
Abstract
Statins are an important but underutilized therapy to prevent cardiovascular events, particularly in high-risk patients. To increase use of statin therapy in high-risk patients, the Centers for Disease Control and Prevention funded a project led by the National Association of Community Health Centers to discover reasons for statin underuse in health centers and identify possible leverage points, particularly among vulnerable and underserved patients. The project further sought to develop training and educational materials to improve statin prescribing for and acceptance in eligible high-risk patients. As a first step, investigators implemented a questionnaire to clinical providers (n = 45) at health centers participating in the project to obtain their perspective on barriers to optimal statin use. We used the practical robust implementation and sustainability model (PRISM) domains to frame the overall project and guide the development of our questionnaire. This paper summarizes top perceived barriers to patient and health system/provider statin initiation and sustainment, as well as facilitators to prescribing, using PRISM as an organizing framework. Our questionnaire yielded important suggestions related to public awareness, education materials, health information technology (HIT)/data solutions, and clinical guidelines as key factors in optimizing statin use. It also informed the design of patient education resources and provider training tools. Future directions include using the full application of the PRISM implementation science model to assess how well our educational and training resources help overcome barriers to statin use in high-risk patients, including evaluating how key contextual factors influence successful implementation.
Keywords
To optimize use of statin therapy, the Centers for Disease Control and Prevention (CDC) funded a project led by the National Association of Community Health Centers (NACHC) to increase use of statin therapy for high-risk health center patients. In the first phase of this project, the NACHC team worked to identify provider perceptions regarding reasons for statin underuse in health centers and to identify leverage points for increasing use. Investigators worked with clinical providers to inform interventions to improve quality of care for statin-eligible high-risk patients and guide future implementation practices. Specifically, we developed and disseminated a questionnaire to collect stakeholder perspectives from the adopting organizations. We used the practical robust implementation and sustainability model (PRISM) domains to frame the overall project and guide the development of our questionnaire (Feldstein & Glasgow, 2008), which focused on identifying provider perceptions regarding patient and health system/provider barriers to statin initiation and sustainment, as well as facilitators to prescribing. The findings from the questionnaire were then used to develop health center patient and provider education tools.
Background
Cardiovascular disease (CVD) accounts for one in six U.S. health care dollars spent—almost US $1 billion per day (Centers for Disease Control Prevention [CDC] and Division for Heart Disease and Stroke Prevention, 2019)—and remained the leading cause of death in the United States in 2020 (Ahmad & Anderson, 2021). Elevated blood cholesterol is a major risk factor for CVD. More than 130 million U.S. adults, 20 years or older, have elevated total cholesterol levels of 200 mg/dL or more, while almost 31 million have levels 240 mg/dL or more (Mozaffarian et al., 2015), which puts them at high risk for a cardiovascular event (Grundy et al., 2018). Individuals with low-density lipoprotein-cholesterol (LDL-C) ≥190 mg/dL, regardless of cause, have a fivefold increased long-term risk for coronary artery disease (Eid et al., 2020).
A meta-analysis of 27 randomized trials demonstrated that for every approximately 40 mg/dL LDL-C reduction, the relative risk of a major cardiovascular event is reduced by 20% to 25% (Aroniset al., 2016). Statin use is a cost-effective method to lower risk of CVD events (Heller et al., 2017; Pandya et al., 2015) and this cost-effectiveness will increase as more statins become generic (Mitchell & Simpson, 2012). Current guidelines identify three high-risk groups that would benefit from statin therapy: (1) individuals with atherosclerotic cardiovascular disease (ASCVD), (2) individuals with LDL-C ≥190 mg/dL, and (3) individuals with diabetes and LDL-C 70 to 189 mg/dL (Grundy et al., 2018). However, of those at high risk, only approximately 55% use statins (Wall et al., 2018); among eligible adults ≥21 years, 39.1 million people were not using statins (Eid et al., 2020).
Management of high cholesterol, particularly for high-risk patients, became even more of an imperative during the COVID-19 pandemic (National Center for Immunization and Respiratory Diseases [NCIRD], Division of Viral Diseases, 2021). In addition, CMS 347, Statin Therapy for the Prevention and Treatment of CVD, recently became a required health center quality measure for reporting under the Health Resources and Service Administration’s Uniform Data System (eCQI Resource Center, 2021).
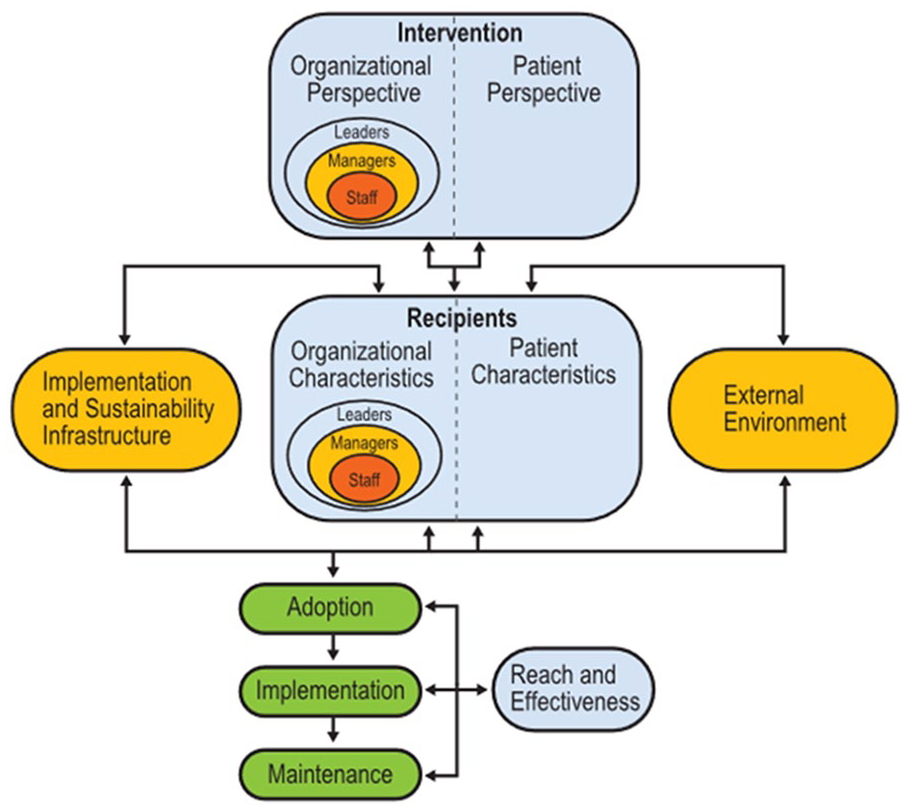
Given the high level of need, the effectiveness of statins, and the low rates of use, it is important to develop, implement, and evaluate programs to promote statin use for vulnerable populations. To ensure effective interventions can be developed and implemented successfully to address this care gap, we used the PRISM implementation science model to inform our formative research and intervention design. PRISM is a more recent expansion of RE-AIM (RE-AIM.org, 2021) that asserts that certain contextual factors influence implementation outcomes (McCreight et al., 2019) (see Figure 1).
The Practical Robust Implementation Sustainability Model (PRISM)
PRISM depicts the relationships between the intervention, recipients, external environment, and implementation and sustainability infrastructure. This is linked with the RE-AIM framework, which assesses reach, efficacy, adoption, implementation, and maintenance to understand how these constructs impact meaningful outcomes (RE-AIM.org, 2021). Using this model, we developed a framework for the overall long-term project goals to improve use of statin therapy among high-risk patients at health centers and an implementation plan that takes into account the complexities and reciprocal relationships involved in health center systems of care.
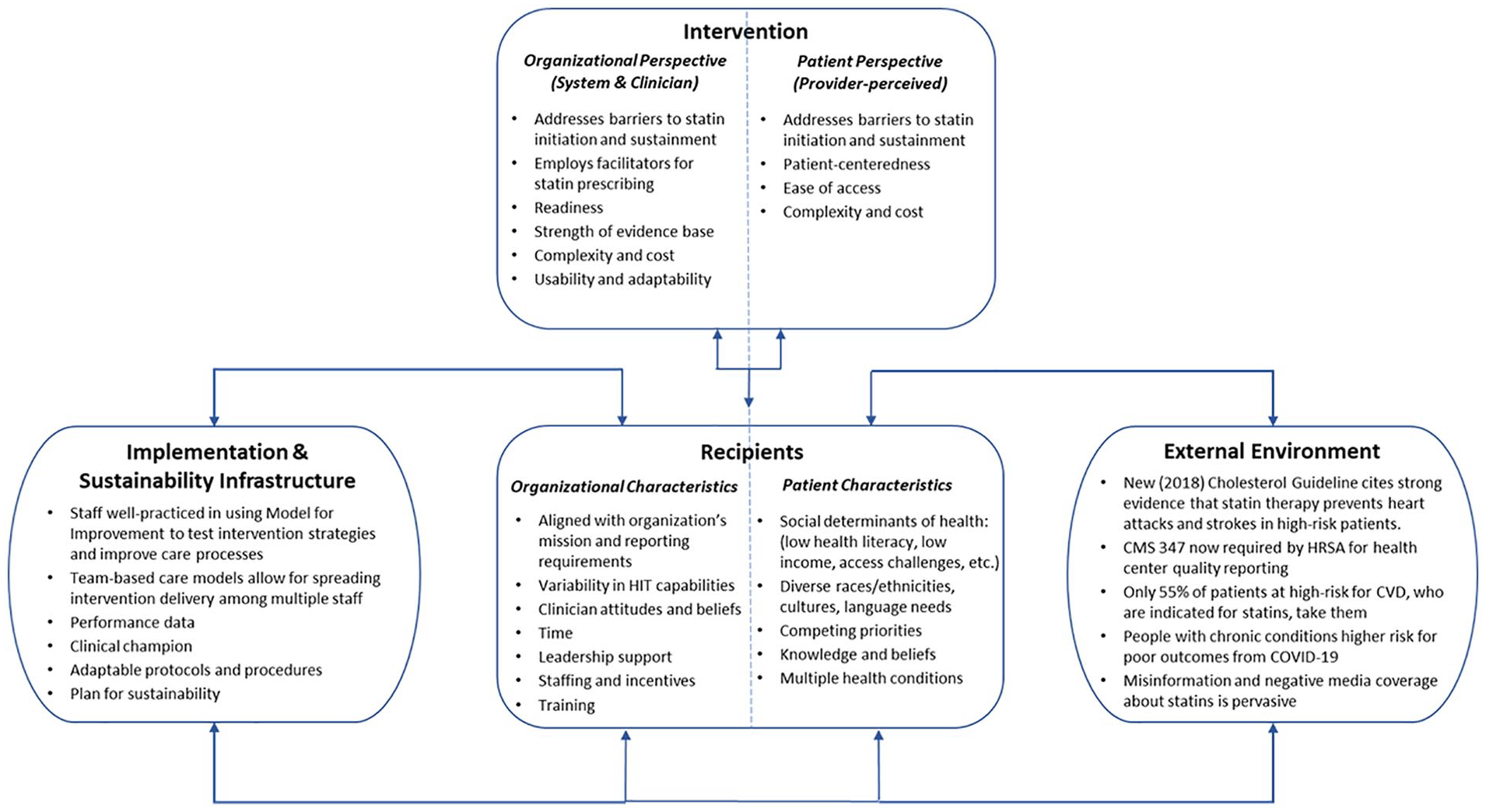
Figure 2 details the specific elements of PRISM used to plan for improving statin use among high-risk patients in health centers. We recognized we needed to understand contextual determinants in health centers’ implementation and sustainability infrastructure that might shape intervention planning and future implementation. Health centers frequently use team-based care models that allow for spreading intervention delivery among multiple staff and utilize the model for improvement (Langley et al., 2009) to test interventions and improve care processes. Furthermore, health centers have access to performance data on appropriate use of statin therapy, which could be used to measure intervention impact/implementation success.
PRISM Applied to Planning for Improving Statin Use Among High-Risk Health Center Patients
Within the PRISM domain of recipients, we assessed organizational and patient characteristics we would need to consider in intervention design and implementation. We recognized the unique vulnerabilities of health center patients regarding social determinants of health, diverse races/ethnicities, cultures, and language needs (National Association of Community Health Centers [NACHC], 2012). We also recognized competing priorities as well as knowledge and beliefs as important patient characteristics, and the fact that many high-risk patients have multiple health conditions needing attention (Eid et al., 2020).
We documented factors in the external environment that can influence intervention adoption by clinicians and acceptance by patients. Several factors are potential catalysts for statin uptake; these include clearer recommendations in the 2018 American College of Cardiology (ACC)/American Heart Association (AHA) Cholesterol Guideline that patients who are high risk for CVD should be on statin therapy (Grundy et al., 2018) as well as the addition of a statin therapy quality measure (CMS 347) for health center compliance reporting (eCQI Resource Center, 2021). These facilitators are countered by pervasive misinformation and negative media coverage about the safety and side effects of statins (Navar, 2019).
We developed a questionnaire using PRISM as a guiding framework and informed by literature review (De Wilde et al., 2003; Kedward & Dakin, 2003; Tobert & Newman, 2016). The questionnaire focused on the PRISM domain of Intervention, with attention to the importance of the other domains described above.
The specific aims of this phase of the project were: (1) to utilize the PRISM implementation science model to develop and implement a questionnaire that would identify provider, health system, and patient barriers and facilitators to statin initiation and sustainment in vulnerable populations and (2) to use the questionnaire results to inform development of interventions to help health centers improve appropriate prescribing for statin-eligible high-risk patients and help patients understand the benefits of statins, while dispelling concerns.
Methods
The institutional review board at A.T. Still University’s Kirksville College of Osteopathic Medicine in Kirksville, Missouri granted exempt status to this study. This article was informed by the SQUIRE Guidelines V2 (Goodman et al., 2016).
Setting and Participants
This project involved five health center-controlled networks (HCCNs). HCCNs identified 21 health centers that enrolled in the project from CA (5), FL (4), IL (2), and NY (2), and one each from the DC, HI, IA, MO, NC, NJ, OR, and WA. Most centers were rural; five were from major metropolises, including DC, Miami, St Louis, and Chicago.
Of the 21 health centers, six served a patient population >50% African American and five cared for patients >50% Hispanic/Latino. Health center patient populations ranged from 4,287 to 104,137; the majority (>50%) were adults 18 to 64 years of age.
Questionnaire Development Utilizing the PRISM
We inventoried key elements under PRISM’s intervention domain, which considers the perspectives of key stakeholders. We identified several items we believed would influence implementation success, including readiness of staff to implement the intervention, strength of clinical evidence underpinning the intervention, complexity and cost, and usability and adaptability (Feldstein & Glasgow, 2008). Patient-centeredness, ease of access, and complexity and cost were the factors we determined would be important patient perspectives in informing our efforts (Thomas-Henkel & Shulman, 2017). For both groups, we recognized we would need to understand and address barriers both to statin initiation and sustainment for any intervention to achieve the desired outcomes. The questionnaire was designed to uncover and confirm which barriers to appropriate statin use were perceived to be most salient in health centers.
The questionnaire included 12 items. See Online Appendix A: Drivers of Statin Underuse—Provider Questionnaire (paper version). It instructed providers to identify patient barriers they believe most influence initiation of statin therapy from a list of potential barriers. Respondents could choose “other patient barriers” and were prompted to describe them in an open-ended format. They were then asked to select the most important barriers from those they identified (including any other barriers they indicated). Respondents then identified and ranked patient barriers they believed most influence sustainment of statins. Similar questions were asked about health system and provider barriers for statin initiation and sustainment. Providers were asked to describe what might make it easier to prescribe statin therapy to high-risk patients. The questionnaire was anonymous but queried respondents on clinical role and the state in which they provide care.
Questionnaire Dissemination
In March 2019, we disseminated this questionnaire electronically to leaders engaged in the project at the five HCCNs (Qualtrics, 2020). These HCCN leaders sent the link to project leads at the 21 participating health centers to distribute to their clinical providers with experience treating patients at high risk for cardiovascular events. The questionnaire was open until June 3, 2019.
Quantitative Analysis
Quantitative responses to questions about perceived barriers were summarized using “weighted” ranks. These ranks were calculated by weighting the rank score for each item by the number of endorsements it received, that is, a weighted linear combination. This score was then divided by number of respondents. Ranks were weighted as follows: 1 = 100, 2 = 75, 3 = 50, and 4 = 25. A weighted rank (WR) score of “100” would mean that all subjects endorsed the barrier and ranked it as “1” (the highest). The higher the WR, the more important participants, as a group, considered the barrier. We did not include “other patient barriers” in the WRs analysis because of their variation and small number but did analyze the associated narrative responses qualitatively.
Qualitative Analysis
We analyzed open-ended survey responses using NVIVO 12 Plus (QSR International Pty, n.d.), to identify commonly used phrases and recurring themes.
Education Tool Development
The NACHC team worked with the American Medical Association (AMA) to develop materials for provider and patient education based on the quantitative and qualitative findings.
Results
Forty-five providers initiated the survey; 37 responded to Q1, 35 to Q2, 33 to Q3, and 32 to Q4 through Q11. Of those respondents who provided their role, the majority were physicians (18), followed by physician’s assistants (7), nurse practitioners (3), other (2), clinical pharmacists (1), and nurses/registered nurses (RNs) (1).
Quantitative Data
Provider-Perceived Patient Barriers
WR scores for provider-perceived patient barriers to initiation of statin therapy are provided in Figure 3. Among the 37 respondents, 59.5% (n = 22) endorsed the idea that patients hold the “belief that drawbacks outweigh benefits of statins” as a significant barrier (WR = 35.1); 56.8% (n = 21) endorsed “lack of understanding of their current disease condition” (WR = 33.8). “Previous negative experience with statin therapy” received a WR = 22.3, and “concerned about prolonged medication use,” received a WR = 17.6. Social determinants, such as “cultural and ethnic beliefs” (WR = 10.8), “difficulty affording statin therapy” (WR = 5.4), and “low health literacy” (WR = 3.4) received lower rankings of significance.
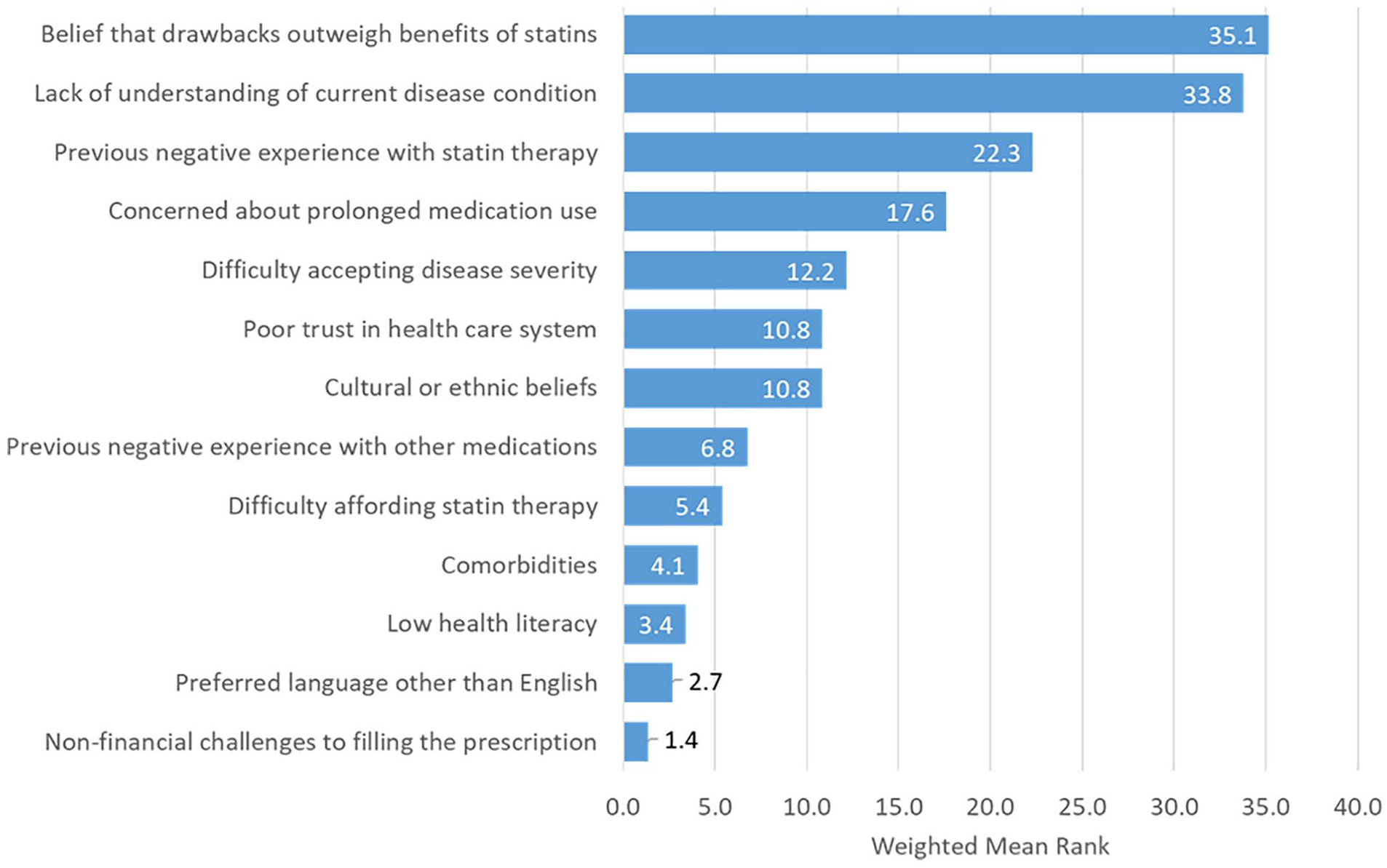
Provider-Perceived Patient Barriers to Statin Initiation (n = 37) Weighted Ranks
WR scores for provider-perceived patient barriers to sustainment of statin therapy (n = 35) are provided in Figure 4. The most highly rated barriers were “lack of understanding of current disease condition” (WR = 25.7) and “overall belief that drawbacks outweigh benefits of statins” (WR = 25.0). Lack of understanding was selected by 34.3% of participants (n = 12) and statin intolerance by 28.6% (n = 10); 34.3% (n = 12) selected “complex medication regimen” but it was not rated as highly as other barriers (WR = 7.1).
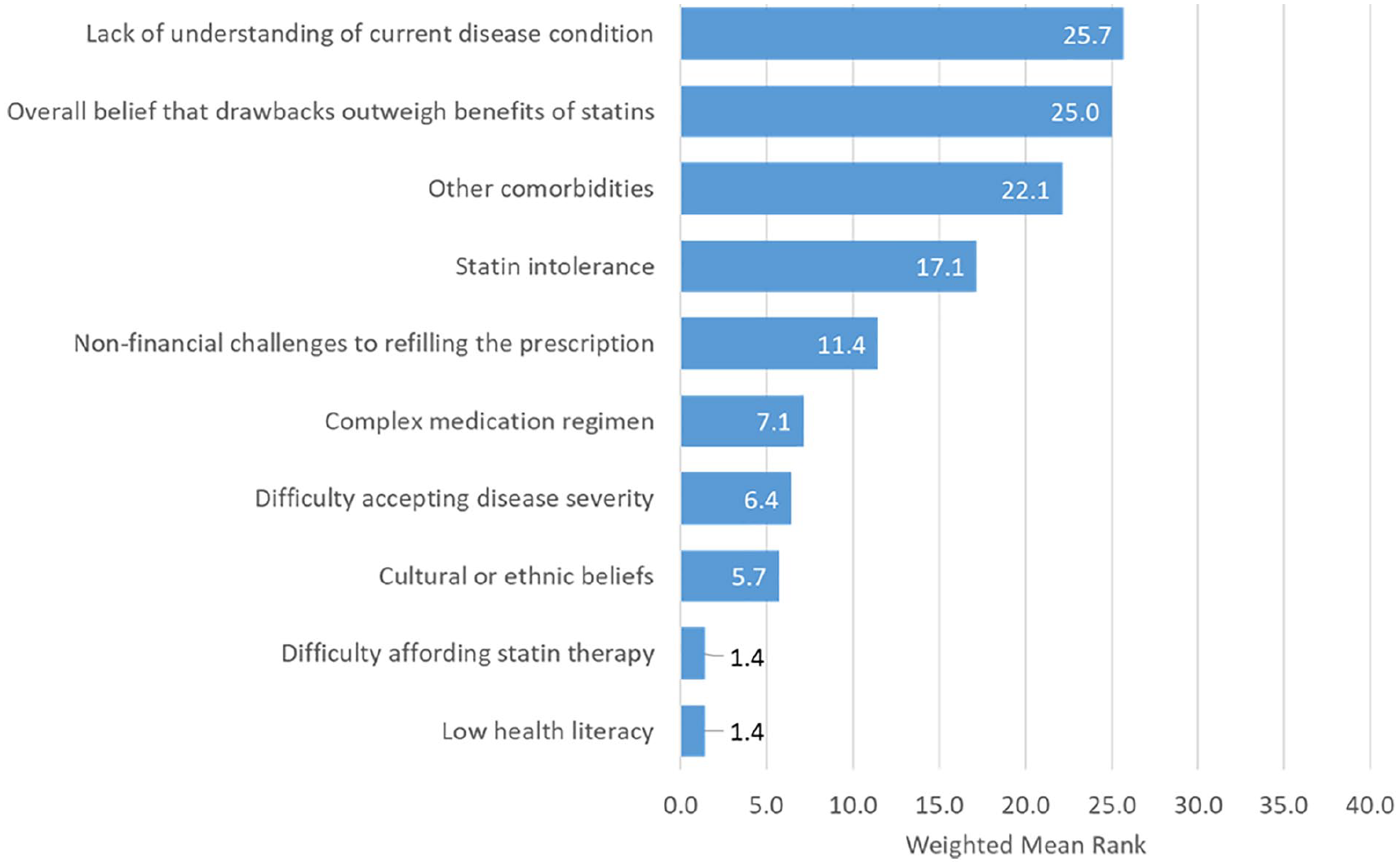
Provider-Perceived Patient Barriers to Statin Sustainment (n = 35) Weighted Ranks
Provider-Perceived Health System and Provider Barriers
“Frequently changing clinical guidelines” was the most highly rated health system/provider barrier to statin initiation (Figure 5), endorsed by 43.8% (n = 14) of participants (WR = 34.1). “Not enough time with patients to provide proper education about their medical condition and medication” was rated second (WR = 28.8) with 46.9% (n = 15) endorsements. “Multiple clinicians providing varying and possibly conflicting details to patients regarding statins” ranked third (WR = 25.8), with 31.3% (n = 10) endorsements (Figure 6).
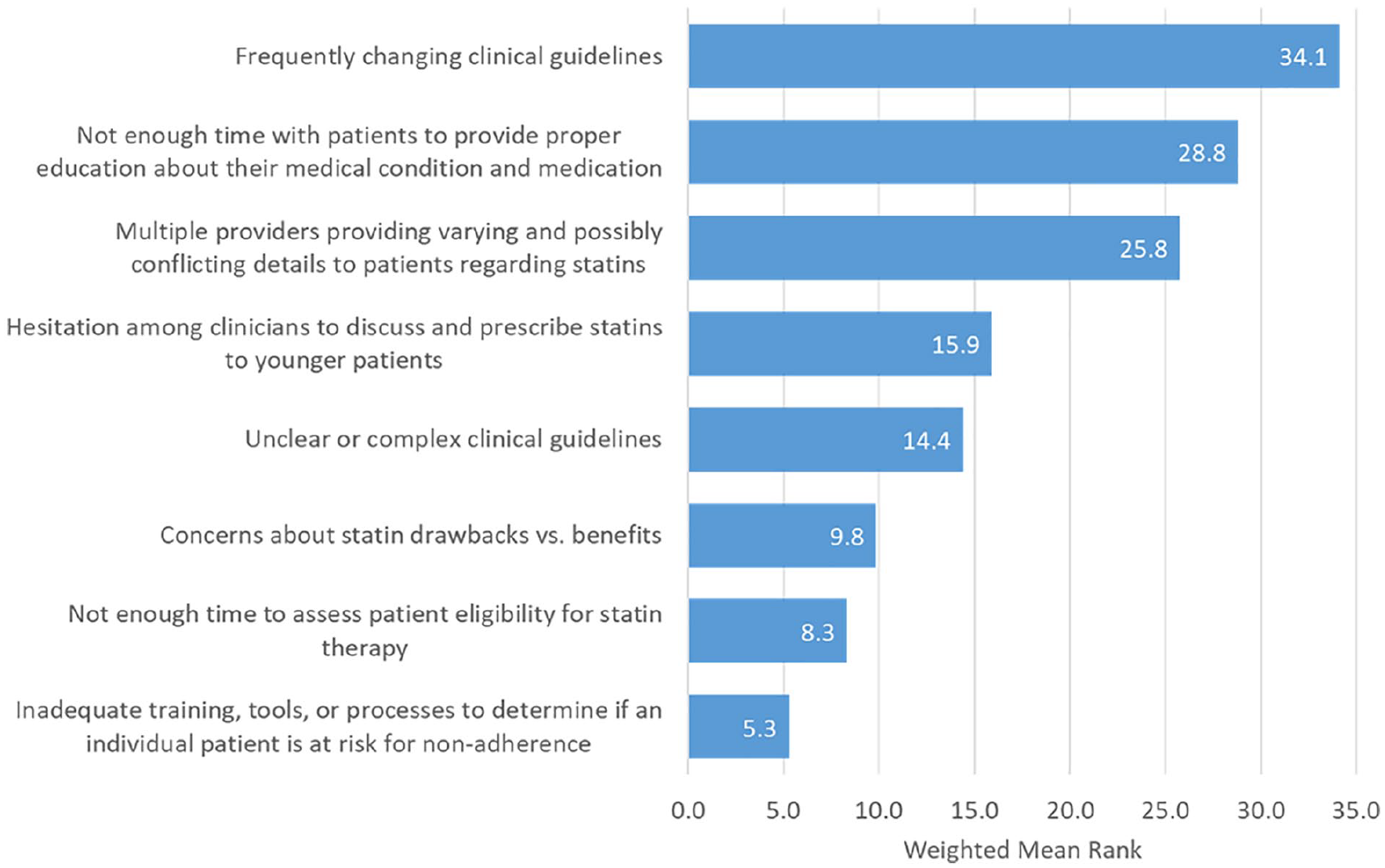
Provider-Perceived Health System and Provider Barriers to Statin Initiation (n = 33) Weighted Ranks
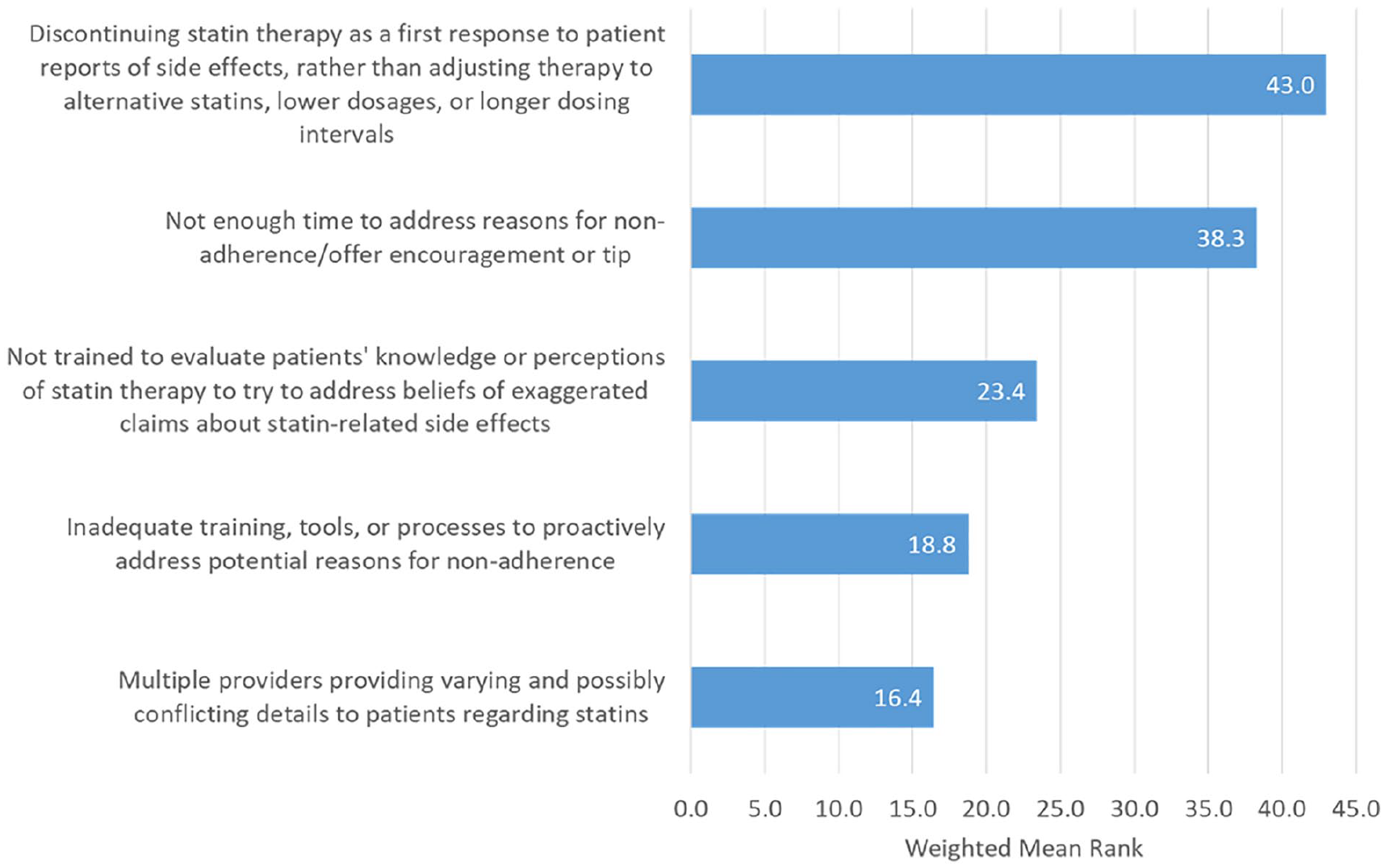
Provider-Perceived Health System and Provider Barriers to Statin Sustainment (n = 32) Weighted Ranks
“Discontinuing statin therapy as a first response to patient reports of side effects, rather than adjusting therapy to alternative statins, lower dosages, or longer dosing intervals” rated highest (WR = 43.0) among health system barriers to statin sustainment (Figure 4); 53.1% (n = 17) endorsed this barrier. “Not enough time to address reasons for non-adherence/offer encouragement or tip” (WR = 38.3) also rated highly, with 53.1% (n = 17) endorsements.
Qualitative Data
Some respondents selected “other barriers” in the questionnaire and described these in open-ended responses. These can be organized using PRISM. Under patient perspectives and characteristics, several patient-based themes emerged; one was intentional medication non-adherence. For example, patients wanting to try lifestyle changes first, preferring “natural treatments” to prescription medication, or believing cholesterol is best addressed with dietary changes. Additional examples included feeling they are taking too many pills already or misunderstanding the concept of a chronic medication that requires lifelong/years of refills. Inadequate perceived benefits was another patient theme under other barriers; for instance, there is “no immediate subjective benefit to statin use (patients physically feel no different whether their cholesterol is high or low)” and “it [addressing high cholesterol] is not a priority.” Finally, inconvenience of regimen compliance was a theme, such as inconvenience of associated lab tests.
Under organizational (health system/provider) perspectives, “other barrier” themes included lack of trust/intentional non-adherence with clinical guidelines and difficulty complying with clinical guidelines. Examples include a distrust of “pharma,” lack of conviction regarding benefits of statin use, and the challenging combination of drug costs, lab tests, changing formularies, and side effects in trying to address high cholesterol.
Open-ended questionnaire responses also revealed what providers believed would make it easier for them to prescribe statin therapy. These solutions can be categorized into three groups: awareness/education, health information technology (HIT), and clinical guidelines.
Providers indicated that public awareness and education could remove the stigma of statin therapy, making it easier to prescribe statins. Providers expressed a need for educational materials available to the “general public” “to combat the myth and lousy reputation of statin therapy.” Furthermore, educational materials should include “clear information that gives patients the risks of NOT using statin therapy and what the data truly says [sic] about the long-term safety of the medications.” Providers expressed the need for “patient-centered teaching materials” in addition to “clearer informatics [that will help in] demonstrating risk to patients.” One respondent suggested “simplified handouts for patients regarding risks and benefits of use.” Furthermore, providers conveyed the need for “adequate time” to discuss statin benefits/risks with patients.
Providers described integrated clinical decision support as another prescribing facilitator. Several cited the need for integrated risk assessment tools, such as “ASCVD risk calculators” into electronic health records (EHRs). One provider articulated that risk assessment tools are external to the EHR and require going “to a website to calculate risk.” Respondents also expressed desire for EHR prompts with reminders; for example, an “automatic pop up with guidelines [that are] patient specific and link to [the] correct order.” Responses concerning clinical guidelines centered on the need for clarification. Respondents stated that “clearer guidelines” would allow much needed ease in prescribing statin therapy.
Providers also indicated the importance of educational materials for them to understand the guidelines and clinical indications for statin therapy for high-risk patients. A respondent expressed wanting “continuous reminders” to prescribe statin therapy for patients in high-risk groups “until it becomes second nature.” The suggestion for “re-education of providers on current clinical guidelines” was given along with training and “expert discussion” on the safety and overall benefits of statins. Respondents also shared that more education on statin prescribing for younger patients who need long-term therapy would help increase appropriate prescribing as well as opportunities to “share experiences and encourage adherence” among fellow providers.
Patient and Provider Education Tool Development
Resources were developed based on questionnaire findings. Patient-focused materials were designed to increase high-risk patients’ perceived benefits of statin use while addressing perceived barriers and improving knowledge about statin therapy. These resources include:
How Do Statins Prevent Heart Attacks and Strokes, an animated patient education video adapted from the British Heart Foundation in English and Spanish
How Do Statins Prevent Heart Attacks and Strokes, an infographic in English and Spanish
Statins and a Healthy Lifestyle, an infographic in English and Spanish
Health center videos: Millie’s Story, Laurie’s Story, and Dr. Jones Q&A series. Patient stories, clinician testimonials, and clinician/patient conversations about statins
NACHC and AMA co-developed a Cholesterol Provider Training Package to help health care providers improve prescribing for statin-eligible high-risk patients. Materials were deliberately produced in different formats to enable clinicians and care teams to use their preferred format(s). These resources include:
Q&A. Common Patient Questions about Statins, a tool to assist providers and care teams in discussing statins with eligible patients
Short, annotated slide decks for train-the-trainer presentations or self-paced learning:
○ Statin Guideline Snapshot
○ Statin-associated Side Effects
○ Statin Adherence
Statin Therapy for High-risk Groups Summary, a web-based, MP4 recording, narrated by a cholesterol expert, that can be shown as a webinar or listened to as a podcast
Statin Therapeutic Inertia Chart Audit Tool
Discussion
Statins are an important but significantly underused therapy in preventing cardiovascular events in high-risk patients (Aronis et al., 2016; Eid et al., 2020). Understanding potential drivers of statin underuse, particularly in underserved and vulnerable populations, is an important step in designing training, education materials, and other resources to help mitigate barriers that negatively influence the uptake of statins. While literature exists on barriers to statin use in the general population, prior research was not directly related to underserved and vulnerable patients. The majority of health center patients are under 100% of federal poverty guidelines (NACHC, 2012). In addition, previous efforts around statin therapy did not use an implementation science framework to inform the approach.
Guided by the PRISM implementation science model, our questionnaire yielded important suggestions related to raising awareness about the safety and importance of statins, developing better HIT/data solutions, and improving clinical guidelines. It also surfaced recommendations and leverage points to inform the design of patient education resources and provider training tools for health centers.
Low perceived threat of disease combined with a perception that barriers to or potential problems from engaging in a health protective behavior outweigh benefits leads to inaction. Thus, we developed resources that can tip scales in the other direction—clarify perceived threat and highlight perceived benefits while lowering perceived barriers to produce action. The How Do Statins Prevent Heart Attacks and Strokes animated videos and infographics for patient education explain why high cholesterol is dangerous, why statins are so effective, and the low risk of side effects.
Several perceived patient barriers ranked highest were based on misinformation that can be addressed through better education. The perception that prolonged statin use is harmful perhaps stems from ideas connected to other medications that are addictive (e.g., opioids) or build up in the body and can impact liver function (e.g., non-steroidal anti-inflammatory drugs [NSAIDs]). However, the opposite is true of statin therapy; larger absolute benefits have been shown to accrue with prolonged use (Aronis et al., 2016). The How Do Statins Prevent Heart Attacks and Strokes videos and infographics emphasize the safety of statins.
Previous negative experiences or statin intolerance due to muscle-related side effects may be inaccurately attributed to statins, as actual risk of statin-induced muscle injury is extremely low (<0.1%) (Newman et al., 2019). Prior to our project, there was a gap in resources to help with broader educational conversations with statin-eligible patients. Our tool, Q&A: Common Patient Questions about Statins, provides responses to common questions and can aid care teams in patient education.
The misconception that high cholesterol in high-risk patients can be managed successfully with lifestyle changes alone also surfaced as a barrier in patients’ willingness to take statins. While a healthy diet, avoiding tobacco, and regular physical activity are important for everyone, engaging in healthy behaviors without cholesterol-lowering medication is not enough to reduce risk of heart attack and stroke in high-risk patients (Eckel et al., 2014; Grundy et al., 2018). While we included this topic in our provider tool, we felt we also needed something visual to help patients understand why a healthy lifestyle is foundational, but not enough, for high-risk patients. Thus, we developed Statins and a Healthy Lifestyle, an infographic that shows expected LDL reduction from a healthy lifestyle alone versus with moderate and high-intensity statins in relation to a patient’s LDL-C goal.
Low health literacy was perceived by clinicians to be a barrier to statin initiation and sustainment. Thus, we intentionally created pieces that were more visual, at lower reading levels, used culturally diverse animations and voice-over actors, and made available in both English and Spanish.
Perceived barriers of medication costs and regimen complexity can be addressed through interventions implemented by the clinical team, such as prescribing low-cost generics, aligning prescriptions, and creating pill packs. We emphasized these strategies in the Cholesterol Provider Training Package that includes short, annotated slide decks for train-the-trainer presentations or self-paced learning, a separate audio recording for podcast-like listening, and a Statin Clinical Inertia Assessment Tool.
Time and training surfaced as the most significant health system and provider barriers. Respondents felt they lacked time to educate patients about their medical condition and initiate statin therapy. When a patient had previously been prescribed a statin, they lacked time to address reasons for non-adherence or offer encouragement or advice. Standing orders and patient education tools that can be used by the expanded care team (e.g., nurses, pharmacists, and medical assistants), such as our newly developed Q&A: Common Patient Questions about Statins resource and our How Do Statins Prevent Heart Attacks and Strokes? video could shift the time burden from clinicians to others on the care team. Moreover, we assumed time to complete training on optimizing statin use would also be an important design factor; thus, in our Cholesterol Provider Training Package, we offered a variety of short audio and visual formats that could be viewed or listened to in under 15 minutes.
There may be some concurrent health system factors at play, such as lack of clinical decision support tools that could remind providers to prescribe statin therapy for patients in high-risk groups. These tools can make taking appropriate action quicker and easier. Providers may also perceive the gravity of high cholesterol relative to other conditions as lower, reducing their urgency to focus on statin therapy. Most high-risk patients have multiple chronic conditions (Eid et al., 2020); prompts for appropriate statin prescribing could be embedded in EHR templates and order sets for other conditions like hypertension and diabetes. This more holistic approach could trigger providers to address statin use more efficiently.
Respondents expressed that beliefs about statin safety can lead to clinical inertia or discontinuing statin therapy as a first response to patient reports of side effects, rather than adjusting therapy. Furthermore, clinician misjudgment regarding the impact of lifestyle changes on LDL levels and lack of appreciation of statin benefits can be attenuated by provider training and education. The Statins and a Healthy Lifestyle education piece has the dual purpose of educating patients and care teams. Furthermore, the Cholesterol Provider Training Package clarifies the clinical indication of statin therapy for high-risk patients and presents current clinical guidelines around statins in a simplified and actionable way. The Training Package also includes research on effectiveness in relation to side effects.
Limitations
This study utilized a small sample of health center providers. While the providers who responded to the questionnaire are experienced health center clinicians who work with patients at high-risk for CVD, their responses cannot be generalized to all providers. About half of these providers are physicians; it is not clear how perceptions differ across medical professions. Furthermore, our assessment of care providers only does not fully realize the potential of exploring multilevel perspectives, which the PRISM supports. We did not directly assess patient-perceived barriers. Rather, clinicians provided their impressions of barriers faced by their patients. While this questionnaire identified perceived barriers related to public awareness and education, HIT/data, and clinical guidelines, the educational materials and resources we developed only addressed the public awareness and education domains.
Future Directions
We believe our findings provide an informative look at health center provider perceptions of the barriers to patient statin use. Further research could include larger numbers of health center providers, primary care providers in different settings, or specialty providers, like cardiologists.
One next step could be to explore why these perceptions exist. Perhaps, there are different factors that separately influence statin use in each of the high-risk groups; thus, intervention strategies may need to differ among groups.
Future practice should incorporate education and point-of-care decision tools into EHRs. These activities could provide point-of-care guidelines and risk calculators linked with prescription recommendations based on patient-specific data. We would also like to integrate hyperlipidemia treatment with other chronic conditions, such as diabetes or ASCVD, which are usually deemed as more important. An example would be to embed statin prescribing into EHR templates and order sets for other conditions. Addressing high cholesterol could similarly be woven in with other preventive measures to reduce risk of severe COVID-19.
In the future, as part of the full application of the PRISM, we plan to use the RE-AIM framework (RE-AIM.org, 2021) to assess how well our educational and training resources help overcome barriers to statin use in high-risk patients, including evaluating how key contextual factors influence successful implementation. This additional exploration of the relative importance of organizational and patient perspectives, organizational and patient characteristics, the external environment, and the implementation and sustainability infrastructure could yield important lessons and recommendations in using implementation science approaches in community health centers and in improving chronic disease management.
Conclusion
To improve quality of care for statin-eligible high-risk patients and guide future implementation practices, we conducted implementation research with target clinicians. Our questionnaire yielded important suggestions related to public awareness, education materials, HIT/data solutions, and clinical guidelines. It also informed the design of patient education resources and provider training tools. These materials included patient-centered, simplified, low-literacy, and multi-lingual teaching materials that help patients understand their cardiovascular risk and convey how statin therapy can help mitigate that risk. The tools should help care teams engage in effective conversations with patients about statin therapy and address medication adherence and access barriers. Provider resources include materials related to clinical indications for statin therapy for high-risk patients, education related to the latest cholesterol clinical guidelines in a variety of clear and actionable formats, and training and expert discussion on the safety and overall benefits of statins. Understanding the drivers of statin underuse, particularly in underserved and vulnerable populations is an important step in designing training, education materials, and other resources that can help increase appropriate statin use. Furthermore, using an implementation science approach (PRISM) sets up our interventions for further assessment within an implementation science framework (RE-AIM) (RE-AIM.org, 2021) to contribute to the advancement of health promotion practice in the field of evidence translation.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399221088592 – Supplemental material for Using the Practical Robust Implementation and Sustainability Model (PRISM) to Identify and Address Provider-Perceived Barriers to Optimal Statin Prescribing and Use in Community Health Centers
Supplemental material, sj-docx-1-hpp-10.1177_15248399221088592 for Using the Practical Robust Implementation and Sustainability Model (PRISM) to Identify and Address Provider-Perceived Barriers to Optimal Statin Prescribing and Use in Community Health Centers by Margaret Meador, R. Curtis Bay, Eboni Anderson, Debosree Roy, J. Aaron Allgood and Joy H. Lewis in Health Promotion Practice
Footnotes
Authors’ Note:
The authors wish to thank Kate Kirley, MD, MS and Linda Murakami, RN, BSN, MSHA from the American Medical Association for providing clinical expertise in informing the development of the statin barriers questionnaire and training and educational tools. The authors also wish to thank Laurence Sperling, MD, Judy Hannan, RN, MPH, Hilary Wall, MPH, Haley Stolp, MPH, and Lauren Owens, MPH from the Division for Heart Disease and Stroke Prevention at the Centers for Disease Control and Prevention for informing the development of educational tools and for advising the project. In addition, the authors wish to thank the following health center-controlled networks and their participating health centers for their dedicated work in this project:
• AllianceChicago
• DC Primary Care Association
• Health Choice Network
• HealthEfficient
• OCHIN
• Redwood Community Health Coalition
This project was funded by US Federal Award Identification Number (US) U8OT00223 from the Centers for Disease Control and Prevention. The findings and conclusions in this report are those of the authors and do not necessarily reflect the official position of the Centers for Disease Control and Prevention.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.