
Abstract
Background
Effective dissemination of information about evidence-based programs (EBPs) is essential for promoting health equity. Faith-based and other community organizations have difficulty locating EBPs for implementation in their settings. A research team engaged in a systematic search to identify a menu of EBPs that could be offered to African American FBOs as part of a community-engaged implementation study. Methods. A four-stage process was developed to search for EBPs meeting seven inclusion criteria for dissemination in faith-based organizations (FBOs). Criteria included relevance to identified health disparity topics, endorsement on a federal website, free access to downloadable program materials, facilitator guidance, no requirements for health care providers, and culturally relevant materials for African American communities.
Results
Nineteen government websites were searched. Sixty-six potential EBPs were identified. Six EBPs met all inclusion criteria.
Discussion
The search for EBPs that met seven criteria for implementation in African American FBOs demonstrated challenges that have been described in the literature. Researchers encountered a lack of standardized terminology for identifying EBPs on federal websites, frequent requirement for health care providers or clinics and/or fees for training and materials. FBOs are supportive and safe places to offer EBPs to promote health, and EBPs need to be designed and disseminated to meet the needs and preferences of FBOs. Including members of FBOs and others in the community in EBP development, design, and dissemination, such as searchable health promotion EBP registries, can increase the likelihood that effective programs intended to address health disparities are readily accessible to FBOs for implementation.
Keywords
Dissemination and implementation of evidence-based programs (EBPs) to promote health behaviors and prevent chronic diseases are fundamental elements of efforts to promote health equity (Brownson et al., 2018) and address the social determinants of health (Alcaraz et al., 2020). Health promoting EBPs include a broad variety of interventions that may combine educational, experiential, and environmental elements to be offered at the individual, group, or community level (Videto & Dennis, 2021) The evidence-based process, used to design and implement EBPs, incorporates the use of evidence to support health behavior changes in EBP development, recognizes the importance of including community expertise (capacity), as well as the values and needs of the targeted population (Magura et al., 2022; Melnyk & Fineout-Overholt, 2019).
Online registers have been created as part of efforts to disseminate information about hundreds of EBPs that were developed and evaluated with federal funding and recently several publications have addressed problems in the structure and function of these registers. Among the problems noted in compilations of EBPs are the various definitions of “evidence-based,” the lack of standard criteria for evaluating evidence of effectiveness, the age of many of the EBPs, and difficulty locating EBPs for specific contexts and users (Harden et al., 2021; Percy-Laurry et al., 2021; Singh et al 2023; Zack et al., 2019). While registers of EBPs maintained by federal agencies have varied standards for effectiveness (Zack et al., 2019), they are nonetheless reasonable sources of information about programs that can be disseminated to community organizations whose goals include preventing chronic diseases and addressing health disparities (Percy-Laurry et al., 2021). The registers, mainly developed for use by public health professionals, have been limited in their reach for dissemination to community organizations that could implement these programs (Harden et al., 2021).
Religious institutions have direct and indirect positive impacts on health (Idler, 2014). African American faith-based organizations (FBOs) have a history of engaging in health promotion and are known to highlight the importance of health in their missions (Holt et al., 2009; Parrill & Kennedy, 2011). There is a long-standing connection between healing and faith with early hospitals administered by churches and clergy serving as the first health care providers (Chatters, 2000). Church-based programs have successfully addressed a range of topics including nutrition (Baruth & Wilcox, 2013; Campbell et al., 2000; Resnicow et al., 2001), physical activity (Thomson et al., 2015), cancer preventive behaviors (Campbell et al., 2000; Erwin et al., 1999), disaster relief (Rivera et al., 2019), as well as HIV prevention (Stewart et al., 2017). In general, the FBO is a highly credible community hub for reaching African Americans. According to the Pew Forum on Religion, nearly all African Americans (97%) believe in God and nearly 50% attend church once a week (Pew Research Center: Religion and Public Life, 2009). For many of those individuals, the church symbolizes stability, trust, and wisdom. Moreover, many reach economically diverse populations and respond quickly to congregational needs (McNeill et al., 2018).
Mazzucca et al. (2021) described opportunities for significant impact in disease prevention and health equity with EBPs implemented in FBOs, as well as identifying implementation and sustainment challenges in these settings. Among the challenges are a need for more knowledge about dimensions of the diverse FBO contexts within which implementation strategies and EBPs will need to be adapted as well as the capacity of FBOs to implement and sustain EBPs.
The gap between development of EBPs that can be delivered in community settings to promote population health and their effective implementation is the subject of a plethora of publications over the past several decades (Balas & Boren, 2000; Burkhardt et al., 2015). Proposals to address barriers to uptake of effective programs to reduce health risks include improved marketing platforms and plans (Harden et al., 2021; Miller et al., 2012; Percy-Laurry et al., 2021), direct communication between EBP developers and those in the field who are delivering programs (Wandersman et al., 2008), a focus on dissemination from the outset of EBP development (Williams et al., 2022), and identification of effective strategies for building skills of community-based health care providers (Brownson et al., 2021).
These suggested approaches focus on users who work in academic settings or public health systems, and who have resources, skills, and access to technology for searching scholarly literature and research-based databases. This study was developed to identify programs that reflected community users’ perspectives from the outset. Community input is needed (Kwan et al., 2022; Racine et al., 2022) for identifying the priority health areas, the EBP search methods and sources that would be most helpful, desired formats and delivery methods, processes of assessing health progress for individuals and communities, and approaches community members and organizations can use for accessing updated EBPs with tailored interventions specific for their specific population.
The Engaging Partners in Caring Communities (EPICC) Project was designed to identify EBPs that reduce risk for chronic health conditions that disproportionately burden African Americans, and to partner with FBOs that serve predominantly Black communities to deliver these programs in congregational settings. The EPICC Project was designed as a community-engaged research (CEnR) project to collaborate with FBOs in expanding their capacity to deliver EBPs to promote health equity, and to learn with them about ways academic communities can better develop, disseminate, and implement effective health promotion programs.
The Interactive Systems Framework (ISF) (Wandersman et al., 2008) was identified as a helpful tool for conceptualizing the process of identifying, implementing, and sustaining EBP’s in congregational settings. The ISF identifies three groups of individuals and teams whose efforts are oriented to disseminating and implementing programs designed to prevent chronic illnesses. First are those in the Prevention Synthesis and Translation Systems, including developers of EBPs and the organizations and agencies who establish platforms for disseminating information about them. Second are Prevention Support Systems whose teams focus on building capacity in contexts in which the EBPs are deployed. Wandersman et al. (2008) note that innovation-specific capacity refers to the skills and knowledge associated with successful implementation of specific EBPs, and general capacity refers to enhancements of the organization’s functioning that may help sustain multiple efforts to achieve the organization’s mission. Third is the Prevention Delivery System. In the EPICC Project, members of congregations serve in this system as they deliver an EBP to their fellow congregants.
A critical element of the ISF, for the purposes of the EPICC Project, is the intention for bi-directional information exchanges across the three systems. EPICC Project research staff, functioning in the Prevention Support System, planned to provide information to participating congregations about several EBPs that met criteria described below, to offer an implementation capacity assessment survey, and to provide a summary of the results along with implementation tools and training (Scott et al., 2020) related to the specific EBP selected by the congregation. The EPICC Project research staff also plan to develop recommendations for the Prevention Synthesis and Translation System reflecting their experience in offering technical assistance and the feedback from their community partners in the Prevention Delivery System.
As part of EPICC, a National Institutes of Health (NIH) funded project to enhance the capacity of congregations to offer health promotion EBPs in predominantly African American (AA) communities, our team undertook a search for programs that address health conditions that affect AA communities disproportionately. We identified cancer (DeSantis et al., 2019; Singh et al., 2023), cardiovascular disease (Benjamin et al., 2019), diabetes (Fryar et al., 2017; Haire-Joshu & Hill-Briggs, 2019), hypertension (Fryar et al., 2017; Marabota & Ferdinand, 2020), and obesity (Cuevas et al., 2020) as conditions associated with health disparities in African American communities.
We developed seven criteria for programs addressing these conditions that would be applicable for delivery in congregations that serve AA communities through a review of the literature (Griffith et al., 2010; Mazzucca et al., 2021; Tucker et al., 2021). Program criteria were that each: (a) addresses prevention of one or more of the conditions associated with health disparities; (b) is evidence-based in that it is endorsed by a federal agency such as the Centers for Disease Control and Prevention (CDC) or a branch of the NIH; (c) is free and available via downloading from an internet site; (d) provides a manual or video guidance for the facilitator or facilitating team; (e) does not require a facilitator who has specific health certification or licensure, or is a trained community health worker; (f) required that the material be user-friendly in its formatting including text with white space, interspersed graphic and images, and an engaging writing style; and (g) included illustrations and images that reflect participant diversity.
Critical to using the ISF framework to deliver EBPs in African American congregation, EBP’s that are suitable for use in these settings need to be identified. This paper describes the EPICC team’s search for EBP’s that meet the seven criteria, the results of our search, and our recommendations for those who develop and disseminate programs designed to reduce health disparities for delivery in community-based organizations.
Methods
We developed a four-stage process to identify EBPs that met our criteria for use by faith communities to address health disparities identified for the EPICC project. The first stage began with the NCI’s Evidence-Based Cancer Control Programs (EBCCP) site since they house a specific EBP repository. Because NIH and other federally funded research on health promotion is disseminated on government websites, we searched for similar repositories on other National Institutes of Health (NIH) websites, as well as federal agencies that receive funding for promoting health. The National Institutes of Health website identifies evidence-based practices, programs, and resources under the category of “Dissemination & Implementation Research” while also recognizing that the federal agencies and organizations listed on the NIH website use “their own process to identify what is evidence-based” (National Institutes of Health (NIH), Office of Disease Prevention, 2024, para. 1). The U.S Department of Agriculture site was included due to the connection with the Supplemental Nutrition Assistance Program (SNAP) and various food-related programs. EBP incorporation is also cited as a frequent requirement for federal funding (Lee-Easton, Magura, & Maranda, 2022), another reason searching NIH and affiliate websites for applicable programs.
In the second stage, we searched these 19 federal sites using the term “evidence-based program(s)” initially in the website’s search box. Search results were selected and searched for EBPs that frequently had links that were also then selected and searched. Notes were kept for each website with the numbers of initial search results and subsequent link trail searching for EBPs. Several websites returned no results for EBPs. Other possible terms were not included in this process due to length of time involved in initial searches, subsequent link exploration, and variability in sites. Search results were documented, and potential EBP resource links were highlighted.
In the third stage, these potential resources were screened by five members of the EPICC team to identify health promotion programs that addressed our targeted health conditions, and required a closer look to determine if they met our other specific criteria. We entered these programs into a REDCap database (Harris et al., 2019) and coded as yes or no if they met inclusion criteria regarding health area focus, availability of materials from the internet, and relevance for faith communities. This process resulted in sixty-six programs that addressed the targeted health issues.
In the final stage, the seven essential EBP criteria for EPICC were coded as yes or no in REDCap (Harris et al., 2019) to identify the programs appropriate for delivery by individuals in faith communities. Inclusion criteria included (a) addresses prevention of one or more of the conditions associated with health disparities (cancer screening/prevention, diabetes, heart disease/hypertension, nutrition, overweight/obesity, physical activity); (b) is evidence-based in that it is endorsed by a federal agency such as the Centers for Disease Control and Prevention (CDC) or a branch of the NIH; (c) is free and available via downloading from an internet site; (d) provides a manual or video guidance for the facilitator or facilitating team; (e) does not require a facilitator who has specific health certification or licensure, or is a trained community health worker; (f) required that the material be user-friendly in its formatting including text with white space, interspersed graphic and images, and an engaging writing style; and (g) included illustrations and images that reflect participant diversity. The “Culturally Appropriate Checklist Tool” was used to assess cultural relevance of materials (Chinman et al., 2021). EBPs meeting the inclusion criteria were coded to collect information about targeted age ranges and groups for whom programs were designed, types of materials available, reading levels of the materials, timing and number of sessions, and evaluation methods included in the program. Figure 1 highlights this process.
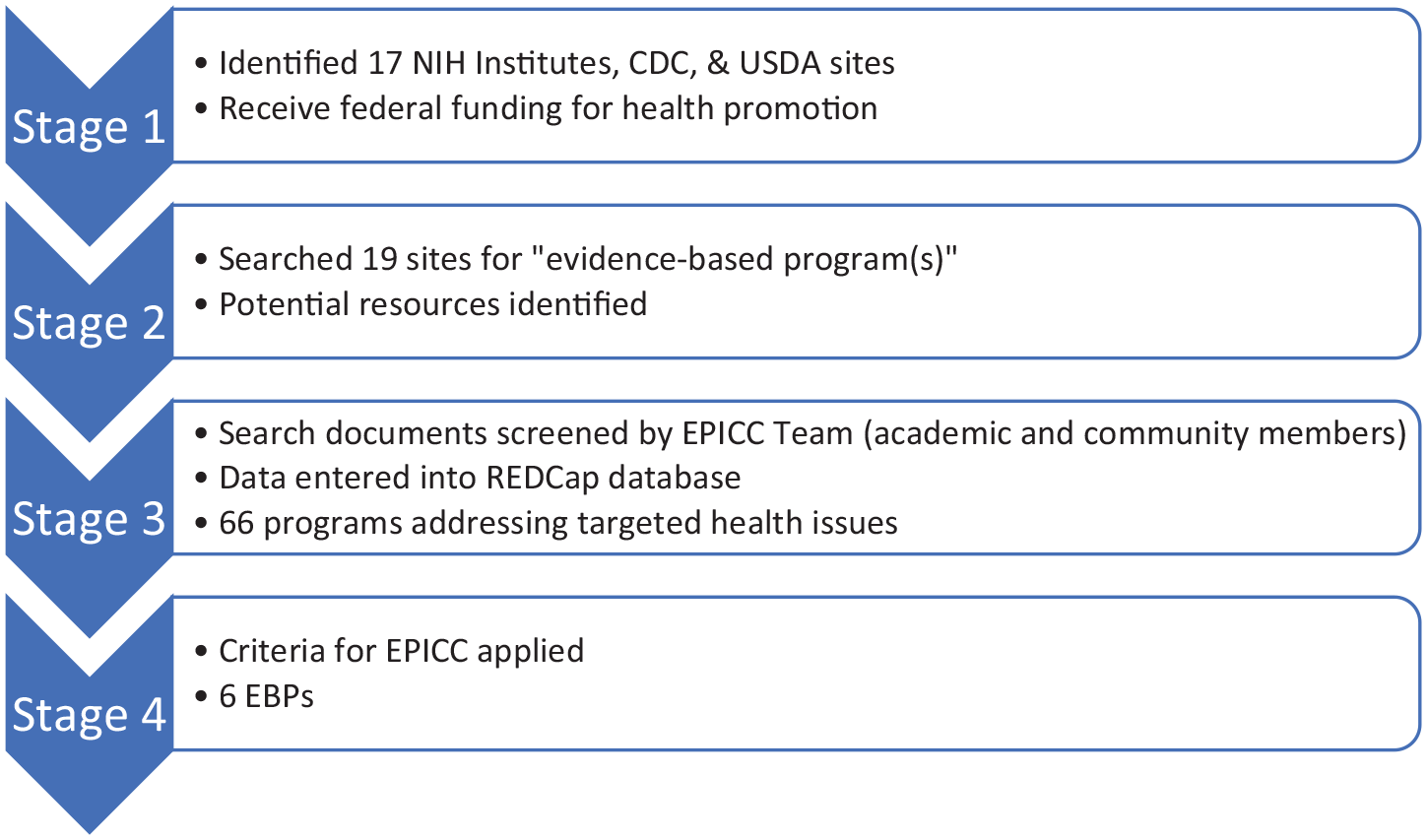
Four Stages of EBP Search
Results
Nineteen websites were searched for evidence-based programs; 66 potential programs were identified initially. Six programs, from the 66 possibilities, met the EPICC criteria.
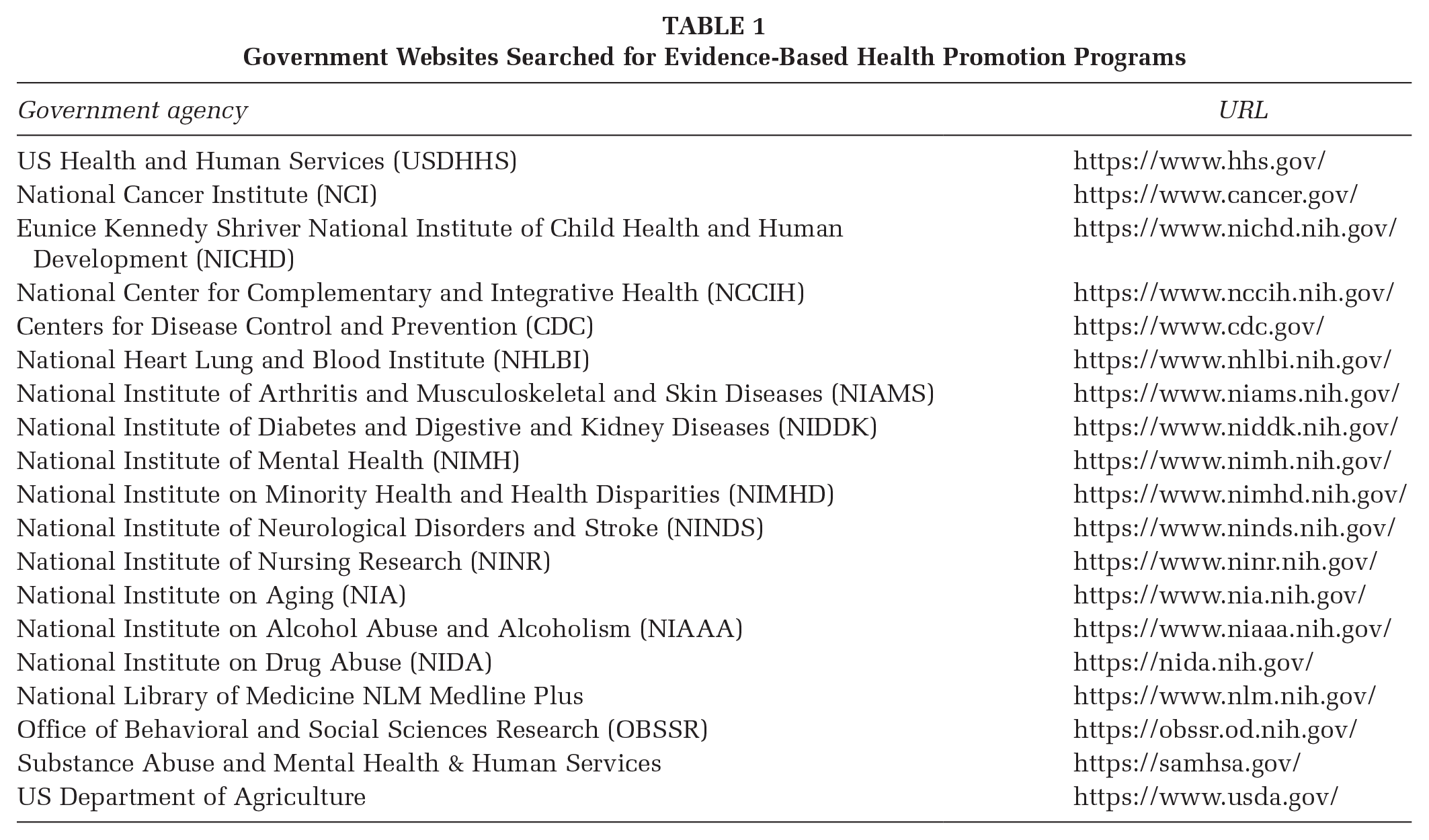
Table 1 shows the 19 government websites searched for EBPs that met the initial screening criteria. Each site was different in format and type of information available. The results of this stage of the search yielded substantial variability in quantity and organization of materials related to EBPs. Information included different or vague definitions of evidence-based, recommended guidelines for practice, notes from meetings and conferences, descriptions of research studies, and peer-review papers. There were no uniform formats for searching for evidence-based programs.
Government Websites Searched for Evidence-Based Health Promotion Programs
When information on a website appeared to meet the criteria for describing an evidence-based health promotion program, it was entered into the REDCap database (Harris et al., 2019) and then coded to determine if it met the specific criteria for a program that is suitable for use in a community setting. We visited each program’s website and used the resources available on that website to evaluate each program’s relevance for EPICC.
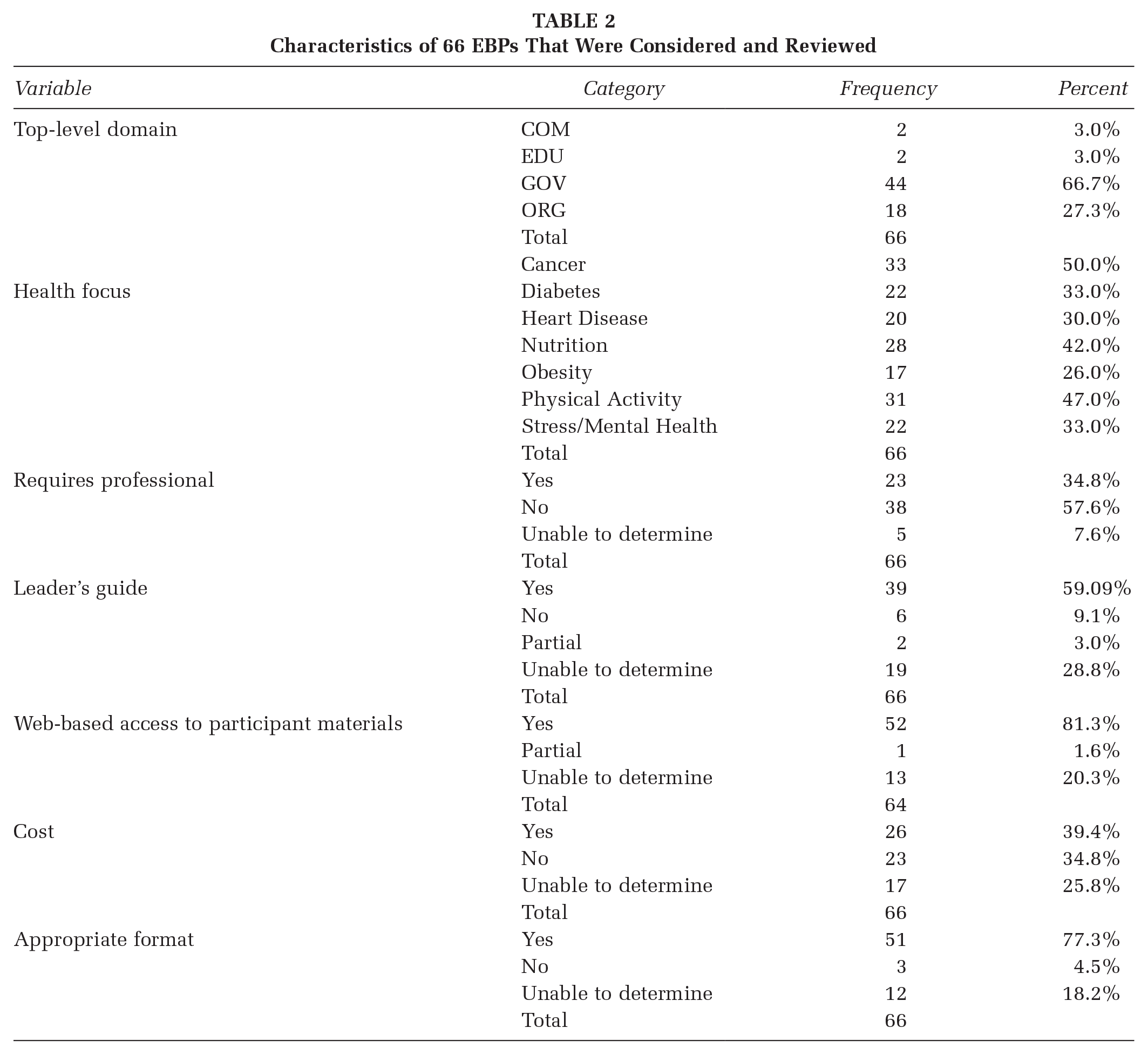
This process resulted in the identification of 66 potential programs. The programs that met our specific criteria for use in the community are described in Table 2. The descriptive categories include the internet domain (e.g., edu and org), the health focus of the program, whether the program requires trained or licensed professionals, the availability of a facilitator or leader guide, the availability of participant materials, whether there is a cost for the program, and if it can be implemented using a group format. The table indicated that not all criteria could be determined from the information available on the website. Programs for which all inclusion criteria could not be determined were considered as not suitable for our EPICC FBOs.
Characteristics of 66 EBPs That Were Considered and Reviewed
Applying the selection criteria to the 66 programs identified in the process described above resulted in identification of six health promotion programs that met all criteria for usability in faith communities. Additional details were extracted for these programs and entered in the REDCap database (Harris et al., 2019). See Supplemental Table for more information including the names and websites of the 66 potential EBPs.
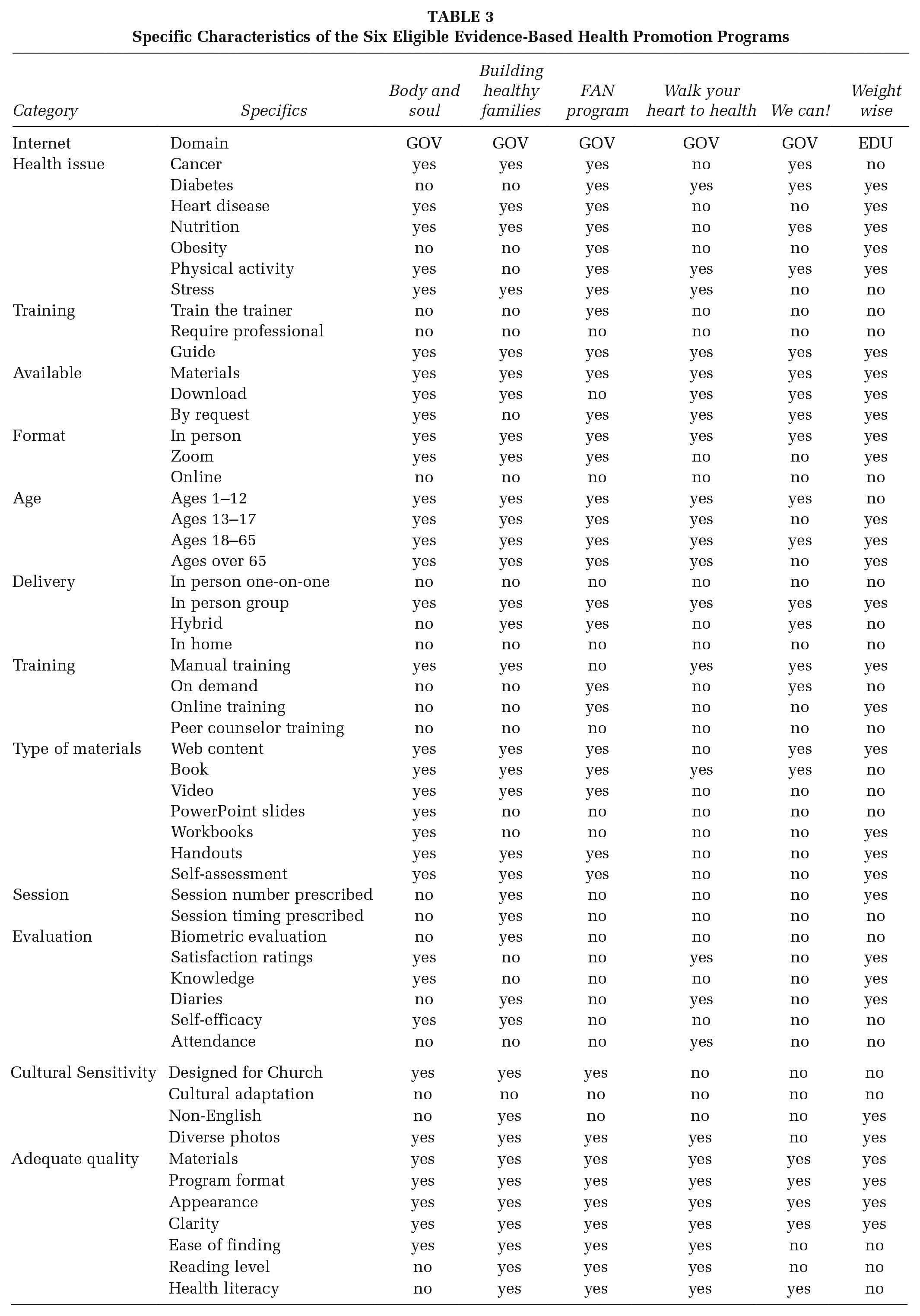
Table 3 presents the results of coding the six programs for their specific characteristics. Across the six programs there is good coverage of the targeted health issues including cancer, cardiovascular disease, diabetes, hypertension, and obesity. Most programs are appropriate for multiple health conditions. We coded whether the program had a train-the-trainer component, which was the case for one of the six programs. We indicated whether the program materials were available using online download or by request. The Faith, Activity and Nutrition (FAN) program (CDC, 2018) is available but requires additional steps beyond downloading or requesting the material; the six train-the-trainer sessions are online. All six programs are suitable for in-person implementation with groups, with none designed for one-on-one delivery. No programs are exclusively online interventions. Adults aged 18–65 years are served by all six programs, and five are designed to include families and young children. Training materials are available for all programs. Across the six programs there are a variety of available materials including web content, books, workbooks, handouts, videos, and self-assessments. There is considerable flexibility in the number and timing of the intervention sessions. Three of the six programs were designed for use in churches, while none of them had specific instructions for adapting the program to different ethnic or cultural groups. Two of the programs are available in languages other than English, and most have photos that reflect ethnic diversity. Most program materials were assessed by reviewers to be attractive and clearly written, with some having potential issues of higher required reading levels and possibly health literacy. Overall, the six programs appear to be quite usable and to apply to many ages and health conditions.
Specific Characteristics of the Six Eligible Evidence-Based Health Promotion Programs
Discussion
Our extensive search for EBPs suitable for implementation by FBOs resulted in the identification of six programs that met all criteria for the EPICC Project. These six programs address risk factors for chronic diseases that are disproportionately prevalent in communities of color in the United States, are available at no cost with materials that can be downloaded from the internet or research teams and include facilitation guidance and resources for community members without requiring professional health care training. The program materials and illustrations have been designed with diverse end users in community settings, and three were developed for use in FBOs. Four include resources that support planning and evaluation of process and behavioral outcomes while the FAN train-the-trainer online sessions are designed to guide the program’s implementation team’s development of an overall plan for their faith community.
The search for EBPs for the EPICC Project was challenging because there is no centralized repository for EBPs that focus on health promotion. Despite substantial investments of time and resources to develop evidence-based programs (Lee-Easton, Magura, & Maranda, 2022) the process of identifying those that are relevant to specific user audiences and health conditions is not straightforward (Lee-Easton, Magura, Abu-Obaid, et al., 2022). Furthermore, it appears that few programs are designed for implementation by community members rather than by clinicians or researchers (Harden et al., 2021).
A number of recent publications have discussed shortcomings of EPB repositories including difficulty finding them, incomplete information about the scientific basis for listing the programs as evidence-based, differences in criteria for inclusion, inclusion of programs that were developed decades ago that lack updated information, and little or no guidance for selecting programs for dissemination and implementation (Buckley et al., 2020; Harden et al., 2021; Percy-Laurry et al., 2021; Zack et al., 2019). Our search process led to many useful resources for promoting health. However, much of the information on federal websites was in the form of guidelines or information that can be combined to design health promotion programs to address diverse health conditions. We found many EBPs that had demonstrated positive health impacts that were designed to be delivered by nurses or other licensed health care providers or trained community health workers. Some programs did not provide facilitator guides or educational materials for participants, and for some the information and/or delivery format was more than 10 years old. Several federal websites did not identify any evidence-based programs or had broken links for identified programs. Other EBPs, credited to federal websites, are now housed by universities or other nongovernmental parties. Fewer than half of the programs are available at no cost. The kinds of challenges we encountered in our attempt to identify EBPs contribute to a lack of access to potential programs for addressing health disparities.
There are many tools on federal websites that are not formatted or organized as evidence-based programs. These tools, such as educational videos, planners, and mobile phone applications identified as “evidence-based resources” have the potential for being configured to serve as community-ready programs; however, currently they are not helpful for people who do not have health and/or program planning backgrounds or resources to purchase or receive guidance on how to prepare for, implement, and evaluate progress and outcomes. Lack of health knowledge, money, access to health care resources and general health literacy are factors contributing to health disparities (LaVeist et al., 2023). These factors need to be considered in packaging these resources to meet the needs of nonclinical community organizations.
Developers of EBPs that are intended for community implementation bear the primary responsibility for designing interventions that can be readily disseminated and used to improve public health (Kwan et al., 2022). The EBP repositories that exist have been developed for researchers and public health professionals rather than for community-based organizations (Harden et al., 2020). The dominant paradigm in current systems for developing and disseminating health promotion programs reflect a push from academic and policy domains, rather than a pull from community-based organizations (Brownson et al., 2018). There is a need for more effective dissemination as part of investigating the impact of EBPs designed to reduce disparities among African Americans (Singh et al., 2023). Providing health promotion programs that are feasible and acceptable for community implementation is one path for increasing capacity in community organizations for positively impacting health outcomes and promoting health equity.
Implications
The following suggestions are offered as ways to address or mitigate the challenges identified in this project:
Utilization of community-based participatory research (CBPR) as the model for designing EBPs could enhance the availability of health promotion programs that meet community needs (Wallerstein et al., 2018). Community participation in program development focused on the actual end users is essential to develop EBPs that will be used in communities (Racine et al., 2022). Funding to support development of health promotion programs that can be delivered by trained community members, with training incorporated into the programs such as via recorded videos, may lead to development of more programs that can be offered to communities that do not have access to research teams or funding for health care providers.
Public health efforts, as well as the work of researchers, will be enhanced if repositories provide clear definitions of evidence-based programs and their criteria for inclusion in their directory.
Searches for health promotion programs for community-based organizations would be simplified with a consistent structure across federal websites. EBPs can be indexed by setting and provider, for example, in addition to health conditions that are addressed.
Improved marketing and promotion of health promoting EBPs need to target desired program end-users, including communities affected by disparities in health outcomes. Rather than requiring community organizations to determine where to search for programs on federal websites, health promotion program developers could take responsibility for disseminating information about their programs through social media to community partners who serve as trusted sources of information about health. State and local departments of health, county extension systems, and public libraries can collaborate in disseminating information about and access to these programs for community-based organizations (Brownson et al., 2018; Flaherty & Miller, 2016; Harden et al., 2020). Evidence-based program registries have been shown to increase EBP utilization in health care practice (Lee-Easton et al., 2023; Magura et al., 2023).
All materials required to put together an effective EBP need to be readily available, in a culturally appropriate format, without additional costs to users. Programs that are developed with federal funding need to remain available through designated sites, especially when proven to be effective in promoting healthy changes.
Federal organizations that fund health promotion and/or behavior change research need to support EBP development of all the program components including clear guidance for facilitators and be available for download. EBPs developed with federal dollars need to be accessible at no additional cost, designed for the expertise or capacity level of the targeted population and include dimensions in the program reflective of that population’s values and needs. This approach reflects the evidence-based practice process and uses federal dollars more effectively.
Strengths of FBOs need to be identified and leveraged to promote adoption of EBPs. FBOs can provide culturally-relevant, supportive environments for implementing EBPs that address risk factors associated with health problems that disproportionately affect African Americans (Brewer & Williams, 2019; Lancaster et al., 2014). Additional research needs to be done to better understand the needs and capacities of congregations, and how to best bring useful EBPs to these community organizations.
Limitations
This search for EBPs focused on federal repositories and did not extend to a wider realm of potential sources of programs to be delivered by community members in their own neighborhoods and organizations. It is likely that there are programs that meet the criteria used for this study that were not identified by our process. Implementing EBPs outside of health care settings or with research support may be beyond the capacity of many organizations, and greater understanding of what FBOs need to be successful is needed. The EPICC Project is designed to learn from FBOs what aspects of technical assistance are desired and effective for EBP implementation with fidelity and beneficial health outcomes.
Conclusion
Lack of access to health information and programs to support behavior change is one of the contributing factors to health disparities (Biglan et al., 2023; Fagan et al., 2019; Lee-Easton et al., 2023; Sampson et al., 2016). A report funded by NIH estimated economic burden of racial and ethnic health inequities to be $421 billion using the Medical Expenditure Panel Survey (MEPS) and $451 billion using the data from the Behavioral Risk Factor Surveillance system (BRFSS) in 2018 (LaVeist et al., 2023). Furthermore, the report found most of the economic burden to be related to the “poor health” (LaVeist et al., 2023, p. 1687) of the U.S. Black population. The need to address health inequities is well documented, and we propose EBPs appropriate for use in faith communities as one approach to addressing this problem. Evidence-based health promotion programs that are accessible, culturally relevant, and up-to-date are one method of disseminating health information, providing resources, and supporting health behavior change.
African American faith communities offer opportunities to address health disparities in communities that have limited resources and access to clinical providers (Brand, 2017; Leyva et al., 2017). Only a small percentage of evidence-based prevention programs have been developed with input from disadvantaged populations (Biglan et al., 2023). Efforts to address health inequities suggested by the findings reported in this paper could be enhanced with development of EBPs tailored for specific communities that do not require professional health care provider facilitation, are available at no cost to the user, are easily located on the internet, and are downloadable. We recommend that these criteria be considered in developing EBPs, and furthermore, that programs to address health disparities be designed with careful attention to the capacities of end users to locate relevant programs (Klesges et al., 2005).
Health promotion programs supported with evidence can be disseminated through federal registers with clearly marked and well-publicized community portals, as well as through community-based organizations and social media. A federally coordinated repository of EBPs linked to federal websites such as the CDC and NIH Institutes could be created to house all EBPs currently available to public users. This repository would need to be routinely updated with user-friendly search options and standardized evidence-based language. In addition, the meaning of an “evidence-based program” needs to be defined in every program that uses that label. These steps could extend the capacity of faith-based and other local organizations to effectively promote health equity.
Future areas of research include EBPs developed with a community-based participatory research (CBPR) approach (Wilkins et al., 2023). Community participation in EBP development can contribute to clearer recognition of community values and beliefs, cultural relevance of products, community buy-in, and user-friendly formats. Furthermore, we recommend that the academic faculty collaborate with community organizations that are connected to neighborhoods in disseminating EBPs that can be implemented by trusted individuals in those communities. Collaboration of all parties is needed to positively impact health inequities.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399241259688 – Supplemental material for Challenges in Disseminating Evidence-Based Health Promotion Programs in Faith Community Settings: What We Need to Include
Supplemental material, sj-docx-1-hpp-10.1177_15248399241259688 for Challenges in Disseminating Evidence-Based Health Promotion Programs in Faith Community Settings: What We Need to Include by Sharon C. Jones, David Schlundt, Neely Williams, Meredith Smalls, Korab Idrizi, Leah Alexander, Monique Anthony and Rebecca Selove in Health Promotion Practice
Footnotes
Authors’ Note:
The authors would like to thank Savannah Childress and Kristina Casterline for their initial work on this project as well as Dr. Arthur Lee for his community perspective, Research reported in this publication was supported by the Office Of The Director, National Institutes Of Health of the National Institutes of Health under Award Number U01OD033244. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.