
Abstract
This is the second in a two-part series of articles about the Icelandic Model for Primary Prevention of Substance Use (IPM) in this volume of Health Promotion Practice. IPM is a community collaborative approach that has demonstrated remarkable effectiveness in reducing substance use initiation among youth in Iceland over the past 20 years. While the first article focused attention on the background context, theoretical orientation, evaluation and evidence of effectiveness, and the five guiding principles of the model, this second article describes the 10 core steps to practical implementation. Steps 1 to 3 focus on building and maintaining community capacity for model implementation. Steps 4 to 6 focus on implementing a rigorous system of data collection, processing, dissemination, and translation of findings. Steps 7 to 9 are designed to focus community attention and to maximize community engagement in creating and sustaining a social environment in which young people become progressively less likely to engage in substance use, including demonstrative examples from Iceland. And Step 10 focuses on the iterative, repetitive, and long-term nature of the IPM and describes a predictable arc of implementation-related opportunities and challenges. The article is concluded with a brief discussion about potential variation in community factors for implementation.
Introduction
This article comprises Part 2 of a two-part series (see Kristjansson et al., 2020, for Part 1) that documents the Icelandic Model for Primary Prevention of Substance Use. In the former article, we described the context, theoretical orientation, and five guiding principles that underlie the Icelandic Prevention Model’s (IPM) approach to adolescent substance use prevention, and summarized the evidence for effectiveness. In this article we describe the 10 core steps of effective practice-based implementation of the model.
The 10 Core Steps of the Icelandic Prevention Model
Heavily informed by the five guiding principles described in the previous article, the IPM is implemented using 10 core steps (see Table 1). Although there can be some variation in how individual communities implement each step, completing each step is essential to engaging community efforts to prevent substance use among young people. Steps 1 to 3 focus on building and maintaining community capacity for model implementation. Sometimes communities may already have parts of the demonstrated capacity to address the primary prevention of substance use, while other may not. Steps 4 to 9 focus on implementing a process designed to focus community attention and to maximize community engagement in creating a social environment in which young people become progressively less likely to engage in substance use. Finally, Step 10 focuses on the iterative, repetitive, and long-term nature of the IPM and describes a predictable arc of implementation-related opportunities and challenges.
Summary of the 10 Core Steps of the Icelandic Prevention Model
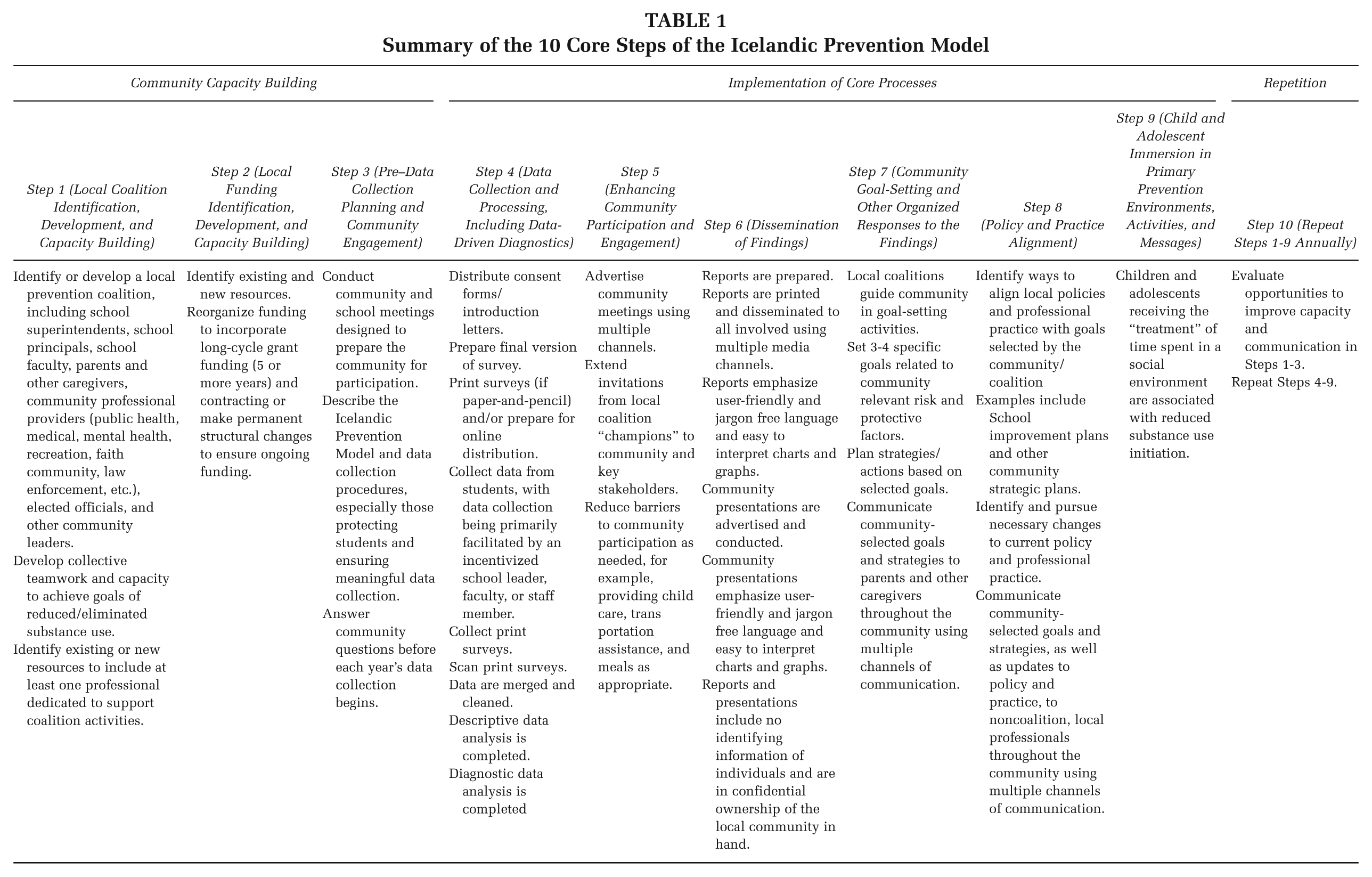
Step 1: Local Coalition Identification, Development, and Capacity Building
Because the IPM emphasizes changes in risk and protective factors at the local level, successful implementation of the model requires a local coalition or team to assume primary responsibility for implementation. Successful local coalitions include four main characteristics. First, maintaining a local ownership and grassroots orientation throughout their work. Although local coalitions often consult and benefit from the unique expertise of outside professionals, decisions should be made at the local level with a high degree of local ownership. Second, successful coalitions consist of a combination of key community members and a specific set of professionals serving in key roles. For example, high-performing coalitions often include school superintendents, principals, and faculty; parents and other caregivers; community professional providers (e.g., public health, medical, mental health, recreation, sports, faith community, law enforcement, etc.); elected officials; and social scientists/researchers able to work in an applied and community-engaged manner. Third, successful coalitions often include “local champions” who are respected members of the community and able to mobilize community and influence action. These individuals can draw a wide range of community members into the process and help the coalition access and garner support from key decision makers and funders. Perhaps most important, local champions should be consensus builders able to help community members and leaders find common priorities on which they can act together. Finally, the most successful coalitions find a way to fund at least one person with paid and protected time to build and maintain coalition capacity, to facilitate coalition activities, and to coordinate and conduct primary prevention implementation. This funding does not have to be new; often existing funds are reassigned for this purpose.
Step 2: Local Funding Identification, Development, and Capacity Building
The IPM intentionally emphasizes long-term contracting, grants, and collaboration as well as permanent reorganization of existing institutional and organizational infrastructure. One of the most important aspects of “matching the scope of the solution to the scope of the problem” (Guiding Principle 5 in Kristjansson et al., 2020) consists of matching how substance use prevention efforts are funded to the enormity of the problem. Changing the social environment takes time. As a result, short-term grants will always be an insufficient means of initiating and sustaining the cultural and community change necessary to prevent future substance use, especially in areas already burdened by a high prevalence of use.
Therefore, the IPM encourages establishing and distributing funding in a minimum of 5-year increments. This shift in funding strategy does not necessarily require an increase in total money spent. Over time, like most true primary prevention approaches, the model promises to be an extremely cost-effective means of reducing the total social and financial costs associated with substance abuse. However, creating these long-term benefits requires that initial investments in efforts designed to change the social environment are given adequate time to do so. In many communities, this requires initiating systems-level changes that include considering how to redeploy existing community financial resources.
Step 3: Pre–Data Collection Planning and Community Engagement
Activities in this step are meant to extend support from the local coalition into the communities themselves. To do so, the local coalition works to raise awareness related to community substance use prevention goals and the model as an intervention framework meant to reduce rates of youth substance use initiation.
Establishing community awareness and support are essential for several reasons. First, the IPM intervention approach is primarily implemented through the routine, day-to-day efforts of local adults as supported by the efforts of engaged local professionals. Early engagement and ownership of the process represent one way to maximize community participation. Second, making community members aware of the data collection procedures, explaining how the data collection team ensures it is safe for students to provide honest responses, and responding to community concerns and questions before data collection begins help ensure community trust in the integrity of the research and high rates of student participation. High levels of student participation are critical; acquiring a response rate of 80% or higher at each school facilitates accurate diagnostics and eliminates concerns by local personnel about whether the data accurately represent their specific school-community. Third, making decisions based on high-quality data is central to the IPM. Therefore, ensuring high-quality data collection maximizes the practice-based utility of data and subsequent data-driven diagnostics. Confidence in the data increases the likelihood that they will be used by the coalition and the community in future model steps.
Step 4: Data Collection and Processing, Including Data-Driven Diagnostics
Annually, or bi-annually, data are collected from each individual school and used to (a) monitor rates of student substance use over time, (b) identify locally relevant risk and protective factors that contribute to rates of substance use, and (c) make strategic decisions tailored to each specific school and the area it represents.
The IPM requires population-based data collection within individual local schools, and is not based on samples, randomly assigned or otherwise. This means that the data collection team attempts to collect data from all students in each school. In most cases, because the model is primarily an intervention activity designed for environmental change instead of a research activity, and is conducted without identifying individuals, parental consent has not been required by participating university institutional review boards and government agencies. In addition to the awareness activities described in Step 3 above, parental notification letters are sent to all parents with instructions for what to do if they would not like their child to participate in the survey. Through the combined efforts described in Step 3 and the “opt out” orientation of the parental notification letters, response rates of over 80% are routinely achieved.
The IPM survey includes measures about the incidence and prevalence of substance use in the school-community, as well as those related to the risk and protective factors found in the broader social environment, including well-established risk and protective factors in the model’s four main intervention domains: (a) parents and family, (b) school, (c) peer group, and (d) leisure time outside of school.
IPM data are then analyzed with the goal of providing each school-community with diagnostic information describing “essential factors” in their environment. The IPM analysis begins by describing rates of substance use and trends in usage over time. But the central thrust of IPM data analysis is to determine the relative importance of various risk and protective factors on adolescent substance use in each specific school-community, thus ensuring that local coalitions and other community members can identify promising targets of intervention specific to the young people in their areas.
Finally, all data are collected via local schools. Most schools are already heavily tasked and underresourced. Therefore, it is essential to carefully prepare schools for data collection, to minimize the intrusion on school personnel, and to protect school personnel from any negative consequences associated with disappointing findings. Although schools are central to the IPM, they are not primarily responsible for rates of student substance use in any community. Taking steps to ensure that the whole community equitably shoulders responsibility for student substance use helps keep schools engaged in the data collection activities central to the IPM. For more detailed information about IPM data collection, see Kristjansson, Sigfusson, Sigfusdottir, and Allegrante (2013) for a previously published step-by-step description of data collection and preparation procedures.
Step 5: Enhancing Community Participation and Engagement
Although local coalition members and stakeholders are critical to the success of the IPM, parents, caregivers, other professionals, and community members play a comparatively outsized role as well. Changing the social environment requires the collaborative participation of a wide range of community members. Therefore, effective implementation of prevention strategies (see Steps 7-9) requires outreach designed to maximize community participation and engagement in all aspects of the approach. Although the specific strategies selected depend heavily on the norms of the community, it is essential to use appropriate communications and marketing strategies to increase community awareness and uptake of the efforts that will be described in Step 6. For example, encouraging community members to access dissemination reports, attend community presentations and goal-setting meetings, and participate in prevention-oriented activities. Additionally, it is critical to consider and address additional barriers to participation in upcoming activities such as by providing food, child care, and transportation assistance at community meetings as needed. Early notice, open communication, and barrier-free participation, especially in the context of community social norms that addressing and preventing youth substance use is important, increases community engagement in following IPM steps.
Step 6: Dissemination of Findings
Within 2 to 3 months post each data collection, a detailed report on risk and protective factors and substance use outcomes is prepared by the research team and widely disseminated within each school-community. Report receivers typically include parental groups, school faculty and staff, and other relevant professionals at the school-community level; higher level administrative units such as county, municipality, or area representatives; and elected officials. The model prioritizes a quick turnaround to ensure the real-time utility of the data. All model reports use accessible, jargon-free language and present data using easily understood bar charts and line graphs whenever possible. The goal is for all model reports to be readable and easily understood by majority of community members.
Each report presents results from the data analysis and diagnostic strategies outlined in Step 4 above and include (a) describing rates of current substance use and trends over time and (b) identifying levels of locally relevant risk and protective factors and their relationship to community substance use. Typically, charts include a comparison between each school-community to other unidentified school-communities in the area. Most often, these data are presented in a chart with only the local school-community being featured in the report being identified. Providing comparison data has proven important, as it allows coalition and community members to understand their progress relative to other communities in the area.
Another central feature of the IPM includes considering the needs of noncoalition key stakeholders and presenting data in a manner likely to motivate them to align with and support the model and partake in future prevention activities. The model assumes that providing key stakeholders with data relevant to the level at which they are responsible is more likely to motivate corresponding action at that level than a collection of school-community reports. For instance, in addition to each local school-community report, additional reports are developed that align with the socioecological level that various key stakeholders serve. While school-neighborhood–level officials receive a report summarizing a specific school-neighborhood, school district–, city-, or state-level officials receive reports that are aligned with their catchment area. In this way, local community members bring heightened attention and motivation to data that describes what is happening in their school-communities, whereas higher level officials may bring attention and motivation to data that primarily align with their areas of concern.
Usually, coalition members, community members, and key stakeholders access the information presented in the annual or biannual reports through a community meeting or worksite meeting (e.g., school faculty and staff, county/municipal professionals, elected officials). Such meetings follow the same basic principles as the reports. They prioritize accessible, jargon-free language and present data visually whenever possible. Community meetings are designed to present data in a manner that maximizes community engagement, decision making, and commitment to participate in prevention activities. Often, existing school-based parent groups offer access to their memberships and align their meetings to ensure member participation in the IPM. In some cases, communities use social marketing to extend dissemination of report findings through a wide variety of media channels.
In all cases the local coalition retains ownership of all data collected, as well as all reports and presentations distributed, regardless of whom they may have hired or contracted with to complete these services. Furthermore, decisions regarding how to distribute each report and presentation materials are made by the local coalition sponsoring the IPM.
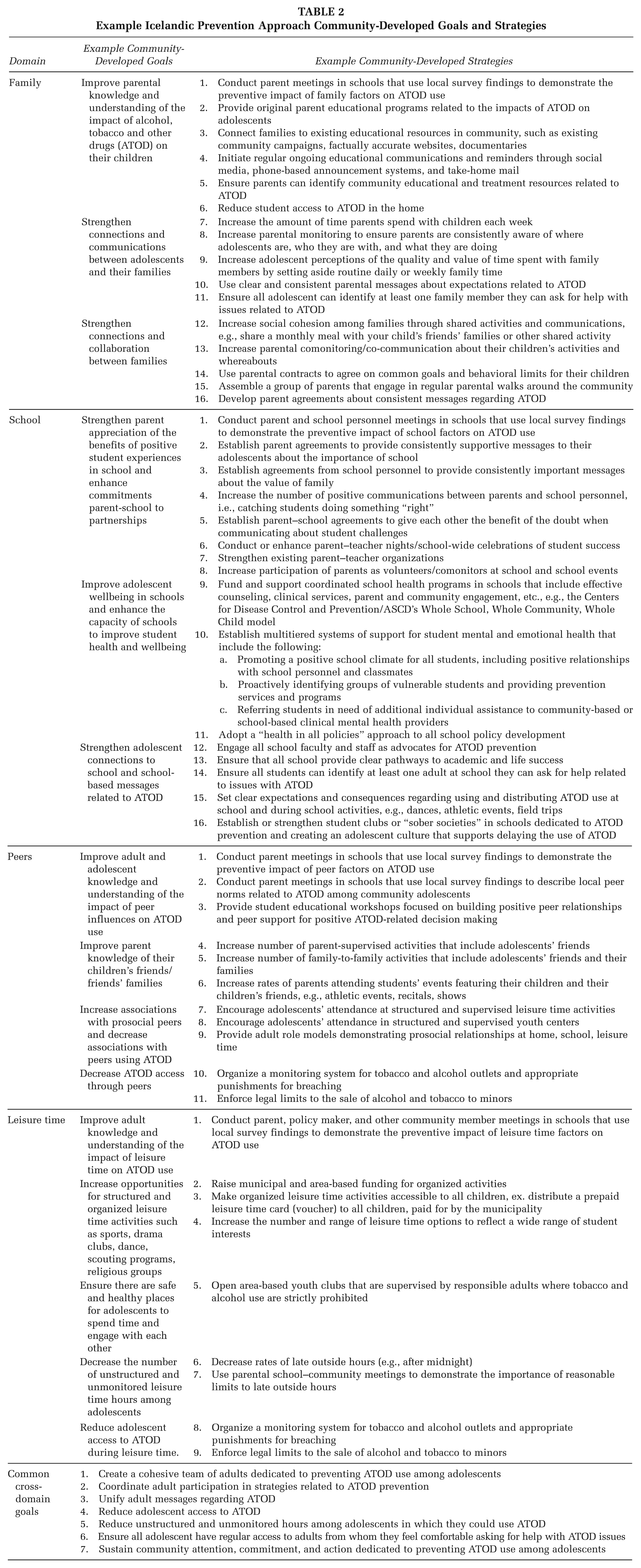
Step 7: Community Goal-Setting and Other Organized Responses to the Findings
The desired outcome of Steps 1 to 6 is that the local coalition will have led the way in establishing three to four widely supported community goals. Informed by the research evidence and local knowledge of area-based norms and culture, these goals should be focused on reducing risk factors and strengthening protective factors for substance use initiation identified as being especially relevant to the community. Goals should also include specific strategies tailored for success within the community context. Assuming that communities differ widely, the selection of goals and strategies is heavily dependent on local knowledge regarding what goals will resonate among community members and what implementation strategies are most likely to work in each specific school-community. Individuals may require less motivation to do what they want to do. Likewise, communities may need less motivation to do what resonates with the community as a whole. Therefore, a key aspect of the IPM is a reliance on the wisdom of the local coalition to prioritize goal setting that makes sense to them and is aligned with the research findings. Table 2 includes a menu of examples of commonly selected community goals and strategies that have been widely used as part of the IPM.
Example Icelandic Prevention Approach Community-Developed Goals and Strategies
Step 8: Policy and Practice Alignment
Once core community goals and strategies are selected by establishing a consensus among community members and researchers, the local coalition works to identify key policies and local mechanisms for achieving the community’s intended outcomes and aligning those goals with current policy and practice. This is where administrative leaders and elected officials are often brought into the picture. As examples, in the United States, School Improvement Plans provide an opportunity to align model goals with existing monitoring and enforcement mechanisms. Similarly, in Iceland, the IPM survey findings have influenced laws around cigarette and alcohol advertisement, guiding regulations on outside hours, and parental norms on community-based monitoring efforts.
While Step 6 focused on activating the participation of the community-at-large, Step 8 focuses on activating and aligning the policy-making and professional practice communities with broader community goals. Because a central feature of the IPM is collaboration among groups of people that commonly do not engage with one another, the IPM relies on policy makers and relevant professionals to join community groups as partners willing to add professional weight to locally derived goals and strategies. This type of local–professional integration typifies the model’s framework and approach to substance use prevention. Community leadership and participation supported and enhanced by organized professional action.
Step 9: Child and Adolescent Immersion in Primary Prevention Environments, Activities, and Messages
After selecting goals and strategies to reduce risk factors and strengthen protective factors in Step 7 and aligning them with current policies and practice in Step 8, the community is now ready to immerse children and adolescents in the environment designed to achieve these goals. If the core goal of the IPM is changing the social environment, then the core treatment of the model is exposing children and adolescents to changed environments that are aligned with the model’s theoretical propositions about preventing substance use initiation. When high-quality data and local diagnostics are properly aligned with community-specific knowledge about what will work in each community, then youth in those environments will be less likely to initiate substance use over time. Therefore, Step 9 focuses on maximizing student exposure to a social environment that is unlikely to breed substance use. Below are demonstrative examples of four goals and five strategies that many municipalities and communities in Iceland have successfully operated as part of their implementation of the model:
Goals
Employ special prevention workers in all municipalities (full-time) and schools within them (part-time) with protected time to work on primary prevention.
Strengthen parental groups at the school-community level.
Decrease late outside hours and unsupervised parties.
Increase participation in organized recreational and extracurricular activities.
Strategies
Prevention workers communicate with parental groups at the school-community level to increase participation and involvement. Organize regular parental meetings.
At parental meetings the research findings are introduced by the research team and used to demonstrate the importance of the issue and that parents need to work together to prevent substance use by their and other youth in the community.
Policy makers create guidelines around outside hours based on summer and winter sunlight periods. The guidelines are widely disseminated and advertised.
Empowered by participation in parental groups in schools, parents mutually agree to not allow alcohol and other substance use by youth in their homes, to prevent unsupervised parties, and to follow guidelines for outside hours made by policy makers.
Policy makers and municipal administrative leaders increase funding for organized recreational and extracurricular activities and create a platform to make such opportunities available to all children and youth.
To cut a long story short, the result of these goals and strategies have been that parental collaboration and co-communication at the local level has been improved substantially throughout large parts of the country, and parental monitoring has increased. Furthermore, late outside hours and participation in unsupervised parties among youth have both decreased greatly, and participation in organized activities such as sports, music, drama clubs, and so on, has increased significantly (Kristjansson et al., 2016; Kristjansson, James, Allegrante, Sigfusdottir, & Helgason, 2010). These holistic changes have then led to decrease in substance use initiation among youth in the country.
Step 10. Repeat Steps 1 to 9 Annually
The effects of the IPM are considerably strengthened over time. At a fundamental level, the model relies on a repetitive and iterative process that increasingly permeates the social and cultural fabric of each school-community year by year. This approach assumes that the relationships among the local coalition and the capacity established between researchers, administrative leaders, policy makers, practitioners, and community members will strengthen if properly attend to in Steps 1 to 3. Similarly, the data collection, analysis, reporting, goal-setting, and alignment described in Steps 4 to 9 will also deepen with repeated use. Continued utilization of research findings to evaluate if progress is being made in the selected goals and strategies will lead to reaffirmation by the community to continue the work. Ultimately, the goal of the IPM is to facilitate a paradigm shift in community norms and culture. A paradigm shift is established incrementally and will most likely require years to fully solidify in most communities. Therefore, repetition and continuation are essential parts of “matching the scope of the solution to the scope of the problem.”
Discussion
The IPM proposes the tailoring of specific intervention processes that are consistent with local needs. Therefore, strong participation and collaboration among local community members are essential. Although researchers will provide the results of analyses of routine data to guide community-level practice and give regular feedback, a high degree of participation and leadership among local personnel is necessary to facilitate a long-term change in behavioral sanctions and norms (Sigfusdottir, Kristjansson, Gudmundsdottir, & Allegrante, 2011; Sigfusdottir, Thorlindsson, Kristjansson, Roe, & Allegrante, 2009). As such, the mechanisms underlying the risk and protective factors within the four domains of parents and family, peer group, school, and leisure time that were emphasized in Iceland may not necessarily be appropriate elsewhere. For example, as stated earlier, in Iceland the most effective approach to strong parental involvement and collaboration at the local community level is the parent–teacher organizations within schools. Those are typically organized and maintained by the schools with support from the municipalities. In other places, the local church may be better suited to bring parents together for this purpose. Put differently, what may have worked in Iceland to get parents organized may not necessarily work in other countries. Another example is the area-based sports teams that have played an important role for prevention in Iceland. In other places, schools are often the main provider of organized sports. Whether the data will show sports participation that is affiliated with schools, and that functions similarly for prevention to the area-based teams in Iceland, is a question to be assessed.
With regard to overcoming the challenges of implementation (see Kristjansson et al., 2020), we underline the guiding principles (the first article) and 10 core steps to implementation (this article) that have been formulated largely in response to the challenges presented in standardizing our description of implementation with this flexible approach. Through experience, both domestically in Iceland and in several other countries, we have learned that when municipalities, cities, and/or other organizational units follow this process, they do tend to produce better outcomes. Furthermore, the IPM is deeply rooted in the premise of collaboration. This is important both across organizations and among individuals, professionals, and laypeople alike. In this respect, the model can be regarded as a process tool to facilitate collaboration for substance use prevention. Challenging the organizational silos and nontransferable funding lines that are often a feature of efforts may be necessary. Team building, capacity assessment, and the procurement of secure funding on the front end of the approach will be paramount for future success. Allowing sufficient time to achieve this capacity building is critical for success in the post–data collection and dissemination phases of implementation. Moreover, allowing the inclusion of all relevant stakeholders in the effort of immersing youth in intervention activities post data translation and local dialogue has shown to be critical for sustainable success of substance use prevention.
In conclusion, the IPM is not a program in the conventional sense but rather a local community collaborative. It emphasizes primary prevention and a shift in local community norms and culture that can be achieved only with access to practice-based local data (Green, 2006, 2008), long-term intervention efforts across a spectrum of prevention activities (Cohen & Swift, 1999), and substantial local input and community voice.