
Abstract
The spread of health misinformation has made the task of health communicators more difficult. However, the success of health messaging hinges not only on meaningful message content but also on the credibility of who is delivering the message. “Trusted messengers,” like local leaders and community-based organizations, have a greater ability to influence improvements in community health, due to their shared cultural experience with their communities. Health communication agencies should empower trusted messengers with the tools they need to succeed in health communication. One tool critical for their success is a succinct health messaging framework to plan and implement health messaging. Marketing has “See, Think, Do”—a simple, practical framework used to influence consumer purchases. As a more trustworthy corollary, we propose the “Lights, Facts, and Goals” framework, a concise, authentic, and transparent method for planning, implementing, and assessing health messaging campaigns that influence health improvements. “Lights” refers to different methods of reaching communities like trusted messengers, advertisements, and text messages. “Facts” refers to key sourced scientific information relevant to a specific aspect of community health. “Goals” refers to actions community members can take to improve their health in connection with the communicated health facts. This article describes how the “Lights, Facts, and Goals” framework both simplifies the creation and communication of scientifically sound health messaging and strengthens the partnership between health agencies and trusted messengers in the community. Through “Lights, Facts, and Goals,” community-based organizations, community leaders, and their partners will be more effective at improving community health through messaging.
Keywords
Requirements For An Improved Health Messaging Planning Framework
Introduction
The fundamental objective of public health messaging is to improve individual and community health. To achieve this goal, health messaging often seeks to promote specific health behaviors. However, the complexity of the health information environment challenges health officials’ ability to affect behavior change.
Defeating Health Misinformation
Insufficient communication from trusted sources contributed to the success of misinformation during the COVID-19 pandemic (Korin et al., 2022). During ongoing and future health threats, doctors, scientists, and public health officials must facilitate health communication from trusted sources to defeat misinformation.
Importance of Community Engagement
As emphasized in the U.S. Surgeon General’s 2021 report on Confronting Health Misinformation, the employment of “trusted messengers” to reach and communicate with specific populations is growing in use in public health (Office of the Surgeon General, 2021). Community-based organizations (CBOs), with strong ties to community members, are key partners in implementation of effective public health messaging (Korin et al., 2022).
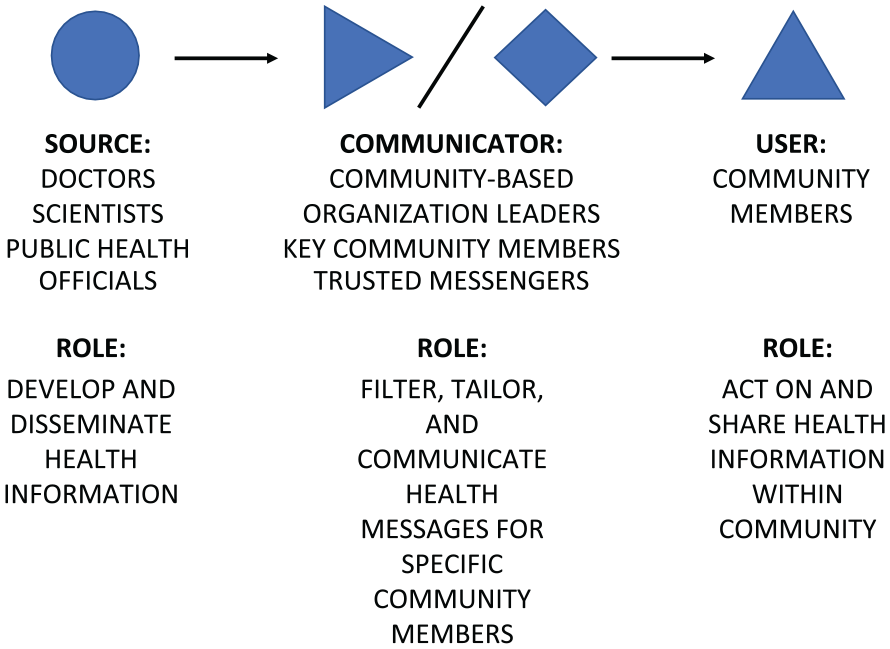
To standardize the critical role of CBOs in community communication, a model for health communication needs to include CBOs centrally as health communicators. As shown in Figure 1, we propose the “Source-Communicator-User” model, which builds on previous models of communication but highlights the more active role CBOs can fulfill in effective health communication (Lasswell, 1948; McGuire, 1981).
The Source-Communicator-User Model for Health Communication
In other communication models (Lasswell, 1948; McGuire, 1981), CBOs might appear as “channels” for information dissemination. However, CBOs can tailor health information by wording, framing, and translating content to be more usable and relevant to their communities, which gives them a significant role within the health communication process as “communicators.” “Sources,” such as doctors, scientists, and public health officials, can communicate more effectively when amplified through trusted messengers and CBOs (Korin et al., 2022).
We also deliberately chose the term “user” rather than “receiver,” as in the McGuire (1981) communication model, to describe community members engaged with health messaging. A user of health information suggests the more active rather than passive role community members have in learning from and acting on health information. The “Source-Communicator-User” model solidifies the necessary relationships scientists, community leaders, and community members should maintain in health messaging campaigns.
Need for Messaging-Specific Planning Frameworks
Communication professionals in fields like marketing rely on communication frameworks to plan and implement messaging, such as “See, Think, Do” which models consumer behavior to generate purchases. Public health communicators could similarly employ several established public health intervention planning frameworks for messaging to improve health. The PRECEDE-PROCEED model is widely used in public health intervention planning and describes steps to ensure interventions address a population’s needs and tie outcomes to health improvement (Green, 1974). The six-step intervention mapping model links intervention design to a specific and modifiable health issue that can be measured and affected through behavioral, environmental, or structural change (Bartholomew et al., 1998). Both the U.S. Centers for Disease Control and Prevention (CDC) and the National Cancer Institute (NCI) developed guidance on communication plans and messaging content through Crisis & Emergency Risk Communication (CERC) (CDC, 2018) and Making Health Communications Programs Work or “the pink book” (NCI, 2011).
These frameworks and communication guidance are valuable for public health communicators. However, these resources were primarily developed for use by doctors and officials from health agencies, rather than CBO leaders and trusted messengers who specialize in community engagement. To empower trusted messengers, health messaging requires a framework to guide both health messaging campaign design and messaging content creation that is as simple and self-explanatory as marketing’s “See, Think, Do” framework.
While “See, Think, Do” focuses on consumers seeing an advertisement, thinking it is relevant, and doing or making a purchase, a health messaging campaign equivalent should focus on empowering community members with information to make improvements to their health in an authentic way that promotes mutual trust. Thus, we created the “Lights, Facts, and Goals” framework as a succinct planning, implementation, and assessment tool specific for health messaging campaigns, complementary to other established public health frameworks, and easily employed by partnered messaging groups.
“Lights, Facts, And Goals”: A Novel Planning, Implementation, And Assessment Framework Specific For Health Messaging Campaigns
Framework Introduction
The process of designing a public health messaging campaign can be described in three segments: “Lights, Facts, and Goals.” “Lights” refers to methods of community engagement that illuminate key elements of health information important to a supported population. Lights could include specific trusted messengers like barbers or stylists talking to community members, billboard advertisements staged in public areas, or text messages sent directly to community members. “Facts” are sourced and concise scientific information that are relevant to a specific and modifiable health threat, such as the increased risk of cardiovascular disease (CVD) in people who smoke. “Goals” are the pertinent, culturally relevant, and realistic behavior changes community members or users of health information can undertake to improve their health, such as quitting smoking or increasing physical activity.
Below, we describe how a CBO or health communication team can employ the “Lights, Facts, and Goals” framework in both planning and implementing a health messaging campaign. In planning, the CBO starts with goal-setting, aligns facts to support those goals, and finally chooses the lights or methods of engagement to communicate the facts and goals. As shown in Figure 2, the CBO, in the “communicator” role, translates prepared content for implementation through specific framing to enhance usability by the supported population. During implementation of the campaign, the CBO evaluates success or failure of the health messaging campaign from both a short- and long-term perspective. Short-term evaluation focuses on message receipt and engagement by the users. Long-term evaluation focuses on metrics of individual or collective behavior change and differences in community health outcomes.
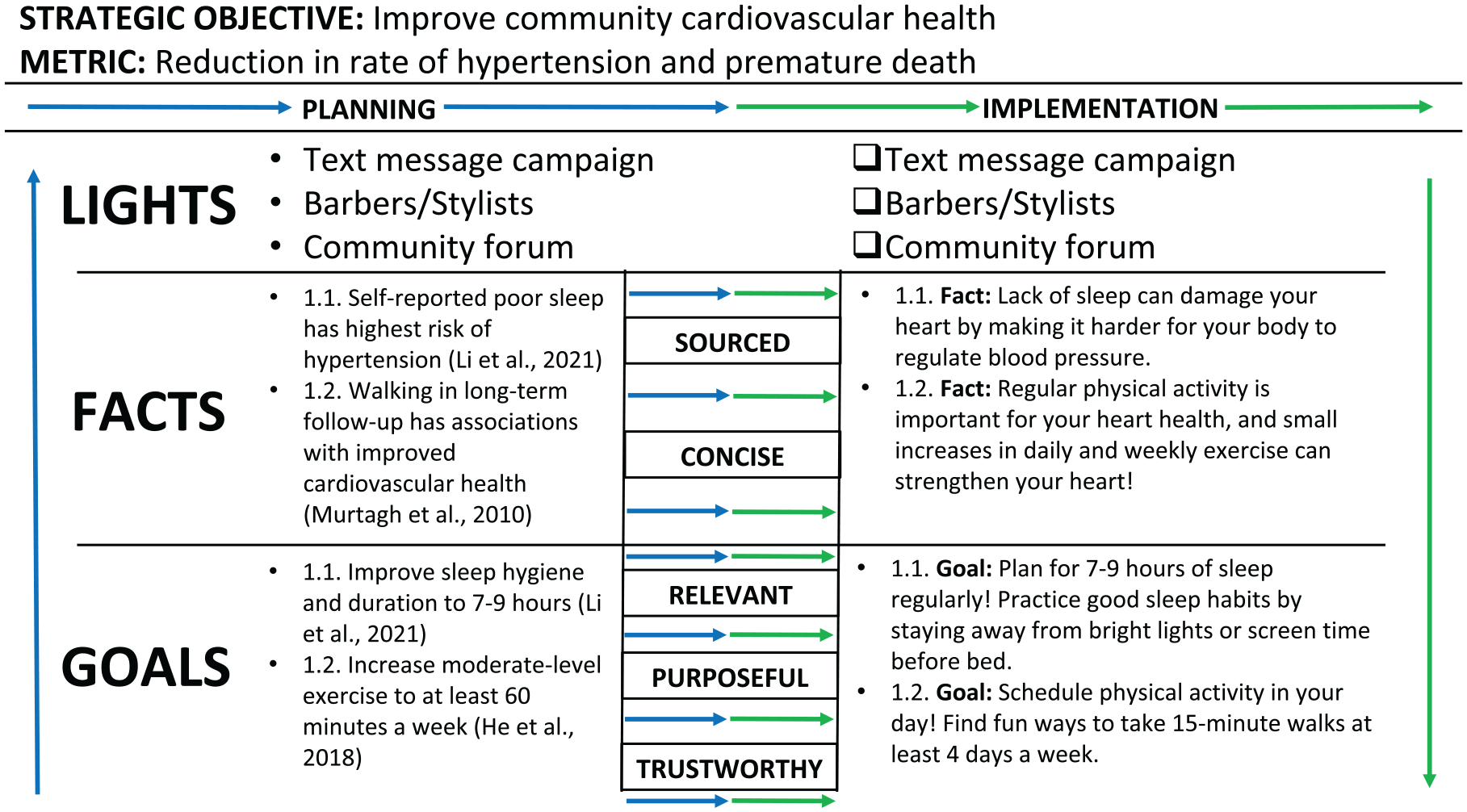
The “Lights, Facts, and Goals” Planning and Implementation Worksheet
Using the Framework—Starting With Goals
The “Lights, Facts, and Goals” framework requires initial focus on a desired health objective, such as reduced measures of cardiovascular disease in a specific community. Goals, like increasing physical activity or cutting down on smoking, represent changes to behavior that make individuals more likely to achieve the campaign’s intended improved health outcome. Goals should be specific with research-backed metrics. For example, defining increased activity by minutes allows individuals to guide their own behaviors. Defining goals thus requires significant research to understand the needs and capabilities of a supported community; methods like the BEHAVE framework—which identifies who you are trying to reach, what you want them to do, what factors influence their behavior, and which actions will most effectively address these factors—can help define meaningful and measurable behavioral change goals (Parvanta et al., 2011).
As intended through the self-explanatory nature of the “Lights, Facts, and Goals” framework, defining goals translates quickly to what is communicated by the CBO to its users. A clear and concise goal could be set off simply as “
Aligning Facts to Support Goals
Facts provide the meaning and purpose behind the goals included in a “Lights, Facts, and Goals” messaging campaign. Facts must be straightforward, understandable, and supported by verifiable scientific evidence. Through research and consultation with experts, the CBO should define facts relevant both to the specific behavior change and strategic community health objective. Facts can be communicated as simply as “
Choosing “Lights” or Engagement Methods to Reach the Community
While facts and goals are communicated explicitly to community members, the lights portion of the “Lights, Facts, and Goals” framework represents different methods of engagement, rather than basic messaging content. Community members could encounter a billboard, read an online advertisement, or receive a text message with a fact and a goal related to a specific health threat. Defining lights to reach the supported community requires analysis of settings, or places community members encounter health information like on public transportation, and channels, or the communication methods used like radio, television, online, or cellular (Parvanta et al., 2011). The CBO or health communication team must ensure selected lights can reach as much of the supported community or users as possible. Specific trusted messengers, like local leaders, clergy members, or barbers and stylists with direct access to their communities, represent effective lights as they can ensure message receipt more directly than an advertisement or a text message (Korin et al., 2022).
Short- and Long-Term Assessment
Assessment of public health communication campaigns in general can be summarized with two questions focused separately on process and effect: “are we doing things right?” and “are we doing the right things?” (Parvanta et al., 2011). For short-term assessment specifically in health messaging, the process question of “are we doing things right?” can be asked as “did the supported community (or users) engage with the messages?” This question addresses the effectiveness of the lights or methods of engagement in the messaging campaign. Engagement can be measured by views, clicks, shares, and response rates or through feedback surveys that rate message utility, relevance, and trustworthiness.
The effect question of “are we doing the right things” has both short- and long-term aspects. The short-term aspect of the desired effect is behavior change: “did the supported community (or users) make the desired behavior change?” Since individual adherence to chosen goals generally cannot be measured directly, surveys on behavior intention and behavior can substitute for direct measurement of behavior change. These surveys also can define changes in health literacy and trust in health messaging, as a further assessment of messaging engagement. Both surveys and engagement data, such as views, clicks, and shares, facilitate in-stride assessment of messaging effectiveness, which allows the CBO or health communication team to enhance messaging content and maximize community engagement.
The long-term aspect of “are we doing the right things” focuses on the health outcome: “did the supported community (or users) achieve a better health outcome?” This question aligns more with the fundamental objective of public health messaging: to improve individual and community health. For a CBO, attempting to measure a novel aspect of a community health outcome could be costly and difficult; however, seeking to improve a health outcome tracked regularly by a local or regional Department of Health allows for a CBO to follow changes over time. Even if only through correlation, the true success or failure of a public health messaging intervention lies within changes in these specific health outcomes.
Conclusion
“Lights, Facts, and Goals” Summary
The “Lights, Facts, and Goals” framework can be implemented by any organization aiming to improve health communication. The use of established health messaging principles in the creation of the “Lights, Facts, and Goals” framework, such as goal-setting, authenticity, and transparency, suggests its success in implementation during health messaging campaigns. Defining goals and facts initially in planning focuses a health communication team on a specific and modifiable health outcome important to the users or supported community. Using multiple lights or methods of engagement ensures that a messaging campaign will reach its users. Finally, the “Lights, Facts, and Goals” framework translates to content creation more directly than other public health intervention models. CBOs and trusted messengers, specialists in community engagement, can improve community health more effectively through this simple messaging framework and the larger scientific community in a strictly supporting role.