
Abstract
Sex workers experience elevated risks of sexual and gender-based violence (SGBV) from intimate partners, clients, and community members that harms health and human rights. While SGBV contributes to poorer sexual and reproductive health (SRH) outcomes among sex workers, including elevated human immunodeficiency virus (HIV) vulnerabilities, stigma targeting sex workers reduces SRH service access and uptake. The Congo Republic is an exemplar context to address stigma toward sex workers. Sex workers’ HIV prevalence (8.1%) in Congo Republic is double the national prevalence, yet research indicates that nearly one-fifth (17.2%) of sex workers in Congo Republic avoid health care because of stigma and discrimination. This Resources, Frameworks, & Perspectives article describes the process of developing Esengo ya Bosembo (“Joy of Equity”), a culturally tailored advocacy video that aims to reduce health care and community stigma toward women sex professionals (e.g., sex workers) in Pointe-Noire, Congo Republic. This knowledge translation product stems from a participatory mapping intervention with sex professionals in Pointe-Noire that revealed the need for sensitization tools and activities to reduce sex work stigma among health care providers and community members. The video incorporates three overarching key messages: (1) sex professionals are human beings with equal rights to dignity, protection, and health services; (2) elevated risks of SGBV and stigma targeting sex workers reduce SRH service access and uptake; and (3) participatory mapping is a potential way to empower sex professionals to share their experiences and recommendations for change. This article details how health promotion practitioners and sex professionals may use the video to advocate for change.
Keywords
Assessment of Need
Sex workers experience elevated sexual and gender-based violence (SGBV) risks from intimate partners, clients, and community members (Logie et al., 2020). SGBV contributes to worsening sex workers’ sexual and reproductive health (SRH) outcomes, including human immunodeficiency virus (HIV) risk (Decker et al., 2015). Stigma toward sex workers reduces SRH service use despite increased need (Shannon et al., 2014). Stigma toward sex work, SGBV, and HIV are profound barriers to accessing adequate health care and to realizing human rights (Decker et al., 2015; Shannon et al., 2014).
This Resources, Frameworks, & Perspectives article describes the development of a video that aims to reduce stigma toward sex professionals among health care providers and community members in Pointe-Noire, Congo Republic. In Pointe-Noire, as the term “sex professionals” is preferred over the term “sex workers,” we use “sex professionals” from here on. In Congo, sex professionals’ HIV prevalence (8.1%) is double the national prevalence (UNAIDS, 2018). In a study with sex professionals in Congo, nearly one-fifth (17.2%) reported avoiding accessing health care because of stigma and discrimination (UNAIDS, 2018). Together these findings signal the urgent need to address stigma and advance health equity with sex professionals in Congo.
From 2022 to 2023, we developed and piloted a multi-methods study in collaboration with the Union pour l’Assistance aux Femmes Prostituées d’Afrique (UAFPA; Union for Assisting Female Prostitutes in Africa), a community-based organization supporting women sex professionals, and a health care clinic located in Pointe-Noire. In brief, this study involved (1) participatory mapping (Logie et al., 2023) to amplify lived experiences of stigma and SGBV among sex professionals, and (2) voluntary, complimentary, and confidential HIV and sexually transmitted infection testing offered as part of these workshops, with access to care and follow-up treatment provided. We conducted a series of five 2-day participatory mapping workshops, each with 20 participating sex professionals aged 16 or more in Pointe-Noire. A cross-sectional study examining HIV prevalence among women sex professionals in five cities in Congo reported Pointe-Noire as having the highest prevalence (12.8%; Niama et al., 2017) of these five cities. Findings from participatory mapping revealed profound, pervasive, and persistent stigma and barriers to accessing health services, with recommendations for stigma reduction sensitization activities with community members and health professionals. The video herein described directly responds to these recommendations for stigma-reducing sensitization leveraging the participatory mapping findings. The original study received Institutional Review Board/Human Subjects approval from the University of Toronto Research Ethics Board (Protocol Number: 41845), and Comité d’Éthique pour la Recherche en Santé de la Fondation Marie Madeleine Gombes (“Research Ethics Committee in Health of the Marie Madeleine Gombes Foundation”). The video described in this article is part of knowledge sharing and did not require research ethics board approval.
Description of the Innovation
The short video combines French narration, English or Lingala subtitles, stigma-reducing digital photographs of the participatory mapping process and context of Pointe-Noire, music inspired by sex professionals in mapping sessions, and basic graphics.
Our knowledge translation planning framework for video creation followed the required steps of identifying knowledge user audiences, linking knowledge user audiences to specific goals, and developing messages from these goals (Barwick et al., 2020). The first step was to identify the main stakeholders who will use the video as an advocacy tool herein referred to as “users”: (1) health promotion practitioners and (2) sex professionals; and these users’ main audiences: (1) decision-makers, policymakers, health professionals, funders and (2) sex professionals, communities, and funders. This allowed us to identify goals for the video, outlined in Figure 1.

Goals for Advocacy Video
The second step was to develop a set of key messages based on the intended users (Graham et al., 2006) and the related goals. The third step was to develop a set of interview questions to identify the key knowledge translation messages. Table 1 outlines the interview questions used to generate understanding about key messages.
Sections Included in Video
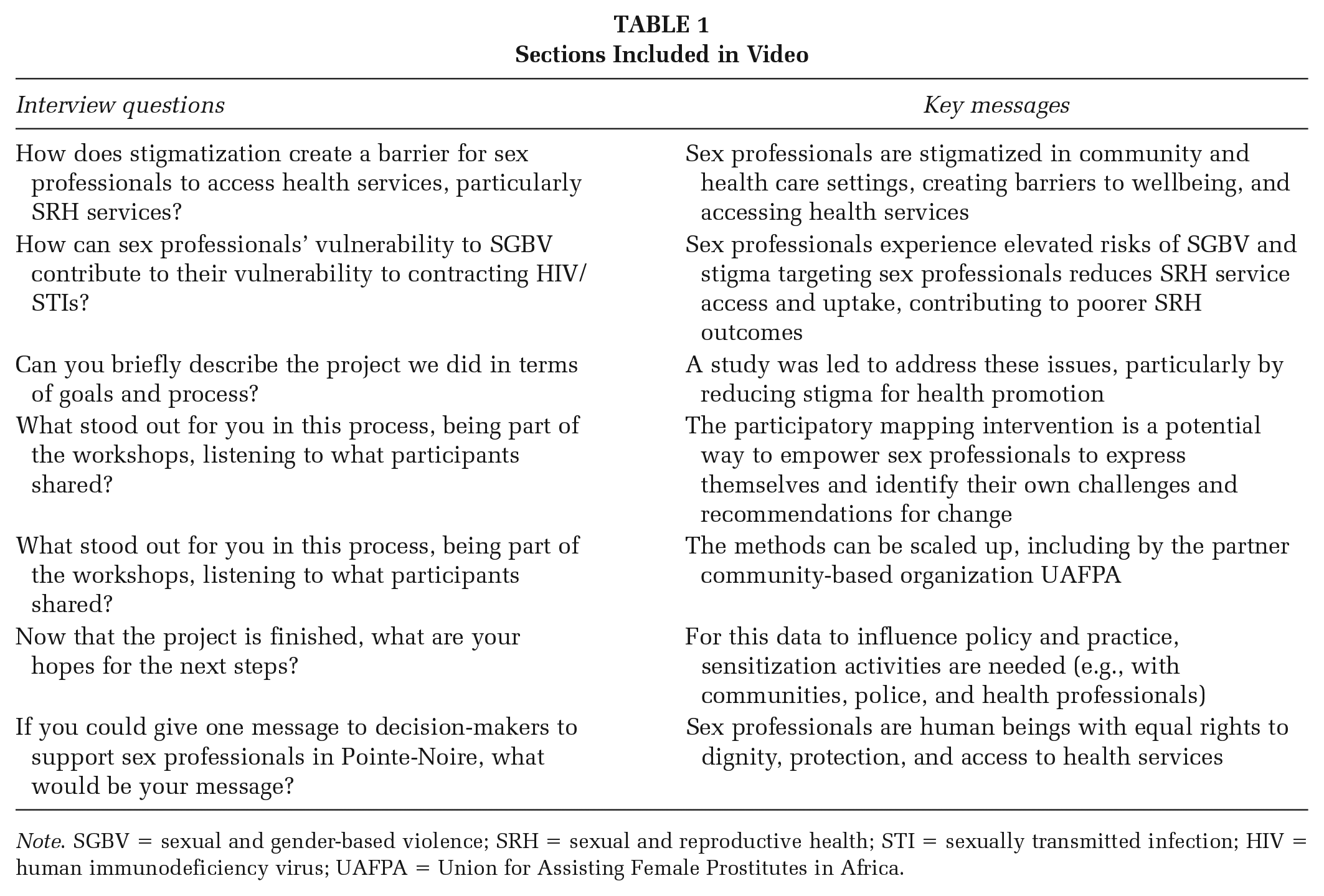
Note. SGBV = sexual and gender-based violence; SRH = sexual and reproductive health; STI = sexually transmitted infection; HIV = human immunodeficiency virus; UAFPA = Union for Assisting Female Prostitutes in Africa.
Intended Impact
This video, which is culturally tailored to ensure relevancy and relatability, provides a tool for public health education on sex work stigma reduction. The culturally tailored elements of the video include: (1) narration derived from an interview with a local community leader; (2) images of Pointe-Noire and workshop processes; (3) instrumental music produced by a Congolese musician based on a song created by participants; and (4) subtitles in the local language of Lingala. This health promotion video offers an educational tool to raise awareness of violence and stigma against Congolese sex professionals with different stakeholders and can inform SRH service provision with sex professionals.
Video-Making Methodology
Below we outline the main steps involved in the process of making this video.
Interview
As part of engaging with community stakeholders in the design, implementation, and evaluation of the video, we recorded an interview with a local community leader and study assistant at the end of the project, inviting her to reflect on the study method and impact. Selecting the main narrator perspective for an advocacy video is essential to ensure the video is well communicated in narrative form and contextually tailored (Hébert et al., 2020), and to further the project’s aims by respectfully representing the local population it is engaged with in health promotion activities. Audio was recorded in a quiet, private location using a free voice recorder app on a smartphone.
Photography
To create stigma-reducing images for use in the video, we photo-documented various phases of the project using smartphones. These were nonidentifying photos taken from the back of participants to protect anonymity. We also photo-documented a variety of places around Pointe-Noire (e.g., a pharmacy, a beach, and neighborhoods) that connect to sex professionals’ experiences, using a range of perspectives, for example, an aerial view of the city taken from an airplane and eye level taken from standing at the edge of the ocean surf.
Scripting
After recording and transcribing the interview, the next step was to write a script. The aim was to build a compelling narrative by, first, highlighting key quotes in the transcript and, second, arranging these quotes in a particular order to develop a narrative structure. This is where a focus on personal storytelling and conversational language may help to increase the potential emotional impact. For example, in the video, the narrator states, “I’ve never heard a sex professional say she was raped, and the rapist used protection. It is always without a condom.” The first sentence here brings a tone of sarcasm that helps to engage viewers in a way that simply stating the fact “unprotected sex” could not do. We created a storyboard to facilitate this process.
Video Editing
With the script written, the next step was to edit together the various sound bites selected, and in the order planned. Keeping the original timestamp reference from the transcript in the script, to estimate the approximate start and end times of each sound bite, helps expedite this process. It is in this stage where you will discover whether the real-time audio of the interview can be used as planned. For example, you may cut part of a sentence and shift its placement to produce new meaning. Challenges can emerge when the audio files are edited together. For instance, a sentence may end with a voice inflection that is left hanging, or something may have been said very quietly or quickly and is difficult to understand. In shifting from the written word to working with the spoken word, affectivity becomes more important—whereby the video can spark the viewers’ emotions while sharing affective knowledge. Once satisfied with the narrative arc, we conducted fine-tune editing of the audio clips to adjust the pacing and flow so that it would sound and feel more natural. Once there was a clear narrative with a natural flow, we edited photos alongside the narration to build a visual narrative and help bring the story to life. To ensure anonymity within images, a Gaussian blur filter was applied to blur out faces and other identifiers, such as the name of a pharmacy, license plate numbers, and the brand of HIV self-test.
Sound
Background music is key to video-making palettes, as music helps to shape audience emotions at every moment in the piece. With our video, the background music consists of two songs. The first is a royalty-free song RUN by Ant.Survila sourced from http://dig.ccmixter.org/ and selected for its serious mood, to accompany the narration establishing the issues the study sought to address. The second song is an output from our study. As part of the participatory mapping workshops, participants were engaged in developing songs which communicate their dreams for reducing sex work stigma in their communities, in health care settings, and with the police. To develop this song-making methodology, we worked with peer navigators who were trained as participatory mapping facilitators and created a song that we developed to be broadcast-quality through collaborating with a Congolese musician. An instrumental version of this song is integrated into the second half of this video, with the joyous mood suggesting the enjoyment experienced by participants in participatory mapping. The song files needed to be trimmed to fit the length of the video, with sections cut and rearranged so that various moods within each song would align with particular parts of the story. The final step in sound design was sound mixing, which involved adjusting the levels of the narration and music to achieve the desired effect.
Translation and Subtitles
The original language of the interview and script is French. To support wider use of the video toolkit, the script was then translated, and the video subtitled into English and Lingala, resulting in two versions of the video. Translation from French into Lingala, and approval of the placement of Lingala subtitles against French narration, was done by the same local community leader and study assistant in Pointe-Noire who was interviewed and featured in the Esengo ya Bosembo video to ensure accuracy for the local context. Translation from French into English was done by a bilingual (English/French) researcher from the University of Toronto who had been part of the study’s fieldwork in Congo and who could verify the meaning in consultation with the local community leader. For example, it was extremely important to retain the intended meaning behind the use of “professionels du sexe” (“sex professionals”) when translating from French to English.
Graphics
A closing slide was produced which includes essential elements to consider for any advocacy video: the logos of key partners and the funder, and a URL where viewers can find more information. We provide access to Esengo ya Bosembo freely through our website (https://sshinelab.com/) so it may be widely used by health promotion practitioners.
Using This Tool in Advocacy: Next Steps and Opportunities
Short videos have been shown to be effective in reducing patient-directed stigma (Ng et al., 2017), and are an accepted knowledge translation and training tool among health professionals (Hébert et al., 2020). Health promotion practitioners can use the Esengo ya Bosembo (“Joy of Equity”) video for health care training and advocacy. The video is under 2 minutes in length so it can be hosted on X, formerly known as Twitter, a social media platform for leading global public health organizations, and posts can be shared with allies (e.g., African Sex Workers Alliance), used as a resource or for alliance-building, and linked to advocacy campaigns, for example, the Global Network of Sex Work Projects’ International Sex Workers’ Rights Day. Focused communication strategies with use of specific hashtags such as #SexWorkerRights can maximize outreach and impact. Once natively hosted on X, the post can be shared across additional social media platforms. The post can be used to draw viewers to other resources or events related to reducing sex work stigma. For example, the video can be used in sensitization workshops as a catalyst for dialogue and could become part of a comprehensive advocacy toolkit, together with synthesized participatory maps, songs, a summary of mixed-methods findings presented through accessible infographics, and stigma training modules. The process of translating research into changes in policy and practice may be accelerated by such multi-media knowledge translation endeavors (Graham et al., 2006).
The video can also be used by sex professional partners in Pointe-Noire, for example, UAFPA, and sex professional organizations across other African regions for their own sensitization and scaling up efforts. To support such use of the video by local partners, we made a version available with subtitles in Lingala.
This advocacy video is a culturally tailored, relatively inexpensive way to share study findings while aiming to reduce sex work stigma among community members and health care providers. Integrating arts-based methods (song, video, art) into the science of stigma reduction with sex professionals offers an innovative way to advance health and rights through showcasing alternative methods of health care practice. Although we did not formally evaluate the effect of the video on stigma reduction, we hope that future researchers can use the video and conduct rigorous evaluations on its utility for health promotion and stigma reduction among sex professionals. We look forward to hearing from researchers and practitioners in diverse settings about their use of the video.
Footnotes
Authors’ Note:
This study is funded by Grand Challenges Canada (2022–2023; Logie, grant no. R-ST-POC-2205-52021), and Canada Research Chairs Program (Logie).
Author Contributions
Sarah Van Borek: Substantially contributed to the conception and production of the advocacy video, project management and facilitation of the study, preparing research tools, acquisition, analysis, and interpretation of data, and writing of the manuscript; critically reviewed the manuscript for important intellectual content; provided final approval of the version to be published; agreed to be accountable for all aspects of the work, ensuring accuracy and integrity.
Carmen H. Logie: Substantially contributed to the conception and design of the work and to writing the manuscript as Principal Investigator; acquisition, analysis, and interpretation of data; critically reviewed the manuscript for important intellectual content; provided final approval of the version to be published; agreed to be accountable for all aspects of the work, ensuring accuracy and integrity.
Bibiche Mbende: Substantially contributed to project management and field work involving data collection; critically reviewed the manuscript for important intellectual content; provided final approval of the version to be published; agreed to be accountable for all aspects of the work, ensuring accuracy and integrity.
Laure Stella Ghoma Linguissi: Played a significant role in project management and contributed to field work involving data collection; critically reviewed the manuscript for important intellectual content; provided final approval of the version to be published; agreed to be accountable for all aspects of the work, ensuring accuracy and integrity.
Frannie MacKenzie: Substantially contributed to project management, and analysis and interpretation of data; critically reviewed the manuscript for important intellectual content; provided final approval of the version to be published; agreed to be accountable for all aspects of the work, ensuring accuracy and integrity.
Anaïs Ouedraogo: Played a significant role in preparing research tools, and analysis and interpretation of data; critically reviewed the manuscript for important intellectual content; provided final approval of the version to be published; agreed to be accountable for all aspects of the work, ensuring accuracy and integrity.
Anoushka Lad: Played a significant role in project management and in preparing research tools; critically reviewed the manuscript for important intellectual content; provided final approval of the version to be published; agreed to be accountable for all aspects of the work, ensuring accuracy and integrity.
Anicet Boumba: Played a significant role in project management and contributed to field work involving data collection; critically reviewed the manuscript for important intellectual content; provided final approval of the version to be published; agreed to be accountable for all aspects of the work, ensuring accuracy and integrity.
Lesley Gittings: Played a significant role in project conceptualization; critically reviewed the manuscript for important intellectual content; provided final approval of the version to be published; agreed to be accountable for all aspects of the work, ensuring accuracy and integrity.
Hugues Loemba: Played a significant role in project conceptualization; critically reviewed the manuscript for important intellectual content; provided final approval of the version to be published; agreed to be accountable for all aspects of the work, ensuring accuracy and integrity.
Ethics Approval and Consent to Participate
This study received approval from The University of Toronto Research Ethics Board (Protocol Number: 41845) and Comité d’Éthique pour la Recherche en Santé (CERS) de la Fondation Marie Madeleine GOMBES (Research Ethics Committee in Health of the Marie Madeleine Gombes Foundation).