
Abstract
Our Grassroots Maternal and Child Health (MCH) Initiative works to build the capacity of individuals and organizations in zip codes with persistently high infant mortality rates to bring about systems change that will improve maternal and child health (MCH) outcomes. Foundational to the Initiative is the training and mentoring of local women to become Grassroots MCH Leaders. We greatly honor that these women possess community expertise, essential to the Initiative’s success. Our training equips them with strategies they can use to bring about changes in social, economic, political, and/or cultural systems that underlie poor birth outcomes. One impactful strategy they learn is the use of critical narrative intervention (CNI). This approach, grounded in the crafting and sharing of stories, complements statistical, behavioral, and medical approaches to improve MCH outcomes. This article describes the impact of CNI within the Grassroots MCH Initiative. Drawing from 14 Grassroots MCH Leaders’ narratives, we present five significant maternal traumas and influential supports in their surrounding contexts. We explore the leaders’ reflections on the impact of story development and dissemination. Our findings reveal that situating CNI within the context of a grassroots initiative provides opportunities for leaders to use their stories to advocate for systems change. Personal MCH narratives provide a powerful and respectful approach to public health promotion, as they highlight important systems-level failures that need to be addressed to sustainability improve MCH outcomes.
Keywords
Despite highly ranked health care systems, Indiana consistently ranks poorly on measures of maternal and infant health, with a 2019 pregnancy-associated mortality ratio of 74.2 per 100,000 live births, (Indiana Department of Health, 2021) and a 2020 total infant mortality rate of 6.6 with a Black infant mortality rate nearly double that—13.2 (Indiana Department of Health, 2020). Efforts to sustainably improve maternal and child health (MCH) outcomes must address inequitable social, economic, and political systems that traumatize mothers from marginalized communities (Yamin, 1997). Beginning in 2018, university-based faculty and staff at IU Fairbanks School of Public Health collaborated with state- and community-based partners to launch the Grassroots MCH Initiative (Marquam et al., 2020; Skinner et al., 2019; Turman & Swigonski, 2021). The Initiative’s unique approach seeks to build the capacity of women living in zip codes with high infant mortality rates, referred to in the project as Grassroots MCH Leaders (GMCHLs), to bring about systems change to improve pregnancy and infant health outcomes in marginalized communities. One major aim of this initiative is personal and societal transformation through MCH storytelling. While the Initiative continues to engage in and has expanded the scope of its capacity-building work, this article reflects findings from the first 3 years of effort to improve MCH outcomes through storytelling.
Critical narrative intervention (CNI) is a new and compelling framework for using narratives to advance systems change in public health (Fiddian-Green & Gubrium, 2021; Gubrium et al., 2019). CNI prioritizes 1) rendering otherwise discounted local knowledge as relevant by working with marginalized communities to produce their own stories, 2) bolstering social support and solidarity in the process, and 3) critiquing and recalibrating damaging and disempowering conversations on social health and well-being, ultimately to create more supportive policies with and for marginalized communities (Gubrium et al., 2019, p. 2).
The incorporation of CNI into public health initiatives has yielded promising results, transforming the understanding of domains like sexual and reproductive health (Gubrium et al., 2019; Kendrick et al., 2021; Krause & Gubrium, 2019; Mamo et al., 2021) and substance use (Bartoszko, 2021; Oudshoorn et al., 2021). Within the Grassroots MCH Initiative, our approach to storytelling aligns tightly with the CNI strategies and aims. Infant mortality is regarded as an important indicator of population health, living conditions, and social well-being (Reidpath & Allotey, 2003); by recruiting and supporting GMCHLs from zip codes with high infant mortality rates, we reach and learn from communities that are economically and socially marginalized. Faculty and staff provide leadership and storytelling workshops as well as ongoing instrumental and social support. Over their year (or, if desired, more) of participation in the Initiative, GMCHLs receive and take on opportunities to share their MCH stories to bring about systems change.
Throughout history, grassroots movements and their leaders have been important drivers of change, particularly in women’s health (see, e.g., Mothers2Mothers, 2020; Our Bodies Ourselves, 2022). Such movements often share common features: in addition to harnessing the power of storytelling, they navigate across the social–ecological model, build leadership structures to support collective efficacy, and view empowerment as a process, not a product (Marquam et al., 2020). Situating CNI in a grassroots initiative that embraces these principles has offered unique benefits, articulated herein through GMCHLs’ reflections on the narrative creation and intervention process. We hope the discussion of the initial results of our efforts adds to our understanding of the potential benefits of CNI as an important health promotion practice and the support structures that may maximize its success.
Method
Figure 1 offers a summary of the Grassroots MCH Initiative’s curriculum and overall structure, which was described in detail elsewhere (Skinner et al., 2019).
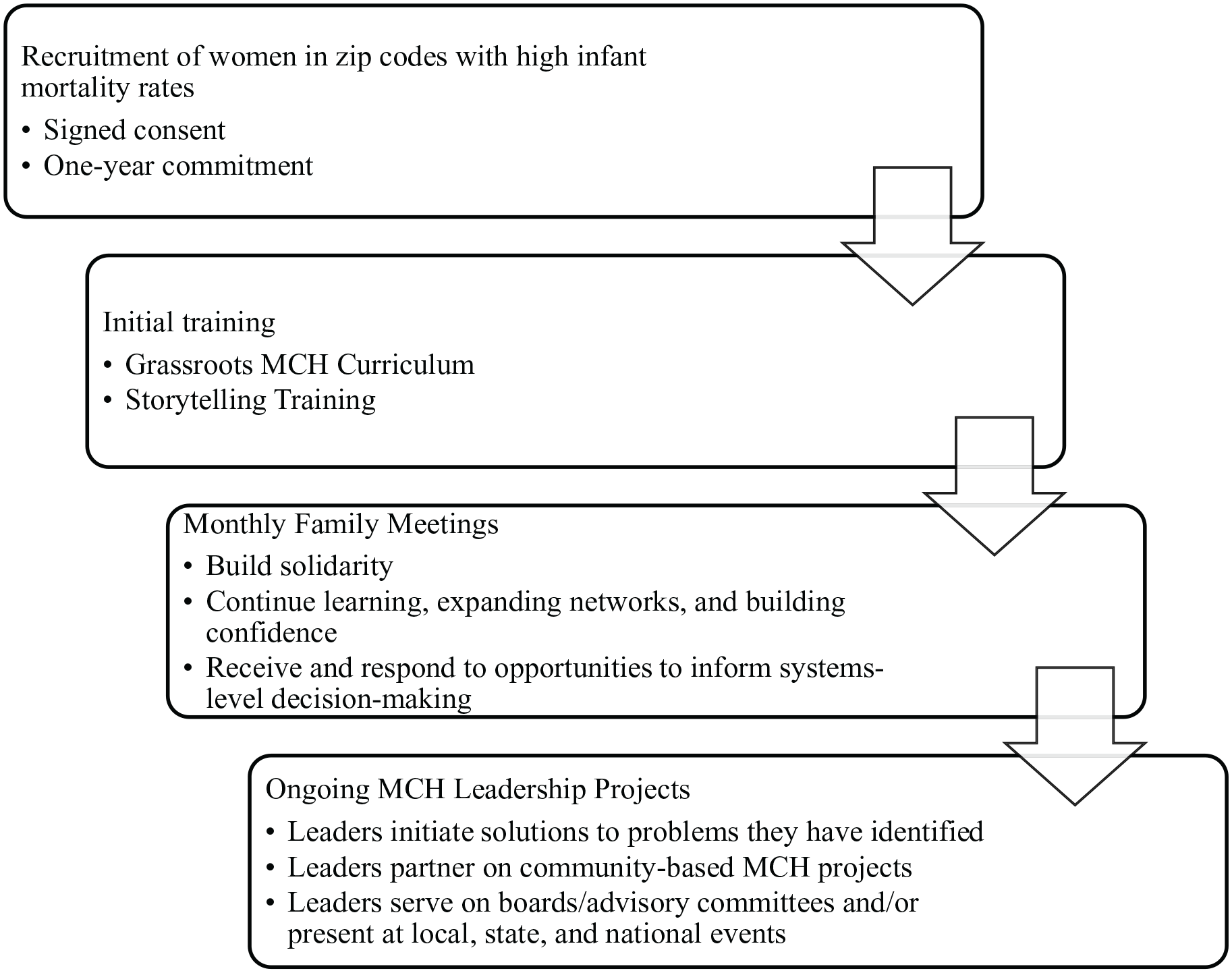
Grassroots MCH Initiative Approach
Recruitment
Our university-based team recruited women from zip codes with the highest infant mortality rates through recommendations from partnerships with affordable housing complexes, Healthy Start employees, health care workers, and social service agencies. This article presents findings based on the first 14 participants in the GMCHL training program. GMCHLs were asked to commit to at least 1 year of participation through an institutional review board-approved process and offered monthly US$300 gift cards for 12 hours of service per month.
Narrative Creation and Intervention
After completing the leadership curriculum, which includes instruction in community health promotion, causes and consequences of infant mortality, building health equity to reduce disparities, using the social–ecological approach to improve MCH, and building women’s empowerment to improve MCH (Skinner et al., 2019), GMCHLs participated in a four-part storytelling workshop. A graduate student in anthropology and co-author (N.L.) developed and implemented the narrative creation methodology (Figure 2). Participatory Action Research (PAR) frameworks (Baum et al., 2006), which are rooted in the notion that participants and researchers exist in an equitable relationship that balances power, guided the development of the storytelling training. We asked each GMCHL to write a two- or three-page personal MCH narrative that could be used for communication with state officials, community organizations, and neighbors to raise awareness about and build coalitions to reduce infant mortality in their community. GMCHLs were encouraged to include a call to action, leveraging their knowledge of their communities’ needs. Narrative development sessions occurred in community venues convenient to the leaders.
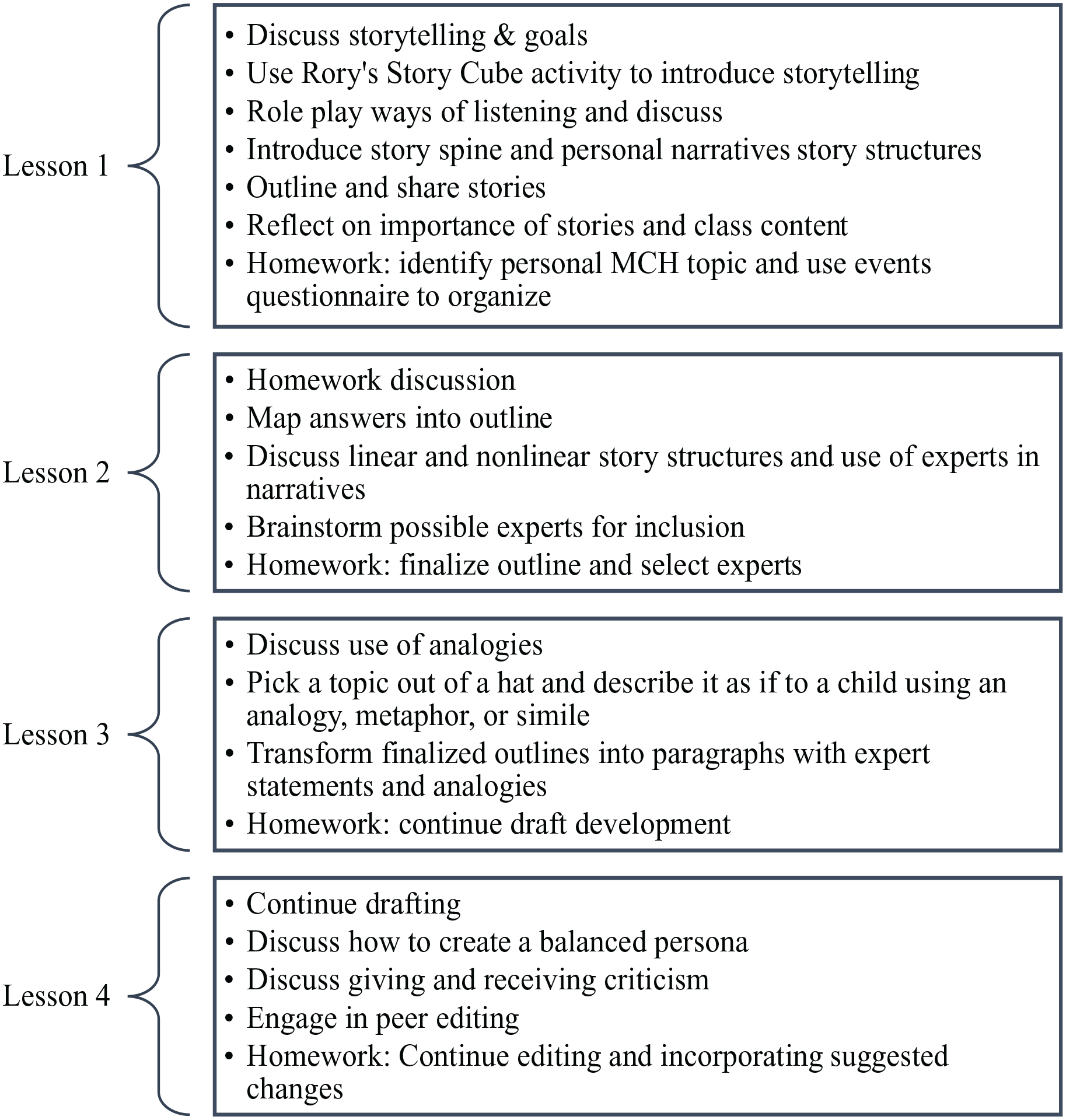
Outline of Storytelling Curriculum
Following the development of their written narratives (n = 14), leaders were coached in story presentation for a wide range of stakeholders and shared their stories with each other to practice and gain positive reinforcement. Throughout their remaining time with the Initiative, leaders were regularly invited to participate in opportunities to share their stories. These included presentations at state and local conferences, YouTube recordings, meetings with legislators or reporters, training sessions with staff in MCH programs, and other venues (Table 1).
Critical Narrative Intervention
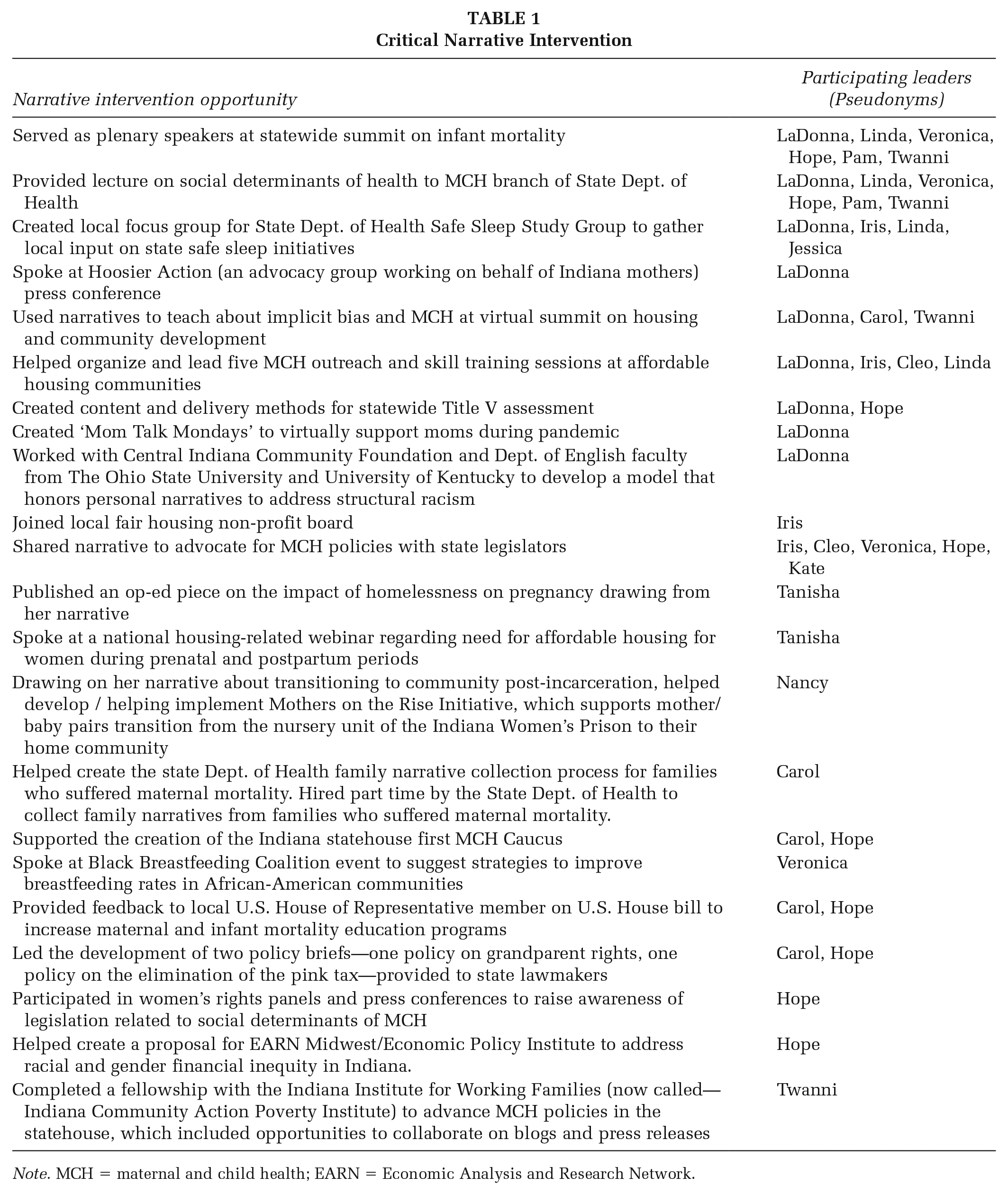
Note. MCH = maternal and child health; EARN = Economic Analysis and Research Network.
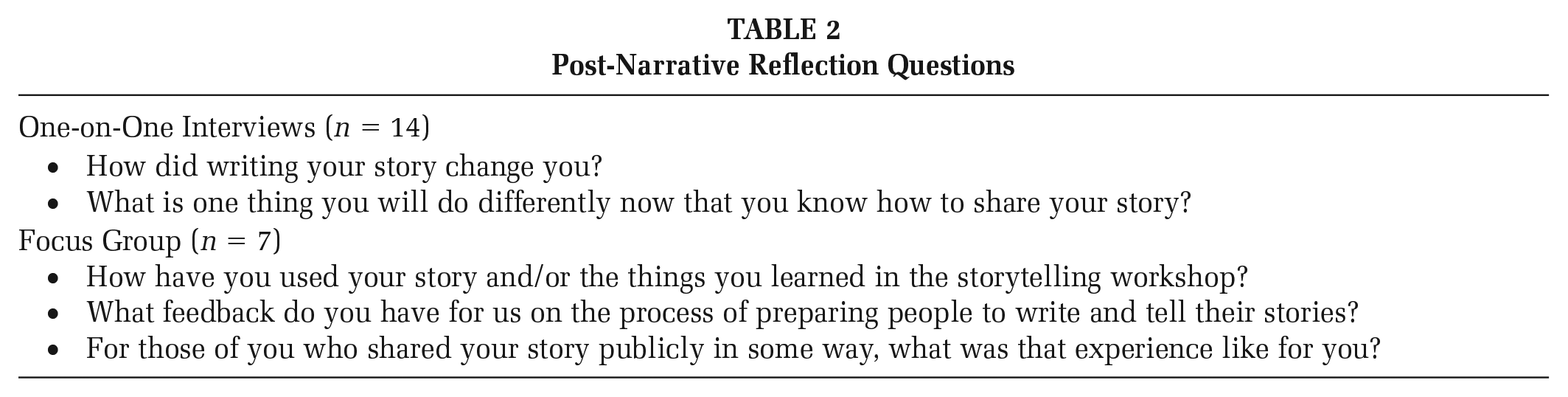
Approximately 3 months after a leader completed the storytelling curriculum, a coauthor and Initiative staff member conducted a one-on-one, face-to-face structured interview with that leader (n = 14) about their narrative development experience. In the third year of the Initiative, two coauthors also conducted a focus group with GMCHLs (n = 7) during one of the Initiative’s monthly meetings to invite reflection on the process and impact of storytelling activities. Table 2 displays the interview and focus group questions. These feedback sessions are collectively referred to as “post-narrative reflections.”
Post-Narrative Reflection Questions
Two coauthors used NVivo software to analyze written copies of the leaders’ narratives, the interview transcripts, and the focus group transcripts, grouping segments into codes and themes (Crabtree & Miller, 1999; Malterud, 2001). We met repeatedly over the course of several months to discuss emerging themes and how best to organize and present our analysis. Our existing relationship with the leaders and with each other created a level of comfort in challenging each other’s interpretations and questioning codes and themes. Narrative and post-narrative reflection data were coded with an eye toward capturing the diverse array of leaders’ perceptions of the process and outcomes of narrative creation and intervention.
Results
This article focuses on the 14 GMCHLs’ narratives and their reflections on the narrative creation and intervention process. These participants included 11 Black women and one White woman from an urban area and two White women from rural area. Eight were single, four were married, and two were divorced. The majority (n = 10) had annual incomes below 200% of the federal poverty level. Education levels ranged from some high school (n = 2) to bachelor’s degree or higher (n = 3). All 14 GMCHLs participated in post-narrative one-on-one interviews (n = 14) and seven participated in the follow-up focus group (n = 7). In addition to developing their written narratives, these GMCHLs received and took advantage of opportunities to share their stories with more than 3,000 individuals over a period of 18 months (Table 1).
Personal Transformation Through CNI
GMCHLs’ narratives centered on traumatic experiences associated with pregnancy, birth, and new motherhood. These included infant loss (n = 6), traumatic birth experiences (n = 2), intimate partner violence (n = 3), substance use (n = 2), and economic deprivation (n = 3); some narratives contained more than one trauma. In their post-narrative reflections, GMCHLs described the personal benefits associated with crafting and sharing these narratives; these included having an opportunity to process, increasing self-awareness and self-acceptance, and prompting commitments to personal change.
“Unbottling” Feelings Associated With Trauma
Many GMCHLs described developing narratives around these experiences as a form of processing that which had been “bottled in” or buried. Veronica opened her narrative with “I am a mother of two beautiful little girls, ages three and five, they are my inspiration for what I do.” The narrative describes her “domestic violence relationship with their father” before describing her transformation to being a support for other women, noting that because of her experiences, she can now tell when another mother “tells me everything is fine, but in reality she feels like her life is hell.” In her reflection on the process of writing and sharing her narrative, she summarized, It changed me by knowing that my truth is a testimony and is better to be talked about to inspire others than to keep it bottled in to myself.
Similarly, Jessica shared in post-narrative reflections that “Writing my story helped me deal with feelings that I did not even realize I had.” Her narrative offered a vivid account of discovering that her child would be stillborn: The screen is still. His legs, arms and body are still. And so is his heart. My son was born still August 31, 2016. His heart was still and my heart was shattered into a million pieces.
Other leaders also discussed the social norms around hiding or burying pain, including Aubrey who suffered infant loss and described walking around “with my strong face on even though on the inside I was screaming.” Similarly, Pam theorized in her narrative that her pain and substance use went undetected because she “looked good on the surface.” Narratives created space to shed light on what was under this veneer.
Self-Awareness
GMCHLs also described the narrative creation process as increasing self-awareness, especially of their own progress and strength. “I realized I am strong and I can do hard things. If I made it through that, I can do anything,” Hope explained in her post-narrative reflection. Her story described the incredible effort it took to try to keep her head above water in the context of an unplanned pregnancy: I continued life as I always did: going to work and school full time, living with family. But now I was a lot more tired, hungry, always needing to use the bathroom, emotional, and still stressed and depressed about what I needed to do to make sure I could take care of my baby.
Hope’s narrative describes how she lost her job for attending her prenatal visits, spent time couch-surfing and then in a shelter, and struggled to work because of diaper needs. It concludes by taking aim squarely at state policy: “Infant mortality and the lack of resources to support mothers to have healthy babies should be a priority for everyone in our state.”
In terms of personal gains, Nancy also felt that that narrative process helped her realize she was “making progress.” In her story, she wrote, The struggle to survive affected the choices I made as mother to my other children. I was out, hustling, scamming and conning just to get the bare basics to live life. I put my children at risk daily just trying to survive.
Nancy’s narrative then describes how she found respite in a prison program that allowed her to keep her infant daughter with her during incarceration. “This was the first time I was able to build a bond with my child, the first time I felt the need to provide for her and protect her. I was able to care for my daughter without struggling to survive.” Her narrative concludes with a call for policy change to create safe, stable housing, child care, and other supports for previously incarcerated women.
Linda, who also felt that crafting and sharing her narrative “revealed to me how strong I am,” wrote a poetic account of her child’s birth, emphasizing her loss of agency at the hands of medical professionals: I wasn’t ready for my first decision as a mother to be taken away from me. . . I wasn’t ready to be told I couldn’t walk, stand or do anything that felt natural to me, due to the drugs I was given. . . I wasn’t ready to feel like spectator on the sideline of my daughter’s birth. I wasn’t ready for a life or death choice to be made for me.
She concluded by acknowledging that this experience created memories “I’ll hold on to and some I wish I could un-see” and that she moves forward “eyes wide open and focused on what’s ahead: Teaching women to advocate for themselves and sharing my experience to encourage change.”
Self-Acceptance
Some GMCHLs expressed that increased self-awareness also brought increased self-acceptance. Twanni opened her narrative by sharing that once she got married, “life started getting tough and the verbal and physical abuse progressed.” Not wanting to reach out to the “safe haven” of her mother and father, Instead, I reached out to substances abuse; it introduced me to a new way of life of escape. I never thought are even imagined I would use drugs with my unborn children and by the grace of God they weren’t addicted.
Her narrative goes on to describe the support she received and to decry the lack of support for other mothers struggling with addiction. In her post-narrative reflections, she suggests that writing and sharing her narrative “. . . allowed me to take a second to look at myself and embrace my accomplishments, defeats and struggles, knowing I’m still a work in progress.”
Similarly, Aubrey described “not feeling as guilty” and releasing the judgment of others through the narrative process. In her story, she moved step by step through the moments and days after the death of her son by positional asphyxiation, exploring each feeling—or sometimes the lack of feeling—as she and her family simultaneously navigated an investigation and his burial. Aubrey’s narrative then zooms out: Being judged and talked about by my community was a horrible feeling on top of everything that happened. Our story was in the paper—so word got out—and I will say that no matter where I went or what I did, I felt like everyone was judging me for what happened. I felt like everyone was thinking the same thing I did: that I was guilty and had caused what had happened.
In her narrative, she then shifted to focus on preventing the same pain for others, writing “. . . you don’t have to stay in the dark place where you feel like there is nothing left to live for. I am here to tell you that it does get better” before encouraging others to take risks to their children’s lives very seriously.
Commitments to Personal Behavior Change
LaDonna’s narrative recounts being called to her cousin’s home, where her newborn “died face down on an adult bed with a bib around his neck in a house filled with the stench of marijuana.” LaDonna adds, “This was another devastating, but preventable, infant death in Indianapolis.” In her reflections, LaDonna shared that creating this narrative “revealed some generational behaviors I never noticed or acknowledged. It motivated me to stop negative inherited generational behaviors with me, and not pass it down to my kids.” In fact, her narrative concludes with that commitment: “I am breaking the cycle of smoking so that it stops with me. I am laying out a healthier lifestyle for me and my three beloved children and our community.”
Other leaders also made personal commitments in both their narratives and their reflections: to volunteer work, to advocacy, and to paying more attention to their learning,
Using CNI Toward Interpersonal, Community, and Policy Change
Beyond personal benefits, many GMCHLs described in their post-narrative reflections both goals and accomplishments for narrative intervention to change others’ behaviors, increase community supports, and transform policy. For some, this advocacy became a way of honoring or making sense of their past; for example, in her reflection, Jessica shared, “I am going to be able to make Indiana a better place for moms to have babies. [My son’s] brief life will forever change the world.” GMCHLs discussions about advocacy revealed important underlying beliefs about the power of narrative to make change.
Narrative Intervention can Break Generational Cycles Through Knowledge
Berta, who received an urgent request from her “hysterical” daughter to “meet me at the hospital, the baby[’s] not breathing,” was among many GMCHL who felt that although the knowledge transmitted via storytelling, “cycles are being broken.” More specifically, GMCHLs articulated a belief that traditional methods of transmitting public health knowledge may not be as influential as hearing directly from someone who has been through a traumatic event. Aubrey, who lost her infant to asphyxiation, explained “I feel that no matter how many times you hear about the dangers, or read about the dangers it is still more impactable [sic] to hear from someone—a real life person that one may know—who has been through it than anything else.”
Twanni expressed a similar sentiment, noting that she believes by sharing her experiences with substance use as a mother and telling them about where she now provides others with a greater sense of hope: Sometimes I, you know, I tell my story to give people hope because I’ve got the experience, because the way, you know, back then in my story to where I’m at today, I don’t look like what I’ve been through in my story.
Narrative Intervention Reduces Isolation and Builds Solidarity
GMCHLs also felt narratives could help others feel less isolated and more connected. Cleo was one of two GMCHLs whose narratives focused on traumatic birth experiences, describing a context in which she felt a sense of powerlessness and fear: According to the doctor, the “good news” was that I had the option of picking whether he should try to save me or my daughter during delivery. The news caused me to become so upset that I burst out crying.
While she sought a second opinion and both ultimately survived, Cleo’s narrative is dominated by doctors’ decision-making and obscure language. “At one point, I remember at least 10 doctors standing at the foot of my bed and it was at this time that they realized that we weren’t understanding all the big words they were using, so they began breaking down the words so that we could better understand what was happening.” After weeks, she was finally allowed to take her home at 1 month old and just over 4 pounds. Cleo expressed hope that through storytelling, she could help other “young ladies” know “that they are not alone.”
Similarly, Pam, whose narrative focuses on “the pain of being consumed with smoking crack” and loneliness, took aim at both the isolation of other mothers who struggle with substance use and the policies that they need to feel supportive: We can’t allow another mother to be consumed by her addiction, lonely with no one to talk to. We must speak for them and be their voice when their addiction won’t give them a choice.
Veronica took this a step further, inviting, through the conclusion of her narrative, solidarity toward systems change: They say it takes a village to raise a child, and this is most definitely true. But it also takes that same village to stand up together, unite, and create change for the better future and development of a child and the many generations to come.
Narrative Intervention can Motivate Policymakers
While Pam and Veronica’s desires to “stand up together” or “speak for them” hint at policy change, several leaders made the policy change an explicit focus of the call to action at the conclusion of their narratives.
LaDonna and other GMCHLs expressed hope and belief that narrative could be a powerful tool to motivate decision-makers and resource-holders specifically: . . . you can give the data, you can give the statistics. But when you share those heart tugging stories, those are the pieces that sometimes helps a provider or somebody in a position of power to rethink what they might be doing or to join the initiative.
LaDonna, like others, articulated a belief that by “tugging” at the heart, narratives might be more effective than data at moving policymakers to act.
Discussion
The Grassroots MCH Initiative incorporated storytelling for personal and systems transformation to improve MCH outcomes. In line with the aims of CNI, we worked with women in marginalized communities to render their local and personal knowledge relevant to ongoing discussions about maternal and child health, create a network of social support and solidarity, and critique and recalibrate damaging and disempowering conversations on social health and well-being, with an aim of policy change with and for the zip codes most impacted by infant mortality.
Others have described a wide array of potential benefits of implementing CNI: among them, “rebalancing our intellectual scale in public health with a shifted weight toward community-based knowledge production” (Gubrium et al., 2019, p. 13) and “interrupting presumptions” (Kendrick et al., 2021, p. 41). Along the way, we learned from GMCHLs that CNI offered a host of personal and social benefits. Even as GMCHLs described harmful social norms around burying or masking grief and suffering, CNI serves as a method to “unbottle” or become more aware of suppressed feelings and experiences. As in other storytelling initiatives with women who experienced trauma (Mannell et al., 2018), GMCHLs found that storytelling created opportunities for healing and self-acceptance. It also prompted new personal commitments. While promising, we acknowledge that these findings also suggest a frightening lack of institutional support for processing grief and trauma and supporting personal growth.
GMCHLs also highlighted important ways that CNI promotes societal change. They pointed out that knowledge—especially knowledge derived from personal experience—can affect decision-making and health. They suggest that both generational patterns and isolation can be tackled through storytelling, and they challenged the efficacy of those in positions of authority but without experience to truly connect and communicate information in meaningful ways.
GMCHLs also expressed hope and faith that storytelling could push beyond decontextualized public health messaging or statistics to motivate policy change. Elsewhere, CNI scholars have described this as producing the “narrative shock” required to bring listeners “to their senses, into caring about and wanting to support the storytellers and their families” (Krause & Gubrium, 2019, p. 434). GMCHLs narratives certainly illuminate a host of systems failures—in housing, workplace accommodations, social support, reentry, substance use prevention and recovery, and beyond. Their narratives transport maternal and infant health from a statistical realm to a human one that “tugs” at our hearts; whether moves policymakers’ remains to be seen.
Situating CNI within the context of a grassroots movement that included a leadership training program, and an ongoing support structure offered a number of advantages. It gave GMCHLs the opportunity to learn from one another’s experiences with respect to storytelling, echoing findings in other contexts where such opportunities created a sense of connectedness (Bernardes et al., 2020; Marquam et al., 2020). It also facilitated the ability to offer multiple avenues and platforms for story sharing. Future scholars and practitioners may wish to explore similar structures for CNI initiatives to maximize their benefit.
The extent to which participants feel they can be honest and authentic is a key element of valid qualitative research (Lincoln & Guba, 1985). Leaders may not have felt comfortable expressing all elements of their stories or critiquing the storytelling process. We guarded against this by engaging in a long-term relationship with leaders and creating multiple opportunities for feedback, although we acknowledge that the lack of an anonymous feedback option is a weakness of the study given the potential discomfort in expressing critique.
We also did not collect data to assess the impact of narratives on other audiences. One danger is that stories inadvertently reinforce stereotypes (Wiessner, 2005). Studying listener responses in the future will be an important step toward better understanding how audience members receive and respond to narratives (Kendrick et al., 2021).
Finally, as is the case with many narrative analyses, with our limited number of participants, we know that generalizability and saturation are concerns (Saunders et al., 2018). Because our focus is state- and zip-code specific, it is possible our findings would not hold true for other participants in other contexts. Even as we acknowledge these limitations, we suggest that the narratives and reflections yield important insights for practice and policy, and we hope they inspire others to engage in similar undertakings.
Conclusion
Through the process of narrative creation, GMCHL unearthed traumatic motherhood experiences and details about their context. Situating CNI in a grassroots initiative offered opportunities for narratives to be used in settings that spanned the social–ecological model and supported GMCHLs’ personal transformation. As we continue to build this movement, we celebrate the courage of GMCHLs to engage in personal transformation while challenging systems that harm women during prenatal and postpartum periods.