
Abstract
Objective
To identify effective methods for local public health departments to secure policy and systems changes that will achieve health equity and improve health outcomes across diverse populations.
Methods
We reviewed 220 documents from a philanthropic initiative that funded collaborative efforts to improve conditions for health and equity in 14 California communities from 2010 to 2020. We examined the role of factors associated with movement-building approaches—such as organizing, base-building, investing in organizational capacity, and forming alliances—in securing policy and systems changes that foster more equitable community conditions.
Results
All 14 sites made progress in implementing policies and systems to improve the social determinants of health, including neighborhood conditions and the built environment, health care access, social and community context, economic stability, and education access. All 14 also shifted processes to be more inclusive of and responsive to community members, who in turn gained capacity to advocate for change and build collective power.
Conclusion
Local public health leaders can make progress toward health equity by drawing on movement-building approaches to change policies and systems that affect social determinants of health.
Keywords
Background
Public health has a long and rich history of engaging with community activists to respond to pressing health threats. From enforcing workplace safety standards to building protections into consumer products such as gun-safety locks and car-safety seats, public health practitioners have successfully influenced policies, upheld regulations, and transformed systems to improve conditions for population health (Fairchild et al., 2010; Wafer & Carruth, 2003; Westly, 2022).
Recognizing the profound and unjust health impacts of inequities that permeate our societal systems, leading public health entities, including the World Health Organization (WHO), Centers for Disease Control and Prevention, and National Academy of Medicine, have named health equity as a central goal. Health equity means that everyone has a fair and just opportunity to attain their full health potential and that no one is disadvantaged, excluded, or dismissed from achieving this potential (Braveman et al., 2017). In response, local and global public health leaders are re-evaluating how they address the social determinants of health—the wider set of forces and systems, including the economic policies, land-use and environmental policies, social norms, social policies, and political systems that shape the conditions of daily life (WHO, n.d.). Black and Latino U.S. residents, for example, bear 56% and 63% excess exposure to fine particulate matter (PM2.5) pollution relative to their consumption of goods and services (Tessum et al., 2019). Linked to slowed lung-function growth and asthma in children and increased illness and death from heart and lung diseases (California Air Resources Board, n.d.), this PM2.5 “pollution burden” stems from decades of differential land-use policies and zoning rules that sited environmentally hazardous industries and major highways in Black and Latinx neighborhoods, and prioritized investments in parks and green space in suburban residential White communities (Prevention Institute, 2016). Taking such systemic inequities into account in its monograph on the social determinants of health, the WHO states that, “any serious effort to reduce health inequities will involve changing the distribution of power within society to the benefit of disadvantaged groups” (Solar & Irwin, 2010, p. 22).
To achieve equity, we must address inequitable social, physical, and economic conditions that shape community environments—factors that drive elevated rates of illness and injury—and challenge the decisions, decision makers, policies, and practices that create and perpetuate inequitable conditions. This means addressing power imbalances, social and political hierarchies, and norms and values that perpetuate racism, discrimination, and exclusion. Yet addressing the societal distribution of power is not a core focus of public health training nor is it something the public health sector can do alone. Sustainable changes require local, democratic participation.
Public health can learn from community health initiatives that address systemic health inequities (Institute of Medicine, 2014) through movement and power building, such as the Building Healthy Communities (BHC) Initiative, a 10-year, US$1 billion effort launched in 2010 by The California Endowment, California’s largest private health foundation. The goal of the BHC Initiative was to advance local and state policy that would support health equity, as well as promote a narrative of empowerment for communities affected by long-standing health inequities. The initiative supported local participation and advocacy in policy and systems changes to transform deeply inequitable health conditions in 14 California communities in rural, suburban, and densely populated urban areas across the state (see Table 1). During the initiative, the funder and its partners grew increasingly explicit about the critical nature of power building and community organizing to achieving health equity (Pastor et al., 2018).
Building Healthy Communities Sites
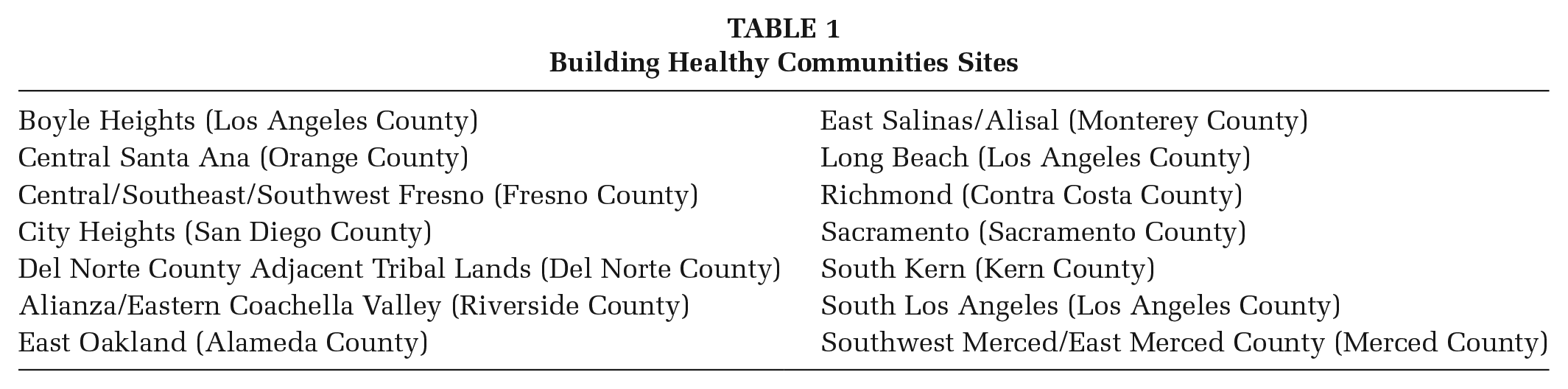
The 14 BHC communities varied greatly in terms of geography, demographics, and political orientation. In communities with large immigrant populations—whether Latinx, East African, or Southeast Asian—the work proceeded in multiple languages. Sites also differed in terms of experience with advocacy and community engagement, with some communities having an array of active community-based organizations and others having little history of resident engagement, few nonprofits, and resistance from policymakers to residents exerting power over local decision-making processes. As such, the 10-year initiative provides a unique case example for those interested in exploring how a portfolio of movement-building strategies interact with different community contexts to support more equitable health outcomes and more equity-oriented processes.
Purpose
This article identifies lessons for local public health leaders who seek to achieve health equity and improve health outcomes across diverse populations. Specifically, we explore methods employed by the 14 BHC communities to create a healthier policy landscape over the course of the 10-year initiative. We define a healthy policy landscape as one in which local policies and systems, and the procedures and decision making that inform them, are designed to provide every community with fair and just conditions that support all residents to thrive.
Recognizing that it takes generations—or longer—to reverse entrenched health inequities, we identify and highlight interim accomplishments that might signal progress toward long-term health equity and help public health practitioners to identify promising strategies. Our hypothesis was that the BHC Initiative’s movement- and power-building orientation helped change local conditions over the course of the initiative to become more conducive to and supportive of community-identified health equity priorities—resulting in a healthier policy landscape.
Method
We conducted a literature scan to understand how movement- and power-building strategies have been employed in community health and other social change initiatives to advance equity-focused policy and systems change. Drawing on the scan, we created a framework that connects movement-building approaches to community health initiatives and used it to analyze documents describing the work at BHC sites. Document reviewers were trained to use the framework as a coding tool and met periodically during the review process to assure intercoder reliability.
We reviewed 220 documents from the BHC document library, including reports summarizing each site’s activities, accomplishments, and challenges, and educational and promotional materials developed by the sites themselves. We also reviewed initiative-wide reports and evaluations that summarized efforts at multiple sites and synthesized emerging lessons from the initiative. Document reviewers used an inductive approach, identifying patterns, commonalities, and differences across the sites’ efforts, and using them to develop general observations or themes about the movement-building strategies employed by BHC sites and the impact of community contexts on sites.
As part of our document review, we tracked policy and systems changes from 2011 to 2020 to understand the extent to which active participants within the BHC initiative were furthering a healthy policy landscape by removing obstacles to health—such as poverty, discrimination, and their consequences including powerlessness and lack of access to good jobs with fair pay, quality education and housing, safe environments, and health care. We grouped policy changes into five categories in alignment with the Healthy People 2030 Social Determinants of Health domains—neighborhood and built environment, health care access, social and community context, economic stability, and education access and school climate (Healthy People 2030, n.d.).
Results
Policy and Systems Changes to Improve Health: “The What”
External evaluators documented more than 1,500 distinct changes in policy, systems, and the physical environment that were tracked and reported by BHC sites and their local partners (Center for Outcomes Research and Education, 2021). Priorities across sites varied—from environmental and immigrant justice to affordable housing, supportive schools, and justice system reform. Across all 14 sites, there was evidence of local policy changes addressing BHC priorities (Table 2), which at times led to efforts to secure regional and statewide policy changes as well. In some cases, these issues aligned directly with the social determinants of health, like regulating environmental hazards and adding sidewalks. In others, the collaboratives took on community concerns that are typically seen as outside the health sphere—such as alternatives to incarceration (Acker et al., 2019)—that have a significant bearing on life outcomes and access to opportunities that influence individual, family, and intergenerational health status.
Examples of Policy and Systems Changes in BHC Communities Mapped to Social Determinants of Health
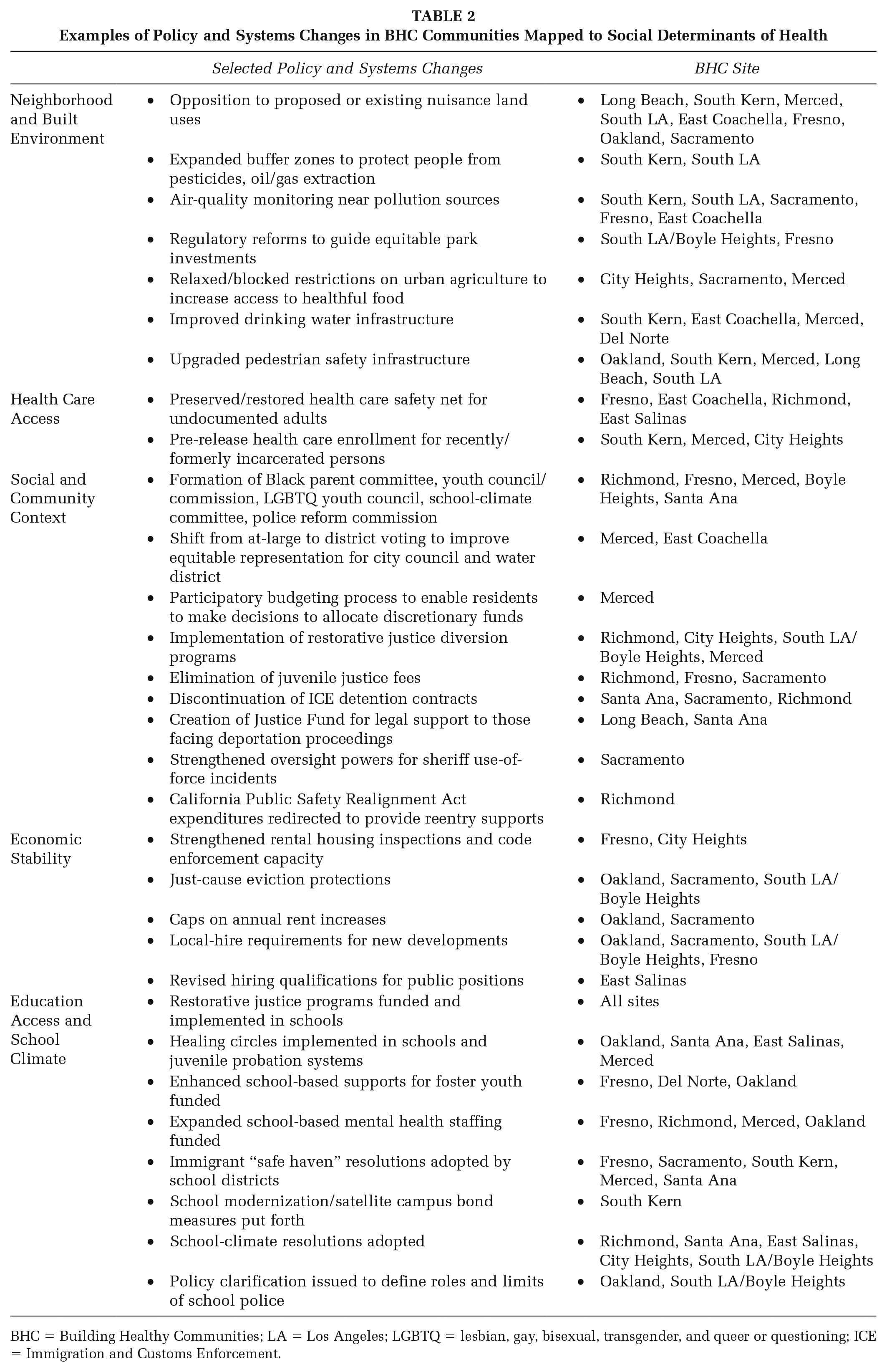
BHC = Building Healthy Communities; LA = Los Angeles; LGBTQ = lesbian, gay, bisexual, transgender, and queer or questioning; ICE = Immigration and Customs Enforcement.
Changes to Neighborhoods and the Built Environment
All 14 BHC sites made progress in improving the neighborhood conditions and addressing the built environments where people live, work, and play. Breathing polluted air and having limited access to parks and other safe spaces for physical activity can increase the risk of illness and injury. Alternatively, having easy access to healthy food and public transportation can reduce the risk of disease. Eight BHC sites focused on combating toxic land uses, and six BHC collaboratives won regulatory reforms to guide park investments to communities of greatest need and loosen or block restrictions on urban agriculture.
Improvements to Health Care Access
BHC advocacy generated civic support for new public investments to improve health care coverage. Early on, stemming from passage of the Affordable Care Act, sites focused on enrolling uninsured residents in the state’s Medicaid program. Later, some communities shifted to expanding coverage to undocumented immigrants and incarcerated people awaiting release. Some political environments were more hostile to health care and immigration reform; those sites worked to build a base of support and educate the public to secure county-level coverage for undocumented adults.
Impacts to the Social and Community Context
As a social determinant of health, social and community context covers a broad range of topics, including level of civic participation (Healthy People 2020, n.d.), extent of social connection (Holt-Lundstad, 2021), and rates of incarceration (Kruger & De Loney, 2009).
All BHC sites had success in strengthening social conditions, increasing civic participation, or securing reforms that reduced contact with Immigration and Customs Enforcement (ICE) and the criminal justice system in marginalized communities. Community members gained representation on public committees and decision-making boards, influenced the creation of new advisory groups, and replaced at-large voting structures that had prevented political representation for neighborhoods and groups battling health disparities.
Improved Conditions for Economic Stability
Economic insecurity, including poverty, unemployment, and housing instability, increases risk of illness and injury through direct and indirect pathways (Khullar & Chokshi, 2018). Most work by BHC collaboratives in this arena related to housing, such as capping annual rent increases and restricting no-fault evictions, as well as expanding rental housing inspection and code enforcement. Several BHC collaboratives also extended fair employment practices, such as revising hiring qualifications for city positions.
Increased Education Access and Changes to School Climate
Youth and parent advocates across BHC sites changed school discipline policies. Districts adopted restorative and trauma-informed approaches to support healing and alternatives to punishment. School-climate resolutions were adopted by districts in six places, and collaboratives moved school districts to reallocate funding toward foster youth and mental health supports. Five BHC sites took non-cooperation stances on immigration enforcement by designating schools as safe havens.
Means of Achieving Policy and Systems Change: “The Who and the How”
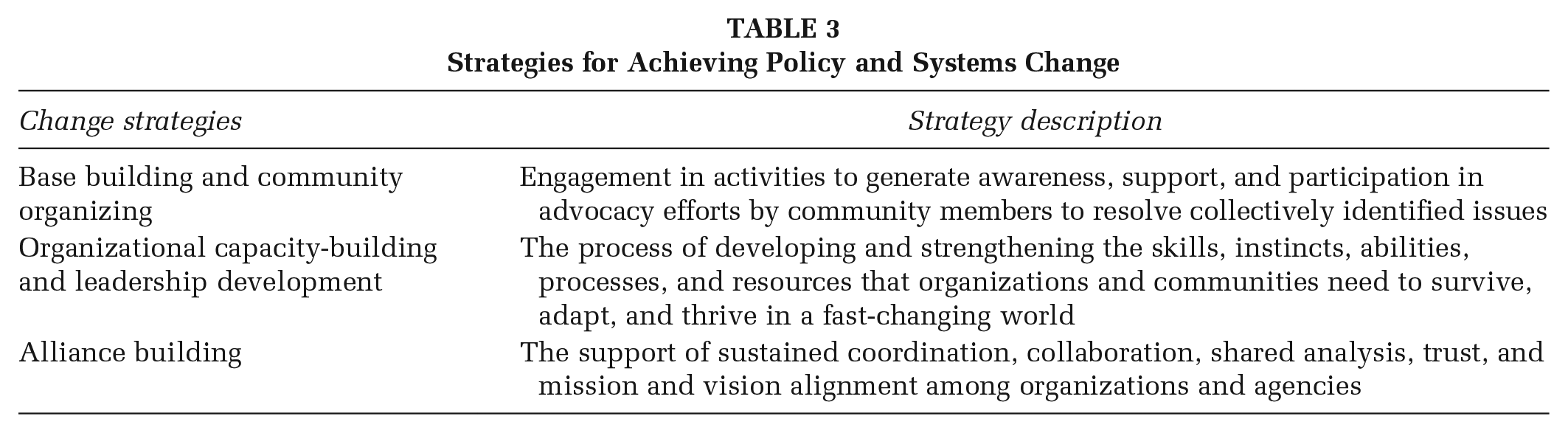
BHC sites deployed movement-building strategies, including base-building and community organizing, organizational capacity-building, leadership development, and alliance-building to influence policies and practices and change community conditions (Table 3).
Strategies for Achieving Policy and Systems Change
Base Building and Community Organizing
Base building and community organizing galvanize community awareness, support, and active participation in advocacy efforts, with the goal of increasing community power over decision making to resolve collectively identified issues. In addition to building public will, base-building efforts often engage youth in advancing solutions to the inequities their communities face, and directly support their own healing—using organizing as a strategy for individual and community-wide health (Jimenez et al., 2019).
Where possible, local BHC grantees drew on existing grassroots support, and every site worked to galvanize and expand community engagement through, for example, community events and meetings in multiple languages. Santa Ana and Del Norte each conducted outreach meetings to familiarize community members with their community initiatives and shape priorities. In City Heights, house meetings in numerous languages helped build networks. Community events like Noche Familiar (East Coachella) and the Richmond Youth Summit provided unique opportunities for people to come together, while connecting residents to organizing opportunities.
Some BHC sites located in communities that had not had high levels of community and resident engagement with government agencies and policymakers prior to the BHC initiative succeeded in increasing community participation in policy advocacy. Sites’ organizing efforts resulted in coordinated advocacy that shifted local policymakers’ expectations and, in some cases, receptivity to resident priorities. In Merced, the BHC site cultivated advocates from adjoining unincorporated areas—a place where policymakers and government agencies were not used to community input and were resistant to it. As resident participation grew, government leaders evolved to expect community input and advocacy as a normal part of the process; public meeting times and locations were shifted to be more accessible to working residents, with materials translated into Spanish.
Organizational Capacity-Building and Leadership Development
BHC efforts included education, training, and technical assistance in areas such as the relationship between community conditions and health equity; the basics of community organizing; and how to pursue policy and systems changes. Each site organized trainings based on specific needs of local youth, residents, and advocates, engaging the expertise of community organizers, policy-focused organizations, and research partners to support capacity-building. Trainings on trauma-informed and racial-justice approaches were a particular focus, as was investment in youth and resident leadership. In South Kern, Cal State University Bakersfield’s Center for Social Justice provided ongoing policy training and technical assistance. In Sacramento, community-based organizations rooted in the Black, Latinx, and Southeast Asian communities expanded their focus from service provision to active engagement in local policy advocacy. In Salinas, BHC helped establish the Resident Organizing Leadership Academy, with the goal of moving residents up a “leadership ladder” and into decision-making roles on local advisory boards governing zoning decisions, water systems, and other policy areas.
Alliance Building
Alliances between community-based organizations, statewide nonprofits, and government agencies played an essential role in BHC successes. The process of building and strengthening these alliances involved reconciling dissimilar norms for meeting routines, decision-making processes, advocacy tactics, and tensions over turf, as well as coming to shared understandings on racial equity framing. Healing practices implemented at trainings were adopted to manage conflict within these tables, and to sustain the well-being of staff and participants.
In many places, grassroots organizers challenged BHC site staff to better communicate with community members in determining priorities and maintaining accountability, which eventually led to committee structures that included more resident and youth representation, and meetings planned around needs and preferences of lay participants. Most collaboratives reorganized more than once during the BHC time span to shift strategy and organizing decisions toward nimbler “action” teams driven by community and issue advocates. These power shifts helped groups work more effectively, increased accountability, and enabled advocacy to be confrontational when needed.
Discussion
All 14 communities demonstrated progress toward a healthier policy landscape in which the terrain of local policies and systems shifted: policy-development processes became more inclusive of residents most affected by health inequities; community residents, youth leaders, and representatives of community-rooted organizations gained capacity to advocate for systemic changes and built collective power; and policy- and systems-change priorities were designed to foster more equitable community conditions. Taken together, these accomplishments demonstrate progress toward health equity.
Drawing on the results of this research, we developed the “Framework for Community-Based Movement Building for Health Equity” (Figure 1) that connects health-oriented policy and systems changes with movement- and power-building strategies that have generated improvements in social justice and civil rights movements. This framework can be used by local health department leaders, health-related funders, and communities to link the “who and how” of community-driven advocacy strategies with the “what” of policy- and systems-change solutions. Our research supports the understanding that both elements are necessary to build power, change systems, and achieve more equitable community conditions that support health, safety, and well-being.
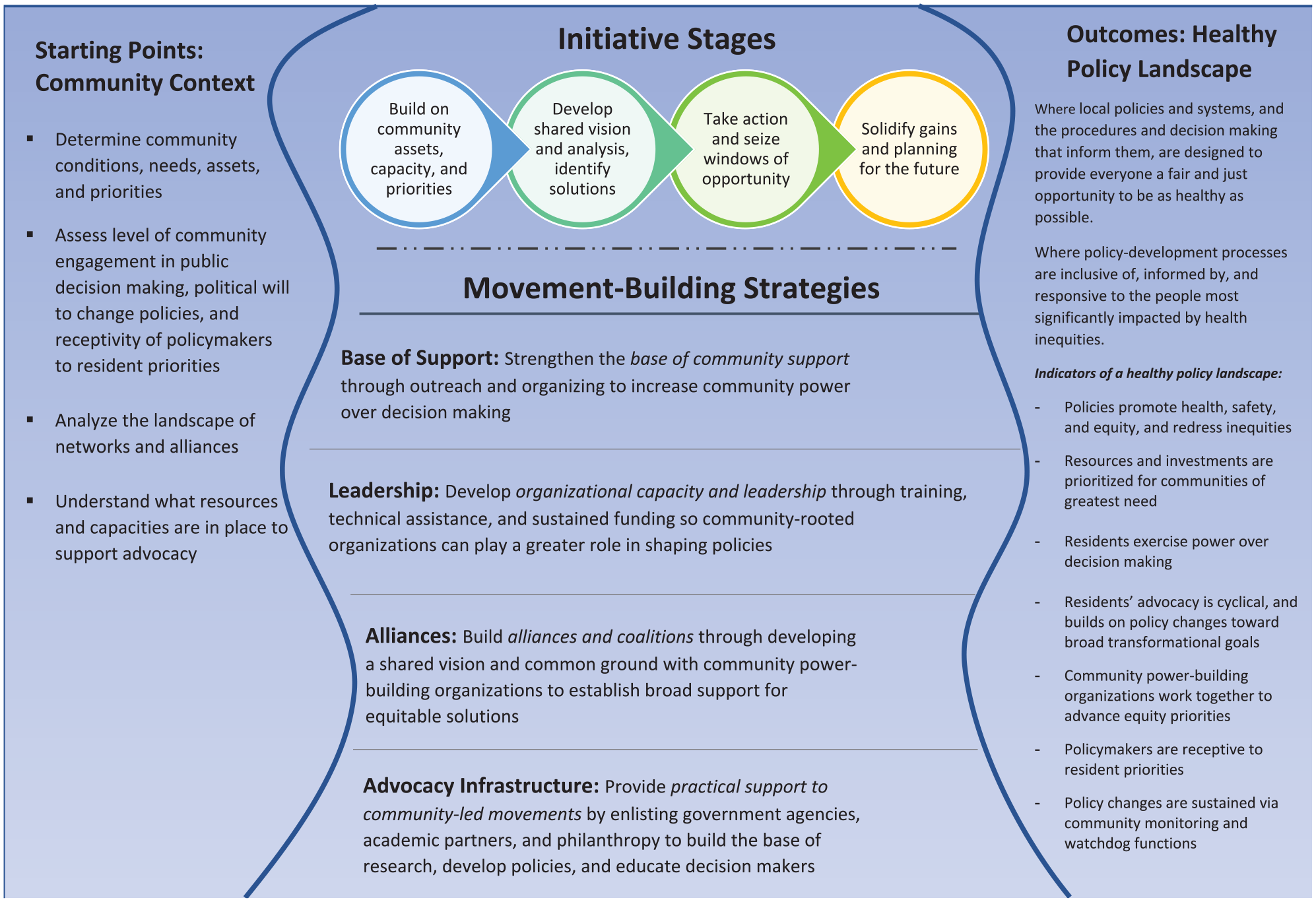
Framework for Community-Based Movement Building for Health Equity
The role of public health in lending support to community-led movements represents the leading edge of public health practice (Orr et al., 2021). Despite a relative paucity of peer-reviewed research, many groups representing and working in close alignment with public health, including the National Association of County and City Health Officials, National Academies, Bay Area Health Inequities Initiative, and Government Alliance on Race and Equity have named a set of practices, levers, and internal changes to complement the organizing and advocacy efforts of community-based organizations, residents, and youth leaders (Bay Area Regional Health Inequities Initiative, 2020; National Academies of Sciences, Engineering, and Medicine, 2017; National Association of County & City Health Officials, 2014; Nelson & Spokane, 2015).
One way for public health to demonstrate support to community and resident leadership is to show up for meetings and events when asked to by community representatives, without having to lead the agenda. When public health staff participate in coalitions or collaboratives with community members, they can make space for residents and youth to identify root causes of inequities and have equal (or greater) power in determining priority policy solutions (Wolff et al., 2017). Public health departments also can re-examine contracting procedures to prioritize funding to smaller, community-rooted organizations with experience organizing residents and building resident leadership.
Core functions of public health—data collection and assessment, communications and education, and policy development—can be helpful to community equity work. For example, public health plays a valuable role in “shifting the narrative” when it educates nonhealth sectors and policymakers in how systemic inequities and community conditions create and perpetuate racial and health inequities (Minkler et al., 2019). Through published reports and public testimony, public health leaders can help elevate the health impacts of key policy decisions, supply relevant and timely data, and urge elected officials and agency leadership to act. Some health departments have mobilized their data analysis capacity to support community partners, such as making GIS (Geographic Information Systems) mapping specialists available to community organizations to help map neighborhood data that residents have gathered (Sims et al., 2018).
Other local health departments have worked to center health equity internally by embedding equity goals into strategic plans required for accreditation, organizational budgets, engagement processes, and evaluation plans (Nelson & Spokane, 2015). Capacity-building programs such as the Government Alliance for Racial Equity have been used to create greater institutional momentum and capacity for addressing racial equity within local governments and health departments (Nelson & Spokane, 2015). In addition, some departments have established leadership academy programs for youth and residents to build civic engagement skills (Sims et al., 2018).
Limitations
This study is limited to a review of BHC initiative documents and does not include interviews with BHC site staff and their partners to gather firsthand accounts. Furthermore, across sites, documents varied in focus, and level of detail was inconsistent. The breadth, depth, and complexity of this initiative undertaken in 14 distinctive environments present unique challenges to research, assessment, and evaluation. These factors limit the potential for cross-site comparison and made it difficult in some cases to attribute or apportion credit for policy achievements to specific BHC efforts.
Without longitudinal data, we were unable to consider the direct effect of policy and systems changes on community health outcomes. Thus, this research used explanatory models such as the social determinants of health to connect BHC strategies with policy and systems changes associated with progress toward long-term health equity. Future evaluation efforts should document how BHC’s policy and systems changes lead, over time, to measurable improvements in each community’s social, physical, and economic conditions.
Implications for Practice
Local public health departments can draw important lessons from the BHC experience to inform priorities (“the what”) and processes (“the who and how”) to accelerate progress toward equitable health and safety outcomes. The dominant public health approach to addressing health inequity continues to focus largely on the “medical model” that emphasizes services for specific diseases and health education and literacy. The BHC’s strategy is instead based on the recognition that supporting participatory democracy is key to creating health equity, particularly for communities that have been politically and socially oppressed and marginalized because of racism and other forms of structural bias.
Our review reveals that community-based collaboratives and regional networks can successfully deploy foundation resources and the community health frame to support organizing and power building that changes policies, systems, and the context in which important health decisions are made. Because health, and more specifically health equity, is within the purview of local health departments and public health leadership writ large, this finding strongly suggests a need for public health leaders to proactively partner and collaborate with community-based organizers seeking to address a broad range of social justice concerns, also known as the social determinants of health.
Our literature review and analytic tool brought together two relatively distinct fields of study: public health and social movement theory. We found this alignment useful in providing a more robust lens with which to view a complex, decade-long initiative which was designed from the outset to catalyze health-promoting policy and systems changes and support the youth and resident power-building activities that community-based collaboratives had identified as necessary for changing policies, nudging systems, and securing structural improvements over time.