
Abstract
Background. Behavior change has been a critical factor in slowing the spread of COVID-19. In South Africa where infection rates are high, research is needed on the protective behaviors adopted by youth who have low infection rates but are carriers of the virus. Aims. The purpose of this study is to (1) identify the protective behaviors young people adopted during the pandemic and (2) to estimate the probability of positive behavior change by demographic and socioeconomic characteristics. Methods. The study uses data from the South African National Income Dynamics—Coronavirus Rapid Mobile Survey 2020. The sample includes 985 (n) youth aged 15–24 years. The outcome of interest is behavior change due to the Coronavirus. Cross-tabulations and an adjusted binary logistic regression model showing odds ratios, are fit to the data. Results. Not all youth adopted protective behaviors. The most prevalent behaviors adopted include washing hands (67.75%) and staying at home (54.02%). Youth in households with six or more members are more likely to change their behaviors (ORs = 1.67 and 1.64, both p-values < .05). However, youth who do not have access to water to wash hands (OR = 0.71), reside in households with food insecurity (OR = 0.94), and those living in nonformal housing (OR = 0.69) are less likely to adopt behavior change. Conclusion. Due to the socioeconomic inequalities associated with behavior change, there is need for more tailored approaches to address youth living in impoverished households in the country.
COVID-19 continues to affect the health and well-being of the global population. In South Africa, where health care services have been under severe strain, the government and civil society have stressed the importance of behavior change to curb the spread of the disease (Jassat et al., 2021). Since the start of the pandemic, the public has been encouraged to wear masks, social distance, and frequently wash hands with soap among other behavior change recommendations (Hatefi et al., 2020).
However, behavior change under nonpandemic circumstances can be slow and at times disrupted by misinformation and socioeconomic constraints (Armitage, 2015; Kelly & Barker, 2016; Peters et al., 2015). Studies show that nonpandemic protective health behaviors have been slow to change, especially in less developed countries, because of the associated monetary costs, such as the adoption of healthier diets to prevent malnutrition and associated diseases (Govender et al., 2011; Jankielsohn, 2015; Mutyambizi et al., 2018). This is particularly true among young people who struggle to adopt and maintain safe behaviors (Breinbauer, 2005). For youth (and others) during this pandemic, monetary costs for personal protective equipment (PPE), have been incurred by the public, despite the limited government support offered (Sefah et al., 2021). These costs include the purchasing of face masks, hand sanitizer, and other disinfectants needed to clean surfaces regularly.
In addition, there are behaviors, such as social distancing, which are difficult for young people who reside in areas of high population density and crowded households (Jeffrey et al., 2020; Rocklöv & Sjödin, 2020). Research has shown that young people are less likely to get seriously ill from COVID-19, but are carriers (Efuribe et al., 2020). Knowing this could influence the perceived risk among young people and competing interests, including employment, education, and social engagements, might result in youth not being able to change their behaviors to earn an income, gain education, or be able to see friends and care for family members. However, the importance of adopting protecting behaviors to reduce transmission of the virus cannot be understated and identifying the factors supporting or limiting behavior change remains necessary.
Given the complexity of behavior change and its relationship to social and economic conditions, this study utilizes the Social Determinants of Health framework which wherein living, social, and economic conditions are key determinants for health outcomes (World Health Organization, 2010). For this study, the framework is used to understand the health behavior outcomes of youth in South Africa. Therefore, the purpose of this study is to (1) identify the main protective behaviors young people adopted during the early months of the pandemic and (2) estimate the probability of positive behavior change by demographic and socioeconomic characteristics of youth in South Africa. This research will inform national policies and programs aimed at further reductions of transmissions through behavior change. The results could also inform the health promotion practice interventions of other developing countries.
Method
Data
This study uses data from the National Income Dynamics Study—Coronavirus Rapid Mobile Survey 2020 (NIDS-CRAM). The study investigates the socioeconomic impacts of the national lockdown associated with the State of Disaster declared in South Africa at the start of 2020 (March 2020). The survey further investigates the social and economic consequences of the global Coronavirus pandemic in the country. NIDS-CRAM forms part of a broader study called the Coronavirus Rapid Mobile Survey (CRAM) which aims to inform policy using rapid reliable research on income, employment, and welfare in South Africa, in the context of the global Coronavirus pandemic. For this study, variables were selected based on the Social Determinants of Health framework which demonstrates an emphasis on demographic, household, and socioeconomic factors associated with behavior change. The data for this study come from the first wave of data collection which ran from May to June 2020 (Spaull et al., 2020). The data are made freely available for research purposes at https://www.datafirst.uct.ac.za/dataportal/index.php/catalog/817.
Sample Size
The sample for this study includes 985 (n) youth aged 15–24 years who participated in the study. Of these youth, 896 (90.96%) had responded positively (yes) to the question “Have you changed your behavior since learning about the Coronavirus?”
Study Variables
The outcome of interest in this study is behavior change due to the Coronavirus. Specifically, participants were asked two questions. First, “have you changed your behavior since learning about the Coronavirus?” to which respondents answered “yes,” “no,” or refused. Those who refused were excluded from the analysis. The second question is as follows: “In what ways have you changed your behavior?” For this question, respondents were asked to indicate, from a list of 12 behaviors, any that they had adopted due to the Coronavirus. In this study, the protective behaviors that have been recommended by the World Health Organization (WHO) are estimated, and include social distancing, wearing a face mask when around other people, washing hands regularly, coughing and sneezing into elbow, and cleaning or disinfecting surfaces frequently (WHO, 2022). “Staying at home more” was asked but was also a regulated activity enforced by the government during lockdown. For this reason, it is not included in the probability of behavior change analysis.
The control variables selected for this study are respondents’ demographic and socioeconomic characteristics. These include gender (man or woman), race/population group (African/Black, White, Colored, Indian/Asian, or Other), highest level of education (Primary, Secondary, or Tertiary), access to water to wash hands (yes or no), receiving a grant from government (yes or no), 1 household lost main source of income since hard lockdown (yes or no), household ran out of money for food in April 2020 (yes or no), and type of dwelling (house/flat; traditional house, like a mud hut; informal house, like a shack). 2
Analysis Plan
Descriptive and inferential statistics are used in this study. For descriptive purposes, cross-tabulations showing the percentages of youth behavior change and type of protective behaviors adopted by respondents’ characteristics are calculated. The behaviors are also ranked to estimate the most (1) and least (9) adopted behaviors among young people. For the inferential statistics, a Hosmer–Lemeshow test was run to determine the goodness of fit for the binary logistic regression model, showing odds ratios, fit to the data to estimate the probability that youth will adopt positive behavior change by demographic and socioeconomic characteristics. All data analysis was done using STATA 15 and statistical significance is determined through p values less than .05.
Results
More young women (54.75%) have changed behaviors than young men (42.25%) in the sample (Figure 1). Among the young people who did not change their behaviors (No), there were also more women (64.04%) than men (35.96%) whose behaviors did not change.
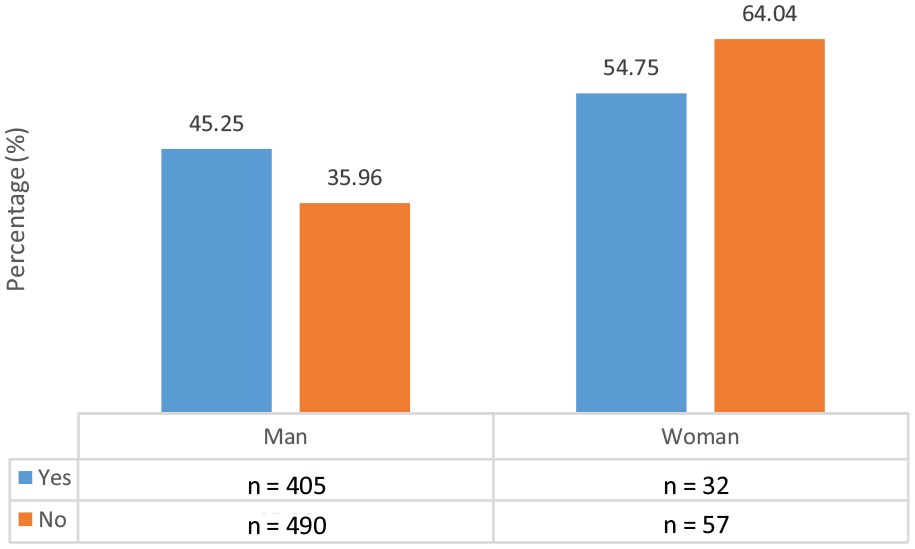
COVID-19 Behavior Change (Yes or No) by Gender of Youth in South Africa (p < .05)
Table 1 shows the behavior change status by characteristics of youth in the sample. In total, 90.96% of youth had changed their behavior. However, by certain characteristics, more than 10% of the youth had not changed their behaviors. In particular, 10.42% of women, 12.9% of Colored and 16% of White, and 10.53% of those with primary education did not change their behaviors. In addition, households with six or more members, those without water to wash their hands (10.87%) and youth living in a traditional house (11.81%) were not able to change their behaviors.
Frequency (n) and Percentage (%) Distribution of Behavior Change Status by Characteristics of the Youth (18–24 Years Old) Respondents in South Africa, 2020
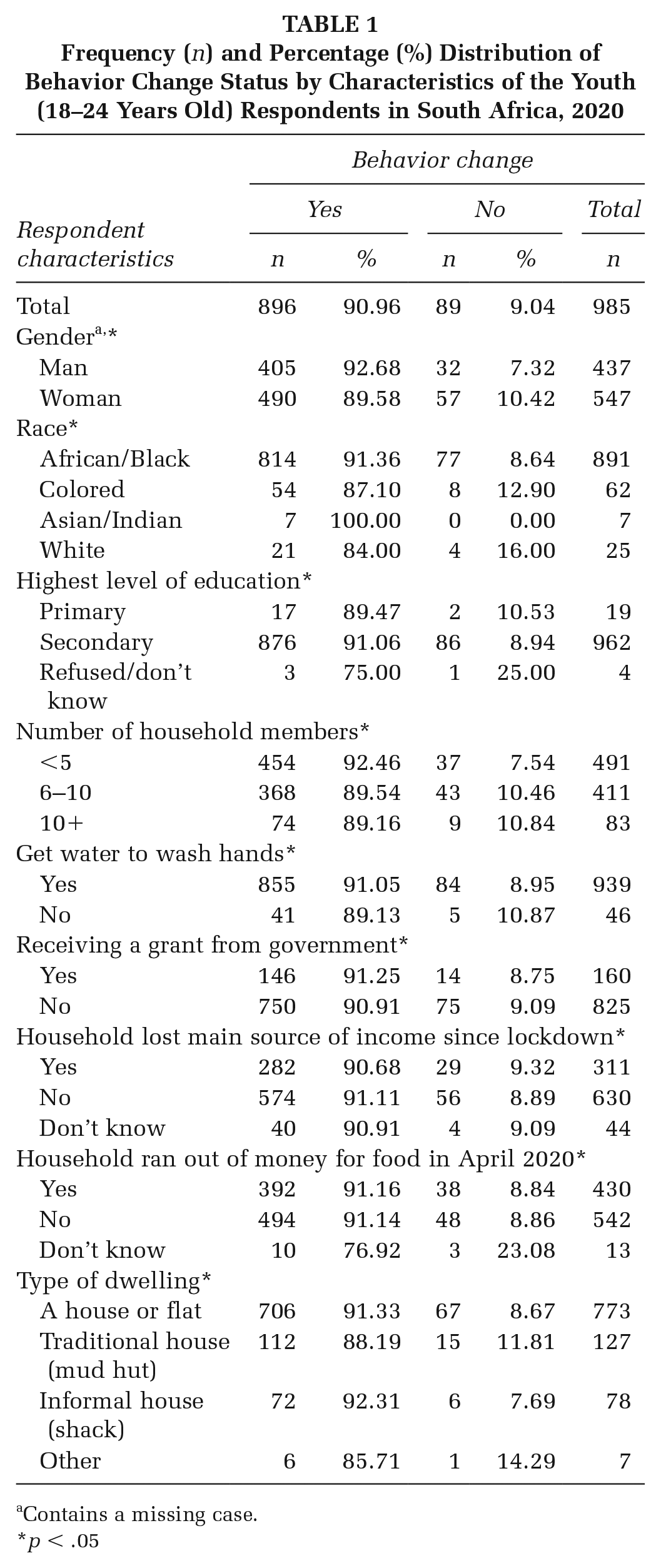
Contains a missing case.
p < .05
The percentage distribution of behaviors adopted by youth shows that most youth washed hands more (67.75%) and stayed at home (54.02%; Figure 2). A further 48.21% reported wearing a mask, 17.75% avoided close contact with others (hugging, kisses, etc.) and 15.63% avoid big groups. Less than 10% of the respondents use sanitizer (9.26%), clean and disinfect surfaces regularly (3.13%), social distance (1.07%), and cough/sneeze into elbows (0.56%).
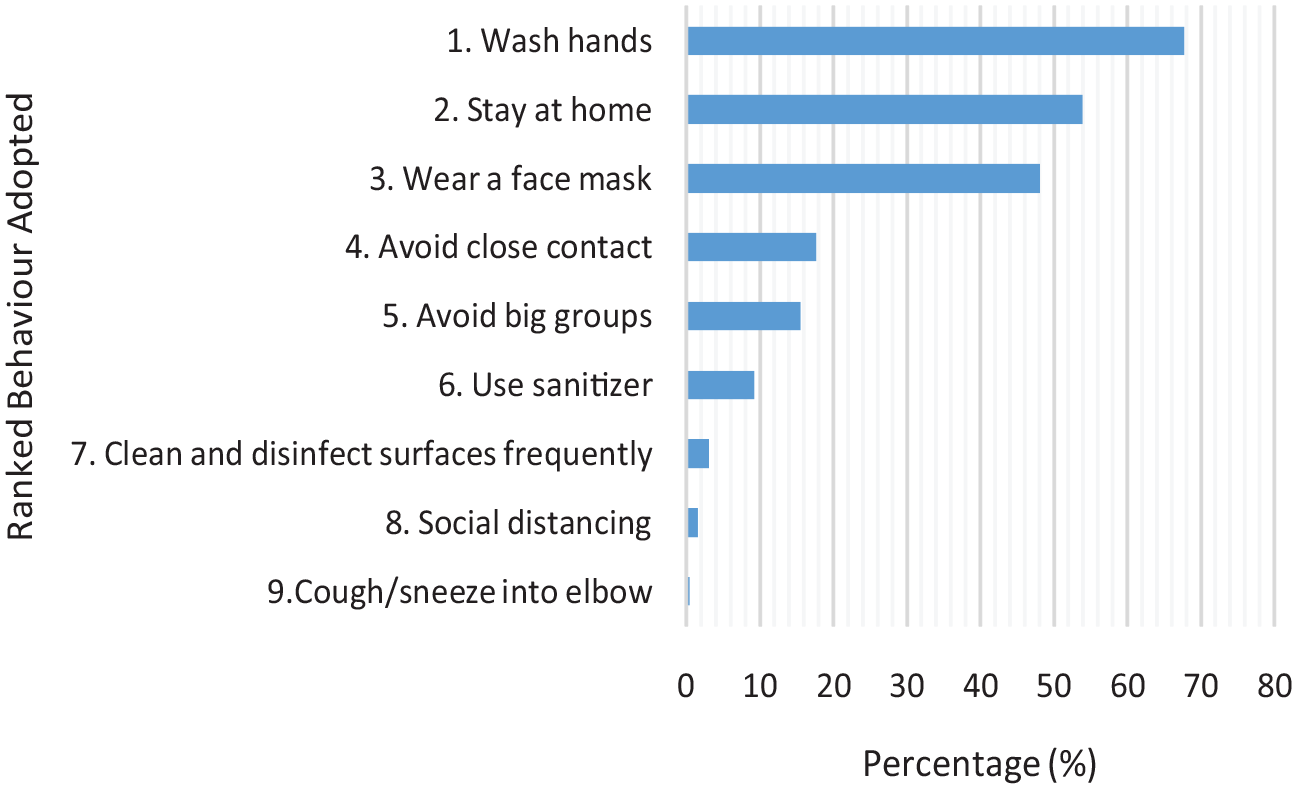
Percentage Distribution of Behaviors Adopted by Youth (18–24 Years Old), South Africa
Figure 3 shows the percentage distribution of behaviors adopted by number of household members (<5, 6–10, or 11+) of the respondents. The graph shows that there are more protective behaviors adopted in percentages when there are five or fewer household members. Furthermore, only 26.16% of youth were able to avoid close contact in households with 6–10 members and only 7.14% in households with 11 or more members. Similarly, in households with 11 or more members, only 2.50% of youth were able to wear a face mask.
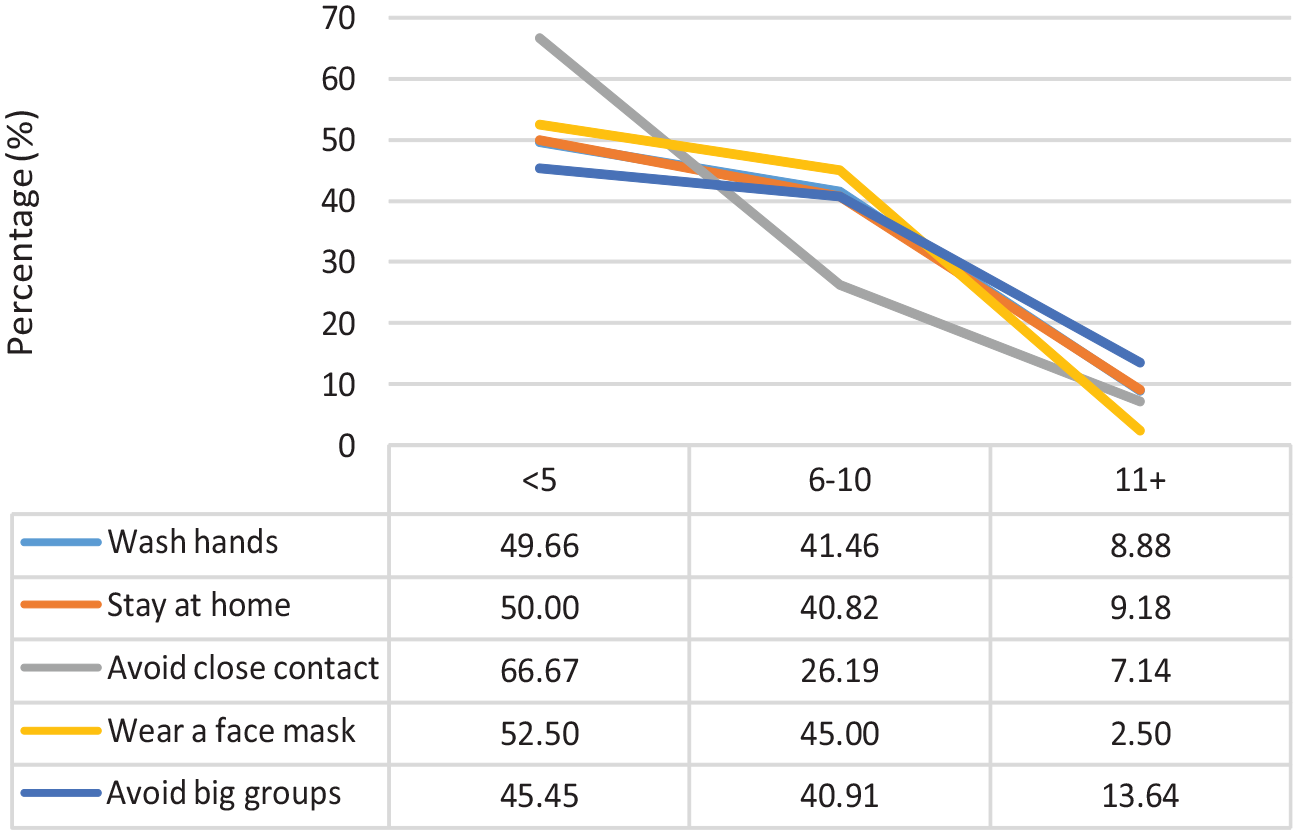
Percentage Distribution of Behaviors Adopted by Number of Household Members, South Africa
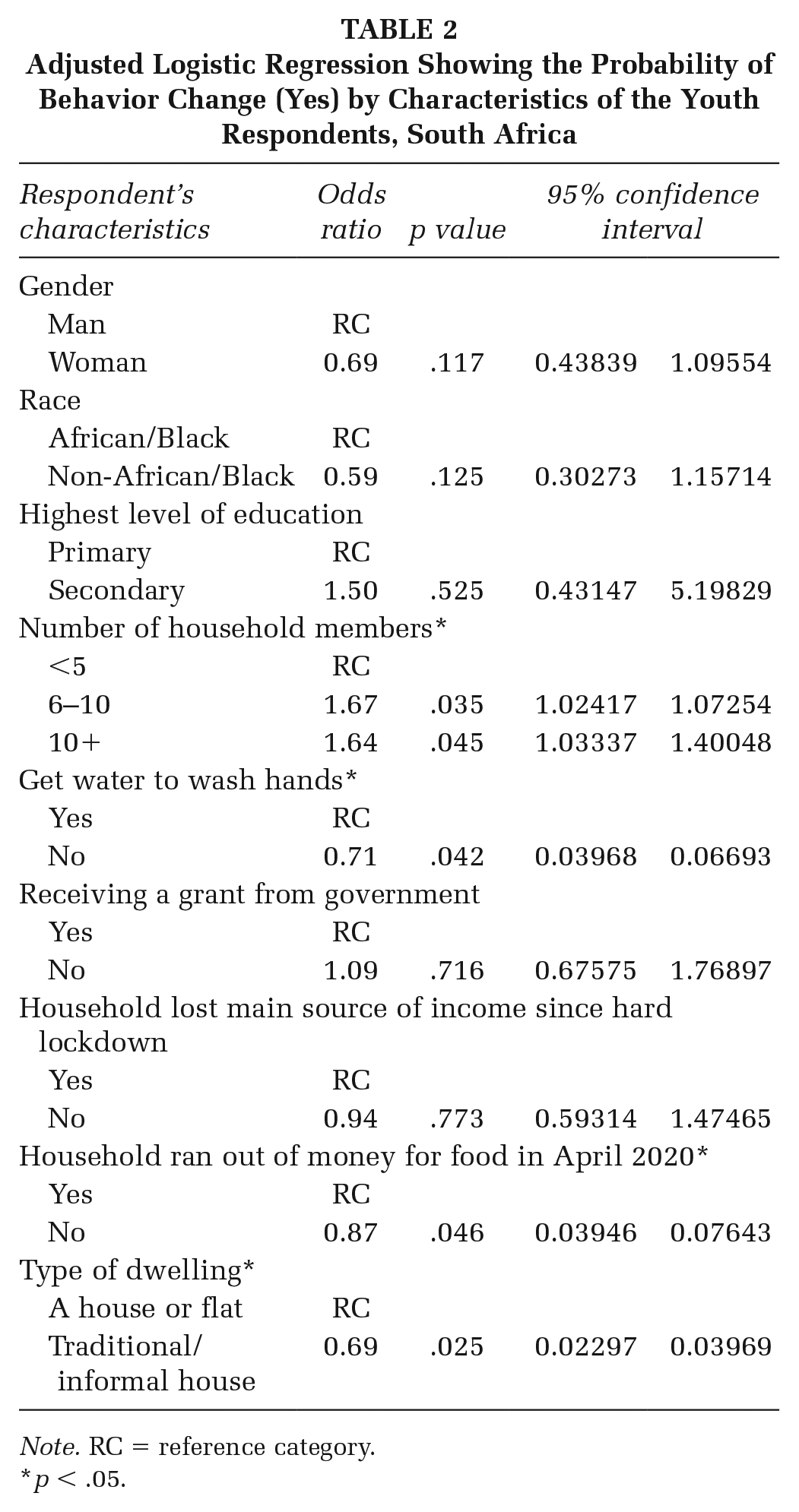
The results of the adjusted logistic regression analysis show that gender, race, highest level of education, receiving a grant from the governments, and losing a main source of household income are statistically insignificant (Table 2). However, the odds of adopting behavior change are more likely for youth in households with six or more members (ORs = 1.67 and 1.64, both p-values < .05). In addition, youth who do not have access to water to wash hands are less likely to adopt behavior change (OR = 0.71; CI = [0.03968, 0.06693]). Furthermore, youth who reside in households that ran out of money for food in April 2021 are also less likely to adopt behavior change (OR = 0.94; CI = [0.03946, 0.07643]). Finally, youth living in traditional or informal housing are also less likely to adopt behavior change (OR = 0.69; CI = [0.02297, 0.03969]).
Adjusted Logistic Regression Showing the Probability of Behavior Change (Yes) by Characteristics of the Youth Respondents, South Africa
Note. RC = reference category.
p < .05.
Discussion
The purpose of this study was to determine the extent to which youth in South Africa were able to adopt protective behaviors during the early days of the COVID-19 pandemic. Results show that, during this critical time period, not all youth were adopting the protective behaviors prescribed by the WHO.
Living in households with more than five members makes it more difficult for youth to adopt protective behaviors. In South Africa, the average household size is 3.3, therefore households with more than five members are overcrowded (Statistics SA, 2021). For youth, the restrictions in large households include limited space and privacy, but also limited time to focus and invest in education and employment attainment due to the several household duties (such as child and elderly care) which fall on their shoulders (Joseph et al., 2020; Madhavan & Crowell, 2014). Average household structures in South Africa cannot accommodate overcrowding in terms of the number of rooms and sanitation facilities available per person (Nkosi et al., 2019). Therefore, for individuals within the households, the ability to practice handwashing and other personal protective behaviors might be compromised by lack of sufficient sanitation facilities within the structure. A similar result was found in a study of informal urban settlements during the pandemic (Corburn et al., 2020). Given these restraints, it is therefore plausible that a focus on COVID-19 protective behaviors would be equally as difficult.
There are gendered differences in the adoption of protective behaviors, with young women more than young men showing protective behavior adoption. In general, studies on behavior change also found females are more likely to embrace protective behaviors than males (Bish & Michie, 2010; Clark et al., 2020; Ho et al., 2005; Manandhar et al., 2018). During the current pandemic, a study on the behaviors among adults in the United Kingdom also reported females adopted protective behaviors more than their male counterparts (Moussaoui et al., 2020). In South Africa, which is also challenged by high rates of HIV/AIDS and other infectious diseases, and the cultural and historical roles of females as primary caregivers, a dimension of responsibility for women to protect themselves so they can care for others in the household explains adopting protective behaviors (Schatz, 2007). This rationale could apply to why young women during the early stages of COVID-19, who were more likely to adopt protective behaviors.
The probability that youth will adopt protective behaviors shows association with socioeconomic factors. Youth without access to water to wash hands, who have experienced food insecurity and live in a traditional dwelling are less likely to adopt protective behaviors. These results, however, are subject to the confounding effects that the government issued social grant, specifically for low-income households during the pandemic, had on the adoption of protective behaviors. These characteristics are also signs of lower economic status and poverty, and therefore a conclusion can be drawn that youth living in more impoverished settings find it harder to adopt protective strategies to avoid COVID-19. Intergenerational poverty in South Africa is a problem with research showing that young people are continuously hindered by vulnerabilities and disadvantages experienced by their parents during Apartheid (De Lannoy et al., 2015). Further data show that more than half (58.5%) of young people live in low-income households (De Lannoy et al., 2015). In another study in South Africa, a positive relationship between socioeconomic inequality and reduced behavioral change was found (Kollamparambil & Oyenubi, 2021). The researchers attribute the lack of immediate behavior change to early misinformation about COVID-19 which suggested that it is a “rich-man’s disease,” and the less affluent underestimating their perceived risk of contracting the disease (Kollamparambil & Oyenubi, 2021). Therefore, the association between lower socioeconomic status and poverty, which are rife among youth in South Africa, and the inability to adopt protective behavior is likely.
More than two thirds of the youth in the sample reported washing their hands more regularly. While this is a substantial percentage, it is still not all youth who reported doing so. Handwashing remains the most effective means of reducing transmission. A study on youth noncompliance with government mandates in Switzerland found that 53% of youth did not wash hands regularly among other noncompliance behaviors (Nivette et al., 2021). Researchers in this study attribute youth noncompliance to disruptions to social factors, including low parental involvement and monitoring, and to education interruptions (Nivette et al., 2021). For many youth, education and employment were disturbed due to the lockdown in South Africa and many other parts of the world (Mahaye, 2020). The stress caused by this disruption to learning and daily life may have resulted in youth becoming despondent and not focused on adopting healthy behaviors. This is concerning as it suggests that powerful social determinants are overwhelming young people’s abilities to fully protect themselves from contracting the virus.
The results of this study must be borne in mind with the behavior change mandates issued by government and the nationwide lockdown which forced behavior change for the entire population and not just youth (Schröder et al., 2021). For example, the lockdown restricted travel, social gatherings. A nationwide curfew to encourage the public to stay at home and practice social distancing, and refrain from crowding in public areas. These measures forced behavior change, which youth report to have done during the 6-month time frame of our study. However, to ensure that rates do not increase, these behaviors need to be willingly adopted by youth beyond the limited duration of emergency orders. This level of behavior change could reduce the need for harsh lockdown regulations and the subsequent impact on family resources and the national economy.
Study Limitations
This study is limited in its ability to understand why socioeconomic differences make it difficult for young people to adopt protective behavior, although the relationships are not hard to imagine. The quantitative nature of this study does not provide insight into the depth of the problem between health behaviors and socioeconomic and other conditions. Second, the sample of youth in this national study is relatively small, therefore, a study with a larger sample size, with more variables pertaining to living conditions and social disruptions should be done to identify more covariates in the adoption of protective behaviors in young populations. A final limitation of the study is the exclusion of occupation as a variable to measure socioeconomic status. While the data do have occupational codes, for this age group, the nonresponse rate for this variable was about 82% and therefore not included. With better capturing of occupation type a better measurement of socioeconomic standing can be determined since income differs by type of occupation.
Study Strengths
A strength of the study, however, is that the data are recent and were collected during the pandemic. Thus, the behaviors reported are not subject to recall bias and reflect the actual behaviors of young people at that time. A second strength of the study is the ability to quantify and rank key protective behaviors regarding COVID-19. With this extensive, quantitative data more accurate and focused interventions can be developed.
Implications for Health Promotion and Future Research
The results from this study are key to understanding the challenges youth face in adopting protective behaviors during pandemics. Of notable importance to health promotion is the hindrance associated with lower socioeconomic status and the gendered differences. South Africa is one of the most unequal countries in the world, showing high indices of both income and gender inequality (Goga & Mondliwa, 2021). It is not unreasonable therefore to assume that one of the far reaching consequences of this is the inability for young people to adopt protective behaviors during COVID-19 and arguably other pandemics to come. It is precisely this point, that COVID-19 may not be the most severe or last pandemic young people will face, that health promotion interventions should not be in isolation from social and economic interventions to improve the livelihoods and equality among youth in the country and other less developed countries. Therefore, in order for youth to be able to control their behaviors and adopt safe behaviors, interventions to address gender inequality and socioeconomic conditions need to be strengthened.
In addition to more robust and inclusive socioeconomic intervention reform, qualitative research is needed to better understand the ways in which household composition, living conditions, and similar factors are affecting youth behavior during the pandemic in the country. Furthermore, since youth are embedded within diverse households, a study on the collective behaviors of household members and how that encourages or hinders protective behaviors would be useful in informing programs aimed at household health promotion.
In conclusion, the ability and feasibility for youth to adopt protective behaviors against COVID-19 are hampered by socioeconomic inequalities. In the context of those powerful social determinants, changing slowly in South Africa, there are still preventive behaviors which, if not broadly adopted, further disadvantage the health status of lower socioeconomic groups. Specific programs to support impoverished youth in adopting and maintaining preventive behaviors is an immediate priority. At the same time, recommendations by government and international organizations need to be more aware of broader challenges in the living conditions of South Africans and disregard a “one-size-fits-all” approach to behavioral compliance with emergency public health guidance.