
Abstract
Introduction. Immigrant nail salon owners and employees face multiple barriers to accessing occupational health training and services. We formed an academic-community-based organization–business owner partnership—unique in that all partners were culturally congruent—to develop a pilot intervention program for the nail salon community. Methods. Eighteen individuals (nine salon owners and nine employees) from the Greater Philadelphia region received the training in their native language and provided feedback through in-depth qualitative interviews. Interview guide was developed using the Consolidated Framework for Implementation Research (CFIR). Themes of perceived benefits and barriers were identified and aligned with relevant CFIR constructs to gain better understanding of the implementation challenges. Results. Reported benefits of program were improved knowledge of the workplace hazards and safety practices, and the potential to attract more customers and retain employees. Perceived barriers to implementing recommended practices were limited availability of safer products and high cost, challenges communicating with customers, lack of engagement from some owners, organizational management practices affecting employees’ motivation, and limited partnership with local government to assist small immigrant-owned businesses. Conclusions. Our study revealed multiple factors that pit long-term health protection of nail salon workers against the economic viability of the businesses that employ them. Our research highlights the need to (1) advocate for federal policies making safer products to be more accessible to the masses, (2) establish local policy and culturally appropriate technical support programs that engage community-based organizations, and (3) develop economic opportunities and mentorship for immigrant entrepreneurs to operate profitable healthy salons.
Keywords
In the United States (U.S.) today, nail salon customers expect to pay around $20.00 for a “standard” manicure and $35.00 for a basic pedicure (Smart Mom HQ, 2021). The price point varies by city; however, in general, smaller shops compete for customers in more densely populated locations by undercutting the price of services. Customers may observe that their nail technician does not speak English. They probably do not know that even with their tip of a few dollars, their nail technician is likely to earn less than what is considered a livable wage in most states (Economic Policy Institute, 2023; Sharma et al., 2018).
Women and first-generation immigrants represent approximately 81% and 79%, respectively, of the U.S. nail salon workforce (Sharma et al., 2018). Of this group, more than half identify as Vietnamese; other Asian communities such as Nepali, Chinese, Korean, and Khmer and Spanish-speaking workers account for smaller proportions. Among those born outside of the United States, almost half have limited English proficiency (Sharma et al., 2018). Nail salon workers typically work in small salons with fewer than 10 employees (Sharma et al., 2018) owned by first-generation immigrants who also work as nail technicians. These immigrant-owned microbusinesses are less able to avail themselves of occupational health information and assistance from governmental agencies, due to linguistic and cultural barriers.
Nail salon workers are among the most overlooked, and possibly at-risk, employees functioning in plain sight in the present economy. Nail technicians frequently experience health problems including respiratory, eye, and throat irritations; headaches; skin problems from chronic exposure to chemicals in nail products; and musculoskeletal pains from repetitive tasks (Dang et al., 2021; Quach et al., 2008; Huynh et al., 2019; Ma et al., 2019; Roelofs et al., 2008). Studies have also implicated long-term exposure to chemicals in the nail salon environment to adverse birth outcomes (Quach et al., 2015; Siegel et al., 2022), neurological impairment (LoSasso et al., 2001), and potentially cancers (Quach et al., 2010). Despite these clear public health concerns, evidence-based interventions for this worker population are scarce (Ward et al., 2022).
Building on our prior work surveying health and safety training needs of nail salon owners and workers in the Greater Philadelphia area (Freeland et al., 2021; Huynh et al., 2019), we formed an academic–community partnership to develop a pilot intervention program for the Vietnamese nail salon community. This article briefly describes the training content as well as the process and summative evaluation on implementation readiness among nail salon stakeholders participating in the intervention.
Methods
Community Partnership
Guided by community-based participatory research principles (Wallerstein et al., 2018), our academic team partnered with a local community-based organization, VietLead, to co-design the intervention and the research study. Our community partner guided the research team in many aspects of the study including recruitment, cultural norms, language assistance, data collection, training, research dissemination products, and opportunities (e.g., community events and briefs).
Development of Training Modules
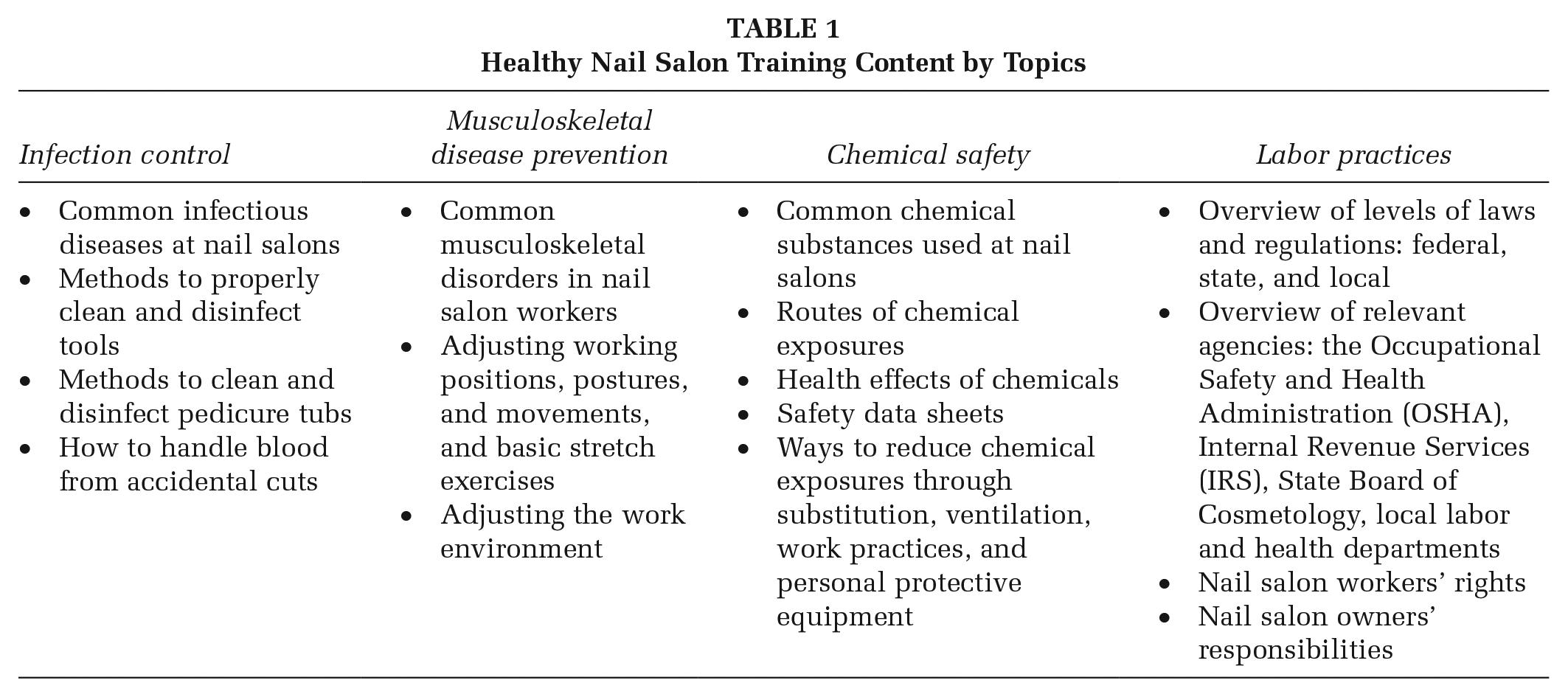
An environmental scan was conducted to identify relevant health and safety resources for nail salon workers from governmental sources, industry trade magazines, and nonprofit organizations. These materials were the basis for new content included in four training modules: infection control, musculoskeletal disease prevention, chemical safety, and labor practices. The academic and VietLead team co-developed the training modules, and the training was delivered by the academic project coordinator (DTN) and VietLead trainer (NV), both of whom happened to also be former nail salon technicians. An iterative process of reviewing the material in English and Vietnamese ensured the content and translations were technically accurate as well as culturally and linguistically appropriate. Table 1 shows the module titles and core content.
Healthy Nail Salon Training Content by Topics
Recruitment and Intervention Delivery
Eighteen participants (nine Vietnamese nail salon owners and nine employees) were recruited using snowball sampling through VietLead’s network of nail salons. Participants were at least 18 years old, current part-time or full-time technicians or owners at nail salons in the “tri-state” (Pennsylvania, New Jersey, Delaware) area. VietLead trainer (NV) delivered the training through an online platform from October to December 2020, and in-person at the salons from January to March 2022. Seven individuals participated in the online training, 11 recruited to complete the in-depth interview from the in-person training cohort.
Data Collection and Analysis
Process Evaluation
During the online training, participants were asked to join 10-minute breakout sessions with our bilingual study team to provide feedback on the content and delivery (N = 7). Nail salon employees were interviewed separately from owners to minimize discomfort and potential interference in responses.
End-Point Evaluation
After completion of the training, we conducted in-depth interviews with participants from both the online and in-person training (N = 18) using a Vietnamese language questionnaire consisting of closed- and open-ended questions based on the Consolidated Framework for Implementation Research (CFIR) to gain a better understanding of factors that might influence intervention implementation and effectiveness (Damschroder et al., 2009; Keith et al., 2017; CFIR Rearch Team-Center for Clinical Management Research, 2023). Our questionnaire focused on implementation readiness constructs from the CFIR framework to ensure the collected data were relevant to our research objectives (Kononowech et al., 2021). Responses were typed by the interviewers into Qualtrics (Qualtrics, Provo, UT) during the interview, and later translated into English for analysis.
Responses were independently coded by two team members in NVivo (QSR International, 2020, released in March). The Health Belief Model (HBM) provided the framework for a priori codes, focusing on identifying the perceived benefits and barriers to act on the training recommendations, as well as self-efficacy in making changes (Jones et al., 2015). Emergent themes were also identified using a grounded theory approach (Charmaz, 2006/2009). Both coders and a third team member discussed themes, created draft coding schemes, examined intercoder discrepancies, and through an iterative process, built consensus around final codes and their definitions. Descriptive statistics were performed on the few closed-ended questions to provide context for this primarily qualitative study.
The project was approved by the Drexel University Institutional Review Board.
Results
Quantitative Data
When asked to rank the quality of the training during the process evaluation, most of the participants (95%) ranked it high or very high. When asked about the complexity of the recommended practices, 67% expressed that they are easy to implement, 28% average, and 6% difficult. All of the participants (100%) thought that many of the “small” recommendations can be applied immediately in their daily practices and these involve personal hygiene and ergonomics techniques such as frequent handwash, use of PPE (masks, gloves), proper working positions to prevent injury, proper cleaning, and disinfecting techniques and stretching muscles during the breaks.
Perceived Benefits
Table 2 presents thematic results organized by CFIR and HBM constructs and provides supporting quotes from participants. We identified two key perceived benefits of the training from our analysis. The first benefit was improved knowledge and awareness of workplace hazards and safety practices to protect their health (HBM knowledge and belief construct). Relating to this theme is the perception that the training supplements their cosmetology training specific to the health risks. Some participants expressed that it has been years since they had their license, and there is a lack of continuing educational materials in their native language (Vietnamese). One salon employee noted, “I find [this training] very helpful. I had lessons from school in the past, but they were not this detailed and practical.” One owner participant expressed, “There are many small things that we can implement, clean pedicure spa, wear gloves.” (CFIR trialability construct). The second perceived benefit is the potential to attract more customers, increase income, and retain employees (CFIR relative advantage construct). One salon owner said, “Customers like healthy salons (no smell, clean) and feel assured. More income.” Another owner added, “Employees like working in healthy salon environment.” However, others were less certain about this benefit.
Themes of Perceived Benefits and Barriers Related to the Consolidated Framework of Implementation Research (CFIR) Constructs and Supporting Quotes From the Participants
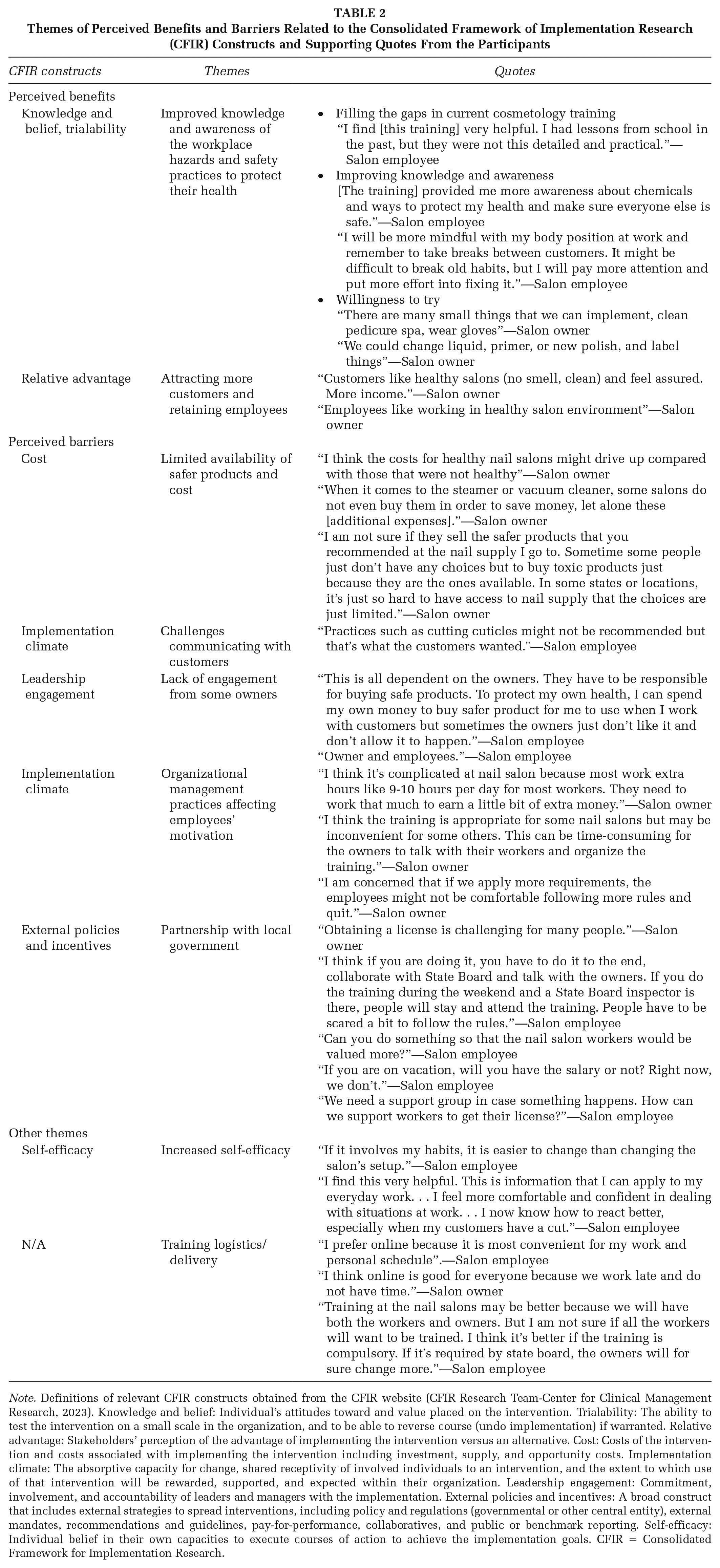
Note. Definitions of relevant CFIR constructs obtained from the CFIR website (CFIR Research Team-Center for Clinical Management Research, 2023). Knowledge and belief: Individual’s attitudes toward and value placed on the intervention. Trialability: The ability to test the intervention on a small scale in the organization, and to be able to reverse course (undo implementation) if warranted. Relative advantage: Stakeholders’ perception of the advantage of implementing the intervention versus an alternative. Cost: Costs of the intervention and costs associated with implementing the intervention including investment, supply, and opportunity costs. Implementation climate: The absorptive capacity for change, shared receptivity of involved individuals to an intervention, and the extent to which use of that intervention will be rewarded, supported, and expected within their organization. Leadership engagement: Commitment, involvement, and accountability of leaders and managers with the implementation. External policies and incentives: A broad construct that includes external strategies to spread interventions, including policy and regulations (governmental or other central entity), external mandates, recommendations and guidelines, pay-for-performance, collaboratives, and public or benchmark reporting. Self-efficacy: Individual belief in their own capacities to execute courses of action to achieve the implementation goals. CFIR = Consolidated Framework for Implementation Research.
Perceived Barriers
We identified five themes related to implementation barriers (Table 2). The first barrier was the limited availability of affordable safer products at local nail suppliers and the high cost of purchasing new equipment and materials, and upgrading the existing ventilation systems (CFIR cost construct). The second barrier related to challenges communicating with customers about the salon’s policy, likely stemming from language barriers (CFIR implementation climate construct). One such example is customers preferring their nail tech to cut cuticles when such a practice is not considered safe. The third barrier was the lack of engagement from some owners (CFIR leadership engagement construct). Most salon employee participants expressed that they and their coworkers did not have much power to implement changes in their salons and thought that the owners should actively engage in the process to make any meaningful difference. One salon employee said: This is all dependent on the owners. They have to be responsible for buying safe products. To protect my own health, I can spend my own money to buy safer product for me to use when I work with customers but sometimes the owners just don’t like it and don’t allow it to happen.
Two employee participants indicated that both owners and employees should be engaged. The fourth barrier pertained to the organizational management practices (implementation climate) such as low wage and long work hours that may impact employees’ motivation for change. One owner participant shared, “I think it’s complicated at nail salon because most work extra hours like 9-10 hours per day for most workers. They need to work that much to earn a little bit of extra money.” Some owner participants suggested the training needed to consider challenges putting these recommendations into practice and be more realistic about the expected outcomes and potential resistance from salon employees. Finally, there was the expressed need to partner with local government to support small, immigrant-owned business owners, and their employees (external policies and incentives). Some participants expressed difficulty in obtaining a license for new immigrants with limited English skills “How can we support workers to get their license?,” others suggested the need for local government involvement as a catalyst for change. While most owner and employee participants agreed that collaboration with the government (e.g., Department of Labor, State Board of Cosmetology, public health departments), will improve the credentials of a voluntary training program and facilitate enrollment and participation, some employee participants believed it would be better if the training were compulsory and enforced, I think if you are doing it, you have to do it to the end, collaborate with State Board and talk with the owners. If you do the training during the weekend and a State Board inspector is there, people will stay and attend the training. People have to be scared a bit to follow the rules.
Furthermore, some employee participants expressed their hope to raise the dignity of nail salon work and a sense of solidarity in helping each other. One worker participant said, “Can you do something so that the nail salon workers would be valued more?” Owner participants expressed the need for financial support to “renovate the salon” such as “tax breaks,” and business development classes so they can help their employees with “health insurance and 401k,” as well as “classes on safety and labor laws.”
Other Themes
Self-Efficacy
Employee participants expressed higher confidence in changing personal behavior after the training but low confidence in changing the work environment and their coworkers’ behaviors (HBM self-efficacy construct). One employee said, “If it involves my habits, it is easier to change than changing the salon’s setup.”
Training Logistics/Delivery
Preference for the training format was mixed. Online was preferred by some participants because of the convenience and flexibility in scheduling the training late at night after work. Participants preferring in-person over online format expressed that it would be easier for them to comprehend the training and they would not need to deal with technology challenges. Another nail technician added that the training should be offered at the salons and made mandatory for both owners and employees.
Finally, many participants noted that having the training in simple “mother-tongue language” made the training much easier to understand, “it is easy to understand in Vietnamese because it is my first language.” The participants also acknowledged the trainers for being clear, detailed, approachable, and passionate in their instructions, “the trainer is passionate and explains in detail.”
Discussion
Immigrant nail salon owners and their employees have unique occupational health needs and due to their disadvantaged background, cultural and linguistic barriers, and status as family-owned small businesses, nail salons often have limited resources and technical capacity to implement occupational health best practices. To address this gap, we employed a community-based approach to co-develop an in-language occupational health training intervention and document the perceived benefits and barriers to its implementation. While participants recognized that improved knowledge of workplace hazards and the potential to grow their businesses as promising benefits, many structural barriers such as cost, availability of safer alternatives, limited engagement from owners, and lack of partnership from local government may hinder successful implementation.
Implications for Policy and Practice
Our results revealed that there is a need to address structural inequities simultaneously with offering in-language, in-house occupational health training services to ensure nail salon health, and safety recommendations can be implemented by these small immigrant-owned businesses. Potential impacts include both long-term positive impact on worker health and the economic vitality of these businesses. The following highlights some of the multipronged initiatives that may be considered by local governments, community-based organizations, and the nail industry to address these unmet needs.
The few “safer” alternatives to current nail salon products are limited in availability and are generally more expensive. Recognizing that individuals with disadvantaged socioeconomic status, women of color, and salon workers bear the disproportionate harm from toxic products, passing of policy proposals such as the U.S. Safer Beauty Bill Package that target manufacturers and suppliers is a critical step in addressing the cost and limited availabilities of safer products in the nail salon supply chain (Office of Congresswomen Jan Schakowsky, 2021). This bill package federally bans toxic chemicals in beauty and personal care products, requires safety data sheets to be available in English, Chinese, Korean, Vietnamese, Spanish, and other languages upon request, provides funding for development of safer alternatives, and creates transparency in the supply chains (Campaign for Safe Cosmetics, 2023). At the state level, California is at the forefront of establishing policies banning toxic ingredients in beauty and personal care products such as the California Toxic Free Cosmetics Act of 2020.
Currently, very few states offer or support comprehensive in-language occupational health education to assist nail salon owners and employees. A promising strategy to overcome linguistic and cultural barriers to chemical safety and other best practices uptake is to invest and empower CBOs with occupational health skills and resources so that they can work with nail salon workers and owners within their communities. Not only do the trainers speak the same language as the participants but are most credible if they are from the same community and/or have the lived experience of the nail salon environment. Our participants noted a positive feature of our training was our community trainers, suggesting that they were a significant factor in the positive reception of the training. Successful government–community–business partnership models have been replicated in several states where effective nail salon worker organizations exist, such as the California Healthy Nail Salon Collaborative, Boat People SOS, Adhikaar in New York, VietAID in Massachusetts, and VietLead in Pennsylvania. Each of these organizations have played significant roles in advocating and delivering culturally appropriate services to salon owners and employees.
Challenges operating small businesses were a recurring theme that emerged from our study, suggesting that to get the owners’ buy-in to support occupational health training, their business concerns need to be addressed. Immigrants with low-English proficiency have limited income mobility and thus for many immigrant owners, their business is necessary for survival. During the pandemic, many salon owners were financially impacted and had difficulty accessing financial assistance from dedicated government programs due to language and immigration-related barriers (Herrera et al., 2022; Sharma et al., 2022). Moreover, many salon owners are not part of a business association or a local chamber of commerce, further isolating them from resources, business development opportunities, mentorship, and legislative influence. There is a need for the larger business community and local government partnerships to support small businesses within the nail industry. Examples of investment could be in-language business trainings and mentorship to immigrant entrepreneurs on business management best practices, and grants and low-interest loans to upgrade their salons with safer products and better ventilation.
Finally, challenges relating to obtaining a work license continue to put many immigrant nail salon employees and owners in vulnerable predicaments. In Pennsylvania, trainees are required to sit in 250 hours of learning in a cosmetology school but many reported learning more and better on the job. Allowing for an apprenticeship program so that new immigrants can quickly earn a living while learning on the job would reduce some of these barriers. As an example, the New York Committee for Occupational Safety & Health established the New York Nail Salon Worker School (New York Committee for Occupational Safety and Health [NYCOSH], 2023) to support new manicurists, regardless of immigration status, by offering a shorter in-language training program (26 hours) and allowing them to register as apprentices and earn fair wages until they are ready to take the licensing exam. Such programs or any efforts to reduce barriers to obtaining a work license will help reduce worker vulnerabilities and fear of authorities.
Other Intervention Considerations
Owing to the COVID-19 pandemic, some trainings were offered remotely. While there were challenges helping participants navigate Zoom technology, we also saw tremendous opportunities in the use of online training formats (synchronous or asynchronous) and social media platforms to reach more nail salon workers and owners in a more cost-effective way. Within the Vietnamese nail community, there are numerous social media platforms being used to advertise new nail products and services, and form connections. Many of these channels can be easily accessed with mobile phones at work or home and could enhance outreach efforts to accommodate busy work and family schedules. While online training may be an efficient way to deliver information to certain members of the nail workforce, it will be important to provide on-going local and interpersonal technical support after the training to help owners and workers implement the changes. Cultural and linguistic knowledge will be critical to bridging that connection.
An important consideration in salon training interventions is the differences in state regulations for nail salons. While federal standards on safe workplaces enforced by OSHA are appliable to all nail salons across the country, the nail salon owners and employees we interviewed believed that State Board of Cosmetology inspectors visited more frequently than OSHA. Future trainings that cross state’s boundaries should address each state’s specific regulations to ensure that this training component is relevant to the intended audience.
Strengths and Limitations
The primary strength of our work is that it was all culturally and linguistically congruent. Our study was done in the Philadelphia focused tri-state area, and results may not be applicable in other areas of the country, and certainly are not generalizable to all nail salon workers and owners, particularly those of different ethnic and cultural backgrounds. Our sample size of 18 might be noted as a limitation, but we were able to reach thematic saturation in our qualitative study. Our snowball sampling approach is a strength, as it extended from VietLead’s years of relationship-building with salons. However, the final sample may be biased toward salons that were more receptive to adopting new practices than others.
Conclusions
To our knowledge, few nail salon intervention studies document the perceived benefits and barriers to implementing occupational health recommendations. Our study may offer strategies to develop public health programming to support immigrant salon owners and employees. To help overcome structural inequalities immigrant salon owners and workers face, we advocate for (a) a federal mandate requiring manufacturers to eliminate the production of toxic chemicals in beauty and personal care products and to invest in the development of safer and cheaper alternatives, (b) establishment of local policy and technical support programs that are culturally and linguistically appropriate and engage local CBOs to address the gaps of occupational health regulations at the state and federal levels, and (c) economic investment and business mentorship for immigrant nail salon entrepreneurs to grow and market their healthy salons. Nail salons are the economic backbone of many immigrant families. Empowering businesses and their employees to work safer and together will help uplift the community as a whole.
Footnotes
Authors’ Note:
We are indebted to the participants for their feedback on the training and opinions about issues affecting nail care professionals and industry. We are grateful of the following individuals who helped facilitating the training: Tracy Nguyễn, Hoang Anh Nguyễn, Mai Anh Nguyễn, Emily Nguyễn, and Trisha Lê. We thank Châu Nguyễn for the translation of the responses and Dr. Igor Burstyn for reviewing the initial draft of the manuscript and the anonymous reviewers for their feedback. This work was generously supported by the National Institute of Occupational Safety and Health through grant numbers (K01OH011191and R21OH011740), the Drexel Urban Health Collaborative’s Pilot Grant, and Dr. Arthur Frank.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.