
Abstract
The American Academy of Pediatrics recommends that children and adolescents be universally screened for access to firearms and exposure to violence. The purpose of this study was to characterize how often pediatric residents at one institution document screening for firearm access and violence risk factors and provide risk reduction counseling in the primary care setting. A retrospective chart review was conducted at two primary care clinics in Baltimore, Maryland, for patient ages 10 to 25 years who were seen by resident physicians for well care between October 2019 and December 2020. We reviewed 169 patients’ charts meeting the inclusion criteria. Forty (24%) patients had a documented history of exposure to violence or history of suicidal ideation. Based on resident documentation, one (<1%) patient was screened for firearm access or exposure to firearm violence and 10 (6%) were provided risk reduction counseling or any type of firearm safety counseling. Pediatric resident physicians at our institution rarely screen for firearm access or provide violence prevention counseling in the primary care setting. Targeted interventions and quality improvement projects are needed to address screening barriers and design novel interventions to overcome these barriers.
Keywords
Introduction
Firearms are a leading cause of death for children and youth (Centers for Disease Control and Prevention [CDC], 2021). The American Academy of Pediatrics (AAP) recommends firearms be stored locked, unloaded, and stored separate from ammunition (Dowd et al., 2012). However, currently, an estimated 4.6 million children live in households with at least one unsafely stored firearm (Azrael et al., 2018). The presence of firearms in the home has been repeatedly shown to increase the risk of death for children and adolescents (Brent et al., 1991; Dowd et al., 2012). For example, firearms are used as the lethal means in about half of all suicides (CDC, 2021; Miller et al., 2015) and safe firearm storage has shown to be a protective factor against adolescent firearm suicide (Grossman et al., 2005).
For over a decade, the American Academy of Pediatrics (AAP) has recommended that children and adolescents be universally screened for access to firearms and exposure to violence (Dowd et al., 2012). In spite of this recommendation, recent studies have shown low rates of firearm screening and safe storage counseling by pediatric residents in the inpatient and emergency settings (Monroe et al., 2020; Naureckas Li et al., 2019). Prior research from two decades ago has also shown low rates of firearm access screening in the outpatient setting (Cohen et al., 1998; Gielen et al., 1997; Solomon et al., 2002). However, recent studies have not evaluated screening and counseling practices by pediatric residents in the outpatient setting where most primary prevention is completed. Furthermore, youth in Baltimore have a disproportionate exposure to firearm violence with an overall firearm homicide rate 8 times the national rate (CDC, 2021). Given practice changes and attitudes on firearm screening, this study sought to characterize current rates of screening for firearm access and violence risk factors as well as providing risk reduction counseling by pediatric residents in a primary care setting at one institution serving a community that experiences a high rate of violence.
Methods
A retrospective chart review was conducted at two primary care clinics in Baltimore, Maryland. Both sites are university-affiliated and community-based clinics serving patients in urban neighborhoods. Patients between the ages of 10 and 25 years who were seen by resident physicians for well care were included in the review. We reviewed up to 10 individual patient visits per month for 10 months from October 2019 to March 2020 and September 2020 to December 2020. April 2020 to August 2020 were excluded due to low rates of primary care visits secondary to the COVID-19 pandemic. Patient encounters were reviewed starting on the first day of the month and continued until 10 patients were reviewed or the month ended. If a patient had ≥2 well care visits during the review period, only the first visit was included.
Demographics (age, sex, race, ethnicity, and primary language) are self-reported by patients/guardians at their first visit to the clinic and recorded in patients’ charts. While neither data on socioeconomic status nor insurance status was collected as a part of this study, about 95% of patients seen in these clinics are insured by Medicaid or the state’s Children’s Health Insurance Program. For each patient, the free text search function in the electronic medical record was used to search patients’ charts for any history of exposure to violence or any history of suicidal ideation including: witnessed or personal involvement in firearm violence, violence toward another person, injury inflicted by another person, and suicidal ideation or attempt. Resident well care notes from the date of the encounter were then reviewed for documentation on screening for firearm access and violence risk factors as well as risk reduction counseling. Only resident notes from the date of the encounter were reviewed and documentation from other health care professionals was not included. This study was approved by our Institutional Review Board.
Results
We reviewed 169 patients’ charts meeting the inclusion criteria, 100 from Site 1 and 69 from Site 2 (see Table 1). The median (interquartile range [IQR]) age was 14 (12, 18), 87 (51%) were female, 161 (95%) were non-White, 25 (15%) identified as Hispanic/Latinx, and English was the primary language for 149 patients (88%). Forty (24%) patients had a documented history of exposure to violence or history of suicidal ideation: 20 (12%) had a history of suicidal ideation or suicide attempt, 15 (9%) had a history of violence toward another person, 11 (7%) had a history of injury inflicted by another person, and 8 (5%) witnessed or were personally involved in firearm violence. Based on resident documentation, one (<1%) patient was screened for firearm access or exposure to firearm violence and 10 (6%) were provided risk reduction counseling or any type of firearm safety counseling.
Visit and Chart History Characteristics Stratified by Site
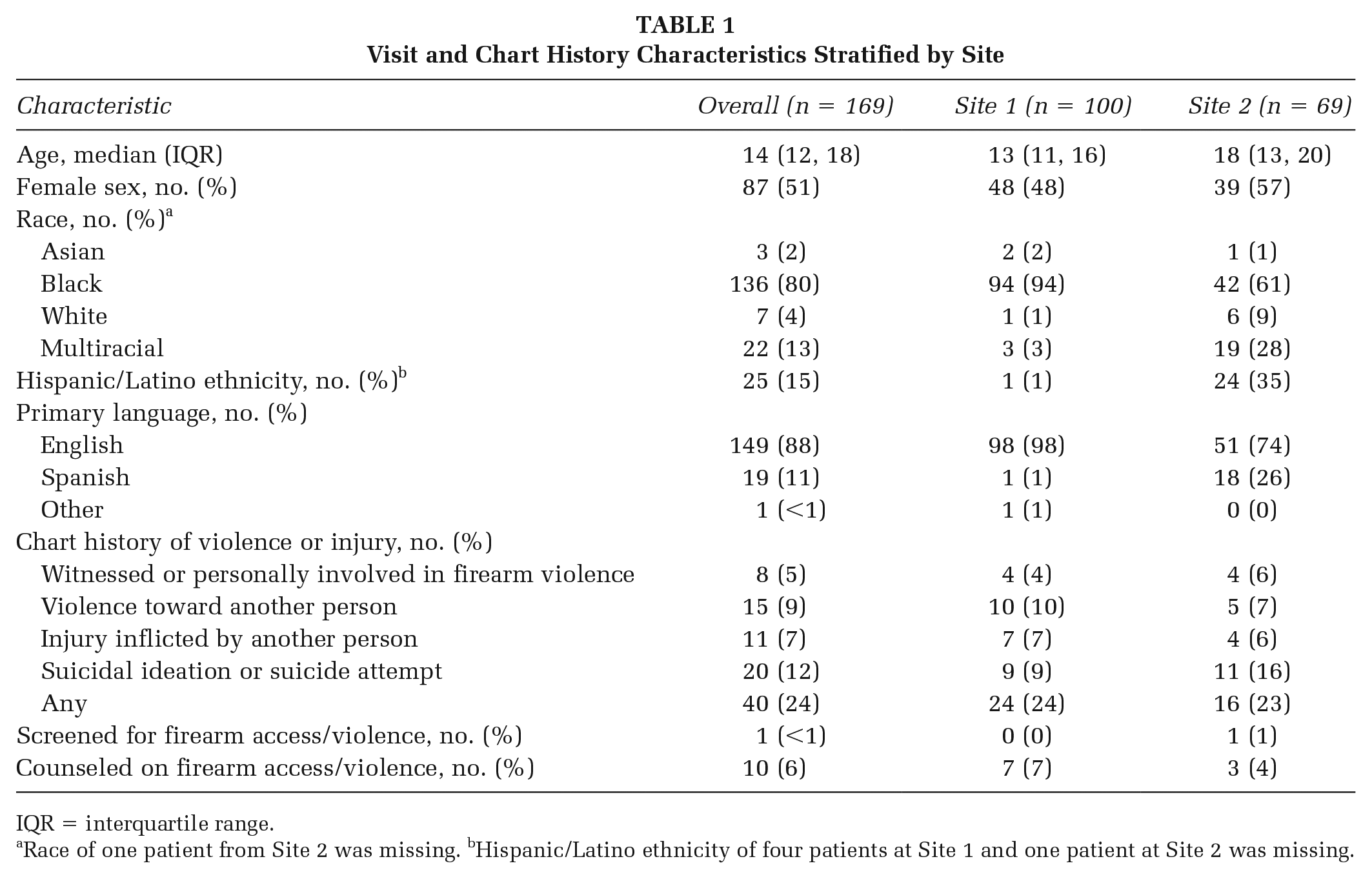
IQR = interquartile range.
Race of one patient from Site 2 was missing. bHispanic/Latino ethnicity of four patients at Site 1 and one patient at Site 2 was missing.
Discussion
Most pediatricians believe violence prevention is a priority and that pediatricians should be screening for access to firearms (Hoops & Crifasi, 2019; Olson et al., 2007). However, our findings indicate a strikingly low rate of firearm screening and risk reduction counseling in the outpatient setting by pediatric residents which is consistent with current research in other health care settings (Monroe et al., 2020; Naureckas Li et al., 2019). Our findings are especially concerning given that almost a quarter of the patients in our sample had a documented history of exposure to violence or history of suicidal ideation placing them at higher risk for firearm-related morbidity and mortality.
Prior research has documented barriers to outpatient pediatric firearm access screening such as lack of adequate training in firearm safety and insufficient time in health supervision visits to deal with firearm safety (Hoops & Crifasi, 2019; Olson et al., 2007). However, implemented interventions have been successful at addressing these barriers. One study documented significant changes in attitudes and confidence in participants’ abilities to provide firearm injury prevention counseling after completion of a web-based curriculum (Dingeldein et al., 2012). Currently, residents do not have any formal firearm injury prevention in their standard curriculum at our institution, which is not uncommon among medical education programs (Blood et al., 2020; Hoops & Crifasi, 2019). Future research and quality improvement projects need to address screening barriers and design novel interventions to overcome these barriers.
Limitations
The retrospective chart review design of this study only identified documented screening or risk reduction counseling. This methodology may have missed screening or risk reduction counseling that was a part of the visit, but not documented in the patient chart. Next, part of our study timeframe included the COVID-19 pandemic when outpatient primary care visits were limited. However, rates of screening and risk reduction counseling were similar in the prepandemic data suggesting that the low rate of screening was not a product of practice changes due to the COVID-19 pandemic. Finally, our data were collected at one institution and were limited to pediatric residents and did not differentiate among postgraduate training levels; therefore, it may not be generalizable to other pediatric residency programs and pediatricians across the country and we may have failed to identify changes in practice that occur during residents’ training.
Implications for Practice and Policy
Youth in Baltimore have a disproportionate exposure to firearm violence with an overall firearm homicide rate 8 times the national rate (CDC, 2021). This was further demonstrated in our sample by a high prevalence of exposure to violence or history of suicidal ideation among the patients seen in clinic. Despite these high rates of violence, based on clinic documentation, resident physicians at our institution rarely screen for firearm access or provide violence prevention counseling. Given the AAP goal of universal firearm screening (Dowd et al., 2012), much more work is needed. Policies need to be implemented to ensure universal screening is completed and that an appropriate intervention is available. Future work will need to be devoted to better characterizing barriers to screening and counseling and to developing tools for residents that improve their ability to approach these challenging issues.