Abstract
There is clear need for more effective public health policies. Coupled with calls for more effective policies, increasing demand to address public health disparities experienced by systemically marginalized and historically oppressed groups emphasizes the long-standing need for policies that improve public health equity. Such need is highlighted when examining public health issues such as alcohol- and substance-exposed pregnancy (ASEP): Current policies are ineffective at reducing ASEP, and marginalized groups experience disproportionately lower benefits and higher negative consequences as a result of such policies. Powerful strategies to develop more effective policies that can account for the complexity of such issues, such as systems science methods (SSMs), are becoming popular. However, current best practices for such methods often do not emphasize the additional efforts that will be required to develop equitable, not just effective policies. Using ASEP as an example of a crucial complex issue requiring new policy, we suggest additional steps to include in SSM projects for developing more effective policies that will also help stakeholders determine high-equity policies to reduce health disparities. These steps include modeling structural differences experienced by marginalized groups via systemic racism and oppression, incorporating existing cultural and community sources of strength and resilience as key areas for policy development, and evaluating the sustainability of policies as a dimension of efficacy. We also discuss using community-based participatory approaches as a framework for all SSM processes to ensure that policy development itself is grounded in equitable shared decision-making for marginalized individuals.
Keywords
Climbing neonatal abstinence syndrome rates in the United States have renewed interest in alcohol- and substance-exposed pregnancy (ASEP) prevention and intervention policy. However, current policies inadequately reduce ASEP and often result in negative consequences. These consequences are disproportionately experienced by marginalized populations, driven in part by failure for policies to address the systemic inequity of contexts in which they are implemented, such as legal, medical, or social service institutions (Faherty et al., 2020). Systems science methods (SSMs) have become popular approaches for identifying effective public health policies, helping policymakers and researchers navigate the complexity of public health issues (Carey et al., 2015). Through various analytical tools such as systems mapping and simulation modeling, SSM help discern the most effective policies by accounting for a holistic set of factors and relationships between them, and helping clarify how those relationships synergistically facilitate and maintain issues on individual and societal levels (Frerichs et al., 2016). SSM projects traditionally focus on identifying more effective policies, for example, identifying which policy would facilitate the biggest decrease in obesity within a community (Carey et al., 2015). However, even “high-efficacy” policies can be less effective for marginalized groups, such as evidence-based practice health programs that may not fit with cultural/social norms and values within marginalized communities (Rasmus et al., 2020).
A growing number of SSM projects focus on identifying effective policies that can both promote health and reduce disparity. However, there is substantial discussion on detailing the best SSM practices to develop models for testing effective policies (Carey et al., 2015), yet little discussion exists surrounding best SSM practices for developing models to test equitable policies (e.g., examining how systemic and individually experienced prejudice, marginalization, and oppression facilitate disparity). We argue that deliberate equity-grounded actions must be part of SSM. These actions include (a) evaluating system structure differences, systemic racism, and oppression; (b) grounding model development and policy testing in cultural and community sources of strength and resilience; and (c) ensuring policies be sustainable in implementation and impact. SSM activities also require a strong community-based participatory framework. Strong involvement from marginalized community members at all stages of the project is essential for equitable policy buy-in, adoption, and implementation. We use ASEP as a case example; however, the actions specified below can be included in a broad array of public health policy projects using SSM approaches.
Current Asep Policy
Substance use and reproductive health share a wide constellation of associated individual-level and interpersonal variables, socioecological contexts, and inequitable outcomes. Criminalizing ASEP is one of the most popular preventive policies in the United States. However, such policies are not effective for reducing ASEP and result in ASEP-related negative consequences (Roberts et al., 2018). Substance-using pregnant women in ASEP-criminalizing states are less likely to seek prenatal care and substance use treatment due to fear of consequences (e.g., termination of parental rights, arrest; Faherty et al., 2020). Punitive policies decrease the odds of child welfare parent reunification and increase foster care placement, reducing children’s access to resources for addressing ASEP-related long-term needs (e.g., developmental delays, behavior disorders; Sanmartin et al., 2020).
Punitive ASEP policies unequally affect racial/ethnic minority women and women in poverty, due to systemic racism and classism of criminal justice, child welfare, and medical institutions in which these policies are implemented. For example, in states with punitive policies, prenatal health providers are more likely to screen Black women and women in poverty for ASEP (Patel et al., 2021). Parental reunification disparities for children in foster care in states with punitive versus nonpunitive ASEP policies is larger for Black children compared with non-Hispanic White children (Sanmartin et al., 2020). Efforts to reduce disparities, such as standardizing ASEP reporting protocols, fail to address biases in other areas, such as provider testing (Patel et al., 2021). As fear of policy consequences reduces the likelihood of pregnant women who use drugs to seek treatment or prenatal care (Faherty et al., 2020), this fear is disproportionate within marginalized groups, further widening health disparity.
Nonpunitive policies such as increasing pregnant women’s access to substance use treatment and creating family-friendly or pregnancy-oriented treatment programs are more effective for reducing ASEP; fewer states utilize such policies (Faherty et al., 2020). More effective and equitable policies are required, as current nonpunitive policies are less effective for marginalized women (Roberts et al., 2018). For example, pregnant women of color have lower substance use treatment completion rates compared with pregnant White women, in part due to a variety of nested socioecological and systemic influences, such as experienced marginalization within treatment settings (Suntai, 2021).
Ssm Practice Considerations for Developing Equitable Asep Policies
SSM is well-equipped to improve policy-development efforts for complex public health issues such as ASEP. Common SSM practices for policy decision-making include (a) identifying a problem within the system to model, (b) developing a model illustrating the problem as existing within the system, (c) and discerning which policies provide the most desired change (Carey et al., 2015). This is carried out through collaborations between researchers, professional stakeholders (e.g., administrators, experts, caseworkers, community organizers, and advocates), and those with personal (nonprofessional) experience with the target issues (Frerichs et al., 2016). There has been little discussion on best SSM practices for examining system-level equity/disparity; however, SSM research can benefit from additional processes to develop more equitable policies. As evidenced by current ASEP policy performance, factors driving health disparities of the “problem” can create inequitable (e.g., lower benefits and higher consequences) policy effects.
First, practitioners and policymakers must specify the system components (e.g., ASEP reports to child welfare) and system structures (the presence or absence of system components and links between components, for example, bias in ASEP testing and reporting to child welfare services) that drive inequity. Identifying barriers to obtaining health-promoting resources is a common approach, such that equity is improved through increased access to resources. However, this must be paired with (a) understanding unique barriers that are experienced by different groups, and (b) evaluating how resource effectiveness differs between groups. For example, the most popular nonpunitive ASEP policies focus on reducing barriers to pregnant women’s substance use treatment access through increasing referrals to treatment. However, such policies are not a panacea to addressing ASEP-related disparities, as racial/ethnic minority pregnant women are less likely to complete substance use treatment (Suntai, 2021). A thorough, concrete mapping of the process facilitating experiences of inequity through system structures, such as the system structures underlying substance use treatment engagement and completion disparity (e.g., experienced racism within treatment institutions which reduces completion; Wolfson et al., 2021), provides a clearer pathway for identifying tangible actions toward equity through policy.
Second, accounting for system differences that serve as leverage points for resilience and health promotion is as important as considering differences serving as barriers. Policies targeting stigmatized issues historically use deficits-based approaches. ASEP-criminalization policies continue this trend, contributing to the stigma experienced by substance-using pregnant women (Wolfson et al., 2021). Strengths-based approaches such as trauma-informed programs are more effective for reducing stigmatized public health issues within marginalized groups (Rasmus et al., 2020). ASEP policies should build upon positive and protective factors for health related to resilience and strength that exist within different marginalized communities or cultures. Programs based on cultural or community practices and knowledge, or those emphasizing development of strong social support networks (e.g., extended kin networks) or cultural identity, demonstrate reduced substance use in some racial/ethnic minority or marginalized groups (Rasmus et al., 2020). Therefore, examining systemic marginalization and resilience to marginalization should be considered in tandem; as the first step discussed focuses on the unique factors contributing to what doesn’t work (e.g., ineffective treatment for specific groups), the second step focuses on the unique factors that demonstrate what does work (e.g., culturally based systems of care).
Considering existing sources of strength and resilience as leverage points for health also promotes the third action for equity-focused SSM approaches to health policy: considering policy sustainability as a dimension of efficacy. Communities with higher rates of marginalized residents have lower access to and availability of public health resources. This scarcity often results in a dependence on external funding and specific providers for implementing policies for preventive and intervention programs (failing to build on existing leverage points). External funding reliance creates a cycle of need defined by program duration, with minimal long-term community health improvement. This capability trap reduces the impact of the policies themselves as more time and effort is devoted to securing funding or maintaining infrastructure as initial funding starts to end, requiring new resources if additional funding cannot be obtained. Continual resource turnover inhibits the growth of community-level trust in resources, reducing resource engagement, and resource affects community well-being. Current ASEP-reduction programs exemplify this issue. ASEP burdens are highest in low-resource communities, resulting in the implementation of short-term and externally funded programs that require little community support. However, such interventions have weaker long-term effects in disparate communities (Symons et al., 2018), compared with interventions that devote more resources toward long-term and sustainable impacts. As SSM approaches allow for policy testing, comparison of different policies should include evaluating sustainability, that is, how long the policy can be implemented within the community, and the duration of positive policy effects within the community. This should also include an evaluation of the balance between the duration of the cost and benefits of the initial policy, and new costs from additional required policies (if policy benefits decline over time, or decline faster for marginalized groups). SSM projects should also strive to account for how low-resource sustainability is a broader symptom of health inequity as facilitated by systemic marginalization (e.g., what is driving the resource scarcity that necessitates continual external funding). Beyond examining the sustainability of individual policies, examining how to change system structures to increase overarching policy sustainability will provide the strongest health equity gains.
Community Inclusivity and Equitable Decision-Making In SSM Project Teams
Including these actions within SSM projects require strong researcher–stakeholder partnerships (Frerichs et al., 2016) with a diverse group of individuals, including individuals belonging to marginalized groups. Stakeholders provide critical information for model development and policy identification and buy-in. Collaborative group partnerships that effortfully provide an inclusive and empowering space for marginalized community members to contribute will result in more equitable (and more effective) models and developed policies (Rasmus et al., 2020). A lack of dedicated inclusion will reinforce the same power dynamics driving inequity through withholding decision-making power. Community-facing health care professionals and providers are critical stakeholders in collaborative partnerships for health policy SSM projects (Frerichs et al., 2016), representing both policy-implementing institutions (health care systems) and the communities in need. Although contributions from such stakeholders involve content-area expertise, community-facing health professionals are well-positioned to serve as equity and representation champions. For example, they can be strong community liaisons, encourage marginalized community members to participate in SSM projects, and help ensure that all project protocols are tailored to address power dynamics and cultural/community competence in ways that promote active engagement in SSM activities.
Community-based participatory frameworks can guide the trust-building that is necessary for community partnerships, and the actions to ensure that decision-making power for all project actions (design, implementation, interpretation of results, and use of results) is distributed equitably based upon need and current decision-making power within the community. Community-based participatory research consensus-making protocols dovetail with consensus-making activities within participatory SSM frameworks (e.g., group model building; Frerichs et al., 2016). These protocols allow communities to come together in ways that reduce power imbalances for more equitable, community-informed strategies for change, and provide a vehicle to engage in the SSM practices necessary for developing equitable policies (Frerichs et al., 2016).
Conclusion
ASEP is one of many complex public health concerns requiring policies that help dismantle the inequity-facilitating contexts in which they are nested (Faherty et al., 2020). SSM can help policymakers discern more effective strategies for positive system-level change (Carey et al., 2015). Equitable disparity-reducing strategies must affect the systems causing them. Such solutions, which empower marginalized groups and account for unique barriers experienced via marginalization, can be discovered by grounding all policy-development practices (e.g., SSM) in an equitable framework.
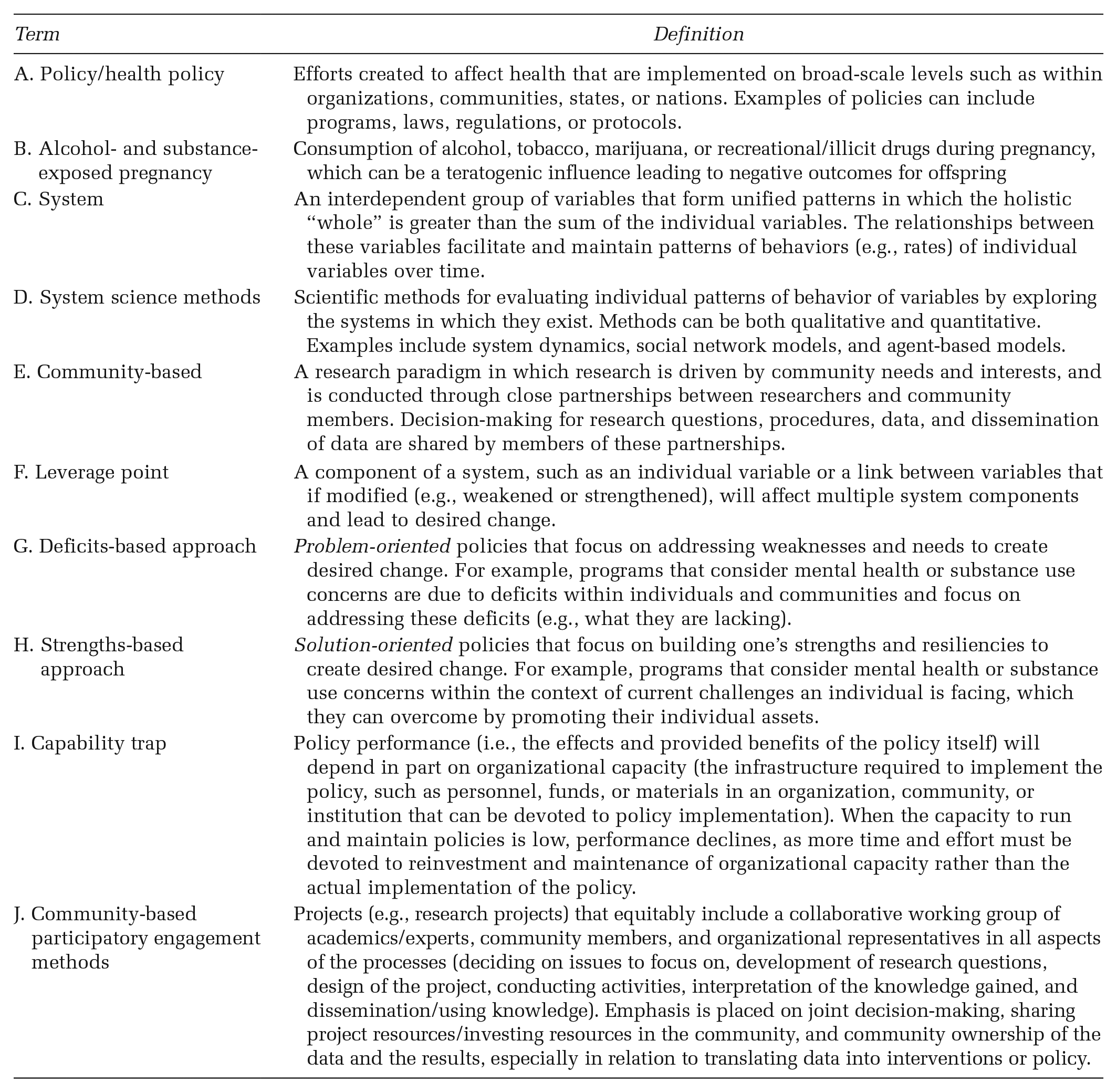
Glossary