastfeeding. Interviewee 24 expressed that maternal food insecurity extends to risks in infants, including infant malnutrition and an increased chance of HIV seroconversion.
Participants noted that the YMM program provides occasional nutrition packages and makes referrals to “the Department of Social Development for nutritional support, supplements, or food security services” (Interviewee 02). Interviewee 03 expressed that additional funding would help to address food security concerns and improve the quality of care and medication adherence.
Challenges related to addressing socio-structural factors
(B) Community-Level Factors. (i) HIV-Related Stigma from partners, family, and community members was a recurrent concern throughout the interviews. Interviewees indicated that some young mothers fear that HIV status disclosure will result in social isolation from family members and IPV. The resulting non-disclosure can impede access to care and adherence to medications, as clients “end up defaulting, not taking their medicines because they don’t want it to be known that they are HIV positive” (Interviewee 28). Certain communities have lower enrollment than others due to fear of disclosure. This stigma means that “it takes time for them to want to join the program,” which might subsequently restrict the “target of reaching those who need to be tested” (Interviewee 07). Partner and community stigma reduce the safety of home visits, meaning YMMs must arrange meetings in confidential locations.
Finally, if a partner does not know the young mother is living with HIV, “it’s very difficult for that partner to. . .have [the] HIV test and. . .to take pre-exposure prophylaxis” (Interviewee 07). Non-disclosure limits the provision of HIV testing, prophylaxis, and treatment for partners. However, the YMM program has made efforts to improve partner disclosure, testing, and engagement, (e.g., 99% of partners who tested positive for HIV have initiated treatment) (ZIMPHIA, 2020; Zvandiri, 2021).
(ii) Cultural and Geographic Differences were also commonly mentioned as a barrier to scaling, including service gaps between rural and urban areas. Several participants believed that religious/traditional values could impede successful implementation and scaling. Many argued that future YMM programs must be designed based on the cultural needs (e.g., languages, societal norms) of the respective region and noted that scaling a women-led program would be challenging in patriarchal-based societies. Interviewees noted decreased access in rural versus urban areas due to farther distances and fewer transportation methods, claimed that YMMs have risk factors for complications during travel (e.g., carrying children on bicycles across treacherous terrains) and indicated that urban YMMs have better phone network access, resulting in improved follow-up and information collection.
Interpersonal factors
(i) Intimate Partner Violence was identified as a challenge to successfully supporting young mothers living with HIV because these women would be less likely to attend YMM visits or adhere to therapy. Therefore, the YMM program screens for IPV or other gender-based violence experiences and refers these young mothers to receive care from a non-governmental organization against violence. Young mothers whose partners are unaware of their HIV status “fear their spouse’s reactions”—and the potential of resultant physical or emotional abuse in the form of “beatings” (Interviewees 03, 07, and 23).
Many young mothers are “financially dependent on their partners” and must continue to be in intimate relationships out of financial hardship (Interviewees 28 and 22). As such, participants noted that gender-based violence hinders medication adherence, access, and service delivery (e.g., clinic/home visits) (Interviewee 17). The YMM program seeks to counter the consequences of gender-based violence, including IPV, through confidential visits and phone messaging check-ins with young mothers.
Discussion
This qualitative study with 29 Zvandiri staff and YMMs revealed key benefits and challenges of a youth peer support HIV care program in Zimbabwe, which can help to inform the scaling up of similar programs in new countries. The YMM intervention seeks to improve HIV care at each social-ecological level, and this study demonstrates how the model can be used in future research and program development. For instance, the identified challenges map onto the social-ecological model (Baral et al., 2013; McLeroy et al., 1988), whereby structural-level factors (lack of funding, food insecurity), community-level factors (HIV-related stigma, socio-cultural differences in accepting HIV care), and interpersonal-level factors (IPV) affect implementation and scale-up considerations and can therefore be considered in future research and health promotion program development. Benefits also span multiple levels, including structural-level considerations of how to “care for the carer” that could change institutionalized practices when hiring peer supporters, community-level factors including social support offered by peers, and intrapersonal-level factors associated with self-empowerment.
One key benefit of the YMM program is its use of peer support that fosters improved adherence, follow-up retention, mental health, and well-being. This corroborates findings from previous studies, such as a randomized control trial of Zvandiri’s peer-based system, which found that the peer-based support intervention significantly decreased the proportion of patients with a detectable viral load 36-weeks post-intervention (Ndhlovu et al., 2021). Our findings are also consistent with a review of psychosocial interventions among youth living with HIV, which found that important aspects of strong HIV service delivery include patient empowerment, tailored approaches, self-care skills, digital delivery, and peer support (Laurenzi et al., 2022). We build on this literature by highlighting the importance of “caring for the carer” in a peer support model for young mothers living with HIV. Participant narratives highlighted the importance of prioritizing the physical and mental health of YMMs through regular screenings so that carers can better support clients.
Our findings suggest that government leadership, support, and collaboration are vital for success, and economic advancement training for YMMs. This builds on previous research, which highlighted the importance of routine data collection by HIV facilities and African health ministries to inform policy revisions and programming (Mark et al., 2019). Participant responses in our study indicate that government and peer support programs should collaborate to create targeted programs and policies.
Findings also revealed key barriers to program success, including IPV, food insecurity, and stigma. This substantiates research from the EMPOWER study, which evaluated empowerment techniques and HIV prevention in peer-based clubs of adolescent girls and young women in South Africa and Tanzania (Baron et al., 2020). The EMPOWER study found that gender-based violence (including IPV) and stigma were key barriers to HIV prevention medication adherence among this population (Baron et al., 2020). Previous literature has identified that women in Sub-Saharan Africa who experience IPV are less likely to achieve viral load suppression than those who do not (Kuchukhidze et al., 2023). Participant narratives of our study confirm that IPV is a barrier for adolescent girls and young women receiving HIV treatment, especially those who are also young mothers. A study among adults living with HIV in Uganda found that food insecurity was a widespread barrier to HIV medication access and adherence, whereby participants found that medications increased their hunger and would therefore skip or forget doses (Weiser et al., 2010). Similarly, our interviews elucidate food insecurity as a potential obstacle, although more research on the impact of food insecurity among young mothers living with HIV is needed. Our study adds to this literature to generate insight into strategies to address these challenges which are being integrated into future implementation of the YMM model as it scales up.
Challenges of limited funding and resources are also obstacles to the expansion of other youth HIV interventions in Africa, such as Operation Triple Zero (World Health Organization, 2019). A scoping review of barriers and facilitators of implementing and scaling models for HIV treatment in Africa found that the main barriers were limited funds or resources, stigma, and low literacy (Belay et al., 2022). The interviews we conducted indicate that cultural and geographic differences may also be key factors to consider. These findings are corroborated by previous research. For example, previous research among individuals living with HIV in Southern Africa has identified religious beliefs and traditional medicines as cultural barriers to care (Azia et al., 2016; Peltzer et al., 2011; Wanyama et al., 2007). Azia et al. found that some individuals believed that the use of prayers, holy water, or non-Western medicine (traditional medicine) could cure or cleanse their HIV, which limited their use of antiretroviral treatments (Azia et al., 2016). In addition, a systematic review conducted by Lankowski et al. found that issues such as geographic and transportation-related barriers (e.g., transportation costs, far distances) negatively affected HIV outcomes (i.e., counseling, testing, linkage to care, adherence, viral suppression) among individuals living with HIV in Southern Africa (Lankowski et al., 2014).
Due to time constraints and COVID-19 restrictions, we were unable to interview non-English speakers, which may bias responses. To mitigate this potential selection bias, we interviewed a range of staff and YMMs to improve response diversity. A second limitation was that interviews were conducted virtually and were limited by poor network connection and time zone restrictions. To address this, we used WhatsApp calling when needed to circumvent Zoom connection issues and rescheduled missed appointments when possible. Language and connectivity barriers reduced YMM participation. However, although our sample was mainly staff including former YMMs and senior staff, the staff who were interviewed provided necessary insights regarding future scalability (e.g., funding, government cooperation). Our sample is of higher educational and employment status, which is reflective of Zvandiri staff and YMMs, who must be literate and have attended school. Finally, our interview responses only included perspectives from persons working at Zvandiri and not external stakeholders. Future research should consider the perspectives of stakeholders and clients. Despite these limitations, this study is unique in contributing to knowledge on the experiences of staff and YMMs who provide peer-based HIV care to young mothers living with HIV in Zimbabwe.
Implications for Practice
The success of the Zvandiri YMM program in Zimbabwe substantiates the value of a peer support model focused on holistic care for adolescents, including young mothers, living with HIV. However, it is imperative that future adopters of the model, including government, health care, and public health or policy professionals, consider the identified facilitators and benefits, and barriers and challenges, when scaling the program to new countries. As per the social-ecological framework, the YMM program benefits and challenges identified through this study can be used to inform the design and scale-up of future models whereby public health professionals should consider the interplay between these factors and can simultaneously act across multiple social-ecological levels (structural, community, interpersonal) to successfully implement the model in other countries.
Public Health Practitioners Working with Young Mothers Living with HIV Should Consider the Adoption of Peer-Based Models as an Effective Intervention to Improve HIV Care Delivery.
As suggested by our findings, the peer-mentor approach has been well received among youth living with HIV, as it allows adolescents to be guided and cared for by individuals of similar circumstances with shared experiences. This approach can reduce barriers, such as tentativeness to receive care (e.g., due to fear of authority figures), and increase patient understanding of the importance of care. Future adopters of this model should therefore work with community leaders to identify and train youth living with HIV to be mentors for their peers. The training program should be comprehensive and holistic, allowing the incorporation of local cultural and traditional practices where necessary. In addition, adopters should ensure they employ a “caring for the carer” approach, whereby the peer mentors themselves are supported through linkage to health services, such as sexual health and mental health care. Peer mentors should also receive adequate livelihood training to prepare them for success after leaving the program. Strengthening the peer network is vital to creating a long-lasting program where former clients can become peer mentors who can recruit other clients and volunteers before leaving the program or transitioning to a paid staff position.
Public Health Practitioners Working With Young Mothers Living With HIV Should Employ a Holistic Approach to Care
Our work suggests that future adopters of the model should ensure the incorporation of financial, educational, and health support for peer supporters, in addition to a comprehensive program prioritizing mental health and self-empowerment for YMMs and clients. For example, due to their holistic model, 95% of youth enrolled in Zvandiri programs were screened for mental health conditions and enhanced counseling from peer supporters reduced the prevalence of common mental disorders from 68.4% to 2.4% (Zvandiri, 2023). As such, mental health counselors should also be incorporated into the staff of future models and should be accessible to help clients and mentors. Clients and peer mentors should also receive sexual health education and support, family HIV care and counseling with their partners, and health resources and screening tests (e.g., EID) for their infants. Public health professionals interested in adopting the program to a new region should work with community champions to create a model that is tailored to their specific community needs and appropriately incorporate local language and cultural traditions or practices into care delivery. For example, if a local community has certain prayers or traditional rituals that are important to their well-being, practitioners should ensure that these practices are integrated with the program. By working with community leaders, public health professionals can seek to reduce HIV-related stigma within the community via de-stigmatization outreach initiatives in the community. Collaboration with leaders from within the community may be vital to ensuring the program reaches those hardest to reach and is a safe space for clients and their families. Public health professionals must therefore approach conversations with local leaders from a place of respect, recognizing the needs of the community and finding shared perspectives through which to build trust.
Public Health Practitioners Seeking to Scale the YMM Program Should Collaborate With Government Officials and Medical Clinics
To scale this model, improved organizational funding is needed. Currently, the Zvandiri YMM and Community Adolescent Treatment Supporters models are funded by the Government of Zimbabwe, highlighting the feasibility of this approach. Funding should empower YMMs, address food insecurity, increase service provision and accessibility through improved transportation, and improve the financial independence of the YMMs. For instance, a salaried income and funding that allows for snacks/meals to be provided for YMMs and clients could help reduce the burden of food insecurity. YMMs should be provided with safe and effective transportation, including bicycles or transport shuttles. Increased funding can also help support mobile phone access, particularly necessary to contact clients in rural or remote areas. Collaboration with local medical clinics can bridge care delivery for adolescents, including young mothers, living with HIV who may be less likely to access local health care on their own (e.g., due to stigma concerns, lack of support, lack of transport). Working with local government and medical agencies may allow for improved access to HIV test kits, medical supplies, and health care staff. In addition, public health professionals should collaborate with local agencies working to reduce gender-based violence and IPV, so that they may connect clients to timely and safely support without delaying HIV and other health care delivery to young mothers and their infants.
Implications for Research
Through our interview findings, we identified areas for future quantitative and qualitative research on the program. First, qualitative research aimed at ascertaining the perspectives of government officials and funding stakeholders on the benefits and challenges of program scaling would help future adopters of the model understand additional considerations needed for collaboration with government agencies and what funders may prioritize. Quantitative research to gain a sense of the prevalence of HIV among adolescents and young parents in other countries within Southern Africa can help pinpoint which countries and populations to prioritize in the creation of future models. In addition, qualitative studies focused on identifying the specific needs (e.g., cultural tradition) of new regions would also help in scaling this model to different countries and populations. Finally, qualitative work focused on the perspectives of young fathers living with HIV would help in the creation of a young father-focused program, currently in progress through Zvandiri, and may elucidate avenues for engaging fathers in gender-based violence prevention.
Conclusion
Zvandiri’s YMM health promotion program fills a unique gap in individualized HIV care and has several benefits, including peer support, holistic care, and women’s empowerment. Public health practitioners working with adolescents living with HIV should consider the adoption of peer-based models as an effective approach to engage youth in their health care. Based on participant interviews, we advise future adopters of this model to consider social-ecological challenges (e.g., IPV, food/financial insecurity, stigma) and cultural/geographic differences in program establishment, and ensure programs are tailored to the population. Further research focused on the perspectives of stakeholders, clients, and young fathers would improve the ability to effectively scale this program to new regions and countries.
Footnotes
Authors’ Note:
We thank all staff and volunteers who participated in this research. We also thank Moni Kim, Ashima Kaura, and Kimberly Skead for all of their guidance and mentorship throughout the research process, This work was supported by the University of Toronto’s Munk School of Global Affairs & Public Policy Reach Alliance Mastercard Impact Fund,
{kind=link}