
Abstract
This research aimed to inform the development of a health communication campaign to increase the uptake of COVID-19 prevention behaviors among university students. Twenty-eight students attending a mid-sized public university in the southeastern United States and 84 parents or guardians of university students were recruited. The study included an online survey assessing COVID-19 prevention behaviors, perceived susceptibility to COVID-19, perceived severity of COVID-19, and semi-structured interviews to elicit beliefs on COVID-19 prevention behaviors. Students and parents/guardians reported that getting COVID-19 was possible but not necessarily likely. COVID-19 was seen as serious and at least somewhat severe. Dominant interview themes for benefits, barriers, response efficacy, and self-efficacy related to prevention behaviors are reported. Overall, perceptions of behavioral benefits, barriers, and response efficacy were often shared by parents and students but varied across behaviors. These data provide insights for future campaign development for the control of infectious diseases among college students.
After shifting classes online in early 2020 as the Coronavirus Disease 2019 (COVID-19) pandemic spread worldwide, many institutions of higher learning closed campuses, and students remained home throughout the summer of 2020 (Smalley, 2021). As colleges and universities started planning to bring students back to campus for the fall semester, the authors took part in a university work group tasked with assessing the information needs of university stakeholders to inform the university’s response to COVID-19. This theoretically driven formative research conducted with parents and students informed the development of a health communication campaign for students to encourage students to engage in behaviors to reduce the spread of COVID-19. We report on this formative research and present implications for future disease outbreaks on college campuses.
Prior Research to Inform Covid-19 Communication Campaigns
Prior research to inform college communication campaigns to encourage COVID-19 prevention strategies is limited. Mackert et al. (2020) reported findings from focus groups conducted with University of Texas at Austin students, faculty, staff, and parents to test COVID-19 prevention messages. Some findings, such as those that identified adverse audience reactions to message concepts, underscore the importance of conducting formative research to inform messages. Chesser et al. (2020) report on an assessment of COVID-19 knowledge and beliefs conducted in March 2020 with a sample of college students at a university in the midwestern United States. Survey results indicated that the internet and social media were students’ primary and preferred sources for COVID-19 information. Most students surveyed (79%) identified handwashing as an effective prevention strategy, and 68% of students were amenable to receiving a COVID-19 vaccine when it became available.
There is also limited guidance and data available to inform messaging strategies for specific prevention behaviors. Barile et al. (2020) reported on data from a survey of U.S. adults conducted in May and June 2020. Their cross-sectional data suggest that higher confidence in one’s ability to wear a face covering, and higher perceived importance of the use of a face covering were positive and significant predictors of intention to wear a face covering. Botta et al. (2008) conducted formative research for a handwashing campaign using focus groups with college students. At the time the research was conducted (before the threat of COVID-19), “common threats used in hand-washing campaigns such as spreading germs and getting sick were not relevant to the students in the target audience” (p. 373). Finally, Bonell et al. (2020) provide key recommendations from behavioral science in public health campaigns to encourage social distancing including finding ways to build self-efficacy with messaging; creating campaigns with a clear “theory of change” (p. 618) and working with audience groups to design and pilot interventions.
Theoretical Framework
Prior research has demonstrated that health communication campaigns are more effective when they are informed by theory and formative research (Noar, 2006). Our inclusion of family members, specifically parents, was informed by the contextual components of Bronfenbrenner’s (1977, 1979) Bioecological Systems Theory. The college student does not operate in isolation, but is influenced by various systems including friendships, family, and the college environment, among others (Bronfenbrenner, 1992, 2005). Therefore, it was necessary to understand perceptions of COVID-19 health-related behaviors among both students and their parents to inform a university communication campaign. This is consistent with other campaigns that have utilized a family perspective to understand and inform student communication (Jones et al., 2009; McMillan, 2020). In line with recommendations from Bonell et al. (2020), we followed a formative research and campaign development approach adapted from Witte et al. (2001) that incorporates constructs from two theories often used in health communication: the Health Belief Model (Rosenstock, 1974) and the Extended Parallel Process Model (EPPM; Witte, 1992).
Health Belief Model
The Health Belief Model (HBM; Rosenstock, 1974) developed largely to explain preventive health behavior, includes several key predictors of behavior: perceived susceptibility to a health problem or condition, perceived seriousness of the health problem, perceived benefits of taking action, perceived barriers to taking action, and cues to action. The HBM has been used to guide the development of health communication campaigns across multiple topics and audiences, including college students (e.g., Case et al., 2016; Sundstrom et al., 2018). In recent survey research with students at a midwestern university in the United States, Alsulaiman and Rentner (2021) used the Health Belief Model to examine adherence to COVID-19 prevention behaviors, they found a negative relationship between perceived barriers and likelihood of adopting healthy behaviors and a positive relationship between cues to action and COVID-19 prevention behaviors.
Extended Parallel Process Model
The EPPM (Witte, 1992) proposes a process through which individuals respond to fear appeals that include threat components (severity and susceptibility) and efficacy components (response efficacy and self-efficacy). The EPPM predicts that, when both threat and efficacy are high, people will be more likely to make adaptive changes to “avert the threat” (Witte, 1992, p. 338). The EPPM has been used often in formative research and to guide the development of health communication campaigns (e.g., Cho & Witte, 2005), including messages developed for college populations (e.g., Egbert et al., 2014; Escoto et al., 2021). Additional prior research uses the EPPM to explain behaviors relevant to COVID-19 prevention such as handwashing (Botta et al., 2008) and wearing personal protective equipment (Shirahmadi et al., 2020).
To our knowledge, no published research has employed the EPPM to inform COVID-19 prevention efforts among college students, and few have used the HBM, thus our research contributes to the literature by extending the application of these theories into the context of college health campaigns related to COVID-19.
Method
This formative research employed both survey research and semi-structured interviews to inform the campaign. The research was approved by the institutional review board at the authors’ institution, and researchers obtained informed consent from participants. Data were collected in June and July 2020.
Participants
Participants included students and parents or guardians of students at a mid-sized public university in the Southeastern United States. Of approximately 22,000 students enrolled in the fall of 2022, 80.8% were undergraduate students, 51.4% identified as women, 0.5% identified as American Indian or Alaskan Native, 1.6% identified as Asian, 15.2% identified as Black or African American, 3.8% identified as Hispanic, and 72% identified as White (Mississippi State University, 2021). Of approximately 18,000 undergraduates, 22% were classified as Freshmen, 17% were sophomores, 24% were juniors, and 37% were seniors (Mississippi State University, 2021). A diverse cross-section of university students was nominated by the interdisciplinary work group (which included faculty, staff, and student representatives from units across campus). Students were purposively selected to maximize diversity in terms of major, classification, student organizations, and other characteristics and invited through email to participate in the research. Of 44 students invited to participate, 31 started the survey and 28 completed it. All 28 students who completed the survey were invited to participate in an individual interview, and 14 completed an interview. Parents and guardians were recruited through an email distributed to a university parent email list. Ninety-one parents began the survey, and 84 completed it. Of these 84, 29 were randomly selected and invited to participate in an interview, and 16 completed an interview. Participant characteristics are presented in Table 1. Students who participated in interviews had demographic characteristics similar to those of the larger student body; 78.6% were undergraduates (compared with 80.8% in the student body), 57.1% identified as female (compared with 51.4%), 21.4% identified as Black or African American (compared with 15.2%), and 78.6% identified as White (compared with 72%). Students responding to the survey represented majors from five different colleges and represented approximately 40 student organizations (including student government, Greek organizations, athletics, and others). We also had participants who reported having no involvement in organizations. Of parents who participated in interviews, 62.5% identified as female, 12.5% identified as Black or African American, and 68.8% identified as White. Parents of undergraduate students (vs. parents of graduate students) were overrepresented.
Participant Characteristics
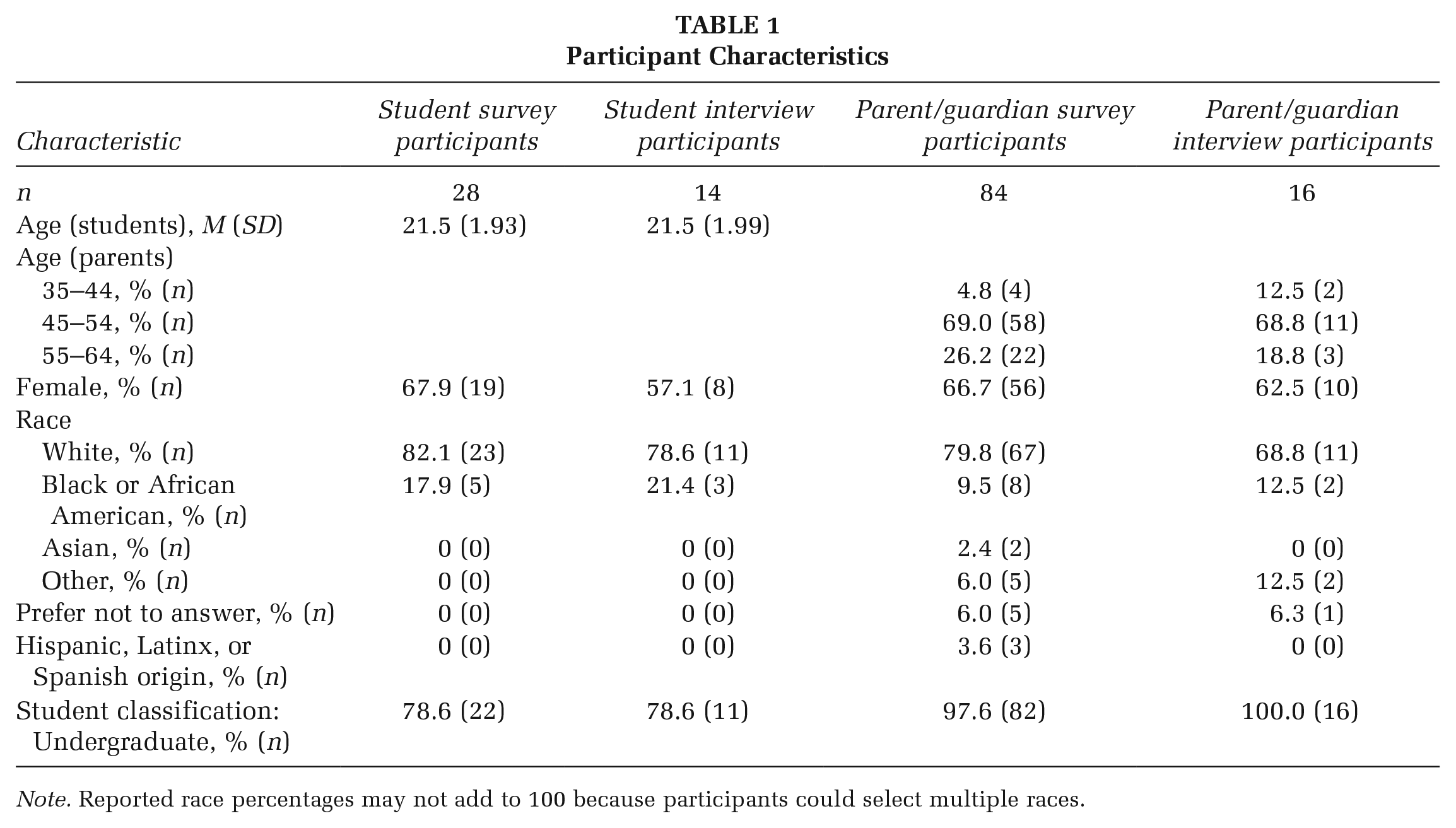
Note. Reported race percentages may not add to 100 because participants could select multiple races.
Instruments
Survey
Participants completed a web-based survey administered through Qualtrics that collected characteristics including age, gender, race, ethnicity, student classification, and education (parent/guardian survey only). Additional measures not reported in this manuscript are in the online supplement: behavior to prevent the spread of COVID-19, personal experience with COVID-19, perceived susceptibility to and severity of COVID-19 (adapted from Witte et al., 1996), and frequency of actions to reduce the spread of COVID-19.
Interview
Structured interviews followed an interview schedule to collect data on five key infection control behaviors: using hand sanitizer (washing hands was later added), wearing a face covering, physical distancing, participating in a daily COVID-19 screening, and staying home when sick (Centers for Disease Control and Prevention, 2020). For each behavior, we asked questions related to constructs of the Health Belief Model and EPPM including barriers to performing each behavior, benefits of performing each behavior, perceived response efficacy of each behavior to prevent the spread of COVID-19, self-efficacy to perform each behavior, and key referents who would influence each behavior. Interview questions were adapted from an existing instrument (Witte et al., 2001), and the interview schedule for parents and guardians differed from the student version in that it omitted self-efficacy and referents. The order of prevention behaviors was varied among participants to gather equal amounts of feedback about each behavior.
Interviewers elicited perceived COVID-19 consequences by asking “What do you see as the possible negative consequences of getting COVID-19? List all of the possible consequences you can think of.” Then, the following set of questions was repeated for each of the five behaviors (with hand washing added as a sixth behavior in later interviews). Beliefs were elicited by asking participants “What thoughts come to mind when you think about [your student] [behavior]? List all of the thoughts that come to mind.” Barriers were elicited by asking “What might keep [you/your student] from [behavior]?” Benefits were elicited by asking “What benefits do you see from [behavior]?” As defined by Witte (1992), response efficacy is “an individual’s beliefs as to whether a response effectively prevents the threat” (p. 332). For using hand sanitizer, hand washing, and physical distancing, perceived response efficacy was elicited by asking “Do you agree or disagree with the statement ‘[Behavior] will keep me from experiencing the negative consequences of COVID-19’? Please explain why you agree or disagree.” For wearing a face covering, participating in screening, and staying home when sick, statements read “[Behavior] will help prevent the spread of COVID-19,” as those behaviors were perceived as behaviors that primarily protected others. Perceived self-efficacy was elicited by asking “Do you agree or disagree with the statement ‘I am confident that I could [behavior]’? Please explain why you agree or disagree.” Important behavioral referents were elicited by asking students to “Please list the people or groups who have an important influence on your [behavior].”
Analysis
Interviews were recorded, transcribed verbatim, and coded by three authors and two graduate assistants using NVivo. Interviews were first coded deductively as pertaining to one of the behaviors and one of the theoretical constructs. Then, within each behavior and construct, the responses were coded inductively for emergent themes using the thematic analysis procedure described by Braun and Clarke (2006). The entire coding team coded two transcripts together to establish coding procedures. The team then divided the transcripts, generated initial codes, and met weekly to review transcripts and coding procedures. After all transcripts had been coded, three authors worked together to review initial codes and search for themes and illustrative quotes. Two of these authors then named and defined themes and selected final quotes for each theme. The remaining author reviewed and approved final themes, definitions, and quotes.
Results
Consequences
Four themes relating to the consequences of experiencing the coronavirus were identified. First, participants acknowledged the physical health consequences of the coronavirus associated with morbidity and mortality. Second, participants noted consequences related to the social, mental, and emotional effects of the coronavirus. Third, participants reported educational repercussions, including the adverse impact on academic participation and performance. Finally, participants noted the economic consequences of the coronavirus, including losing income, changing employment status, or depending on care while experiencing symptoms. Themes, definitions, and descriptive quotes to support the themes are reported in Table 2. Some themes were identified only in parent participants or student participants, and these differences are indicated in the table.
Themes Related to Consequences of COVID-19
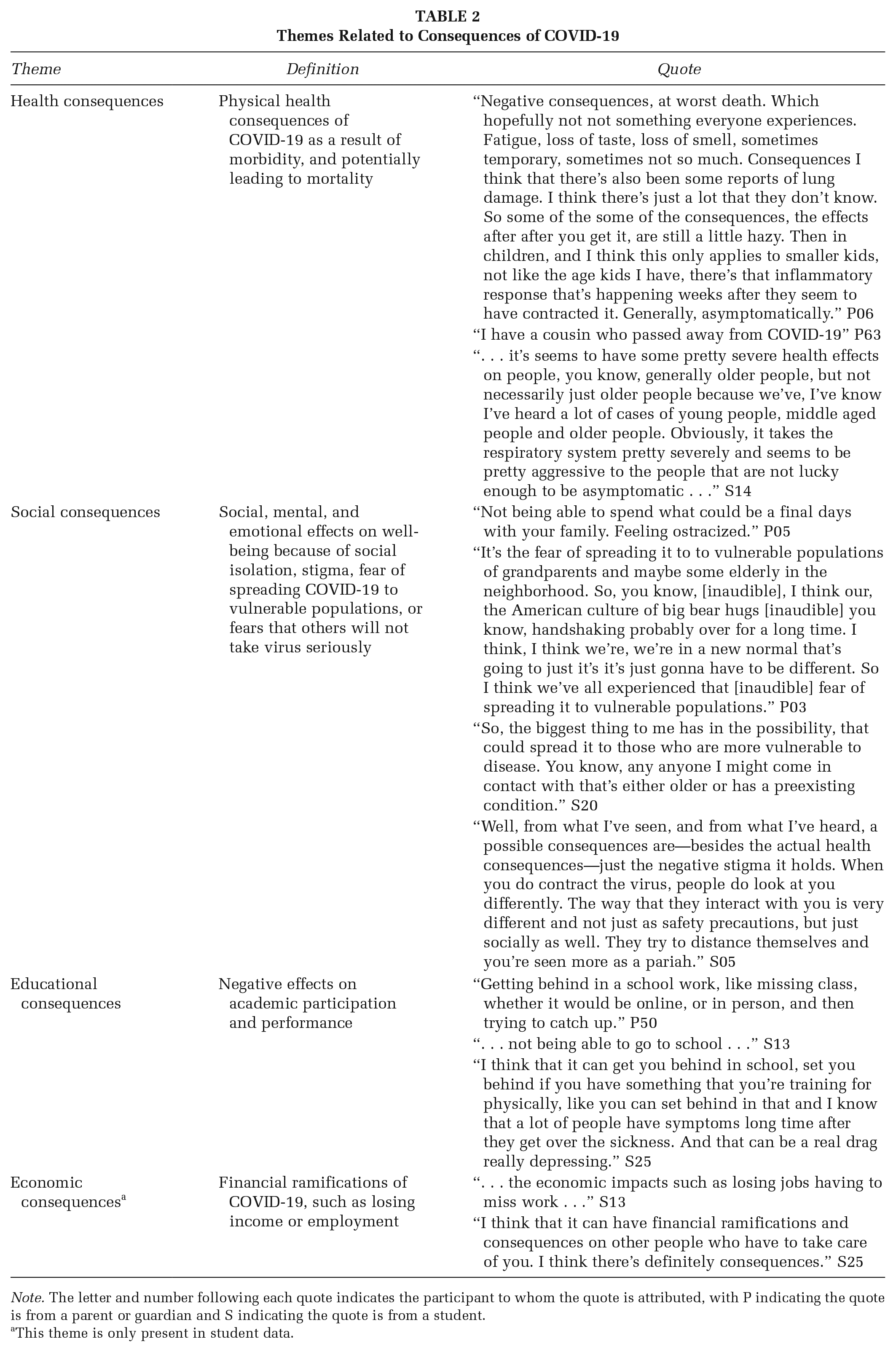
Note. The letter and number following each quote indicates the participant to whom the quote is attributed, with P indicating the quote is from a parent or guardian and S indicating the quote is from a student.
This theme is only present in student data.
Benefits, Barriers, Response Efficacy, and Self-Efficacy
Themes related to cleaning hands, wearing a face covering, physical distancing, screening, and staying home were identified and categorized according to the constructs of benefits, barriers, response efficacy, and self-efficacy. Themes are presented in Table 3, and each theme is supported by a definition and illustrative quotes by at least one parent or guardian and one student. Some themes were identified only in parent participants or student participants, and these differences are reflected in the table.
Themes Related to Benefits, Barriers, Response Efficacy, and Self-Efficacy, by Behavior

Note. The letter and number following each quote indicates the participant to whom the quote is attributed, with P indicating the quote is from a parent or guardian and S indicating the quote is from a student.
This theme applies only to parents. bThis theme applies only to students.
Cues to Action
In this study, cues to action were considered an act that stimulated consciousness about preventive health behaviors associated with the coronavirus. Although there was no direct question posed for cues to action, participants noted various cues, presented in Table 4. Participants indicated markers on the ground were helpful to understand physical distancing and to keep people adequately distanced. Group masking also provided a cue to action that helped establish the seriousness of the pandemic and normalcy. In addition, seeing other people wear a mask or use hand sanitizer provided a reminder to participants to be accountable to themselves and others. In summary, cues to action provided participants with a prompt to take action, an awareness of health behaviors taking place in society associated with the coronavirus, and personal accountability.
Cues to Action to Engage in COVID-19 Prevention Behaviors
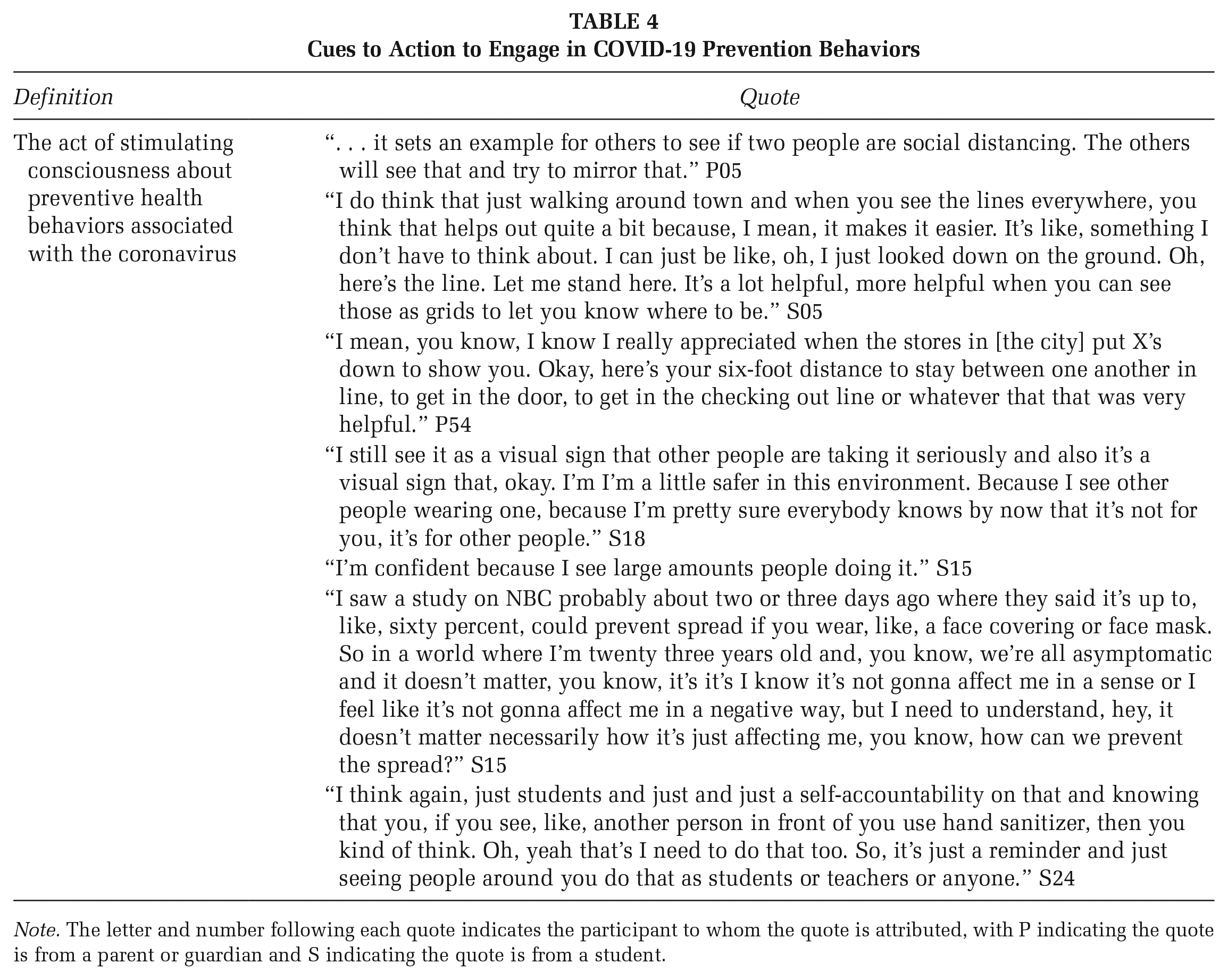
Note. The letter and number following each quote indicates the participant to whom the quote is attributed, with P indicating the quote is from a parent or guardian and S indicating the quote is from a student.
Campaign Development
The results of the study informed the university communications campaign. The following seven primary actions were communicated to students: wear a face covering, clean your hands often, observe physical distancing, stay home if you feel sick, sanitize surfaces, practice self care, and complete the daily screening. The campaign coincided with students returning to campus for the fall semester. A university press release initiated the start of the campaign and various tools were utilized to communicate the seven prevention behaviors including the use of an email signature graphic, mask up hashtag competition, yard signs, welcome back student packs in the residence halls, athletic event messaging, university emails, digital boards on campus, social media videos which included the university mascot, restroom mirror stickers, floor stickers, and a welcome back video that included the University President, Mayor, Athletics Director, Vice President for Student Affairs, Student Association President, the Director of the Diversity Center, and others.
Discussion
The interviews provided insights into key COVID-19 prevention behaviors. Participants noted key barriers to physical distancing with friends, such as forgetfulness and social pressures, highlighting that standing far away from friends and acquaintances while interacting is a new behavior and may feel awkward to some. To further understand reported prevention behaviors and inform communication efforts designed to increase these behaviors, we can return to constructs from the Health Belief Model (Rosenstock, 1974) and EPPM (Witte, 1992). We considered benefits of preventive behaviors, barriers to preventive behaviors, response efficacy, self-efficacy, and cues to action. According to the HBM, in order for someone to take a preventive action, a person needs to believe that the preventive action is beneficial and that they would not face substantial barriers. There also needs to be an “instigating event” (Rosenstock, 1974, p. 332) or cue to action. According to the EPPM, once a person perceives a moderate to high threat (determined by assessing susceptibility and severity), people evaluate the efficacy of the recommended response (determined by assessing response efficacy and self-efficacy). Our interviews yielded a nuanced understanding of these key constructs and novel findings that can inform communication efforts.
Benefits and Barriers
Across all behaviors, participants highlighted the benefit of preventing the spread of COVID-19 and protecting others, suggesting that communication appeals highlighting this benefit would be seen as plausible by this audience. Some behaviors, such as cleaning hands, wearing a face covering, and physical distancing, had the added perceived benefit of protecting the individual from COVID-19. We also observed important patterns related to barriers to protective action. Consistent with research from Scott and Vanick (2007), who found that forgetfulness was the most frequently cited reason for not washing hands, forgetfulness was a frequently cited barrier that highlights the need for reminders. Reminders could include physical signs on campus (e.g., physical distancing floor decals) or mobile push notifications. Second, accessibility was a major consideration for students and parents for behaviors that required materials (e.g., wearing a face covering). Based on this finding, colleges and universities should be encouraged to provide needed supplies to lower perceived barriers to use. Finally, social pressure was cited as an important barrier to behaviors that could be observed by others, such as wearing a face covering and physical distancing. Barile et al. (2020) found that seeing other people wearing a face covering strengthened the relationship between intention to wear a face covering and actual behavior. They attribute this to the power of descriptive norms and the way in which others’ behavior may serve as a cue to action. Barile et al. (2020) also acknowledge that wearing a face covering is a novel behavior that may be particularly susceptible to social forces. The same argument may be applied to physical distancing.
Response Efficacy and Self-Efficacy
Perceptions about response efficacy of and self-efficacy to take each recommended preventive behavior varied across individuals and behaviors, with participants often noting the conditional effectiveness of prevention behaviors and conditions needed to increase self-efficacy. For example, there was widespread acceptance of handwashing as a necessary but insufficient strategy for reducing the risk of COVID-19. Some students and parents perceived it as effective in reducing the risk of COVID-19, but others emphasized that it was only one part of a larger prevention strategy. Others were skeptical that cleaning hands would be effective. Their voices echo prior research by Botta et al. (2008), whose participants “felt that germs were everywhere and thus hand washing . . . did not really do that much to stop the spread [of germs]” (p. 377). Despite differing opinions on response efficacy, participants felt confident that they could wash hands or use sanitizer often as long as sanitizer and hand washing locations were available. This finding is consistent with prior research on hand hygiene from Botta et al. (2008), who found that college students believed they could wash their hands if they had soap and paper towels. On our campus, sanitizing stations with appropriate signage were set up throughout campus to serve as a cue to action to increase response efficacy and self-efficacy to clean hands. Hand sanitizer, both personal bottles and containers for large groups, was also made available in classrooms and other gathering spaces to increase efficacy regarding cleaning hands.
Similar themes in response efficacy and self-efficacy were observed for the other prevention behaviors. Participants believed face coverings could effectively reduce the spread of coronavirus, but participants noted the importance of compliance and perceived differences in the effectiveness of various types of masks. Factors contributing to self-efficacy to use face coverings included ease of access to face coverings and prior experience wearing a face covering. To address the use of face coverings as a protective measure to prevent the spread of COVID-19, the university developed and communicated policies via mass emails to simultaneously encourage mask wearing while emphasizing students’ rights to not wear masks as a gesture to highlight individual autonomy over one’s body. Faculty and staff were required to wear masks when near their colleagues or students. Participants saw physical distancing as somewhat effective in reducing spread, but self-efficacy to implement physical distancing varied, with students and parents voicing concerns about factors outside of the student’s control (e.g., spacing in classrooms). To encourage this behavior, the time between classes increased campuswide, classroom capacities were decreased, and students were only allowed to sit in designated seats at least three from others in classrooms and other gathering spaces. This information was conveyed via official university email correspondence. Screening for COVID-19 was seen as a practice that could slow, but not eliminate, the spread of COVID-19. Participants generally reported high levels of self-efficacy due to prior experiences with screening (such as at doctor’s offices) that normalized the behavior and reduced uncertainty. The university encouraged screening via yard signs, posters, news tickers, and recorded audiovisual advertisements to normalize testing. Randomized testing was also a practice employed by the student health center to gauge the incidence of COVID-19 on the campus. To inform various stakeholders of the COVID-19 morbidity data for the university, a webpage devoted to COVID-19 was developed and updated weekly. While not required, students who tested positive at off-campus locations were encouraged via the webpage and official university correspondence to share their results with the student health center to improve the accuracy of the morbidity data. Finally, participants reported high levels of confidence in the effectiveness of staying home when sick to prevent the spread of COVID-19. Some were also confident about their ability to stay home when sick, but others expressed concerns about missing class.
Limitations and Future Directions
The results of this study should be interpreted with the following limitations in mind. First, there are limitations related to generalizability. The participants were not randomly sampled from the university population, and, although the research team made efforts to recruit a diverse range of students and parents or guardians, those who chose to participate may not be fully representative of the university community. In addition, these results from a rural, southeastern university may not generalize to college students or parents and guardians in other regions. Future research should examine whether college student motivation to adopt preventive behaviors varies in relation to campus and community characteristics (such as size and location).
Second, there are limitations related to measurement and analysis. For example, differences observed between response efficacy themes for different behaviors could be due to the subtle shift in question wording when we asked about behaviors that protect others solely (e.g., staying home when sick) versus those that also protect the individual (e.g., cleaning hands). Interview responses may also be influenced by a social desirability bias; since interviewers were associated with campus health promotion, participants may have been reluctant to express negative thoughts associated with these efforts. Also, although the analysis team worked together to reach an agreement during each stage of the thematic analysis process, the data interpretations reflect the team’s perspective. We also acknowledge that the results of the thematic analysis represent the most prevalent beliefs and thus do not include every response.
Finally, we acknowledge that survey and interview data captured one period during a dynamic event. As science has progressed and recommendations have been updated, it is likely that beliefs about COVID-19 and prevention behaviors have changed as well. For example, the science related to the efficacy of wearing face coverings shifted over the months surrounding this research, and the benefits of wearing a face covering for the wearer became clearer after data were collected (Brooks & Butler, 2021). Future research should examine theoretical constructs related to mask-wearing considering newer efficacy data. In addition, because widely available COVID-19 testing and vaccines were not available at the time of data collection, our data do not include college students’ perceptions of testing and vaccines. Future research should examine factors that might influence these important prevention behaviors on the college campus.
Implications for Research, Practice, and Policy
By identifying beliefs that can inform theoretically-driven communication campaigns to prevent the spread of COVID-19 and other infectious respiratory illnesses, this mixed-methods study of college student and parent/guardian perceptions of COVID-19 prevention behaviors provides important insights that will be useful for health promotion research, practice, and policy.
First, this research provides important insights into how the Health Belief Model and EPPM can be applied to COVID-19 prevention behaviors. The most important contribution is the generation of a detailed list of perceived benefits, barriers, cues to action, and factors associated with response efficacy and self-efficacy for a variety of disease prevention behaviors. We used this list of perceived benefits, barriers, cues to action, and factors associated with efficacy to inform our theoretically-driven communication campaign. In particular, messaging was conveyed mainly through official university correspondence and highlighted the benefits of engaging in the desirable behaviors such as physical distancing, wearing face coverings, cleaning surfaces, and sanitizing hands. The messaging was deliberate in where it was placed and how it was conveyed in brief but attention-grabbing, culturally appropriate, and aesthetically appealing graphics. For example, to encourage physical distancing, floor stickers were placed in spaces in which there would be lines to receive services to ensure that relevant cues were in place to encourage the behavior. In addition, policies were conveyed via official university correspondence, and resources such as face masks and hand sanitizer were available for use in large gathering spaces. This in-depth understanding of the constructs and applicability of measures to align with the constructs can complement and inform future research that uses these theories.
The results also have important implications for health promotion practice and can be used to inform communication efforts to (a) increase infectious disease prevention behaviors among college students and (b) inform parents and other stakeholders about protocols to prevent the spread of the diseases on university campuses. Insights into factors that influence behaviors such as hand hygiene and face coverings may be useful in planning for prevention campaigns for infectious respiratory illnesses other than COVID-19, such as influenza. In addition, our results related to cues to action highlight the important role that communication, including simple signage, can play in prompting behaviors when message recipients already regard the behavior positively and have the self-efficacy to perform the behavior.
This research provides insight into the mental health needs of students. Social, mental, and emotional effects on well-being, because of social isolation, were noted by participants. Therefore, the campaign included a self-care component. This discovery underscores the importance for university administration, including health promotion specialists, to practice preventive and responsive mental health care for university students as they progress in their academic journey.
Finally, colleges can use these findings to inform college-level policies related to COVID-19 prevention. For example, informed by findings that students were concerned about academic penalties associated with staying home when sick, our university altered the attendance policy and communicated that change to students to increase students’ self-efficacy to adhere to recommendations. These policy changes were in addition to the aforementioned mask wearing, physical distancing in classrooms, and schedule adjustment policy changes due to COVID-19.
We acknowledge there are various divisions in the university setting. While our research team was part of a campus work group that aimed to assess and implement a communications campaign with multiple outputs, we acknowledge a more considerable team effort and action by various entities. Many individuals and other campus organizations were involved in implementing safety precautions, procedures, and preventive measures for our university campus simultaneously. Consequently, it is essential to have various levels of buy-in for prevention activities, including university administration, staff, faculty, parents, students, and other constituents.
Conclusion
Key benefits across the set of behaviors included reducing personal risk of contracting COVID-19 and reducing the spread of COVID-19 to others. Key barriers were forgetfulness, access, and social pressures. Students and parents viewed each recommended behavior as a conditionally effective piece of a larger strategy, and students were generally confident in their ability to implement prevention behaviors if they had access to needed resources. These data provide insights for future campaign development for the control of infectious diseases among college students.