
Abstract
Smoke-free policies in multi-unit housing are associated with reduced exposure to secondhand smoke (SHS); however, attitudes toward comprehensive smoke-free policies among residents in subsidized multi-unit housing are unknown. In this mixed-methods study, we explored the socio-ecological context for tobacco and cannabis use and attitudes toward policies restricting indoor use of these products through interviews with residents (N = 134) and staff (N = 22) in 15 federally subsidized multi-unit housing in San Francisco, California. We conducted a geo-spatial and ethnographic environmental assessment by mapping alcohol, cannabis, and tobacco retail density using ArcGIS, and conducted systematic social observations of the neighborhood around each site for environmental cues to tobacco use. We used the Capability, Opportunity, and Motivation behavior (COM-B) model to identify factors that might influence implementation of smoke-free policies in multi-unit housing. Knowledge and attitudes toward tobacco and cannabis use, social norms around smoking, neighborhood violence, and cannabis legalization were some of the social-ecological factors that influenced tobacco use. There was spatial variation in the availability of alcohol, cannabis, and tobacco stores around sites, which may have influenced residents’ ability to maintain smoke-free homes. Lack of skill on how to moderate indoor smoking (psychological capability), lack of safe neighborhoods (physical opportunity), and the stigma of smoking outdoors in multi-unit housing (motivation) were some of the barriers to adopting a smoke-free home. Interventions to increase adoption of smoke-free policies in multi-unit housing need to address the co-use of tobacco and cannabis and commercial and environmental determinants of tobacco use to facilitate smoke-free living.
Keywords
Background
Tobacco use is the leading preventable cause of death in the United States, responsible for over 450,000 deaths annually, and 42,000 deaths from secondhand smoke exposure (SHS; Moritsugu, 2007). Tobacco use disproportionately impacts minoritized populations who have the highest rates of tobacco use, exposure to SHS in multi-unit housing (i.e., high-rise buildings), and tobacco-related disease burden (Cornelius et al., 2020; Homa et al., 2015; Jamal et al., 2016).
Federal and state clean indoor air laws protect people from SHS in public places and hospitality venues (International Agency for Research on Cancer [IARC], 2009), and are associated with reductions in the incidence of cardiovascular disease and lung cancer and hospitalizations from heart disease among smokers and non-smokers (Hahn et al., 2018; Lightwood & Glantz, 2009). However, these laws do not protect people from SHS exposure in multi-unit housing (Homa et al., 2015). Over 80 million individuals in the United States live in multi-unit housing, including 7 million individuals living in subsidized multi-unit housing (U.S. Department of Housing and Urban Development, 2022). However, only a third of the population living in multi-unit housing in the United States are protected by smoke-free policies (Licht et al., 2012).
To address the disparity in access to smoke-free policies in multi-unit housing, the Department of Housing and Urban Development (HUD) implemented a smoke-free policy in 2018 that restricted indoor smoking in public housing authority housing (PHA; U.S. Department of Housing and Urban Development Office of Healthy Homes and Lead Hazard Control, 2014; U.S. Department of Housing and Urban Development, 2015). Approximately 3300 PHA housing implemented the policy (U.S. Department of Housing and Urban Development Office of Healthy Homes and Lead Hazard Control, 2014); however, implementation and enforcement challenges have limited the impact of these policies in PHA housing (Thorpe et al., 2020). Moreover,. the policy does not apply to the majority of federally subsidized multi-unit housing and housing in the private rental market, leaving a gap in access to smoke-free policies unless residents voluntarily adopted smoke-free homes (Thorpe et al., 2018). While the prevalence of smoke-free homes increased from 43% in 1992 to 1993 to 83% in 2010 to 2011 (King et al., 2014; Mills et al., 2009; U.S. Department of Health and Human Services, 2006), smoke-free homes are less prevalent in low-income households with smokers than higher income households (Hafez et al., 2019; Vijayaraghavan et al., 2018; Zhang et al., 2012).
The legalization of cannabis in some U.S. states has also made the regulation of smoking in multi-unit housing challenging (California Department of Public Health, 2018; National Conference of State Legislatures, 2021). While residents of multi-unit housing are supportive of policies restricting indoor combustible tobacco use, their attitudes toward policies that restrict indoor cannabis use is mixed (Delgado-Rendon et al., 2017, 2019). Studies have shown that SHS from cannabis is harmful (Fernandez et al., 2015; Wang et al., 2016); however, indoor use of cannabis is not regulated in multi-unit housing (Anastasiou et al., 2020; Jiang et al., 2018).
The neighborhood and commercial environment, including exposure to pro-tobacco environmental cues and tobacco retail density are also associated with tobacco use and decreased cessation (Cantrell et al., 2015; McDaniel & Malone, 2014). Tobacco outlet density is associated with intention to smoke (Mennis & Mason, 2016; Vyas et al., 2020), and low likelihood of quitting (Reitzel et al., 2011). Multi-unit housing located in a high commercial or mixed residential land use zones where there is an increased density of tobacco retailers can influence multi-unit housing residents’ exposure to tobacco, even in the setting of smoke-free policies (Siegel et al., 2021).
Purpose
In this mixed-methods study, we explored attitudes toward policies restricting indoor use of tobacco and cannabis among residents and staff in federally subsidized multi-unit housing in San Francisco, California. We conducted a geo-spatial and ethnographic environmental assessment by mapping alcohol, cannabis, and tobacco retail density, and conducted systematic social observations of the neighborhood around each site for environmental cues to tobacco use. We triangulated qualitative interviews, neighborhood audits based on observation, and maps of alcohol, cannabis, and tobacco retailers around each housing site to understand commercial and environmental determinants of tobacco use and barriers to smoke-free home adoption (Rucks-Ahidiana & Bierbaum, 2017).
Methods
Setting and Participants
We partnered with the San Francisco Mayor’s Office of Housing and Community Development, focusing on Rental Assistance Demonstration (RAD), federally subsidized housing. At the time of this study, there were 30 RAD subsidized housing properties in San Francisco, of which 15 sites that did not have mandated smoke-free policies were included in this study (Sites 1-15, Figure 3, Table 2). We selected properties based on geographic diversity and property directors’ interest in participating in the study. We contacted the service director of each property to obtain permission to advertise our study and recruit residents and staff. Residents and staff were 18 years or older, living or working in the building, and able to provide informed consent. The University of California, San Francisco, Institutional Review Board approved this study (IRB # 18-25510). The study took place between July 2018 and March 2020.
Study Procedures
At each site, study staff assembled a convenience sample of 6 to 8 resident participants for the focus groups and at least one property management or services staff for in-depth interviews. We conducted 17 resident focus groups including 3 with Chinese monolingual residents. Participants completed a self-administered questionnaire before participating in the focus group or in-depth, semi-structured interviews. We reimbursed all participants $25 for completing study procedures.
Theoretical Framework
We used the social-ecological model to describe the individual, interpersonal, organizational, community, and policy-level influences of tobacco use among residents and staff in multi-unit housing (Figure 1; Glanz et al., 2008). We then used the Capability, Opportunity, Motivation-Behavior (COM-B) model to identify barriers to smoke-free home adoption (Figure 2; Michie et al., 2011). Psychological capability reflects knowledge and awareness, and physical capability refers to skills necessary for behavior change. Opportunity comprises social and physical factors that make behavior change possible. Motivation includes the processes that direct behavior change, including emotional response, habitual processes, and cognitive processes.
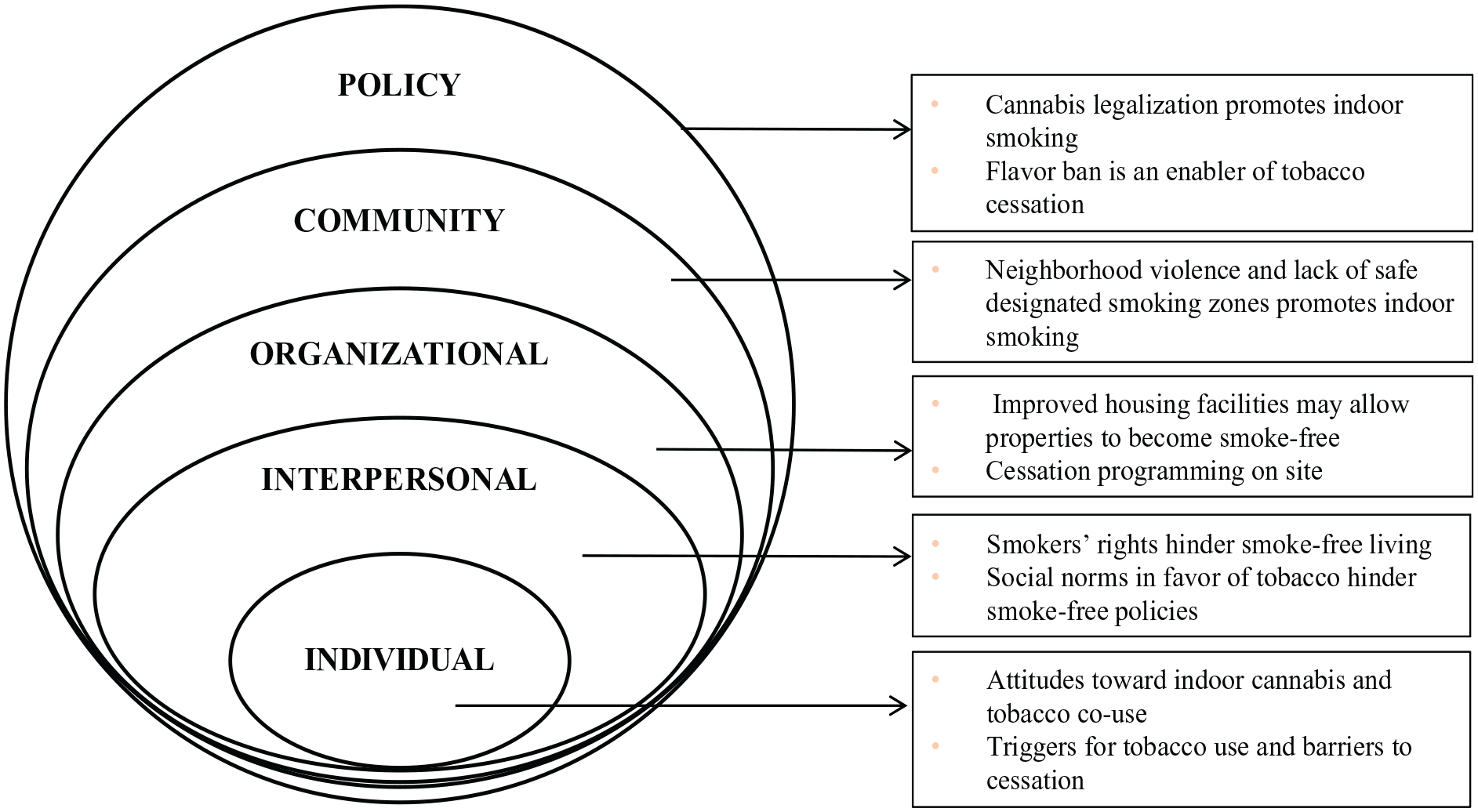
Social-Ecological Model Describing the Context of Tobacco Use Among Residents and Staff in Subsidized Multi-Unit Housing in San Francisco, CA
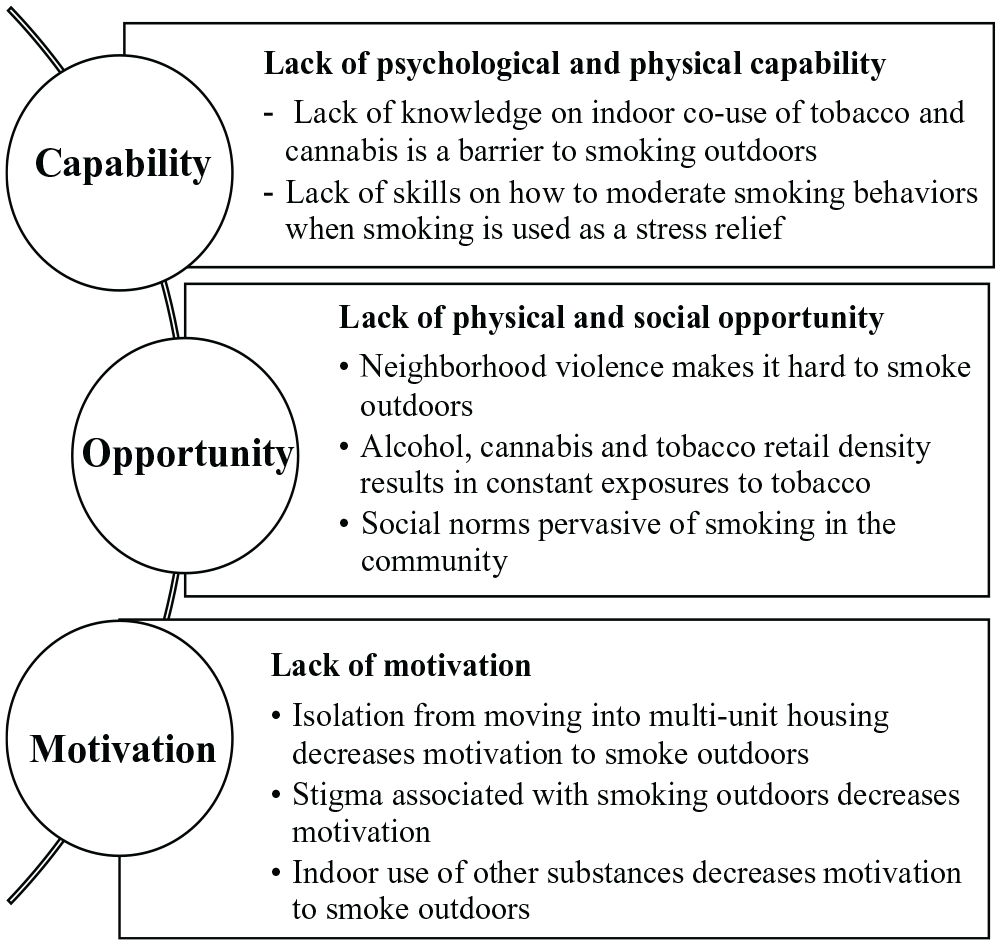
Capability Opportunity Motivation-Behavior (COM-B) Model for Barriers to Smoke-Free Home Adoption in Multi-Unit Subsidized Housing in San Francisco, CA
Quantitative Measures
Residents
Tobacco and nicotine product use
Participants reported whether they had smoked at least 100 cigarettes in their lifetime (i.e., ever smokers); ever smokers reported whether they smoked daily, some days or not at all. We asked participants to report the time it took to smoke their first cigarette after waking, the number of cigarettes smoked on smoking days, and whether they had an intention to quit smoking. Participants reported whether they had made a quit attempt in the past 12 months and whether they used any cessation aids. We asked participants to report past 30-days use of alcohol and cannabis.
Adoption of a smoke-free home
We asked participants who were currently smoking to report whether there were rules around smoking in their home (in my apartment: smoking is allowed anywhere, smoking is allowed in some places or at some times, or smoking is not allowed), and whether they were interested in making their home smoke-free (not interested, thinking about it, decided to make my home smoke-free, and my apartment is already smoke-free). We asked participants to report their level of agreement with statements describing potential barriers to a smoke-free home.
Demographics
Participants self-reported their age, sex assigned at birth (male or female), gender, race/ethnicity, highest level of education, monthly income, and the length of stay in their current residence.
Staff Measures
We asked staff to report their age, sex assigned at birth (male or female) or gender, and race/ethnicity. Staff reported whether they ever smoked, and those who had, reported whether they smoked daily, some days or not at all. We asked participants to report their level of agreement with statements describing their attitudes toward smoke-free policies, attitudes toward smoking cessation programs, and barriers to and facilitators of enforcing a smoke-free policy.
Qualitative Measures
We used the social-ecological model as a framework for the focus groups with residents and in-depth interviews with staff. We asked residents about their personal history of smoking, motivation to quit and barriers to cessation, exposure to SHS, use of cannabis, attitudes toward smoke-free policies, barriers to having smoke-free policies in RAD housing, services for cessation, and neighborhood environment. We asked staff about smoke-free policies on their properties, barriers to implementing and enforcing smoke-free policies, and presence of on-site cessation services.
Neighborhood Assessment of Tobacco Use
We conducted systematic social observations, a method of neighborhood assessment (Sampson & Raudenbush, 1999), where two study staff walked through five randomly selected blocks within a 1000 feet buffer around each housing site to identify environmental cues to smoking (N = 75 blocks, inter-rater agreement 93.8%). Study staff evaluated each block for the following environmental exposures: (a) tobacco (cigarettes butts and/or other tobacco litter, patterns of visible smoking behavior, exposure to pro-tobacco messaging), (b) alcohol (alcohol-related litter or people drinking), (c) substance use (syringes, alcohol bottles), and (d) cannabis (drift from secondhand cannabis smoke). We created a neighborhood assessment score, on a scale of 1 to 4, with higher scores indicating greater neighborhood exposure to alcohol, cannabis, and tobacco.
We mapped alcohol, cannabis, and tobacco outlets within a 1000-feet buffer around each site using ArcGIS online (2022). Our approach of defining neighborhood was based on what could be considered a reasonable walking distance from a participant’s home. Data for licensed tobacco retailers were obtained from San Francisco Public Health Department (San Francisco Department of Public Health, 2022), alcohol outlets downloaded from the Alcohol and Beverage Control (California Department of Alcoholic Beverage Control, 2022), and Cannabis Retailers from the Bureau of Cannabis Control websites (California Department of Cannabis Control, 2022).
Quantitative Data Analysis
We reported sample and tobacco use characteristics for residents and staff using median and interquartile range (IQR) for continuous variables, and chi-square statistic for categorical variables. We categorized responses to attitudes as strongly agree/agree versus strongly disagree/disagree/neither agree nor disagree. We mapped alcohol, cannabis, and tobacco outlets and the neighborhood assessment score around each site.
Qualitative Data Analysis
All interviews were audio-recorded and transcribed verbatim using a professional transcription service. We used ATLAS.ti version 8.1 to facilitate coding. Using directed content analysis (Hsieh & Shannon, 2005), M.V. and M.H.F developed codes to capture domains related to the social-ecological model. Two coders (M.H.F and TK) coded the transcripts, after which coding agreement was reviewed and discrepancies were resolved through consensus. Codes were grouped into broad categories, after which themes and subthemes were identified in an iterative manner. Exemplar quotations were selected to reflect each theme. We used the convergence model of triangulation to identify areas of convergence and divergence in qualitative, quantitative, and neighborhood data (Creswell, 2006; Morgan, 2019).
Results
Resident Characteristics
Of the 134 resident participants, median age was 65 years (IQR: 55–80), 24.6% identified as Asian, 38.1% as non-Hispanic Black, and 11.9% as Hispanic/Latinx (Table 1). Three sites had predominantly Asian residents (Sites 5, 8, and 14), and seven sites had at least half of the participants self-identify as Black/African American (Table 2). Half of the sample had ever smoked, and 57.9% were current smokers (n = 40). Among current smokers, the median number of cigarettes smoked per day was 8.3 (IQR: 2.9–10.1), and 57.5% attempted to quit in the past year (Table 3). Some participants reported past 30-day use of tobacco and cannabis.
Sample Characteristics of Resident Participants in Subsidized Housing (N = 134 Residents)
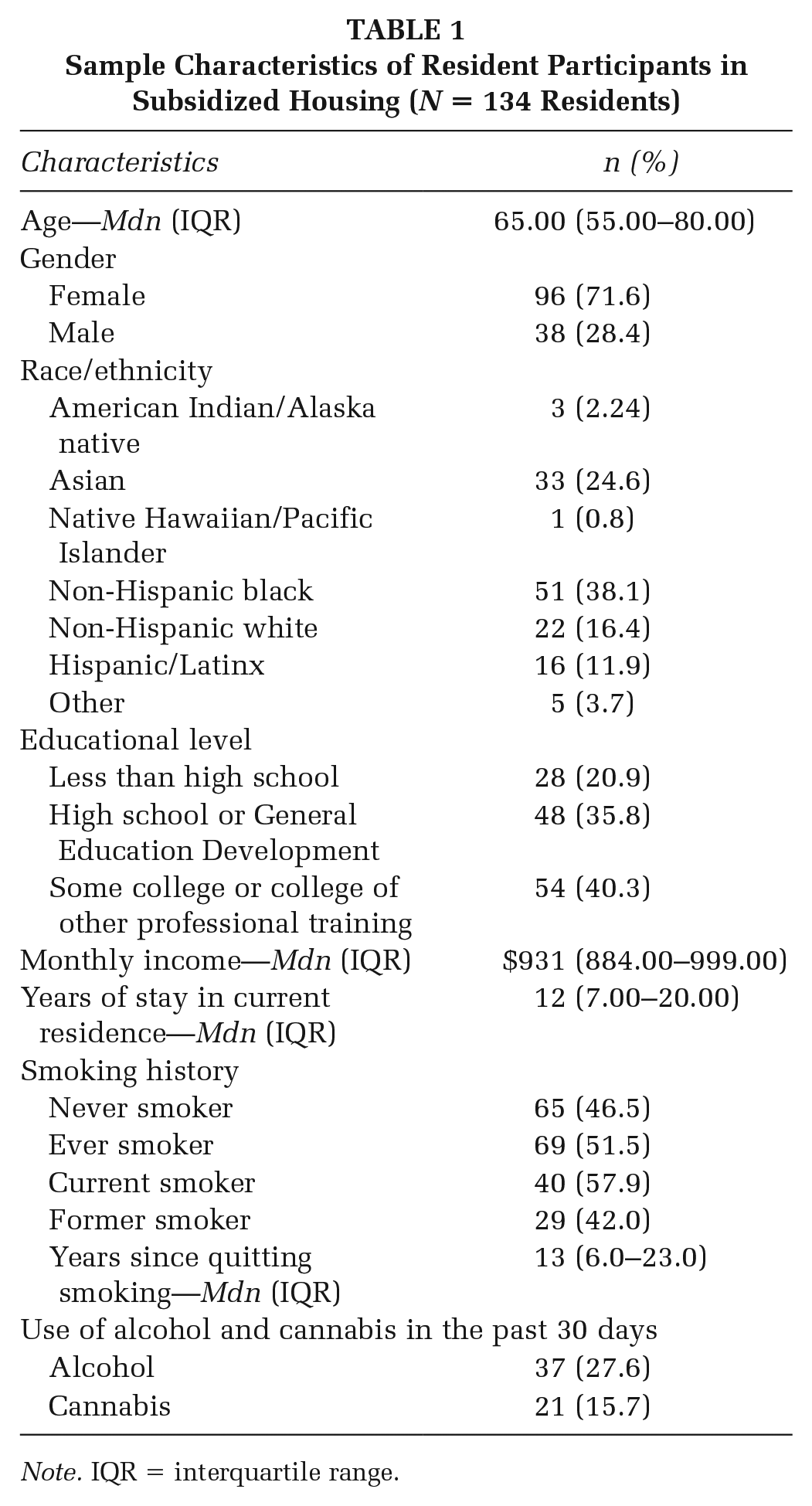
Note. IQR = interquartile range.
Site Characteristics and Neighborhood Assessment Scores
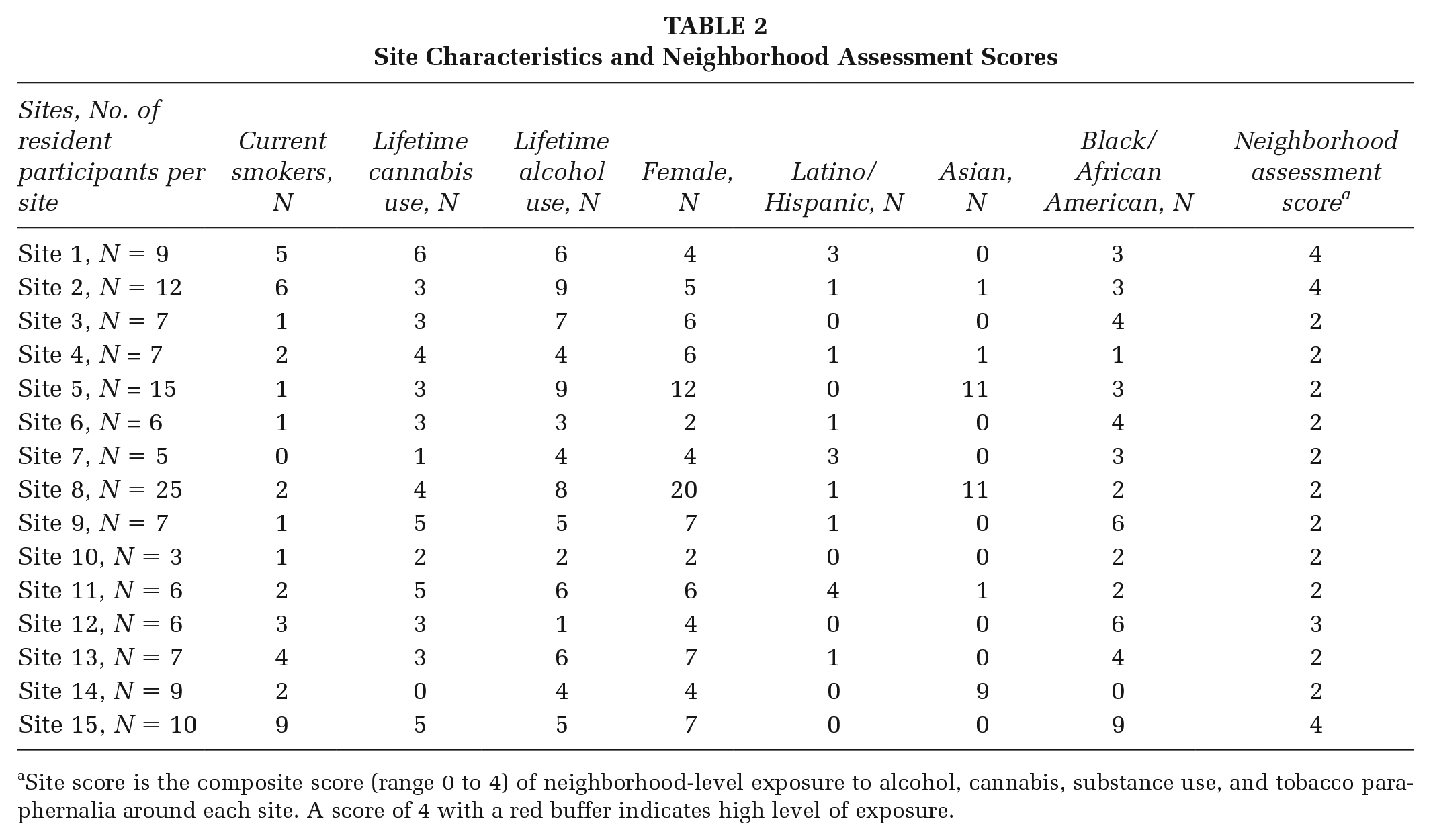
Site score is the composite score (range 0 to 4) of neighborhood-level exposure to alcohol, cannabis, substance use, and tobacco paraphernalia around each site. A score of 4 with a red buffer indicates high level of exposure.
Among those who smoked, 27.5% (n = 11) reported a voluntary no-smoking rule in their home, whereas 42.0% (n = 17) were not interested in making their homes smoke-free. The most common barriers to a smoke-free home were neighborhood safety (45%), having physical disabilities (35%), and bad weather (52.5%).
Staff Characteristics
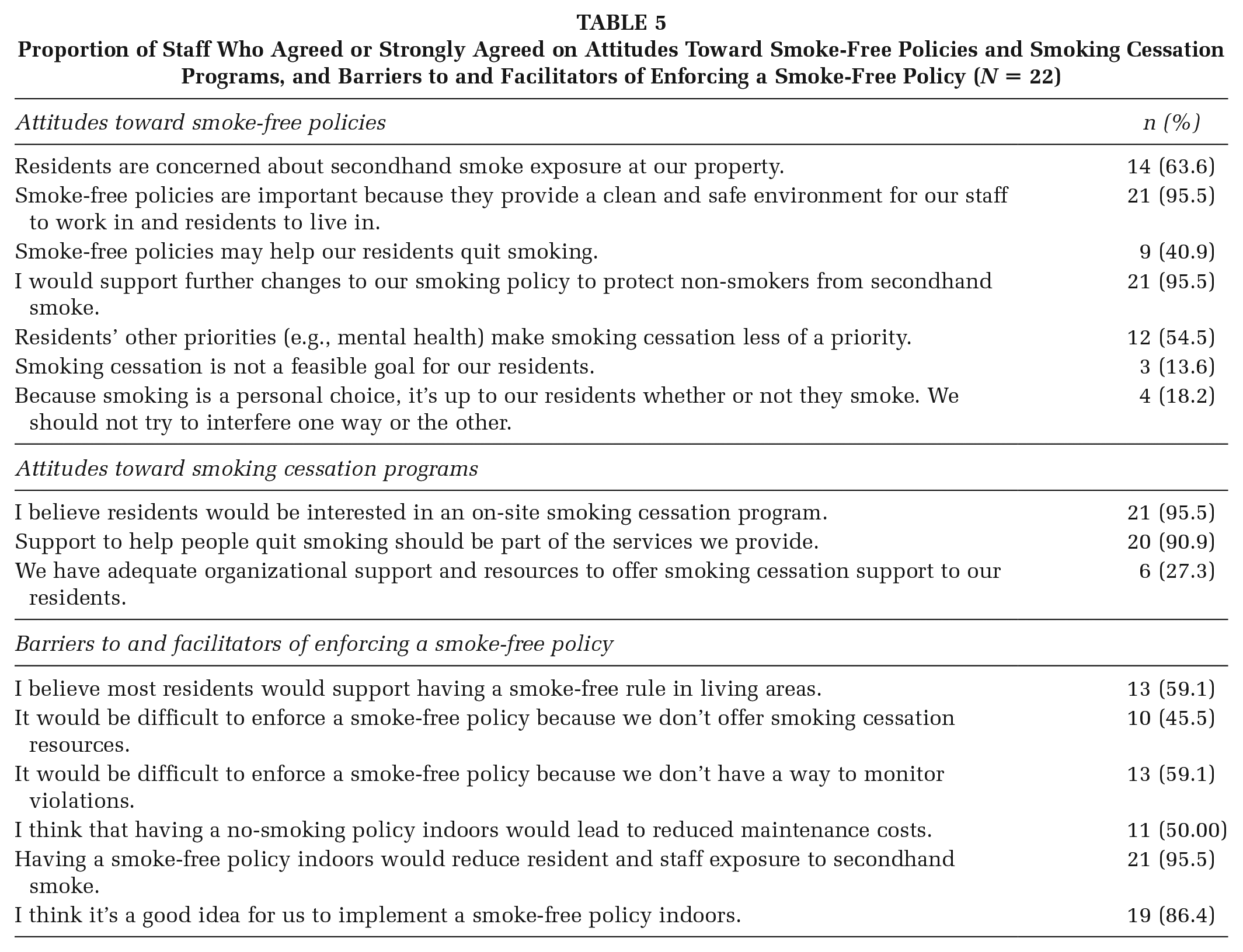
Of the 22 housing staff, the median age was 36 years (IQR: 32–53 years), 77.3% were female, and half were Black/African American (Table 4). Most staff agreed that they would support policies to minimize exposure to tobacco SHS (Table 5). About half the staff agreed that enforcement of smoke-free policies would be challenging because of lack of cessation services and methods to monitor policy violations.
Tobacco Use Characteristics Among Resident Participants Who Reported Current Tobacco Use (N = 40)
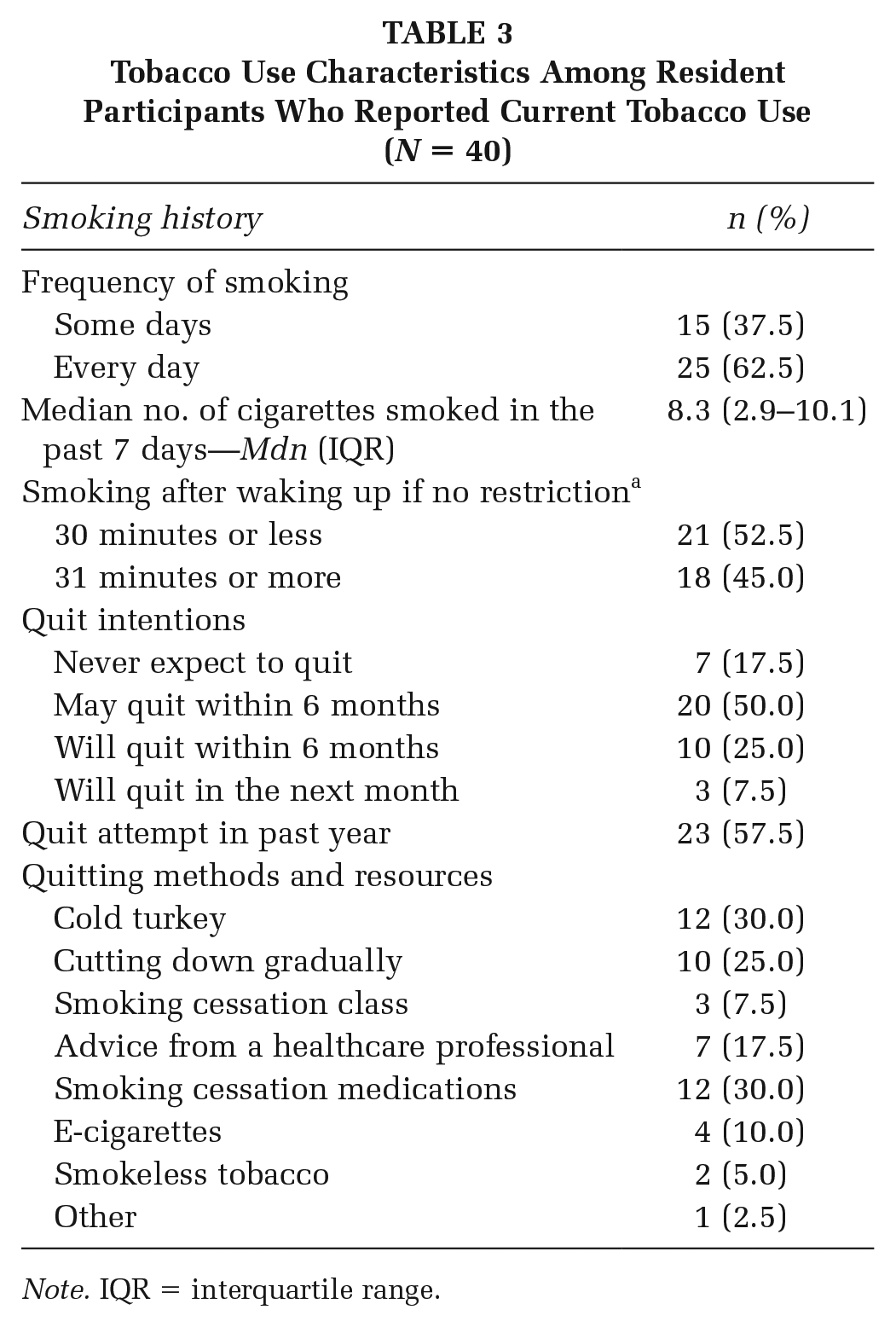
Note. IQR = interquartile range.
Characteristics of Staff Participants (N = 22)
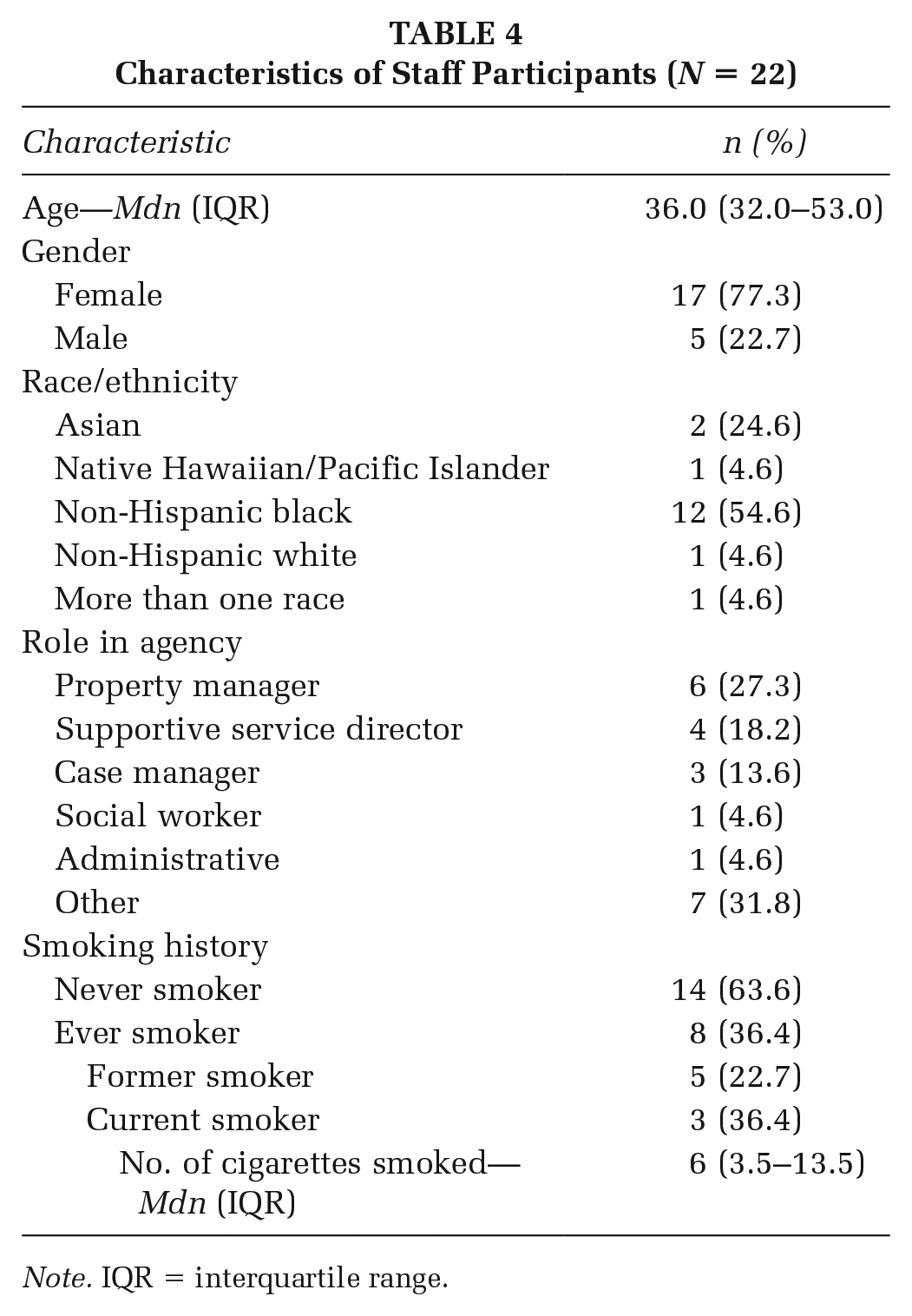
Note. IQR = interquartile range.
Proportion of Staff Who Agreed or Strongly Agreed on Attitudes Toward Smoke-Free Policies and Smoking Cessation Programs, and Barriers to and Facilitators of Enforcing a Smoke-Free Policy (N = 22)
Qualitative Findings
Individual Level
Knowledge and attitudes toward indoor co-use of tobacco, cannabis, and other substances
Residents’ attitudes toward smoke-free policies were influenced by cannabis use. Residents reported that a policy that restricted only tobacco was challenging as indoor cannabis use was common (Figure 1 and Table 6). However, residents who used medical cannabis were concerned that indoor smoke-free policies inclusive of cannabis would restrict their use, which they needed to cope with medical illness.
Select Quotes Representative of Themes and Sub-Themes
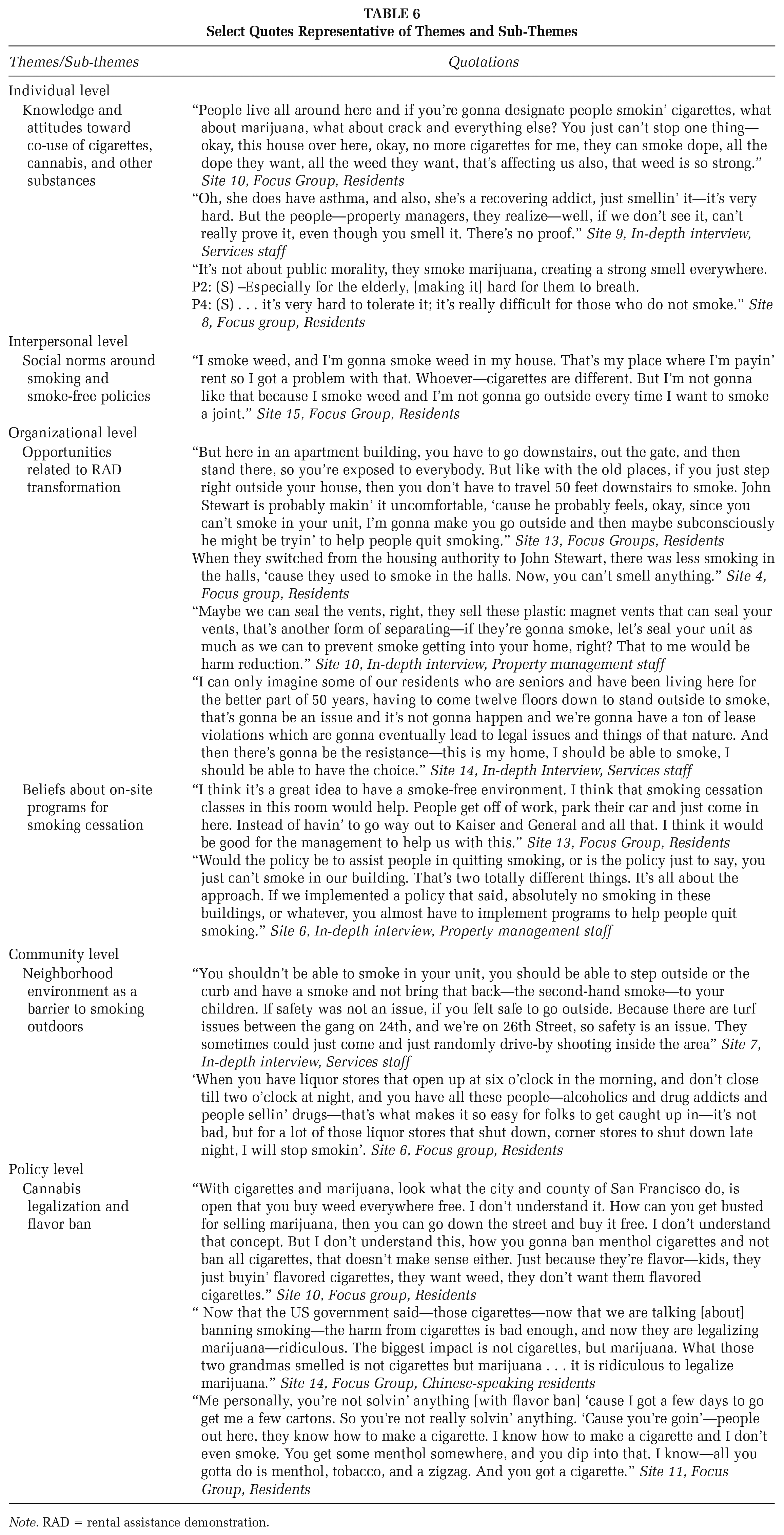
Note. RAD = rental assistance demonstration.
While staff supported a resident’s wish to smoke indoors, they were also sensitive to non-smoking residents’ requests to eliminate SHS exposure. Staff used several mitigating approaches including sealing vents or using air purifiers. Some staff restricted indoor combustible cannabis use, whereas most did not have an explicit cannabis policy. In some buildings, property managers provided lease violations to residents who smoked cannabis indoors despite a no-cannabis policy; however, staff lacked guidance on how to address policy violations and did not support eviction as a repercussion.
Interpersonal Level
Social norms around smoking and smoke-free policies
A few residents who smoked believed that smoke-free policies interfered with their right to smoke. Those residents reported that neither did they have the autonomy to refute a smoke-free policy as it could lead to eviction, nor were they able to afford living in housing without such policies. Non-smoking residents reported lingering exposure to SHS drift from cannabis or tobacco. In some buildings, non-smoking residents expressed fear of speaking out about indoor smoking because of retaliation from their neighbors. In one extreme instance, an elderly participant’s wife who reported her neighbor for smoking in the hallway was assaulted by her neighbor, which led to the property evicting her neighbor for violence.
Most staff acknowledged high rates of smoking among residents, except in buildings for elderly residents where smoking was less prevalent. Rent evasion was the primary reason for termination of lease, and the most common reasons for rent evasion were death of a spouse, loss of section 8 housing with a fixed income, or other financial stressors. In the face of competing priorities that threatened housing, addressing tobacco use was less of priority.
Organizational Level
Opportunities related to RAD transformation of public housing
For most residents, RAD transformation—the conversion of older public housing buildings to newer mixed income housing—led to improved ventilation between units, minimizing exposure to SHS. Paradoxically, this offered less motivation to some individuals to smoke outdoors. While RAD transformation offered properties the opportunity to follow HUD’s smoke-free policy, some properties deferred adoption. In some buildings, residents could choose between smoking and non-smoking rooms. Participants who lived in barrack-style housing (i.e., row housing) and who moved to RAD-transformed multi-unit housing felt stigmatized when they smoked in front of their buildings, opting to smoke indoors. The barrack-style housing offered more opportunities to socialize than multi-unit housing, and the increased isolation from moving to multi-unit housing contributed to people smoking indoors.
On-site programs for smoking cessation
A few residents reported that smoking was an addiction that required a treatment program, and that public housing was not a venue for treatment programs. Others felt that a smoke-free environment with on-site cessation services, with a peer group, would motivate quitting behaviors. However, several residents believed that quitting and/or desire to change personal behaviors around substance use were dependent on one’s own “will power.”
Some services staff believed that if cessation groups were accompanied with RAD transformation and a clause in residents’ leases to not smoke in their units, there might be interest. Another staff agreed that on-site cessation classes would be beneficial, particularly if it was multi-generational, and allowed for children, parents, and grandparents to participate.
Community
Neighborhood environment as a barrier to smoking outdoors
Residents reported that even if they wanted to smoke outdoors, there were no safe designated smoking zones. Neighborhood violence, including violence from firearms, was a common reason to not smoke outdoors in some neighborhoods. Similarly, staff raised concerns about neighborhood violence as one of the barriers to implementing an indoor no-smoking rule. For instance, in neighborhoods that had high rates of crime, the lack of an outdoor designated smoking zone away from the main street forced people to smoke on the curb, which put them at risk for “drive-by shootings.”
Policy
Cannabis legalization and flavor ban
Participants had mixed views on the legalization of cannabis, and discussed the double standard of local policies legalizing cannabis and federal policies criminalizing individuals who sold cannabis. While some participants believed that the flavor ban that went into effect in San Francisco, CA, would discourage use of menthol and other flavored tobacco, others felt that people would make their own products or buy it from another county or online.
Neighborhood Assessments
All sites had evidence of tobacco- or alcohol-related litter and/or people gathering outside housing to smoke or drink (Figure 3 and Table 2). Sites located in more densely populated areas had a higher density of alcohol outlets, cannabis dispensaries, and tobacco retailers; some of these sites also had more evidence of cannabis and drug use evidenced by a higher neighborhood assessment score (Figure 4). Sites 14 and 8 had lower neighborhood assessment scores, potentially reflecting the older, non-smoking resident demographics of those sites. In contrast, Site 15, a site that had not gone through RAD transformation had fewer alcohol outlets, cannabis dispensaries, and tobacco retailers in the surrounding neighborhood; paradoxically, this site had a high site score reflecting a high prevalence of cannabis, drug, and other environmental cues to tobacco use (Figure 5).
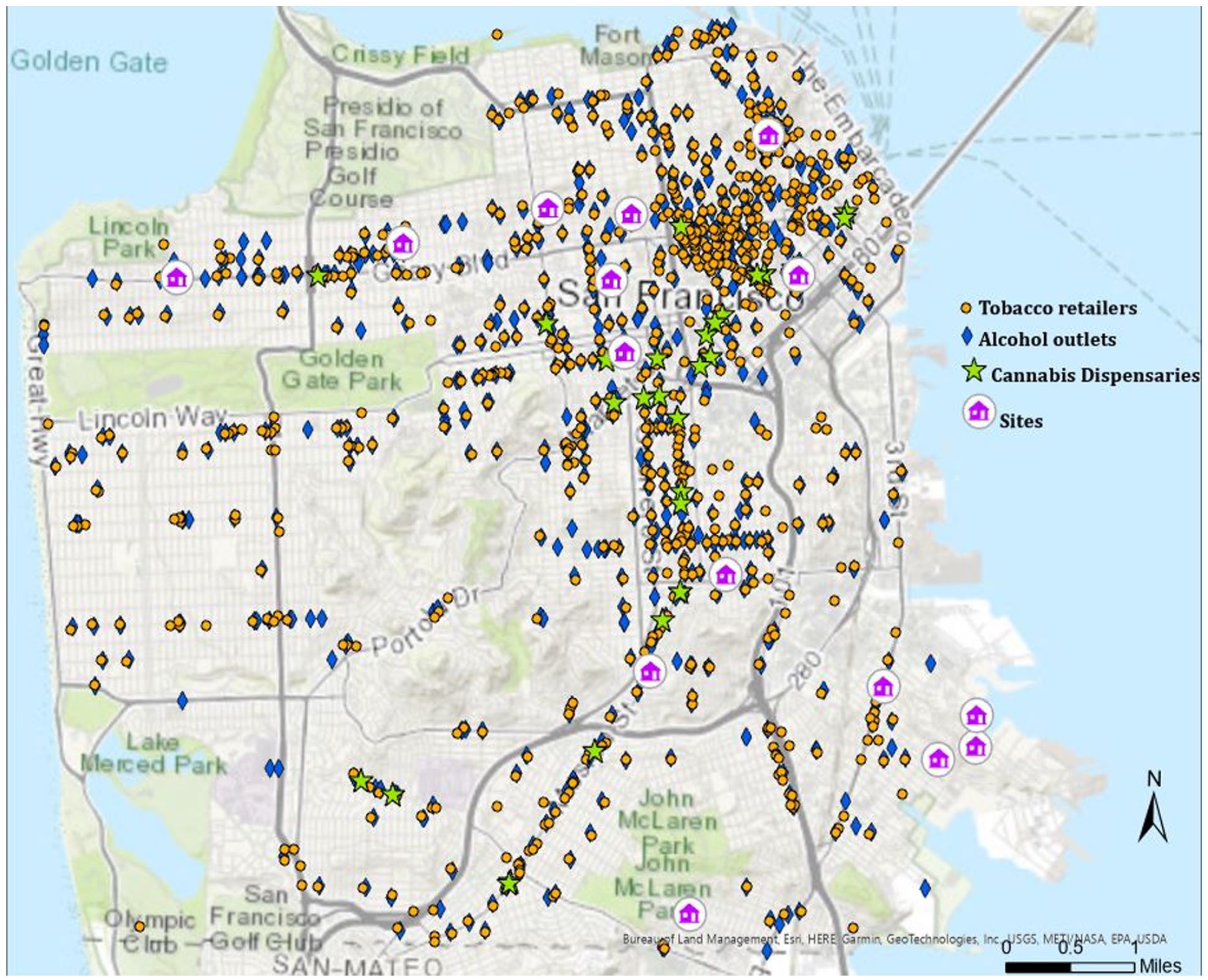
Map of All Housing Sites With Neighboring Alcohol Outlets, Cannabis Dispensaries, and Tobacco Retailers Around Each Site (N = 15 Sites)
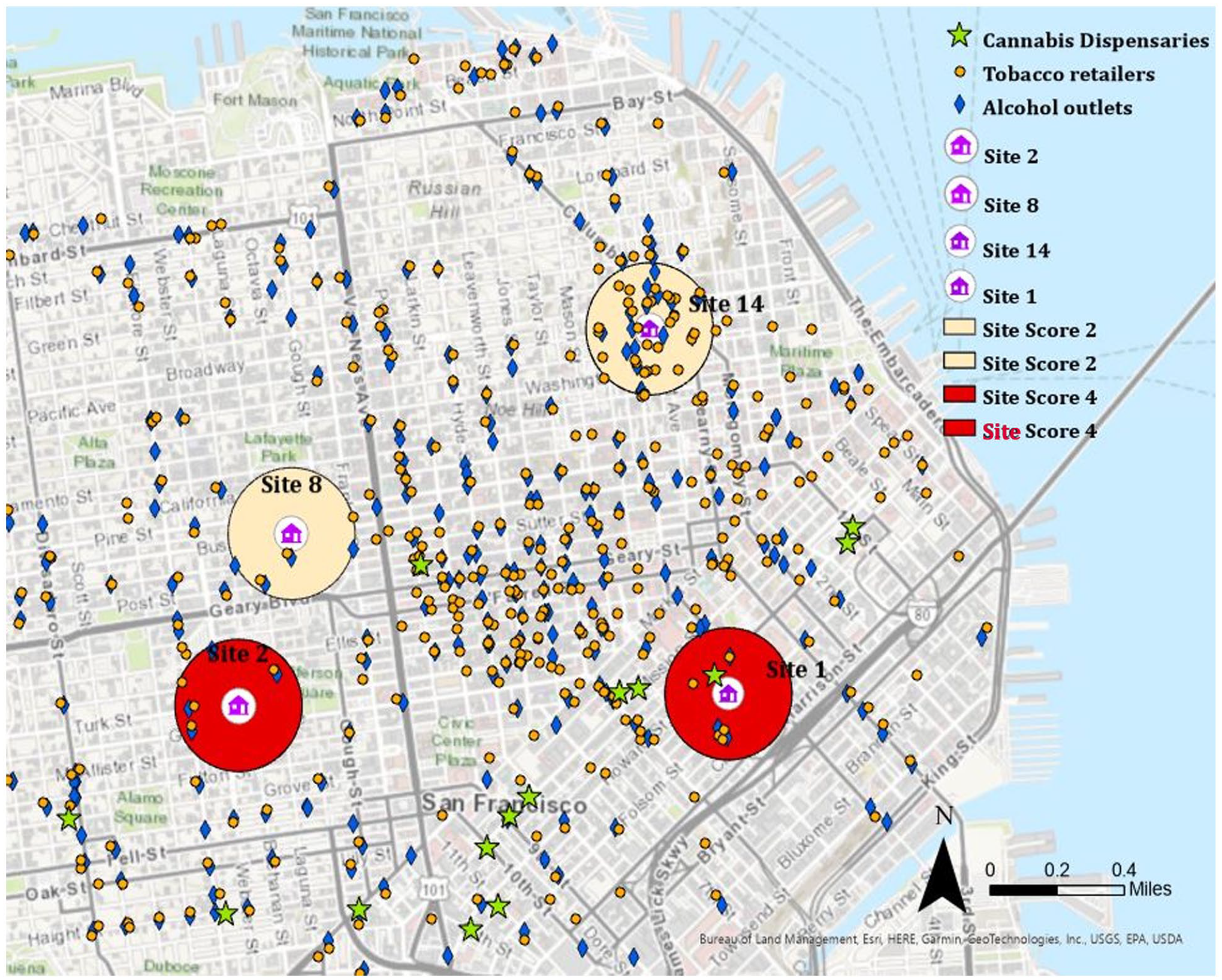
Map of Alcohol Outlets, Cannabis Dispensaries, and Tobacco Retailers Around Site 1, Site 2, Site 8, and Site 14a
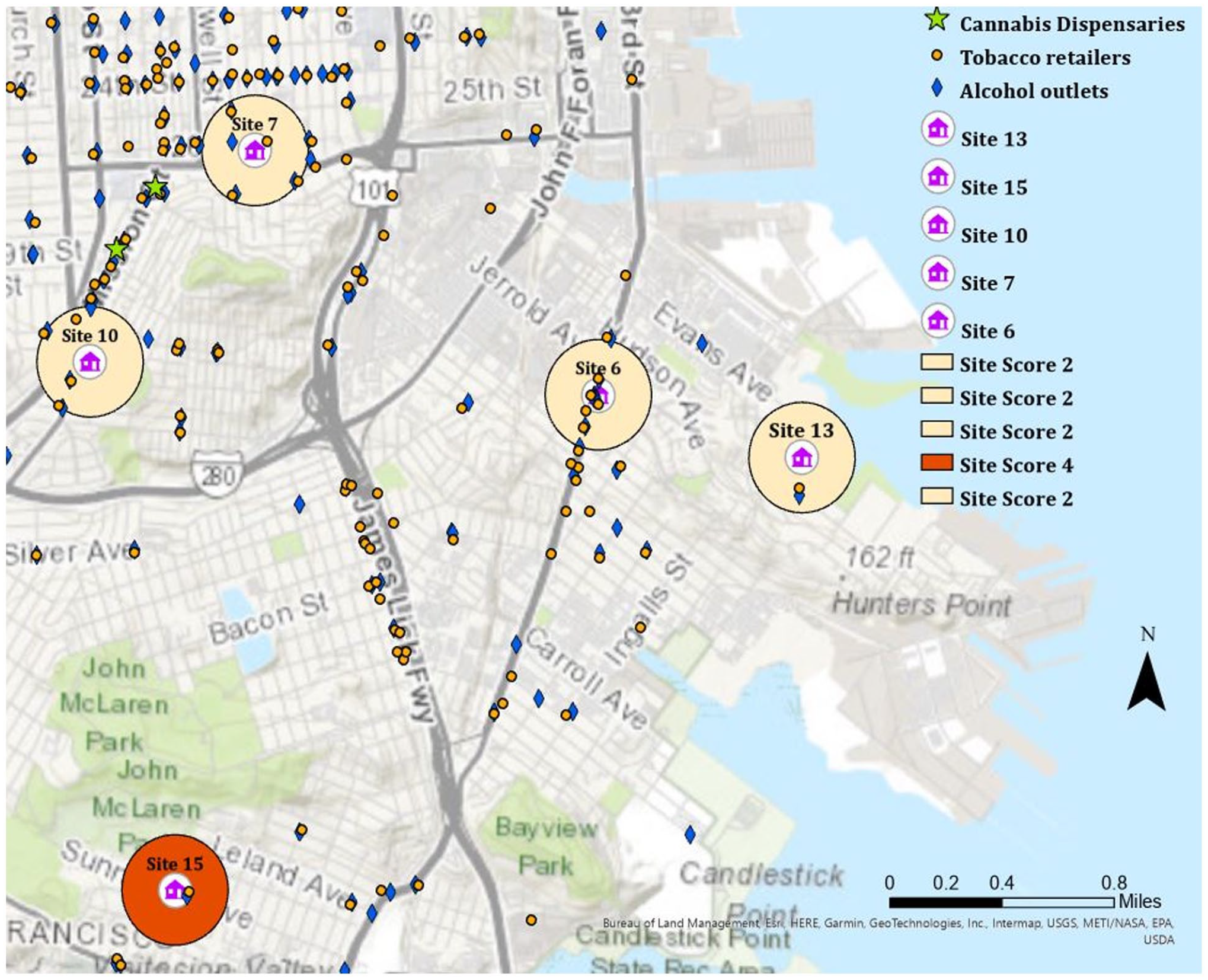
Map of Alcohol Outlets, Cannabis Dispensaries, and Tobacco Retailers Around Site 13, Site 15, Site 7, Site 6, and Site 10a
There was convergence between residents’ reports on neighborhood violence, exposure to tobacco retailers, and audits of those neighborhoods. Residents living in sites that had a high density of alcohol, cannabis and tobacco retailers such as Site 7 reported a high prevalence of neighborhood violence (Figure 5). Residents living in less densely populated locations (e.g., Sites 13 and 15) also reported high levels of neighborhood violence (Figure 5). Neighborhood violence was one of the primary reasons for smoking indoors. Sites 13 and 15 were located in less urban areas with lower density of alcohol outlets, cannabis dispensaries or tobacco retailers relative to other sites; however, participants reported a higher proportion of youth cannabis use in these properties. About half of the participants in those sites reported a lifetime prevalence of cannabis use (Table 2), and they also reported a preference to smoke cannabis indoors, contributing to high levels of secondhand cannabis exposure in these properties.
Mapping Barriers to and Facilitators of Smoke-Free Home Adoption to the Capability, Motivation, Behavior (COM-B) Model
Residents’ lack of knowledge on the harms of indoor co-use of tobacco and cannabis reduced their psychological capability and motivation to adopt a smoke-free home (Figure 2). Residents lacked physical capability to moderate their smoking behaviors indoors, particularly when smoking was used to cope with stressors. Lack of safe neighborhoods and designated smoking zones in areas free from street violence limited physical opportunity to smoke outdoors. Residents with disabilities needed physical accommodations to promote outdoor smoking (e.g., living in a unit close to a building exit). Physical opportunity was also limited by the high density of alcohol, cannabis, and tobacco retail environment, which increased exposure to tobacco use. However, improvements in ventilation in housing were an enabler of physical opportunity. For some residents moving into multi-unit housing decreased their motivation to adopt a smoke-free home because they felt stigmatized when they smoked outdoors and the isolation of living in multi-unit housing triggered indoor smoking. Yet for people anticipating transformation of their properties, the prospect of coming back to a newly refurbished home was appealing and a motivator for smoking cessation.
Discussion
In this mixed methods study, we found that most residents and staff supported smoke-free policies that restricted tobacco use, but there were mixed views on policies restricting indoor cannabis use. Neighborhood violence and lack of safe outdoor designated smoking zones were barriers to an indoor smoke-free lifestyle. Commercial determinants including the density of alcohol, cannabis, and tobacco retailers and exposure to environmental cues to smoking around sites influenced resident’s views of adopting smoke-free homes.
While only 15% of study participants reported past 30-days use of cannabis, most participants reported exposure to secondhand cannabis smoke from a neighboring unit. In a study of residents in New York City subsidized housing, two-thirds reported drift from secondhand cannabis smoke, and most residents perceived that smoking cannabis and exposure to secondhand cannabis smoke was harmful (Anastasiou et al., 2020). In another study of parents of young children attending a pediatric practice in New York city, a third reported exposure to secondhand cannabis smoke, and participants who were non-Hispanic Black or Hispanic/Latinx reported smelling secondhand cannabis smoke more than their white counterparts (Sangmo et al., 2021). Cannabis smoke is not included in the HUD smoke-free policy because cannabis is illegal under federal law (U.S. Department of Housing and Urban Development, 2016). However, the legalization of recreational cannabis in some states has posed challenges for smoke-free policy implementation in multi-unit housing, potentially reducing the impact of existing policies on SHS exposure (Thorpe et al., 2020). Legalization of cannabis may encourage some people to smoke cannabis indoors, which may conflict with an indoor smoke-free policy (Thorpe et al., 2020). Housing providers have established consequences for smoke-free policy violations such as verbal or written warnings to encourage people to comply with smoke-free policies, without having to resort to extreme consequences like eviction for populations that have faced substantial housing challenges (U.S. Department of Housing and Urban Development Office of Healthy Homes and Lead Hazard Control, 2014). These repercussions may also be inclusive of cannabis use indoors to mitigate the harmful effects of SHS cannabis exposure. The high prevalence of exposure to cannabis smoke in multi-unit housing highlight a need for comprehensive smoke-free homes, inclusive of cannabis, as part of a wider healthy-homes policy agenda. Education and awareness-building on the harmful effects of co-use of tobacco and cannabis could address some of these barriers to smoke-free home adoption in multi-unit housing.
The socio-ecological model and COM-B framework helped identify a tension between participants’ desire for smoke-free living and environmental and commercial determinants of tobacco use behaviors. Participants living in more densely populated locales with a high density of alcohol, cannabis and tobacco retailers reported high levels of exposure to these products and neighborhood violence (e.g., shootings or assaults), as did participants living in some of the less densely populated sites. About half of our study sample reported that neighborhood violence and lack of safe outdoor designated smoking zones were some of the major barriers to adopting a smoke-free home. These findings are consistent with studies that have shown an association between neighborhood built environment and physical activity. Perceptions of neighborhood safety and some forms of community violence, such as witnessing an assault in one’s neighborhood, is associated with less physical activity (Ou et al., 2016). Our study highlights the importance of considering the neighborhood built environment as an important physical and social opportunity to promote smoke-free policies in multi-unit housing. To encourage adoption of smoke-free homes, properties need to have safe outdoor designated smoking zones, away from the streets where people may be vulnerable to violence. Given the high concentration of alcohol, cannabis, and tobacco retailers in low-income communities where subsidized housing are located, our study highlights the need for residential zoning of these retailers to reduce widespread exposure to these products (Siegel et al., 2021).
Residents and staff described RAD transformation, that is, the refurbishing of former public housing into newer subsidized housing properties, as an opportunity to transition to smoke-free living. Residents liked the prospect of returning to a new apartment without evidence of smoke residue. However, improved ventilation between units, paradoxically was a deterrent for some participants to smoke outdoors. Findings highlight the need for education campaigns, like the Tips from Former Smokers’ Campaign launched by the Centers for Disease Control and Prevention to educate the public on the hazards of tobacco and SHS exposure (Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, 2022). The barrack-style housing offered more opportunities to socialize and smoke outdoors, normalizing smoking behaviors. Paradoxically, multi-unit housing offered fewer opportunities to socialize, and the isolation and stigma associated with smoking outdoors led some participants to smoke indoors. Although the transition to RAD housing offered an opportunity for properties to voluntarily adopt smoke-free policies, the policy’s impact could be increased by community engagement and voluntary buy-in among residents for the policy (U.S. Department of Housing and Urban Development, Office of Healthy Homes and Lead Hazard Control, 2014). These strategies could mitigate feelings of isolation and de-normalize indoor smoking, which may increase motivation to adopt a smoke-free home.
There were mixed opinions on whether housing could be a venue for smoking cessation treatment. One of the barriers to successful implementation of smoke-free policies in public housing has been the lack of concerted efforts to link residents to smoking cessation services (Thorpe et al., 2020). Findings from our study suggest that if properties are going smoke-free, they could consider providing access to cessation services (either on-site or through referrals) to increase motivation to quit with a policy. Integrating policy implementation with cessation services may capitalize on the momentum of a policy to motivate tobacco cessation behaviors.
Limitations
Our study had several limitations. We conducted the study in 15 properties in one Bay Area County; therefore, findings are not generalizable to subsidized housing in other counties regionally and nationally. Tobacco and cannabis use behaviors are self-reported and are subject to recall bias. Environmental cues to tobacco use, particularly those that were determined by systematic social observations of properties, are cross-sectional and may change over time.
Implications for Practice or Policy
Smoke-free policies are critical to protecting people from SHS exposure. Understanding local policy influencers of cannabis and tobacco use will be critical to developing policies restricting the use of these products in multi-unit housing. To increase the implementation and impact of these policies on tobacco and cannabis use behaviors, policies need to address indoor use of cannabis, the built environment including neighborhood safety, and commercial environmental including alcohol, cannabis, and tobacco retail density in low-income communities. Incentivizing policy adherence by increasing access or facilitating referrals to tobacco and cannabis cessation resources may capitalize on the policy momentum for behavior change. Multi-level interventions that integrate comprehensive smoke-free policies with cessation services, and urban planning to reduce environmental and commercial influences of tobacco use will be critical to supporting healthy homes and neighborhoods.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.