
Abstract
Asthma affects 7.1 million children in the United States, disproportionately burdening African American and Latino children. Barriers to asthma control include insufficient patient education and fragmented care. Care coordination represents a compelling approach to improve quality of care and address disparities in asthma. The sites of The Merck Childhood Asthma Network Care Coordination Programs implemented different models of care coordination to suit specific settings—school district, clinic or health care system, and community—and organizational structures. A variety of qualitative data sources were analyzed to determine the role setting played in the manifestation of care coordination at each site. There were inherent strengths and challenges of implementing care coordination in each of the settings, and each site used unique strategies to deliver their programs. The relationship between the lead implementing unit and entities that provided (1) access to the priority population and (2) clinical services to program participants played a critical role in the structure of the programs. The level of support and infrastructure provided by these entities to the lead implementing unit influenced how participants were identified and how asthma care coordinators were integrated into the clinical care team.
Keywords
Introduction
Asthma affects 7.1 million children (9.5%) in the United States and is a leading cause of school absences and activity limitations (Akinbami, Moorman, & Liu, 2011; Centers for Disease Control and Prevention, 2013; Moorman et al., 2012). Non-Hispanic Black (16%) and Hispanic children (10%) are more likely to have asthma than non-Hispanic White children (8%). Race/ethnicity-based disparities in health care utilization for asthma are marked, with more frequent emergency department (ED) visits or hospitalizations among African American and Hispanic children compared to White children (Akinbami et al., 2011; Ginde, Espinola, & Camargo, 2008). Barriers to asthma control include insufficient patient education (Holsey, Collins, & Zahran, 2013; Oraka, Iqbal, Flanders, Brinker, & Garbe, 2013), fragmented care and lack of coordination between clinic and community services (Butz, Kub, Bellin, & Frick, 2013; Krieger et al., 2006), psychosocial stressors (Koinis-Mitchell, Kopel, Salcedo, McCue, & McQuaid, 2014; Wright et al., 2004), perceived financial burden (Patel, Brown, & Clark, 2013), and home triggers such as tobacco smoke exposure, mold, pests, and dust (Crain et al., 2002; Everhart et al., 2011). Care coordination for asthma is one comprehensive strategy to address these barriers. Care coordination is a client-centered, assessment-based interdisciplinary approach to integrating health care and social support services in which an individual’s needs and preferences are assessed, a comprehensive care plan is developed, and services are managed and monitored by a care coordinator following evidence-based standards of care. (Brown, 2009, p. 1)
Care coordination engages multiple stakeholders, such as family members, health care providers, social services, schools, and community organizations (Bodenheimer, 2008). Care coordination has been shown to reduce asthma symptoms, unscheduled health care use, activity limitations, and school absences, among other positive outcomes (Clark et al., 2010; Clark et al., 2013; Coughey et al., 2010; Mansfield et al., 2011; Thyne, Rising, Legion, & Love, 2006).
The Merck Childhood Asthma Network Care Coordination Programs
The Merck Childhood Asthma Network (MCAN) Care Coordination Programs, Phases 1 and 2, aimed to reduce pediatric asthma morbidity in vulnerable populations. In Phase 1, five sites implemented evidence-based interventions (EBIs) to improve outcomes and explore the factors that led to successful adoption of EBIs in urban settings (Viswanathan et al., 2011). These interventions yielded improvements in symptoms, hospital and ED use, school absences, and caregiver confidence (Banda et al., 2013; Lara et al., 2011; Lara et al., 2013; Mansfield et al., 2011; Turyk et al., 2013). Whereas not all work in Phase 1 focused on care coordination, in a second phase, the four sites selected to continue emphasized care coordination activities. Phase 2 sites are the school-based Los Angeles Unified School District Asthma Program (Los Angeles, California), the health system–based Children’s Hospital of Philadelphia Asthma Care Navigator Program (Philadelphia, Pennsylvania), the Federally Qualified Health Center–based (FQHC) La Red de Asma Infantil de Puerto Rico (San Juan, Puerto Rico), and the community-based Addressing Asthma in Englewood Project (Chicago, Illinois). Due to its care coordination focus, the relative strength of its evidence base, and its success with similar vulnerable populations, all sites chose to adapt the EBI Yes We Can, a medical-social model of care that deploys health workers (referred to as asthma care coordinators [ACCs] for the purposes of this article) to provide asthma education, link families to health and social services, and facilitate communication between the patient and clinicians (Thyne et al., 2006; Thyne & Fisher-Owens, 2011; Thyne, Marmor, Madden, & Herrick, 2007).
Variation across Phase 2 sites provides a unique opportunity to examine the strengths and challenges of implementing asthma care coordination in different institutional and organizational settings. The effect setting has on the manifestation of care coordination for pediatric asthma has not been well documented in the literature. The goal of this article is to use qualitative implementation data to assess (1) the influence of these settings on the structure of care coordination activities, (2) the strengths of implementing care coordination for asthma in a given setting, and (3) the primary challenges that arise. This investigation contributes to the knowledge base on effective models of asthma care coordination across a range of settings, and findings can be used to inform program planning, reimbursement or other funding decisions, and future research priorities.
Method
Data Sources
Members of the University of Michigan cross-site evaluation team used multiple qualitative data sources in the analysis (Table 1): annual site report forms that tracked program components, reach, partnerships, and efforts to effect system and policy change; notes of key informant interviews (verified by audio recordings) with program leaders and ACCs; minutes from quarterly conference calls with sites; and site-completed surveys regarding their perspectives on the influence of the site’s setting on care coordination (there was a 100% response rate from the sites with respect to these data sources).
MCAN Asthma Care Coordination Programs Cross-Site Evaluation Data Sources
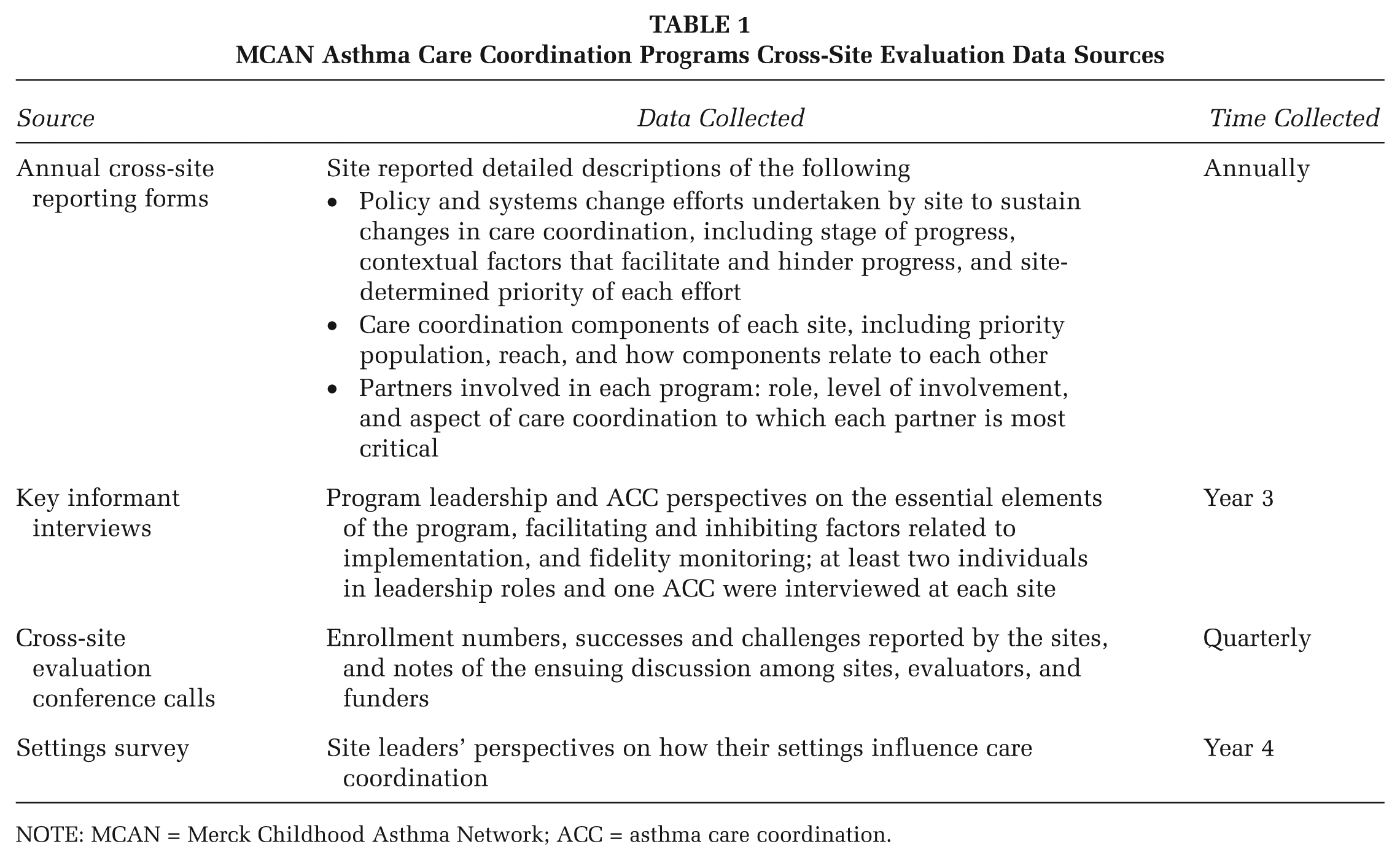
NOTE: MCAN = Merck Childhood Asthma Network; ACC = asthma care coordination.
Analysis
To guide data collection and analysis, the cross-site evaluation used the RE-AIM (Reach, Effectiveness, Adoption, Implementation, Maintenance) framework (Glasgow, Vogt, & Boles, 1999) as well as the factors affecting implementation that were identified by Durlak and DuPre (2008), which include those related to setting such as organizational capacity. While collecting data from the sites over time, the researchers inductively uncovered the concept (which later became the study hypothesis) that the type of setting in which a care coordination program takes place influences how it carries out key functions, representing a form of grounded theory generated from the qualitative data (Patton, 2002). As a preliminary step, researchers read through notes and other data sources and constructed narrative summaries identifying each site’s program activities and sequence. A leader from each MCAN site reviewed the summary for accuracy. Researchers then compared the verified narrative summaries to identify commonalities and differences across sites.
Next, two members of the cross-site evaluation team conducted an inductive theme analysis (Patton, 2002), based on a review of sources listed in Table 1 (with the exception of the Settings Survey), to identify strengths and challenges associated with the care coordination structure in each of the four sites. The researchers used a priori definitions of strengths (i.e., things inherent in a particular structure/setting that facilitated delivery of care coordination services) and challenges (things inherent in a structure/setting that hindered services). Next, strengths/challenges were categorized by dimensions of the care coordination process that emerged from the analysis. Consensus meetings were held with a third researcher to reach agreement regarding both the strengths/challenges and the categorization scheme. As a preliminary step for validating these categories (Miles & Huberman, 1994), we asked site leaders to complete a brief, open-ended survey on the categories and collect any further relevant site perspectives on the topic. Their responses confirmed the categorization, and a few new perspectives were added to the initial findings. As a final verification step, the researchers sought informant feedback (Miles & Huberman, 1994) by presenting preliminary analysis results in table format to MCAN site leaders and making changes as needed.
Results
Care Coordination Activities Common to All Sites
As an initial step in examining how setting influenced the structure of care coordination, an analysis of narrative summaries was conducted to determine the similarities and differences in care coordination activities. The comparison revealed a common set of activities across sites, including asthma education, a home assessment, and follow-up calls or visits (Table 2). The sequence varies from site to site, and each program allows for flexibility in their care pathway; for example, an ACC may make additional calls between home visits to a high-need family.
Observed Care Coordination Activities Common Across All MCAN Sites
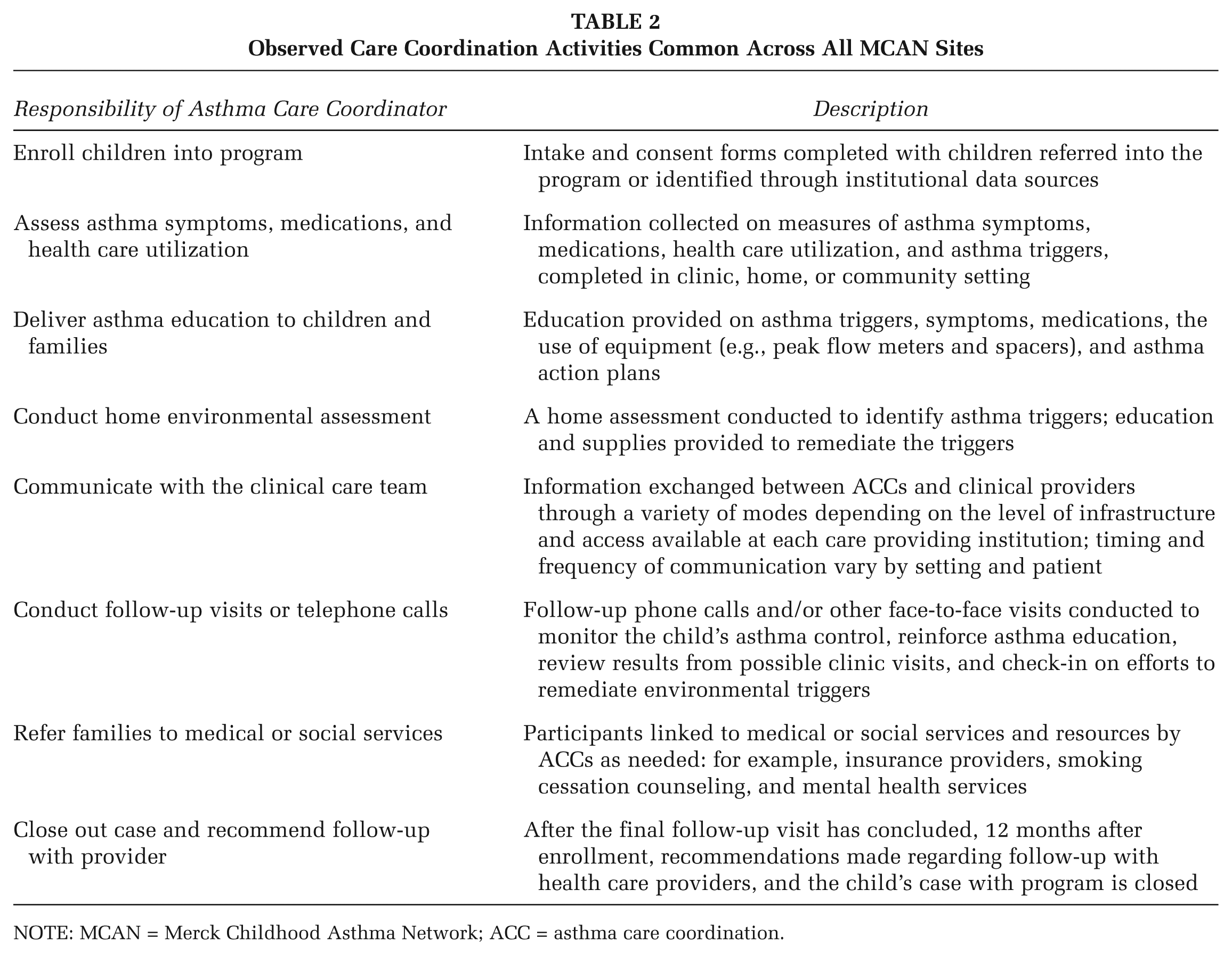
NOTE: MCAN = Merck Childhood Asthma Network; ACC = asthma care coordination.
Defining “Settings”
While analyzing the narrative summaries, it became clear that the functional relationships of the lead implementing unit (LIU) to key partners needed to be accounted for in the definition of “settings.” For this analysis, LIU was defined as the group of individuals leading the design and implementation of the program. In all four sites, each LIU consists of a project director, manager, and the ACCs, all employed by the institution that is the fiduciary of the grant. Two types of partners played a critical role in how care coordination is structured: those that (1) provide access to the priority population and (2) provide clinical services to program participants. The ability of the LIU to identify participants, exchange information about participants, and integrate ACCs into clinical practice hinges on the support of these partners. Table 3 describes each site’s LIU, priority population, as well as the LIU’s relationship to partners for access and clinical care.
Characteristics of participating MCAN Asthma Care Coordination Programs
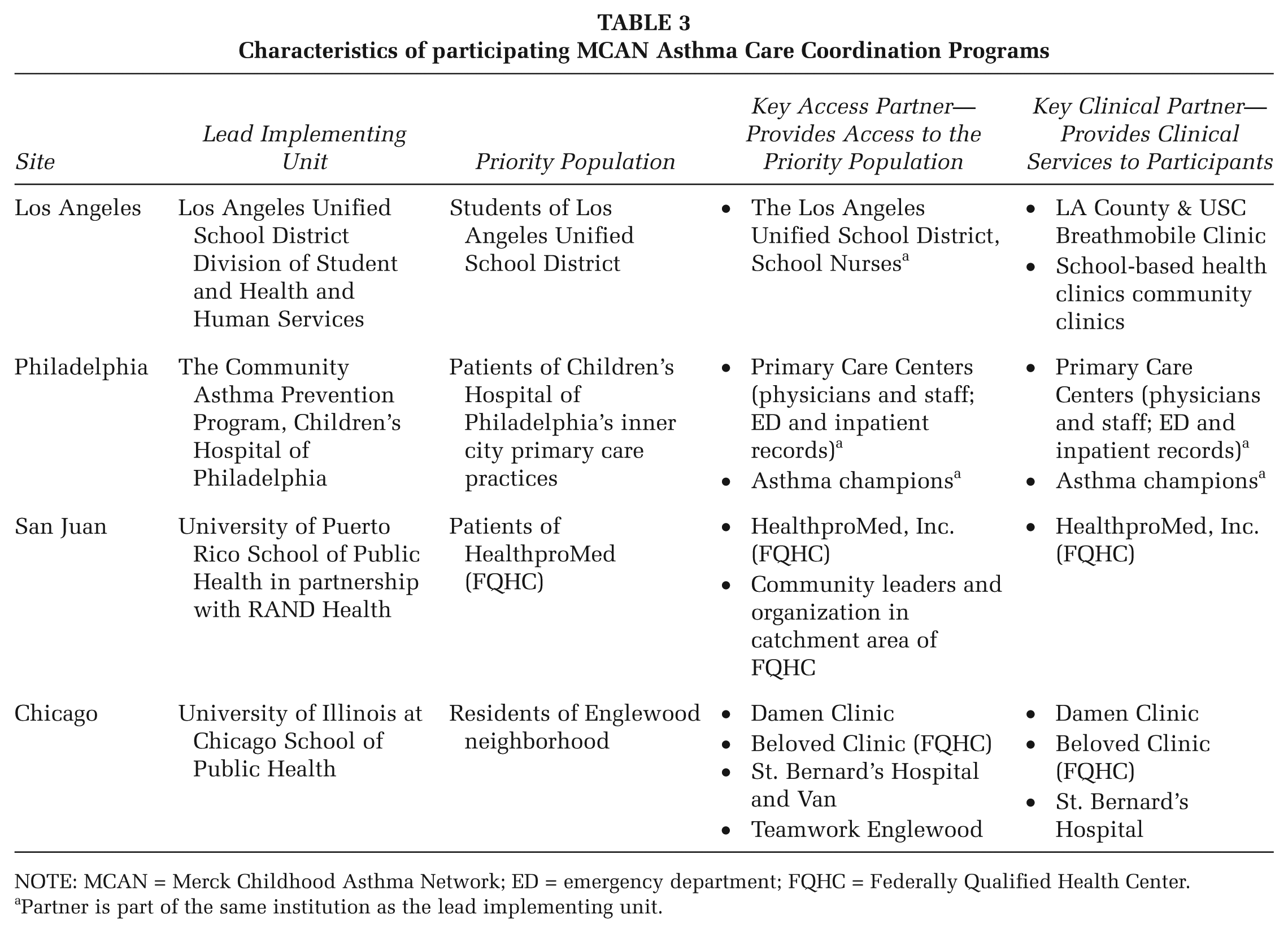
NOTE: MCAN = Merck Childhood Asthma Network; ED = emergency department; FQHC = Federally Qualified Health Center.
Partner is part of the same institution as the lead implementing unit.
Two broad categories emerged in how setting, as defined above, influences care coordination: (1) identification of participants and (2) the integration of ACCs with the clinical care team. Substantial differences in these two categories exist across sites. The strengths and challenges observed in each setting, according to these categories, are described below and summarized in Table 4.
Summary of Strengths and Challenges Associated With the Lead Implementation Unit and Primary Setting for Implementation
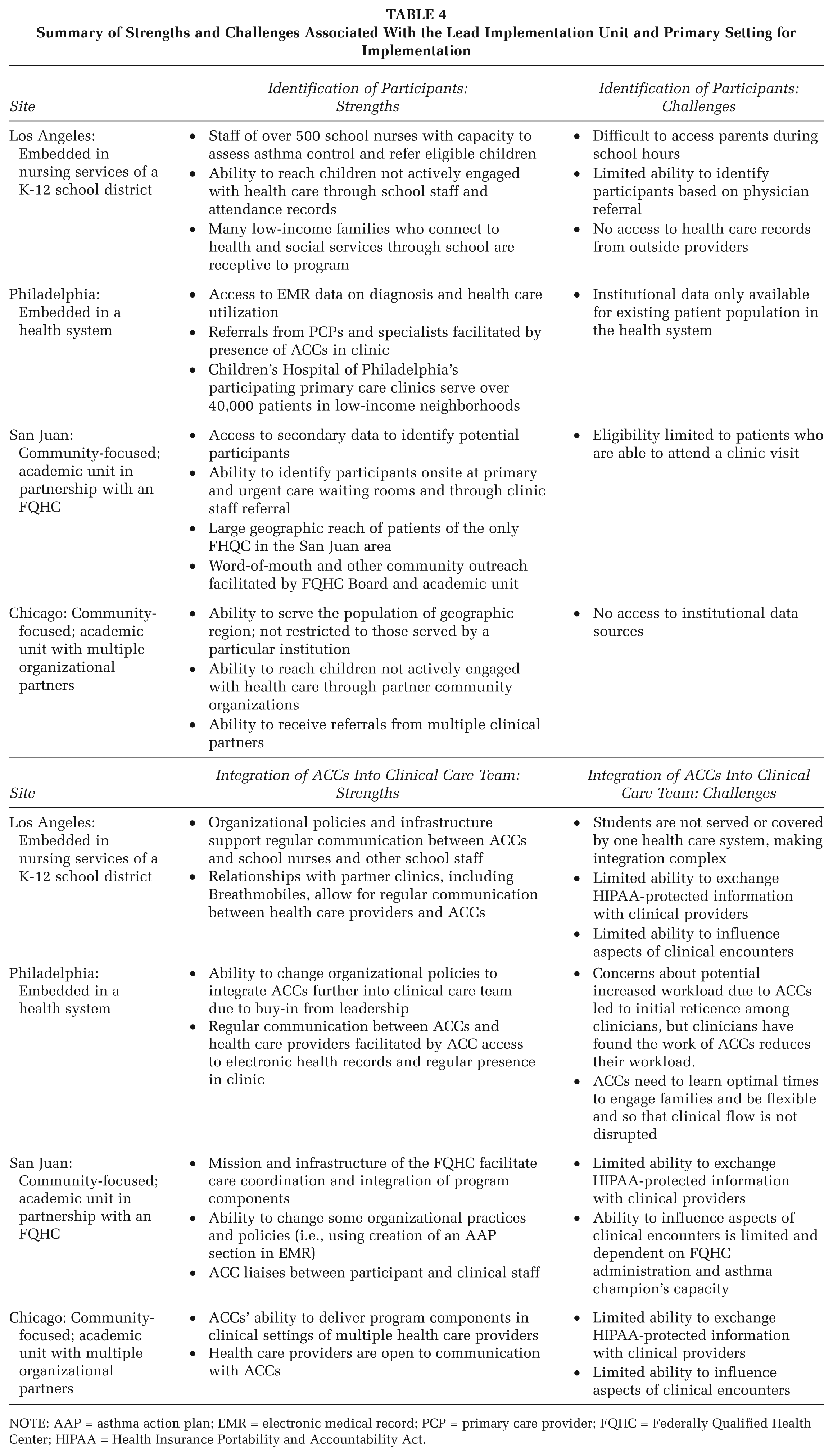
NOTE: AAP = asthma action plan; EMR = electronic medical record; PCP = primary care provider; FQHC = Federally Qualified Health Center; HIPAA = Health Insurance Portability and Accountability Act.
Identification of Participants
Los Angeles: School-Based Participant Identification
Enrollees are children with poor asthma control who reside in Los Angeles Unified School District boundaries. The ACCs are school nurses who specialize in asthma. They receive referrals from the district’s nearly 500 school nurses and school administrators, teachers, attendance counselors, parents, and clinicians at the partner clinics, including a mobile asthma van program (Breathmobiles). Each ACC works with the Los Angeles Unified School District’s nurses in a defined geographic region. The program provides comprehensive training for school nurses, which includes assessment of asthma control, and school nurses use a standardized process to refer students with poor control to the program.
Identifying and helping children through a school system has several advantages. For many low-income families, schools are a primary connection with health and social services; therefore they are often receptive to program services. A program is able to reach students at school, in a safe and convenient environment, and students with poor asthma control can be identified based on staff observation, attendance records, and academic performance. However, while an ACC can easily reach students, reaching parents can be more difficult, and the program requires parental consent and participation. ACCs thus may educate students and parents in separate appointments (e.g., one at school, one at home).
Philadelphia: Health System–Based Participant Identification
The program in the Children’s Hospital of Philadelphia’s system identifies high-risk patients through review of asthma inpatient and ED report and electronic medical records (EMRs) of children seen in primary care centers, and physician referrals.
EMR access is a significant advantage of working from within the health system. The combination of using EMR data to identify eligible participants and the recruitment efforts of ACCs, who are, importantly, staff members within the primary care clinic of potential participants, is particularly advantageous. In contrast to programs that rely on primary care provider (PCP) records or referrals, the Children’s Hospital of Philadelphia’s program is able to identify serious cases that might otherwise go unnoticed if the family does not schedule a follow-up visit with their PCP after an ED visit or hospitalization. Additionally, access to EMRs allows the program to easily identify those who meet enrollment criteria. While participation is restricted to patients in the health system, the Children’s Hospital of Philadelphia’s reach in the area is extensive. Furthermore, the model is replicable and will likely appeal to future Accountable Care Organizations.
San Juan: Clinic-Based Participant Identification
In San Juan, program success depends on the partnership between the researchers and HealthproMed administration and clinicians, and their capacity to partner with local community leaders and agencies for outreach and recruitment. Project staff identifies eligible children by screening potentially eligible families in the clinic’s waiting rooms. These efforts are supplemented by outreach strategies in collaboration with HealthproMed’s Community Advisory Board and staff, who identify potential patients based on secondary claims data. Potential participants are invited to the clinic in order to be screened and consented.
Because HealthproMed is the only FQHC in San Juan, the potential catchment area is geographically large. Access to claims data allows HealthproMed to identify high ED and hospital users. Finally, children coming in to the clinic with exacerbation of symptoms are a “captive” population that is likely to be eligible. However, only clinic patients can be screened and enrolled in the program.
Chicago: Community-Based Participant Identification
The priority population in Chicago is a geographically defined community on the south side. The ACC recruits families at clinics and community events; participants are also referred by physicians, schools, community-based organizations, and word of mouth. One benefit of this approach is that Chicago is able to reach a broad population within a specific community and is not limited to the population of one institution. This approach also allows Chicago to reach children not actively engaged with health care through relationships with community members and organizations. Unlike the other programs that only enroll children with poorly controlled persistent asthma, the Chicago program also serves children with intermittent asthma, as (1) community leaders made clear that denying access to children with less severe diagnoses would not be acceptable to the community and (2) information about asthma control is not always readily available or consistent across the priority population.
To reach a geographically defined population, rather than one served by an institution, demands a great deal of resources to nurture relationships with the diverse referral sources needed to identify eligible children. Additionally, demonstrating the program’s value to multiple organizations may be more challenging than when programs are embedded within a single institution, where established feedback channels to internal referral sources, such as school nurses and PCPs, demonstrate the program’s positive impacts. However, by creating and strengthening relationships with other community organizations and institutions, Chicago was able overcome these barriers and link families with other needed services in the community.
Integration of ACCs
Integration of ACCs into the clinical care team is the second major difference among care coordination sites. “Integration” represents the acceptance of the ACC role by the health care team, incorporation of ACC into the clinic’s workflow when possible, communication between ACCs and health care providers, and sharing of resources with the ACC to facilitate care coordination. Integration of the ACC is an essential element of MCAN’s Care Coordination Programs. Care coordination by the MCAN programs relies on the ACC to provide the link between care delivered outside and inside of the health care office. Limited integration restricts the level of coordination possible.
Los Angeles: School-Based Integration
ACCs and other school nurses communicate with each other through the electronic student health record (e.g., with notes on the completion of program components, results of assessments, supplies and medications provided, and prompts for follow-up). However, due to the separation between the school system and external health care providers, integration with clinical providers is not standardized. Students enrolled in Los Angeles’ program receive care from the Breathmobile or their own private provider. The ACCs provide updates to clinicians during the Breathmobile’s visits to the participants’ schools, and Breathmobile clinicians update ACCs on patient visits, health status, and requests for follow-up from the ACC. Breathmobile clinicians complete an asthma action plan (AAP) for each child that is shared with the ACC. Formal meetings between the ACCs and the Breathmobile clinical team occur every 2 to 3 months in order to discuss program coordination issues. For other providers, communication is not as regular or direct. For example, the ACCs ask parents to deliver uncompleted AAPs to be filled out by the provider. In both cases, sharing of protected personal information is limited by the Family Educational Rights and Privacy Act and the Health Insurance Portability and Accountability Act restrictions as well as the strength of relationships between the program and clinicians.
Philadelphia: Health System–Based Integration
Philadelphia, as a result of being embedded within the same institution providing clinical services, has been able to more fully integrate ACCs into a team of health care providers and to influence clinical encounters, for example, physician adherence to national guidelines for asthma diagnosis and management (National Heart, Lung, and Blood Institute, 2007). To facilitate regular ACC–provider information exchange, health system policies were changed to allow ACCs to view EMR snapshots and enter notes on asthma symptoms, environmental findings from home visits, psychosocial barriers, and referrals to community services. Providers can also send requests via the EMR for ACCs to encourage a family to schedule follow-up visits. In addition, ACCs attend clinical staff meetings to address difficult cases and other issues. This two-way information flow facilitated the acceptance of ACCs as valued members of the clinical team. The initial barrier to smooth clinical integration of ACCs was their potential for interrupting clinic workflow, but they have learned optimal times to engage the family during clinical visits.
San Juan: Clinic-Based Integration
San Juan’s program is composed of a partnership between a local research institution, local community leaders and agencies, and an FQHC. The ability to integrate ACCs depends on the access and clinical collaboration provided by the FQHC and the practical constraints within a busy general pediatric clinic. The first educational session generally takes place in the clinic immediately following a visit. The ACC works with the family to create an AAP, and the AAP is later entered into a specially created template of the EMR for the PCP to confirm and discuss with the family at the next encounter. By holding the educational session immediately following a clinical encounter, patients and caregivers come to the session engaged on the topic of the patient’s health, and ACCs are able to reinforce or clarify points discussed between the patient and the clinician. When it is not possible to schedule a clinical visit immediately prior to the first educational session, the ACCs work with clinic staff to promote communication among the family, clinician, and ACC. Additionally, ACCs communicate directly with clinicians, including the clinic’s social worker, to address issues that emerge, and the educational session is documented in the patient’s EMR.
Chicago: Community-Based Integration
Like San Juan, the program in Chicago is led by an academic team with a history of community-focused work. Due to the lack of a central health care facility in Englewood, Chicago developed partnerships with multiple providers. The levels of infrastructure and support at each location vary, which requires flexibility of the ACCs with regard to implementation. While recruitment and education sometimes take place in the clinic, most activities are implemented in participants’ homes and over the telephone. As a result of not being fully embedded within the institutions providing care, Chicago’s program has limited ability to exchange information with clinical staff. ACCs encourage clinicians to give completed AAPs to the participants, but success varies by provider. ACCs send the providers written notification of patient participation in the program and completion; this may serve as a prompt for the provider to continue communication regarding management of the child’s asthma.
Discussion
Strengths and challenges for the implementation of care coordination programs are evident in the settings of the four MCAN sites. In addition to attributes inherent in particular settings, a key consideration is the relationship between the LIU and the key access and clinical partners. This relationship, including whether or not the LIU is embedded in the institutions providing access and clinical services, influences the program’s reach and the extent to which ACCs are integrated in a clinical care team.
Each site employed unique strategies to identify eligible participants based on feasibility and acceptability for key access partners. By leveraging the internal sources of information within the Children’s Hospital of Philadelphia, for example, Philadelphia has been able to identify cases through health care utilization data found in EMRs. This approach has the potential to reach eligible individuals who are not using primary care services. Similarly, Los Angeles uses internal records on school absences and nurse visits to identify potential enrollees. Those types of data sources were unavailable to Chicago due to limitations in infrastructure and privacy restrictions. Instead, Chicago relied on direct contact with participants and referrals from clinicians and community organizations. Clinician referrals engage patients who are already actively involved in managing their health; this may facilitate engagement overall, but the physician referral approach may miss those who have barriers to accessing care. In the case of referrals from trusted community organizations or schools, this approach lends credibility in vulnerable communities that have had negative experiences with interventions led with minimal community input or reciprocity (Yancey, Ortega, & Kumanyika, 2006). In San Juan, in addition to recruiting directly from clinic waiting rooms and clinician referrals, other outreach strategies and data sources were used to encourage patients to come to the clinic to be screened. A potential limitation of the recruitment taking place exclusively within a given institution is the restriction of reach to the population served by that institution, whereas recruitment through multiple channels expands reaches to a broader population.
Integration with the care team can be limited for sites that do not offer clinical care directly through the lead implementing institution. For example, although Chicago, Los Angeles, and San Juan have core clinical partners, they are limited by the access, support, and resources those providers are willing and able to grant an external entity. Philadelphia, in contrast, was able to integrate clinical care components to a greater extent. The program’s position within the care-providing institution, including the ACCs’ status as employees of the Children’s Hospital of Philadelphia, facilitated the exchange of information between members of the clinical care team and ACCs. That is not to say that care coordination programs cannot be led by institutions outside of the clinical setting. Indeed, coordination can be greatly enhanced by the strength of the partnerships, the level of integration with partnering clinics, and clinic-provided resources to the care coordination program. For example, in Puerto Rico, the strong partnerships and in-kind support of the program by the FHQC have been essential for the successful implementation of the program and promotion of sustainability. Additionally, the ability to integrate with the care team in an institution is not always a function of institutional policy; often the sense of mission and belief in the initiative from key individuals responsible for the implementation of care coordination components, such as clinicians, limit the level of integration achievable.
A limitation of this study is that the strengths and challenges described are limited to the perspectives of the leaders and program coordinators at each site. While not all of the findings described in this article may be generalizable to other similar settings (as resources, infrastructure, and other contextual factors can vary both across and within settings), this article describes key factors that should be considered when developing or implementing care coordination initiatives. At the time of this analysis, health outcome data were not yet available, and the sustainability of these programs beyond grant funding is yet to be determined. Furthermore, while it would have been beneficial to examine issues such as recruitment efficiency and costs of implementing care coordination in different settings, those data were not available from all of the MCAN sites.
Conclusions
The purpose of this article was to explore the influence setting has on care coordination for childhood asthma and to document the strengths and challenges inherent to each of four settings in which such work is likely to take place (school district, health care system, clinic, and community). While at a high level, care coordination across these settings could be described as somewhat similar, factors such as the ability to use data sources, leverage infrastructure, readily communicate with health care providers, and integrate new components of care into practice played a key role in instituting improvements in coordinated care. The analysis also uncovered the importance of the LIU’s organizational relationships to partners providing access to participants and clinical care. Regardless of setting, successful program implementation requires considerable resources, time, and buy-in from key stakeholders. Future research is needed to examine how setting influences the family’s level of engagement, the effects of different care coordination models have on health and health care utilization, and, importantly, the characteristics of care coordination models that facilitate or impede their sustainability. While these topics are critical in demonstrating to stakeholders the value of implementing and sustaining coordinated care, more translational research and development of standardized evaluation tools are needed to facilitate adoption and evaluation of evidence-based programs in different settings.
Footnotes
Acknowledgements
The authors would like to thank the staff and partners at each of the program sites for their devoted work in delivering these programs as well as the student research assistants who aided in the preparation of this manuscript. Last, but far from least, the authors would like to acknowledge the influence of the late Noreen Clark in the development of this article and, moreover, her significant contributions to the field of public health and chronic disease management. We are grateful for her lasting inspiration and guidance.
This work was supported by funding from the Merck Childhood Asthma Network, Inc.