
Abstract
Introduction
Early Head Start (EHS) and Head Start (HS) staff comprise a large segment of the public sector workforce and experience numerous risk and chronic factors for medical conditions or symptoms. Few health and wellness workplace interventions, however, specifically focus on EHS/HS staff.
Methods
A train-the-trainer (TTT) approach was used to build capacity among directors and staff from 57 EHS/HS programs on how to strategically plan and implement a health promoting worksite program focusing on improving nutrition and physical activity practices among EHS/HS staff. Baseline and 3-month post-training questionnaires assessed EHS/HS staff changes on knowledge and practices related to nutrition and physical activity. Paired t-tests or chi2 statistics assessed changes in questionnaire responses over time.
Results
1,363 staff from 57 programs completed baseline and follow-up surveys. Staff had high knowledge regarding healthful dietary patterns at baseline. Over one-third of staff reported drinking soda with meals and almost 50% identified soda as their most common drink. Roughly one-third of staff also reported no physical activity in the prior week at baseline. Staff demonstrated significant improvements in dietary, nutrition, and physical activity practices. Staff also improved grocery shopping behaviors.
Implications for Practice
The TTT approach to disseminate an EHS/HS staff-focused health promotion program, “Eat Healthy, Stay Active!’ provides a potentially promising strategy to build upon and disseminate more broadly to reach the over >300,000 EHS/HS staff workforce.
Keywords
Introduction
The United States faces numerous challenges in supporting and sustaining a healthy working population that is already experiencing a higher risk of developing obesity, experiencing chronic medical conditions, and dying younger with every passing year. Individuals face numerous working conditions that pose a potential health risk including longer working hours per day, low salaries, lack of autonomy, job insecurity, unsupportive co-workers, high psychological demands, and high workloads (Ewen et al., 2021; Simmons & Swanberg, 2009; Yang et al., 2015). There is overwhelming evidence that these work environment conditions, individually or collectively, are related to low job satisfaction, stress, poor sleep, burnout, functional limitations, and poor health and mental health outcomes (Britt et al., 2016; Demsky et al., 2019; Divney et al., 2019; Lopez-Martin & Topa, 2019). Furthermore, low-wage jobs often provide a higher risk of exposure to health hazards while on the job, fail to provide health insurance, and disproportionately employ persons of color and women.(Krieger et al., 2008).
The Early Head Start (EHS) and Head Start (HS) workforce experiences the clustering of several occupational risk factors for poor health outcomes including, but not limited to low salaries and high psychological demands and workloads. HS staff include managers, classroom teachers, and home-based visitors, along with family service workers, who support the development of school readiness and health for children residing in low-income households (Whitaker et al., 2013). HS programs employ close to 300,000 staff who tend to earn low wages, work under stressful circumstances, are women, and are parents of current or former HS children (23% in 2019) (Early Childhood Learning and Knowledge Center, 2019). Not surprisingly, there is evidence to suggest that HS staff have poorer physical and mental health compared with national samples with similar sociodemographic factors. Women working in HS programs were more likely to be obese, depressed, diabetic, hypertensive, and miss more work days every month due to mentally or physically unhealthy days compared with a national sample of employed women in a national sample of women of similar age, education, race and ethnicity, and marital status (Whitaker et al., 2013). The HS staff therefore represent a considerably large segment of the U.S. workforce who experience poorer health outcomes compared with national samples indicating a need for HS workplace programs to support wellness and health promotion.
There is evidence that workplace interventions are effective in promoting wellness and health for all types of employees, organizations, and sectors. Many interventions are geared at supporting healthy behaviors such as smoking cessation, physical activity, healthy nutrition, and stress reduction and have demonstrated effectiveness in reducing obesity, cardiovascular disease, musculoskeletal disorders, psychological disorders, and work absence due to sickness (Pieper et al., 2019; Proper & van Oostrom, 2019; Rongen et al., 2013). The broad components, settings, and study populations of workplace interventions, however, make it difficult to compare across studies and identify best practices and recommendations for HS staff or other groups of staff (i.e., group or individual sessions, frequency of activity) (Weinstein & Cheddie, 2021). The literature and evidence of workplace health promotion interventions for low-wage workers is scarce and almost nonexistent for EHS/HS staff making it difficult to identify best practices for program delivery, uptake, engagement, and effectiveness (Esquivel et al., 2016; Stiehl et al., 2018; Yetman et al., 2021). To that end, the purpose of this study was designed to address this knowledge gap by describing a health promotion initiative focused on supporting healthy eating and physical activity practices among EHS/HS staff and its impact on changing staff knowledge and practices.
Methods
Program Description
The Health Care Institute (HCI) uses a strategic and systematic approach to deliver health promotion training programs for EHS/HS programs across the United States to work effectively with parents, children, and community stakeholders (Herman et al., 2013). Prior trainings have addressed common childhood health conditions including oral health, child safety, managing common childhood illnesses, and nutrition and physical activity practices. Previous evaluations of the oral health and nutrition and physical activity trainings demonstrated improvements in parental knowledge, attitudes, self-reported health behaviors, and health outcomes (Dudovitz et al., 2020). In 2019, the HCI developed a new training focused specifically on delivering a health promotion program for EHS/HS staff around nutrition and physical activity practices.
Through a national application process 57 EHS/HS programs were selected based on a set of a priori criteria (participation of EHS/HS Director/Manager, Health & Nutrition Coordinator, and staff members from each program, statement of interest, reasons for applying and seeking participation). Teams were invited to commit to a 4-year program focused on delivering health promotion around the topics of oral health, sleep, and common childhood illnesses. The fourth year of the program focused on building specific knowledge and skills related to supporting healthy nutrition and physical activity practices for staff. Two to four staff from each of the 57 programs attended a 3-day virtual training due to the COVID-19 pandemic. The goal of the training was to increase knowledge and practices related to obesity and chronic disease prevention among HS staff at their respective sites to support their own knowledge and behavior changes, and in turn, also support similar changes among children and families.
A pretraining webinar was conducted on July 13, 2020, that provided an overview to the core curriculum, “Eat Healthy, Stay Active!” (EHSA). It also provided an opportunity for participants to view and become more comfortable with the online training platform. During the 3-day EHSA Obesity and Diabetes Prevention training, participants learned how a healthy lifestyle can prevent obesity and diabetes. The low-literacy curriculum of EHSA focused on basic concepts such as My Pyramid, food groups, portion control, shopping on a budget, and integrating physical activity into daily life. The curriculum was developed by the HCI team and then reviewed by the California Family Health Council (http://www.healthed.org/consulting). Participants gained knowledge on MyPlate, the current nutrition guide published by the United States Department of Agriculture Center for Nutrition Policy and Promotion, and other topics such as healthy eating & shopping on a budget, the importance of an active lifestyle and exercise, and mindful eating. The “Eat Healthy, Stay Active!” core curriculum and accompanying activities was provided to all of the programs, and the University of California, Los Angeles–based leadership team trained HS staff over the three virtual trainings and provided technical assistance for the programs.
Program Dissemination
During the training, a systematic approach was used to build leadership and workforce engagement around nutrition and physical activity strategies using a TTT model. This approach included (a) development of a coordinated and strategic plan to promote healthy nutrition and physical activity practices for staff; (b) practical strategies to increase motivation and buy-in; (c) learn and apply adult learning principles and effective and interactive delivery techniques; (d) a roadmap to guide goals, planning, and actionable steps; (e) a budget plan; and (f) modeling a mock session using power point slides, handouts, and examples of hands-on-activities for effective implementation of staff training. Examples of hands-on-activities included cooking demonstrations focused on preparing healthy meals; making substitutions for commonly eaten foods; introducing children to fruits and vegetables; healthy shopping on a budget; exercising using common kitchen items; and balancing energy intake with exercise. After the virtual webinar trainings, each program had the flexibility to determine when the trainings would be delivered and what reinforcement activities would be used for staff and also received ongoing content and support to reinforce nutrition and physical activity strategies for staff. Flexibility on the implementation strategies was intentional in order for each program to best meet local needs and cultures while aligning the activities with required federal HS Program Performance Standards. Each team program trained staff during August 2019 and September 2019, and the activities to reinforce the training topics occurred during October 2019 and November 2019.
Measures and Data Collection
Baseline assessments of knowledge and eating and physical activity practices were completed using a paper questionnaire immediately before staff received any training or content at their respective sites, and repeated 3-months after the training. The questionnaire was developed by the study team with attempts to keep all items no higher than a sixth-grade reading level to measure nutrition-related knowledge and eating and physical activity practices. The questionnaire has no formal validity testing, but did undergo iterative changes based on an informal assessment with a convenient sample and has been used in a previous pilot study with Women, Infants & Children Program Staff (Herman et al., 2012). Questionnaire items were grouped into several subtopics and included: knowledge on healthy food choices and the relationship between food choices and chronic health conditions, as well as practices related to nutrition, eating, grocery shopping, and physical activity.
True or false statements were used to assess knowledge on healthy food choices such as, “A baked potato is a healthier choice than french fries.” Response options included, “True,” “False,’ or “Don’t Know” and were scored 0 based on an incorrect or don’t know response, and 1 for a correct response. The questionnaire also included four items to assess knowledge on the relationship between food choices and chronic health conditions. Staff participants were asked to mark “True,” “False,’ or “Don’t Know” after reading a statement such as, “A high fat diet can lead to heart disease.” Each correct answer was scored as 1, and an incorrect or don’t know answer as 0.
Grocery shopping practices were assessed by three questionnaire items. Staff were asked to respond “yes,” “no,” or “sometimes” to the following statements: “I make a grocery list before I go shopping”; “I compare prices in the grocery store to save money”; and “I try to buy fruits and vegetables that are in season.” Responses were scored 1 if a “yes” was marked and 0 if “no” or “sometimes” was marked.
Staff were also asked to answer eight items related to eating practices such as consumption of sugary beverages with meals, preparation of meals, and fast food intake. For example, staff were asked, “During my meal, I add salt to my food.” Response options included “yes,” “no,” or “sometimes.” Responses were scored 1 if a “yes” was marked. Nutrition practices were assessed by asking staff 11 items related to the intake of specific food groups per week. For example, staff were asked, “During the past week how often did you have fruits (fresh, frozen, or canned)?” Response options included “never or less than one time per week”; “two to four times per week”; “five to six times per week”; or “seven times or more per week (everyday).” Finally, to assess physical activity practices, staff were asked to indicate the number of days per week, and duration of time per day dedicated to physical activity. Categories for all practices were collapsed to approximate the dietary practices recommended by the Dietary Guidelines for Americans, ease of interpretation, and the literature on fast-food and sugar-sweetened beverages (Chen et al., 2021).
Data Analysis
Descriptive statistics were generated for all the questionnaire items. Differences in baseline values were examined for staff with and without follow-up data using. A total of 140 staff from four programs did not have follow-up data either because a participating program experienced lead staff turnover or changed leadership. Among those with both baseline and follow-up questionnaires, paired t-tests for items with continuous outcomes and chi-square tests for items with categorical responses were completed to evaluate for differences in baseline and follow-up assessments. All analyses were conducted in STATA (version 15, StataCorp.).
Results
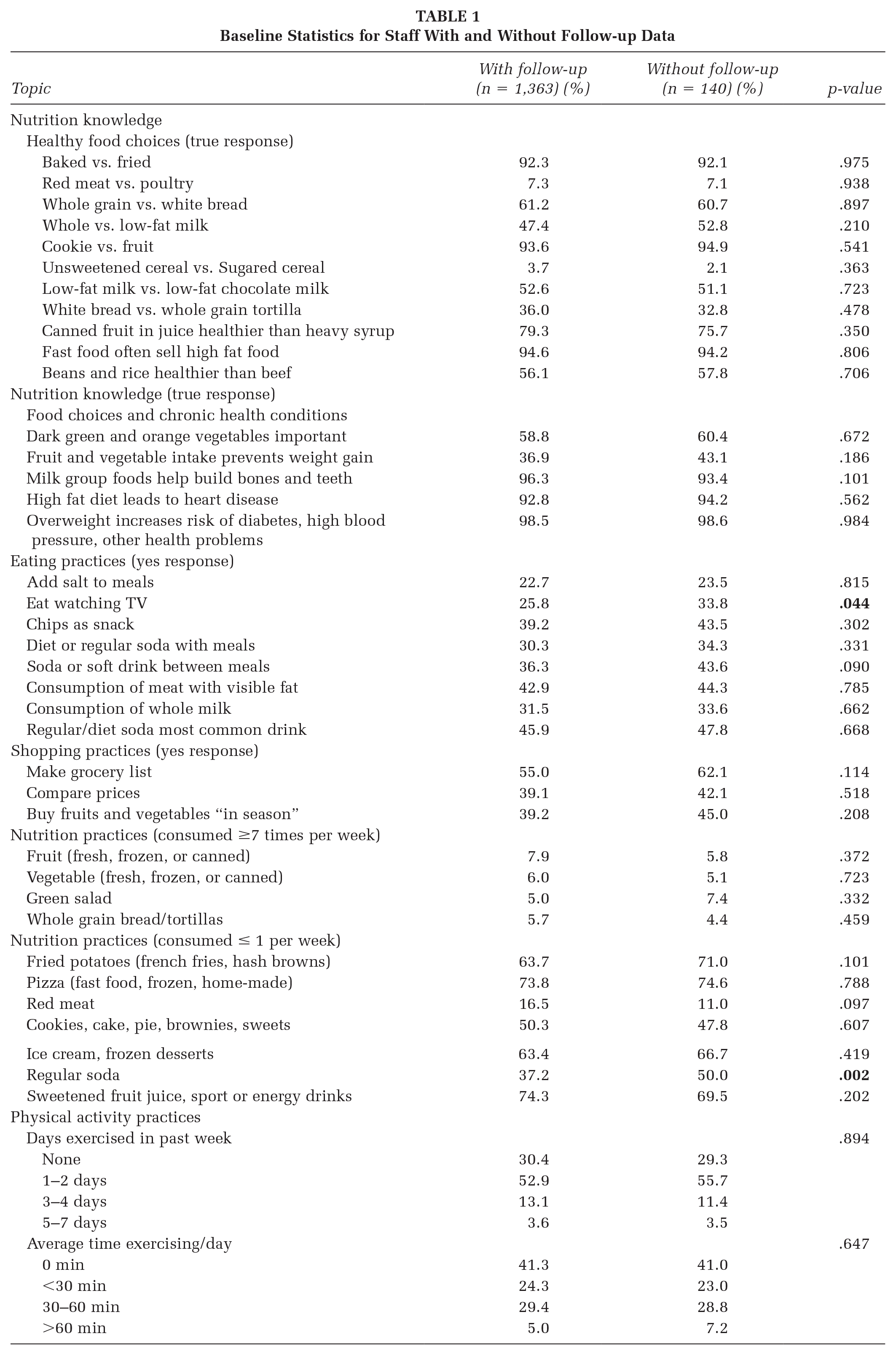
In total, 1,503 staff from 57 programs completed baseline surveys and a total of 1,363 staff completed both baseline and follow-up surveys (90% follow-up rate) (see Table 1). Staff lost to follow-up were slightly more likely than those with follow-up data to report eating while watching television (34% vs. 26%), and drinking one or no soda per week (50% vs. 37%) (Table 2). There were no other significant differences in baseline assessments between staff with and without follow-up data.
Baseline Statistics for Staff With and Without Follow-up Data
Change in Staff Knowledge and Practices From Baseline to Follow-up (n = 1,363)
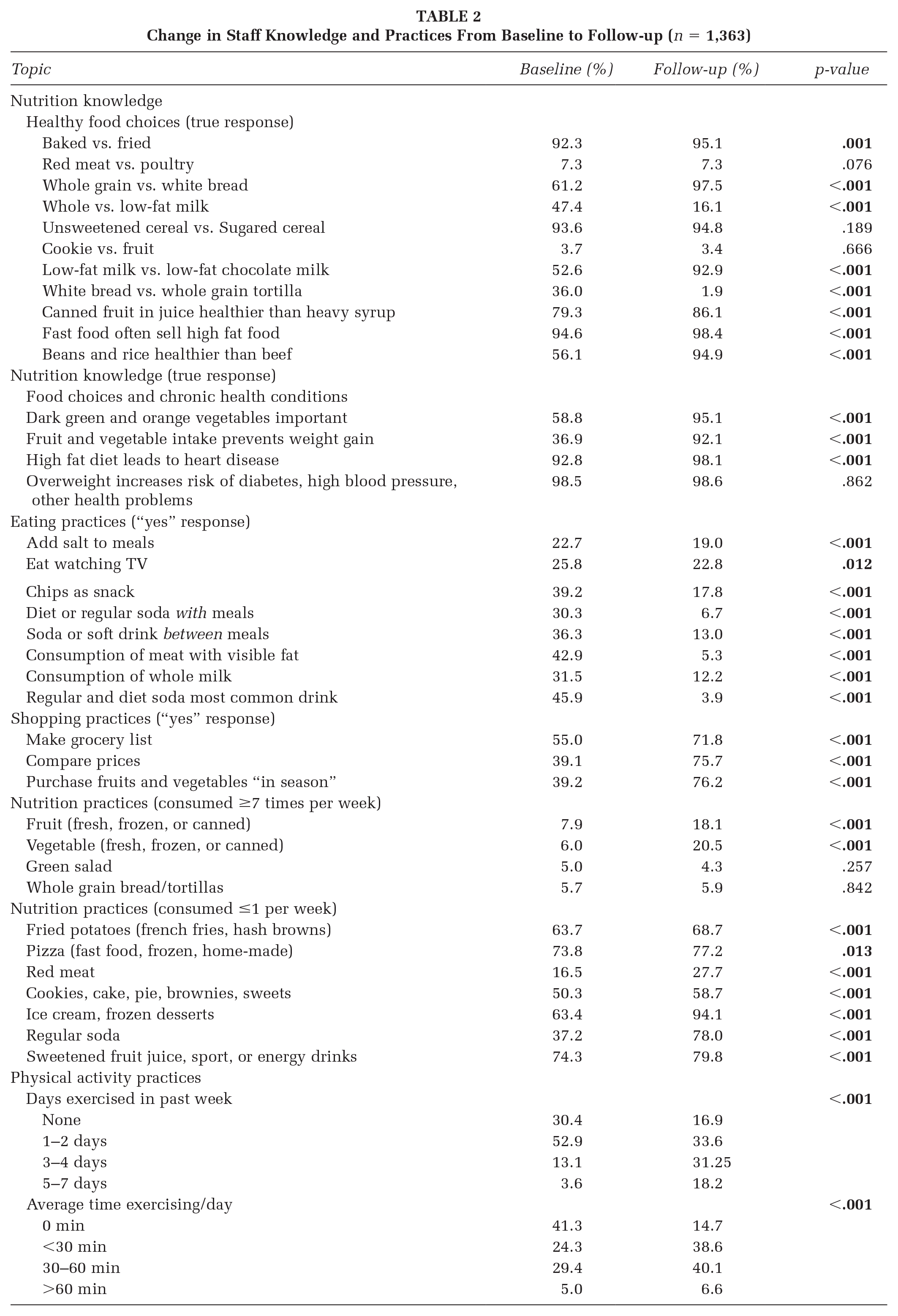
At baseline, staff had relatively high knowledge on differentiating a more healthful option when presented with two food options. Over 90% of staff were able to correctly identify the more healthful option between baked food versus fried food, red meat versus poultry, and unsweetened versus sweetened cereal and canned fruit. A smaller number of items were noted to have large improvements between baseline and follow-up, and included those items related to identifying a more healthful option between common milk varieties and a comparison of beans and rice versus beef. In regard to the knowledge items about the relationships between specific food choices and health conditions, many staff were knowledgeable about the harms of a high-fat diet and cardiovascular disease at baseline. The biggest change from baseline to follow-up was related to the knowledge of fruits and vegetables being important sources of nutrition to prevent weight gain.
Significant shifts between the baseline and follow-up period were noted for all three of the grocery shopping practices. Staff reported an increase in making grocery lists, comparing prices, and purchasing fruits and vegetables “in season.” Many of the items related to staff eating practices had significant changes between the baseline and follow-up period. The eating practices with the highest changes were related to sugary beverage intake, with fewer staff practicing soda intake between meals and with meals. Staff also reported significant changes in consuming daily fruit and vegetables (8% vs. 18% and 6% vs. 20%, respectively) at follow-up. Improved nutritional practices were also noted in the reduction of ice cream and red meat at the time of follow-up. Finally, there was an overall pattern of improved frequency of exercise in the prior week, and an increase in the average time spent exercising every day at the time of follow-up.
Discussion
A TTT approach was used to disseminate a staff-focused health promotion program, “Eat Healthy, Stay Active!’’ to over 1,300 EHS/HS staff across 24 programs in 21 states from diverse regions of the country. This approach was used to build capacity among a small number of leadership and staff members from each program that focused on integrating implementation strategies with nutrition and physical activity knowledge and behavior-changing strategies, who in turn delivered and engaged staff from their respective program. Evaluation of the program shows that staff had relatively high knowledge on basic nutrition and food concepts at baseline, and the biggest gains were changes in eating, nutrition, grocery shopping, and physical activity practices at the time of follow-up. These findings suggest that a TTT approach can be used to support health promoting practices among EHS/HS staff who may experience risk for chronic health conditions due to a workforce that is largely comprised of low wage earners, non-White women, and stressful circumstances and environments (Paschall et al., 2020; Snyder & Hill, 2018).
The EHS/HS workforce, therefore, stands to benefit from worksite wellness and health promotion programs. Despite the likely large return of investing in such programs, to our knowledge, there is only one other documented intervention that has exclusively focused on EHS/HS staff health and wellness (Yetman et al., 2021). The program included 178 HS teachers and support staff, and supported health education, health promotion, and behavioral change technologies such as an iPhone App over a 10-month period. After the intervention, the majority of participants reported making healthier lifestyle choices including decreasing sugary beverages, increasing physical activity, and increasing water consumption. Our EHS/HS staff health promotion program was able to produce similar changes with staff reporting a reduction in soda intake, an increase in fruit and vegetable intake, and an increase in physical activity. Future health promotion interventions should consider an ongoing focus on decreasing sugary-sweetened beverages given these collective results and the high prevalence of soda intake among the U.S. population (Park et al., 2016; Zagorsky & Smith, 2020) and the evidence to suggest that this dietary practice may be higher among EHS/HS and child care center staff (Sharma et al., 2013; Ward et al., 2018).
EHS/HS staff were largely well-versed on basic nutrition and food concepts even at baseline. These findings related to nutrition knowledge have not typically been described among EHS/HS and other early childhood education and care teachers. These differences are likely explained by some of the differences in the style and type of questions used across studies. In our evaluation questionnaire, EHS/HS staff were asked to select the more healthful option between two foods, whereas other studies may commonly use highly specific questions related to servings, percentage of calories from fat, and portion sizes to assess nutrition knowledge (Rapson et al., 2020; Sharma et al., 2013). It is plausible to suspect that EHS/HS staff may be highly knowledgeable on dietary patterns, and less so on the specific foods, nutrients, and amounts recommended by national and professional dietary guidelines. Future studies may consider including a combination of such questions to assess knowledge, particularly in light of recent changes and updates to the 2020–2025 American Dietary Guidelines and the 2021 American Heart Association Dietary Guidelines that have moved in a direction to make guidelines easier to understand, practical, and easier to implement (Lichtenstein et al., 2021; U.S. Department of Agriculture and U.S. Department of Health and Human Services, 2020).
EHS/HS staff also reported an increase in the frequency of physical activity as a result of the “Eat Healthy, Stay Active!’’ health promotion program. These findings mirror the results from Yetman et al. (2021) and add to the evidence that workplace interventions can increase the frequency of physical activity (Proper & van Oostrom, 2019; Song & Baicker, 2019). Although there may be far less evidence that workplace physical activity interventions can impact obesity, biomarkers, medical spending, or other clinical outcomes, there is stronger evidence for the prevention of musculoskeletal disorders and symptoms through workplace interventions focusing on exercise and physical activity programs (Reif et al., 2020; Song & Baicker, 2019). Given this evidence, to push the field of workplace interventions forward that target physical activity among EHS/HS staff, an evaluation component of musculoskeletal pain and discomfort should be considered as close to 40% of HS staff experience lower back pain, almost twice as common as U.S. women who have similar demographic characteristics (Whitaker et al., 2013).
This study has several limitations to consider. The use of self-reported data may limit our results due to recall and social desirability bias. In addition, it is unknown whether participating EHS/HS programs and staff are representative of the larger EHS/HS community. In addition, it is possible that other parent and child training may have reinforced staff’s changes in knowledge and dietary, nutrition, and physical activity practices. We are also unable to assess what components or activities were most effective in driving the observed changes in knowledge and practices, and whether these changes were sustained long-term. Finally, it is unknown whether the changes in self-reported practices are associated with weight maintenance or loss, stress reduction, or improvement in other physical and psychological conditions or symptoms.
Implications for Practice
The TTT approach to disseminate an EHS/HS staff-focused health promotion program, “Eat Healthy, Stay Active!,” provides a potentially promising strategy to build upon and disseminate more broadly to reach the over >300,000 EHS/HS staff workforce. Potential next steps to push this intervention work forward can include establishing the validity of the questionnaire in measuring nutrition-related knowledge and eating and physical activity practices. Future directions may also include evaluating the effectiveness of the health promotion program through implementation among non-EHS/HS child care workers to determine whether results can be replicated. In addition, evaluation of long-term effectiveness of the program is important to determine whether eating, nutrition, grocery shopping, and physical activity practices are sustained at 6 and 12 months after participation.
There is a great need for additional EHS/HS workplace health intervention studies given the dearth of available studies, but a workforce that experiences multiple and chronic risk factors for poor physical and mental health conditions. A continued focus on dietary, eating, and physical activity practices is needed as they have the biggest impact on health and can be supported in the workplace.