
Abstract
The endorsement of myths about sexual violence, victims, and perpetrators may harm victims’ well-being. Thus, understanding the factors associated with their endorsement is crucial. To our knowledge, no systematic review or meta-analysis has specifically focused on both child sexual abuse (CSAM) and rape myths (RM). This study aims to address this gap. Following the PRISMA statement, a systematic search across eight databases yielded 4.019 articles, with full-text extraction of 308 articles and the inclusion of 187 articles in the meta-analyses. For CSAM, 22 articles and 75 effect sizes were analyzed from studies conducted between 1992 and 2024. For RM, 167 articles and 763 effect sizes from studies published between 1980 and 2024 were included. Factors were categorized into four categories: Sociodemographic Factors, Beliefs and Attitudes, Individual Functioning, and Socio-contextual Factors. Results revealed that beliefs and attitudes, especially those rooted in sexual aggression and coercion, acceptance of violence, and gendered dominance, had the largest effect sizes, ranging from r = .299 to r = .441. Being male and having a lower educational level were associated with endorsement of both CSAM and RM, albeit with small effect sizes. Individual factors, such as aggressive behaviors and empathy, were moderately associated with RM (r = .251 and r = –.241, respectively). Socio-contextual factors, particularly peer norms supporting sexual violence, were moderately associated with RM (r = .268). Changing maladaptive beliefs and attitudes while fostering empathy is critical for reducing the endorsement of sexual violence myths.
Introduction
Sexual violence is a global and complex public health issue (Bergenfeld et al., 2024). It can have both immediate and long-lasting negative impacts on victims, affecting their mental and physical health, as well as their economic outcomes (Anderson & Overby, 2021; Bergenfeld et al., 2024; Ferragut et al., 2022), and social functioning (Sanjeevi et al., 2018). This negative impact may be heightened by harmful, false, and stereotypical beliefs about sexually abusive experiences, victims, and perpetrators (Balezina & Zakharova, 2024; Bayer et al., 2025; Burt, 1980). Erroneous beliefs about sexual violence and victims, whether they are children or adults, are prevalent and can negatively affect them (e.g., Papalia et al., 2021; Sanjeevi et al., 2018; Walfield, 2021). These beliefs are widely referred to in the literature as child sexual abuse myths (CSAM) and rape myths (RM). They play a critical role in the denial, trivialization, and justification of sexual violence (Balezina & Zakharova, 2024; Cromer & Goldsmith, 2010; O’Connor et al., 2025) and serve to shift responsibility from perpetrators to victims (Anderson & Overby, 2021; Balezina & Zakharova, 2024; Bayer et al., 2025; Crall & Goodfriend, 2016; O’Connor et al., 2025).
Such myths involve blaming the victim and excusing the perpetrator, attributing the responsibility of the abuse to the victims’ actions (e.g., being intoxicated), clothes (e.g., wearing revealing clothing), behaviors during the abuse (e.g., not screaming, fighting back, or even getting injured), and emotional responses, or apparent lack thereof, after the abuse (Cromer & Goldsmith, 2010; Grella et al., 2025). Moreover, beliefs that most allegations are false, motivated by victims’ regret and/or revenge (Grella et al., 2025), or even that the abuse represents a child’s fantasy or fabulation are identified in the literature as myths that minimize the severity and impact of child sexual abuse on victims (Cromer & Goldsmith, 2010).
Additionally, CSAM and RM involve beliefs that reinforce perpetrator stereotypes. A common stereotype is that perpetrators are only male, strangers to the victim, “dirty old men,” mentally ill, from low socioeconomic backgrounds, and gay, which excludes potential perpetrators such as individuals from higher socioeconomic groups, married or young adults (Cromer & Goldsmith, 2010; Grella et al., 2025). In the context of child sexual abuse, myths include the misconception that abused children always have negative feelings toward their perpetrators (Cromer & Goldsmith, 2010). Furthermore, RM incorporate beliefs that women with a sexual history and sex workers cannot be raped, and that sexual violence does not occur within romantic or marital relationships (Anderson & Overby, 2021; Grella et al., 2025). It is important to note that these are heteronormative beliefs, focusing on male-female sexual abuse (Grella et al., 2025). Specifically, myths suggest that women cannot perpetrate sexual abuse, or that men and boys cannot be victims (Cromer & Goldsmith, 2010; Javaid, 2015; Turchik & Edwards, 2012). However, men can also be victims of rape and child sexual abuse, and women can also commit sexual violence (Cromer & Goldsmith, 2010; Javaid, 2015). For instance, regarding child sexual abuse, around one in seven boys and men are victims (UNICEF, 2025), and 10% of these cases are committed by female perpetrators (Gerke et al., 2020).
Sexual violence myths also include stereotypes about the abuse itself, such as that rape/child sexual abuse always involves intercourse using force, the victim’s resistance, and visible physical marks or injuries (Cromer & Goldsmith, 2010; Grella et al., 2025). Moreover, CSAM involves the false belief that abuse is easily detectable and that sexually abused children will immediately disclose the experience (Cromer & Goldsmith, 2010). Both CSAM and RM also encompass beliefs about the severity of abuse, manifested through either minimization or exaggeration. Minimization occurs especially in cases in which the victim’s characteristics do not match heteronormative expectations (e.g., boys/men, gay and bisexual men, and transgender individuals), portraying the idea that these victims are less affected by sexually abusive experiences (Turchik & Edwards, 2012; Urban & Porras Pyland, 2021). Conversely, exaggeration is especially associated with CSAM, including the belief that all sexually abused children inevitably become perpetrators and that they never recover from abusive experiences (Cromer & Goldsmith, 2010).
More recently, research has increasingly examined RM regarding LGBTQIA+ victims (e.g., Chim et al., 2025; Grella et al., 2025; Urban & Porras Pyland, 2021). Evidence suggests that these RM include the belief that rape is inherent to the lifestyle of gay and bisexual men (Grella et al., 2025) and that such individuals deserve to be raped due to being perceived as sexually deviant and immoral (Turchik & Edwards, 2012). Moreover, in the case of lesbian and bisexual women, myths perpetuate the misconception that women cannot rape other women because the abuse does not involve male anatomy (Grella et al., 2025).
These myths are pervasive across multiple contexts (Bronfenbrenner, 1977; Walfield, 2021), including institutions, systems, and agencies (e.g., healthcare and legal contexts) that respond to victims (Anderson & Overby, 2021; Edwards et al., 2011; Koçtürk & Şahin, 2021). Despite their widespread acceptance, there is a lack of integrative systematic evidence on the explanatory factors of myth endorsement, which is critical for informing prevention and intervention practices. Previous systematic reviews and meta-analyses have focused on either CSAM (e.g., Glina et al., 2022) or, predominantly, RM (e.g., Hyży & Mitka, 2024; Suarez & Gadalla, 2010; Yapp & Quayle, 2018), but not on both. Given the lifespan occurrence of sexual violence and the enduring impact of these myths, it is essential to considering victims across the lifespan (Anderson & Overby, 2021; Bayer et al., 2025; Crall & Goodfriend, 2016; Ferragut et al., 2022; Walfield, 2021). Accordingly, this systematic review and meta-analysis aimed to identify factors associated with the endorsement of CSAM and RM and to determine which factors exert the largest effects.
Method
Literature Search Strategy
In November 2024, a systematic search was conducted using eight databases: Academic Search Complete, APA PsycArticles, APA PsycInfo, ERIC, MEDLINE, Psychology and Behavioral Sciences Collection, Scopus, and Web of Science. The search was restricted to peer-reviewed articles published in English, Portuguese, or Spanish in academic journals. No date limitations were set for this search. The search terms included a combination of the following keywords based on the abstracts of the studies: (a) myth* acceptance OR myth* endorsement OR belief* OR attitud* OR misconceptions AND (b) rape OR sexual assault OR sexual abuse OR child sexual abuse OR sexual violence AND (c) factors OR predictors OR determinants OR contributors. This review was not pre-registered.
Inclusion and Exclusion Criteria
The inclusion criteria for studies in this systematic review and meta-analysis were as follows: (a) studies on the associations and predictors of acceptance of CSAM and RM; (b) studies including community, professional, and forensic samples; (c) studies with quantitative or mixed-methods designs; and (d) studies published in English, Portuguese, or Spanish. Studies were excluded if they (a) were editorial, theoretical, systematic reviews, scoping reviews, meta-analyses, or qualitative articles or studies; (b) focused on prevention or intervention programs; (c) explored predictors and prevalence of the perpetration of any form of violence, including sexual violence; (d) focused on risk and protective factors associated with sexual victimization; (e) explored beliefs, myths, and misconceptions about other types of violence, such as physical or psychological violence; (f) focused on factors related to the disclosure of sexual violence in both childhood and adulthood; (g) examined attributions of credibility and blame of victims and/or perpetrators based on vignettes; and (h) did not include information on factors associated with CSAM or RM endorsement.
Study Selection and Data Extraction
The results of this review are based on the PRISMA Statement—Preferred Reporting Items for Systematic Reviews (Page et al., 2021; Figure 1). The search in all databases identified 4.019 articles, and 7 additional records were identified through manual and citation searches. After removing duplicates, 1.852 studies were identified. Titles and abstracts were screened by two independent judges using Rayyan QCRI software (Ouzzani et al., 2016). Similar to previous systematic reviews (e.g., Castro et al., 2024; Magalhães, 2024; Nussbaumer-Streit et al., 2020), one researcher screened all the articles, and 30% were screened by a second independent rater. Following the guidelines of Polanin et al. (2019), an initial abstract screening training session was conducted with the second rater, which included a discussion of the inclusion and exclusion criteria for the screening process. To avoid any contamination or bias, both raters refrained from any discussion until the process was concluded. An inter-judge agreement of 97% was achieved. Disagreements (3%) were resolved through discussion with a third rater until a consensus was reached, as suggested by Polanin et al. (2019). The small error percentage of the partial double screening served as a proxy for the remaining abstracts, therefore being considered a reliable and appropriate screening method. A double screening of all the abstracts would have been employed if a low inter-judge agreement had been observed. Considering this, of the 1.852 studies identified, 13 records were unavailable in full text, and 308 full-text articles were assessed for eligibility. This process resulted in the inclusion of 187 articles in the meta-analyses: 20 on CSAM, 165 on RM, and two on both. The full list and references of the papers included are provided in the Supplemental Material (Table S1).

Results of the search strategy based on PRISMA (Page et al., 2021).
Coding of Studies
Following the guidelines proposed by Lipsey and Wilson (2001), data were extracted and coded based on the main study characteristics, outcomes, and statistical information necessary to calculate the effect sizes. Specifically, the following information was extracted: bibliographical information (authors, title, year of publication); study characteristics (region in which the study was conducted, study design, situational vs. dispositional approaches); sample characteristics (sample size, sample type—community, professional, or forensic participants, and age range); information about the variables (types of myths assessed—CSAM, RM, or both, measures of myth endorsement); main results; and the respective effect sizes. If the original studies did not provide effect sizes, they were calculated using the reported statistical data.
The main findings on factors associated with myth endorsement in each study were organized and coded into four main categories and 36 subcategories (Table 1): (a) Sociodemographic Factors, with 18 subcategories, which pertain to participants’ sociodemographic information (e.g., age, gender, education); (b) Beliefs and Attitudes, including seven subcategories, which focus on participants’ beliefs and attitudes, such as attitudes regarding dominance, gender norms stereotypes, and attitudes regarding sexual orientation; (c) Individual Functioning encompasses six subcategories, addressing aspects related to both personal and interpersonal functioning (e.g., emotional distress, empathy, and openness to others); and (d) Socio-contextual Factors, including five subcategories, which involve factors related to social connections and contextual aspects (e.g., community group affiliations, media influences). The main results, along with the factors and definitions of each main category/subcategory and coding, were initially conducted by one researcher and subsequently discussed with two other researchers, culminating in a final list (Table S2, Supplemental Material).
Main Categories and Included Subcategories of Factors.

Calculation of Effect Sizes
To identify factors related to the endorsement of CSAM and RM, the correlations (r) between study variables (e.g., gender, sexism, social dominance orientation) and the measures assessing myth endorsement were extracted or calculated. Considering that most of the included studies were correlational and that correlations are readily interpreted in terms of their practical significance (Rosenthal & DiMatteo, 2001), Pearson’s product-moment correlation coefficient (r) was chosen as the effect size measure for this review. Moreover, correlations can be easily computed from other statistical measures, such as chi-square, t, F, and d values (Hunter & Schmidt, 2004).
Correlation coefficients were calculated using the methods and formulas proposed by Lipsey and Wilson (2001) and Borenstein et al. (2009). In line with previous studies (e.g., Camilo et al., 2020; Mulder et al., 2018), effect sizes were calculated using bivariate data, as multivariate results do not directly associate two variables. Fisher’s z-scores were calculated before the analysis to transform correlations into normally distributed values (Cooper, 2010; Lipsey & Wilson, 2001). After completing the analyses, these were transformed back into correlations for easier interpretation. Effect sizes of r > .100 were interpreted as small, r > .243 as medium, and r > .371 as large (Rice & Harris, 2005). Most directions (positive or negative) of the effect sizes matched the statistical data reported in the primary studies. However, in specific cases, the directions were adjusted, as required. For instance, this review aimed to provide evidence on which factors are related to the endorsement of (more) myths; therefore, the directions of the effect sizes were adjusted when the measures used in the studies were such that higher scores reflected greater rejection of myths rather than greater endorsement.
Analysis Plan
Primary studies were treated as random samples from larger populations; therefore, a random effects approach was used in this study (e.g., Camilo et al., 2020; Mulder et al., 2018). Multiple factors and variables organized into four main categories and associated with myth endorsement were reported in most of the primary studies included in this review. Considering this and the dependency between effect sizes from the same study, three-level meta-analyses were conducted for each main category and subcategory, when applicable, for both CSAM and RM separately.
Three variance sources were accounted for in the models: variance between studies (Level 3), variance between effect sizes within the same study (Level 2), and sampling variance of effect sizes (Level 1; Assink et al., 2015; Mulder et al., 2018). Meta-analytic models were conducted in the R statistical environment (version 4.4.2, R Core Team, 2025) using the “rma.mv” function from the metafor package (Viechtbauer, 2010), following the syntax described by Assink and Wibbelink (2016). The Knapp-Hartung adjustment (Knapp & Hartung, 2003) was used to test the model coefficients, resulting in the use of the t-distribution to test individual model coefficients and the F-distribution for the omnibus test of all predictors (except for the intercept). Additionally, two one-sided log-likelihood ratio tests were used to assess the significance of Level 2 and Level 3 variance components, while the sampling variance at Level 1 was estimated using Cheung’s (2014) formula.
Results
Descriptives
For the CSAM meta-analysis, 22 articles and 75 effect sizes were analyzed from studies conducted between 1992 and 2024 in Europe (Norway, Poland, Portugal, Sweden, Turkey, and the United Kingdom; n = 12), North America (the USA and Canada; n = 6), Asia (China, Saudi Arabia, and South Korea; n = 3), Africa (South Africa; n = 2), and Oceania (Australia; n = 1). Sample sizes ranged from 89 to 1.606, resulting in a total of 10.118 participants included, comprising community (n = 15), forensic (n = 7), and professional samples (n = 6). To assess myth endorsement, studies used 14 different self-report measures, primarily the Child Sexual Abuse Myth Scale by Collings (1997; n = 4), Childhood Sexual Abuse Myth Scale by Koçtürk and Kızıldağ (2018; n = 3), Child Forensic Attitude Scale by Everson and Sandoval (2011; n = 2), Bumby’s (1996) Molest Scale (n = 2), and Professional Attitudes Regarding Sexual Abuse of Children by Trute et al. (1992; n = 2). The review included 22 studies in the Sociodemographic Factors category, seven in the Beliefs and Attitudes category, and two each in the Individual Functioning and Socio-contextual Factors categories.
A total of 167 articles and 763 effect sizes from studies published between 1980 and 2024 were included in the RM meta-analysis. The studies were conducted in North America (USA and Canada; n = 109), Europe (Denmark, France, Germany, Greece, Hungary, Italy, Norway, Poland, Russia, Spain, Sweden, and the United Kingdom; n = 35), Asia (China, India, Indonesia, Japan, Kuwait, Lebanon, Pakistan, Singapore, South Korea, and Vietnam; n = 16), Latin America (Argentina, Brazil, El Salvador, Guatemala, Mexico, and Peru; n = 12), Africa (Ghana, Nigeria, Somalia, and South Sudan; n = 3), and Oceania (Australia; n = 3). The sample sizes ranged from 27 to 2.756 participants, resulting in a total of 106.358 included in this meta-analysis. The samples consisted primarily of community members (n = 155), followed by professionals (n = 9) and forensic samples (n = 5). Studies used 38 different self-report measures, some of the most commonly used included the Updated Illinois Rape Myth Acceptance Scale (U-IRMA) by McMahon and Farmer (2011; n = 42), the Illinois Rape Myth Acceptance Scale (IRMA) by Payne et al. (1999), both full, short, or adapted versions (n = 39), Burt’s (1980) Rape Myth Acceptance Scale or adapted versions (n = 33), the Rape Supportive Attitude Scale (RSAS; Lottes, 1991) and Rape Callous Attitudes Scale (Lottes, 1998; n = 13), and the Acceptance of Modern Myths about Sexual Aggression (AMMSA) by Gerger et al. (2007; n = 12). The RM review included 120 studies in the Sociodemographic Factors category, 89 in Beliefs and Attitudes, 73 in Individual Functioning, and 32 in Socio-contextual Factors.
Overall Effects on CSAM Endorsement
The overall effects of each main category on CSAM endorsement are presented in Table 2. Among the four main categories, three were found to be significantly associated with CSAM endorsement: Beliefs and Attitudes (r = .371) with a large effect size, Sociodemographic Factors (r = .180), and Individual Functioning (r = −.149), both with small effect sizes.
Results for the Overall Mean Effect Sizes of the Main Categories on CSAM Endorsement.

Note. # Studies = number of studies; ES = number of effect sizes; SE = standard error; CI = confidence interval for Fisher’s z; Sig. mean z = level of significance of mean effect size; Mean r = mean effect size (Pearson’s correlation); % var = percentage of variance; Level 2 variance = variance between effect sizes within studies; Level 3 variance = variance between studies.
p < .05; **p < .01; ***p < .001.
Regarding Beliefs and Attitudes, all subcategories identified in this meta-analysis are significantly associated with CSAM. Large effect sizes were observed in the Sexually Aggressive Attitudes (r = .439) and Attitudes regarding Non-sexual Violence (r = .420) subcategories, while Dominance, Gender Norms, and Stereotypes (r = .299) and Negative Attitudes Regarding Sexuality (r = .335) showed moderate effect sizes. Individuals who believe in group inequality, hold negative sexual attitudes, endorse sexually aggressive attitudes (such as cognitive distortions), and have favorable attitudes regarding non-sexual violence are more likely to endorse CSAM.
In terms of Sociodemographic Factors, education (r = −.275) and professional background (r = −.356) showed moderate-sized significant associations, whereas gender (r = .201) and criminal history (r = .134) had small effect sizes. Being male with a criminal history, having less education, and having a non-social science background were associated with endorsing myths.
For Individual Functioning, although significantly associated with CSAM, the subcategories (i.e., Psychological and Social Well-being, and Empathy and Openness to Others) included only one study with one effect size each. Therefore, their effect sizes could not be calculated. The results for all subcategories are presented in Table S3 in the Supplemental Material. Analysis of funnel plots (Figure S1 in the Supplemental Material) for sociodemographic factors and beliefs and attitudes did not reveal any serious asymmetry issues.
Overall Effects on RM Endorsement
For the RM meta-analysis, the overall effects of all main categories were significantly associated with myth endorsement (Table 3). The category Beliefs and Attitudes (r = .395) presented a large effect size, while Sociodemographic Factors (r = .204), Individual Functioning (r = .219), and Socio-contextual Factors (r = .161) presented small effect sizes.
Results for the Overall Mean Effect Sizes of the Main Categories on RM Endorsement.
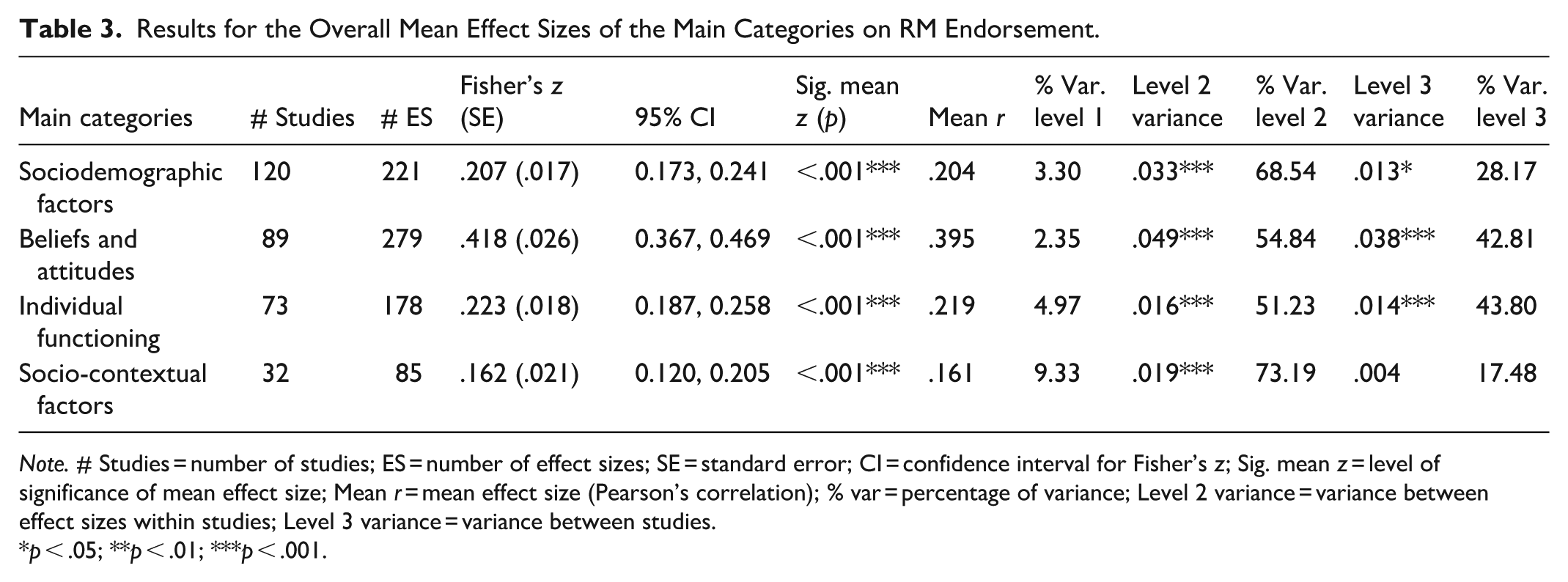
Note. # Studies = number of studies; ES = number of effect sizes; SE = standard error; CI = confidence interval for Fisher’s z; Sig. mean z = level of significance of mean effect size; Mean r = mean effect size (Pearson’s correlation); % var = percentage of variance; Level 2 variance = variance between effect sizes within studies; Level 3 variance = variance between studies.
p < .05; **p < .01; ***p < .001.
In the Beliefs and Attitudes category, large effects emerged in the subcategories of Sexually Aggressive and Coercive Attitudes (r = .375), Attitudes regarding Sexual Orientation (r = .388), Dominance, Gender Norms and Stereotypes (r = .441), and Attitudes regarding Non-sexual Violence (r = .452). Moderate effects were observed for Negative Attitudes and Beliefs regarding Sexuality (r = .295). Therefore, aggressive, unequal, stereotypical, and discriminatory beliefs are associated with the acceptance of RM. Furthermore, only the Religious Beliefs and Spirituality and the Victim Negative Perceptions and Blame subcategories were not significant in this category.
For Sociodemographic Factors, all significant subcategories showed small effects: gender (r = .240), education (r = −.155), previous contact with rape or child sexual abuse (r = −.178), living context (r = .219), and political ideology (r = .235). Race/ethnicity (identifying as White) showed a marginally small but significant effect size (r = −.098). Being male, having a lower level of education, living in a rural context, having a more conservative political ideology, and having less contact with sexual violence (e.g., knowing someone who has experienced sexual violence) were associated with RM endorsement.
Regarding Individual Functioning, moderate effects were observed in the Aggressive and Violent Behavior (r = .247) and Empathy and Openness to Others (r = −.241) subcategories. Small effects were found for the Dark Side of Personality (r = .213), Emotional Distress (r = .143), and Psychological and Social Well-Being (r = −.140), while Substance Abuse and Risky Behaviors showed a marginal but significant effect (r = .077). Individuals with more aggressive and violent behaviors and tendencies, less empathy and openness to others, darker personality traits (e.g., psychopathy, narcissism), higher emotional distress, and lower psychological and social well-being endorsed more RM.
Three of the five subcategories of the Socio-contextual Factors category were significantly associated with RM: Social Norms from Peer Groups (r = .268) with a moderate effect, and Interpersonal Connections (r = −138) and Negative Social Reactions to Sexual Assault Disclosure (r = .215), both with small effects. Individuals with lower-quality relationships, negative reactions to assault disclosure, and integration in peer groups with social norms supportive of sexual violence endorsed more RM. Table S4 in the Supplemental Material presents the results for all subcategories. No serious asymmetry problems were observed in the funnel plots for each main category (Figure S2 in the Supplemental Material).
Heterogeneity
The likelihood ratio tests in both meta-analyses indicated a significant difference in effect sizes within the same study (i.e., Level 2 variance) and across studies (i.e., Level 3 variance) in the Sociodemographic Factors main category (see Tables 2 and 3). For the CSAM meta-analysis, a significant Level 2 variance difference was observed in the Beliefs and Attitudes main category (Table 2). In the RM meta-analysis, significant differences were found in Level 2 variance in the Beliefs and Attitudes, Individual Functioning, and Socio-contextual Factors categories (Table 3). Moreover, significant differences in Level 3 variance were also observed in all main categories, except for the Socio-contextual Factors category in the RM meta-analysis.
Discussion
This study aimed to identify the factors associated with the endorsement of CSAM and RM and to explore which factors revealed the greatest effect sizes. This was achieved by analyzing 838 estimates (75 from CSAM and 763 from RM) from 187 articles, which included a total of 116.476 participants. Most studies included in the current review focused on RM (167 vs. 22 on CSAM) involving a stereotypical view of victims and perpetrators such as young female victims and male perpetrators (Anderson & Overby, 2021; Chim et al., 2025; Walfield, 2021). Unsurprisingly, most studies on RM have been conducted in the USA, where the first scale on these myths was developed (i.e., the Rape Myth Acceptance Scale by Burt [1980]). In some of these studies, aspects related to rape culture are highlighted, particularly in the context of college campuses (e.g., fraternities), which are more common in the U.S. educational system (e.g., Byrne et al., 2021; Lathan et al., 2023) than in Europe. In contrast, most studies on CSAM have been conducted in Europe rather than the USA, which is somewhat unexpected given the pattern observed in RM research. However, this discrepancy may be explained by differences in child protection policies. To date, the USA remains the only country that has not ratified the United Nations Convention on the Rights of the Child (1989). American policies have predominantly focused on post-abuse scenarios, such as requiring certain professionals to report abuse and managing interventions with offenders, which might overlook prevention policies, including providing less funding for research in this area (Helpingstine et al., 2024). By contrast, all European countries have ratified the United Nations Convention on the Rights of the Child (1989), and in 2007, all European Union member states adopted the Council of Europe Convention on the Protection of Children against Sexual Exploitation and Sexual Abuse (Council of Europe, 2007), commonly referred to as the Lanzarote Convention. This convention marked the first regional treaty dedicated to protecting children from sexual abuse (Council of Europe, 2007), requiring states to address this issue through four key areas: prevention, protection, prosecution, and promotion of national and international cooperation (Council of Europe, 2007). Consequently, this divergence in approaches to child sexual abuse may also extend to research, potentially explaining the observed disparity in the number of studies between these contexts.
Regarding sampling, community samples were the most prevalent for both types of myths. Despite significant differences in the number of studies included in each meta-analysis, the distribution of studies involving forensic and professional samples was similar. In the CSAM meta-analysis, forensic samples were the second most prevalent, whereas professional samples occupied that position in the RM analysis, with a particular focus on police officers. While the detrimental impact of the general public’s endorsement of CSAM and RM on victims’ well-being has been documented (Crall & Goodfriend, 2016), the acceptance of these myths by professionals appears to have even more severe consequences. Such beliefs can hinder victims’ disclosure and recovery (Bayer et al., 2025; Magalhães et al., 2022) and compromise the quality of support provided by healthcare and legal systems (Anderson & Overby, 2021; Bayer et al., 2025; Koçtürk & Şahin, 2021; Magalhães et al., 2022; Walfield, 2021).
The results of this meta-analytic review show that factors related to individuals’ beliefs and attitudes had the greatest effect sizes on the endorsement of both CSAM and RM (Table 4). More specifically, these factors included beliefs related to sexual aggression and coercion (e.g., cognitive distortions, adversarial sexual beliefs), dominance (e.g., social dominance orientation, right-wing authoritarianism), gender roles (e.g., sexism), negative attitudes toward sexuality (e.g., sexual double standards, sexual dysfunctional beliefs), and attitudes toward non-sexual violence, such as physical or psychological violence (e.g., cognitions about child neglect, acceptance of interpersonal violence). This evidence suggests that the acceptance of CSAM and RM is rooted in oppressive and aggressive attitudes (Grella et al., 2025), particularly those related to dominance and sexism (Hyży & Mitka, 2024; Nicol & Tóth-Király, 2025). Gender roles encompassing aspects related to how men and women should behave sexually, including sexual double standards, highlight male dominance and negatively shape individuals’ attitudes toward sexuality (Akdemir & Gölge, 2024; Grubb & Turner, 2012; Moyano et al., 2017; Walfield, 2021). Consequently, these roles not only serve to justify sexual violence (Moyano et al., 2017) but also reflect how sexual violence can function as an extension of traditional gender roles (Grubb & Turner, 2012), thereby perpetuating male dominance over women’s submission (Crall & Goodfriend, 2016).
Summary of Critical Findings and Implications for Research, Practice, and Policy.

Large effect sizes for both CSAM and RM endorsement were found for sexually aggressive and coercive attitudes, as well as attitudes regarding non-sexual violence. Cognitive distortions related to sexual violence play a crucial role in its acceptance and justification, as they hinder the recognition of such act as harmful, offensive, or illegitimate (Cromer & Goldsmith, 2010; Mann et al., 2007; Warren et al., 2015). These findings were particularly evident in the CSAM meta-analysis, which primarily included forensic samples. In the case of RM, this subcategory encompassed attitudes toward sexual consent. While positive attitudes toward sexual consent have been identified as protective against RM acceptance, less favorable attitudes may pose as risk factors (O’Connor et al., 2025). Such attitudes can lead to disregard for others’ boundaries, violations of their rights, and misperceptions of behavior (e.g., assuming that a woman consents to sexual activity simply because she agrees to a date; Warren et al., 2015). People’s behavior can be influenced by their attitudes (Orozco Vargas et al., 2022); therefore, less favorable attitudes toward consent are linked to a higher likelihood of engaging in sexual violence (Mann et al., 2007; Nunes et al., 2018).
Additionally, both meta-analyses showed that positive attitudes toward other forms of violence (physical and psychological) were significantly associated with myth endorsement, with a large effect size (e.g., McDermott et al., 2017; Orozco Vargas et al., 2022). The acceptance of these attitudes justifies violence (Orozco Vargas et al., 2022), and sexual violence often co-occurs with other forms of violence and/or maltreatment in childhood (Schuster & Tomaszewska, 2021) and adulthood (Orozco Vargas et al., 2022). Therefore, it is unsurprising that more favorable attitudes toward physical and psychological violence are associated with the acceptance of CSAM and RM, as these myths also serve to justify sexual violence (O’Connor et al., 2025). Being male and having lower education levels, albeit with small effect sizes, were also significantly associated with the acceptance of CSAM and RM. These observed gender differences may also be related to beliefs and attitudes, particularly adherence to traditional gender roles, norms, and stereotypes. These norms benefit men by providing them with a more powerful and dominant social position (Crall & Goodfriend, 2016; Javaid, 2015), making them the higher-status group in the gender hierarchy (Bosak, 2020). Indeed, men seem to support sexist and dominant-oriented beliefs more strongly than women across different countries and cultures (Bosak, 2020; Chim et al., 2025; Nyúl & Kende, 2023). Regarding education, individuals with higher levels of education tended to endorse fewer CSAM and RM. These differences may be explained by processes related to critical thinking skills and awareness of various topics and issues, which are often developed during higher education (Byrne et al., 2021; Van Damme & Zahner, 2022). Furthermore, professionals with higher education typically hold less stereotypical and supportive attitudes toward violence, including sexual violence and related myths (Fávero et al., 2022). Therefore, education and knowledge of related topics may help decrease the acceptance of myths and gender stereotypes (Walfield, 2021).
Significant associations were also found between factors related to one’s Individual Functioning and endorsement of both CSAM and RM. Although there was insufficient data to analyze subcategories regarding CSAM, the results of the RM meta-analysis indicated that aggressive and violent behavior (e.g., physical aggression) and empathy showed the strongest correlations with myth endorsement in this category, although in opposing directions. Specifically, individuals who exhibit sexually abusive behaviors often hold more favorable attitudes toward rape (Bhogal & Corbett, 2016), tend to blame victims, and are more likely to exonerate perpetrators (Hollett et al., 2022). Consequently, while aggressive and violent behaviors are associated with the endorsement of sexual violence myths, these myths can also enable and justify such behaviors (Mouilso & Calhoun, 2013; Yapp & Quayle, 2018). Furthermore, individuals who exhibit aggressive and abusive behaviors tend to have lower levels of empathy. A study by Díaz-Galván et al. (2015), using forensic and community samples, revealed that male inmates displayed lower empathy levels than their community counterparts, particularly in terms of perspective-taking, that is, the ability to understand another person’s viewpoint. In fact, empathy can act as an inhibitor of aggression (Carmona-Cardona et al., 2024), and in the context of sexual violence, empathy, especially toward victims, can function as a protective factor against myth acceptance and victim blame (Koçtürk & Şahin, 2021; O’Connor et al., 2025; Willmott & Widanaralalage, 2024).
The factors in the Socio-contextual category were not significantly associated with CSAM acceptance. However, in the RM meta-analysis, the peer social norms subcategory exhibited a moderate effect. Specifically, peer pressure and acceptance of sexual violence myths are associated with increased likelihood of sexually aggressive behaviors (Cole et al., 2020; Collibee et al., 2021). This association is particularly pronounced in all-male peer settings, such as fraternities and athletic environments, which have been associated with the proliferation of masculine norms and the acceptance of myths (Cole et al., 2020). In turn, RM acceptance, adherence to masculine norms, and peer support for abusive behaviors have been found to indirectly affect sexual violence, mediated by a poorer understanding of sexual consent (Warren et al., 2015). Overall, these findings show that social norms within peer groups that approve violence, including sexual violence, can shape not only the endorsement of RM but also the understanding of sexual consent and the perpetration of sexual violence (Cole et al., 2020; Collibee et al., 2021; Warren et al., 2015). Taken together, these findings highlight both common and divergent factors regarding CSAM and RM acceptance. While individual characteristics, beliefs, and their functioning are linked to the endorsement of both CSAM and RM, factors related to an individual’s social relationships and broader environmental context were found to be significant only for RM. As previously specified, this may reflect the imbalance in the existing literature, with substantially more evidence available on RM than on CSAM, underscoring the need for further research into factors associated specifically with CSAM acceptance. Despite its important contributions, this study has some limitations. Although the systematic search included many databases and keyword combinations, it might not have captured the full scope of the literature on CSAM, considering that all records identified through other sources beyond this search focused on these myths. The effects of heterogeneity were identified and reported in the systematic review. Heterogeneity was observed in both meta-analyses, particularly in Levels 2 and 3. The categorization of factors may explain this second-level heterogeneity. However, conducting analyses by subcategory may have reduced this. Level 3 heterogeneity could be attributed to the diversity of the studies included in terms of socio-cultural contexts (e.g., Norway, Saudi Arabia) and publication periods (from 1980 to 2024; Tong & Guo, 2022). The extensive results and different subcategories presented in the current meta-analysis prevent us from exploring potential moderations, but future research should explore whether geographical and cultural factors might moderate these associations. Social norms and values (e.g., more egalitarian vs. more conservative or oppressive) vary across countries, shaping individuals’ beliefs and attitudes and ultimately impacting CSAM and the acceptance of RM (Fakunmoju et al., 2021). Additionally, even within countries, differences have been observed between rural and urban areas, with individuals in rural settings being more likely to endorse myths (e.g., Hantzi et al., 2015). Therefore, further evidence of these factors is needed.
Notwithstanding these limitations, this review has several strengths. First, and as mentioned, previous systematic reviews and meta-analyses focused on either factors associated with CSAM (e.g., Glina et al., 2022) or RM (e.g., Hyży & Mitka, 2024; Suarez & Gadalla, 2010; Yapp & Quayle, 2018). Therefore, this review represents the first comprehensive effort to examine the endorsement of both CSAM and RM, thereby identifying shared and divergent factors associated with their acceptance and highlighting critical gaps in the literature to inform future studies. This is particularly important considering that sexual victimization, and possible revictimization, can occur across the lifespan, from childhood to adulthood (e.g., Ferragut et al., 2022; Papalia et al., 2021; Walfield, 2021), and sexual violence myths can negatively affect victims throughout their development (e.g., Papalia et al., 2021; Sanjeevi et al., 2018; Walfield, 2021). Furthermore, this systematic search included eight databases and a comprehensive combination of keywords with no date restrictions, which allowed the identification and inclusion of 187 articles published over more than 40 years of research. Moreover, considering papers published in English, Portuguese, or Spanish provided access to a broader scope of literature and publications. Finally, employing a multilevel approach addressed potential issues related to effect size dependency (Assink & Wibbelink, 2016).
The results of this review provide evidence that could inform future research on the factors associated with CSAM and RM endorsement (Table 4). To date, research has mostly focused on sociodemographic variables. However, individuals’ beliefs and attitudes play a crucial role in the acceptance of CSAM and RM. Consequently, future research should explore the variables and factors within this domain and their association with CSAM and RM. Moreover, considering the observed imbalance in the number of studies addressing CSAM compared to RM and the vulnerability of child victims due to their developmental stages (Papalia et al., 2021), further studies on CSAM are necessary. In addition to focusing on CSAM, individual functioning and socio-contextual factors should also be considered. In this review, three-level meta-analyses of the association between these categories and CSAM could not be conducted due to the limited existing literature on these factors. This contrasts with the RM, where significant associations with small to moderate effect sizes were observed. Therefore, further research is necessary to explore and better understand the effects of these variables in the context of CSAM and its endorsement. Finally, most studies used community samples, with a high discrepancy observed between community and professional samples (CSAM: 15 vs. 7; RM: 155 vs. 9). Future research should include more diverse samples, such as professionals, considering the harmful effects of their endorsement of these myths, particularly on the recovery of victims and the quality of support provided (e.g., Anderson & Overby, 2021; Magalhães et al., 2022).
Regarding implications for practice (Table 4), these findings could help inform prevention and intervention programs. These programs may enhance their efficacy by targeting maladaptive beliefs rather than individual characteristics (e.g., gender; Angelone et al., 2021; Murphy & Hine, 2019). Previous research suggests that focusing solely on sociodemographic aspects (e.g., gender) or on changing sexually violent supportive attitudes might not be sufficient; instead, interventions should address the core beliefs sustaining these attitudes (Angelone et al., 2021). Targeting these beliefs is particularly relevant because changes at the cognitive level may also influence behavior and norms across familial, social, and cultural contexts (Koçtürk & Şahin, 2021; Sivarajasingam et al., 2022). Emotional elements should be considered when designing and implementing prevention and intervention programs. According to the elaboration likelihood model, emotions can influence individuals’ judgments, especially when they are not motivated or able to think and elaborate on the subject at hand, and can also create thought bias about the topic in higher-order thinking situations (Petty & Briñol, 2015). Therefore, to enhance persuasion in changing attitudes and beliefs, it might be important to match the emotional content of arguments to the experienced emotion (Petty & Briñol, 2015). Moreover, evidence suggests that emotional regulation—such as cognitive reappraisal, in which participants are asked to think analytically about the content—seems to also be important for reducing negative attitudes (Albarracin & Shavitt, 2018). This might be particularly relevant to consider, as some audience members might be more motivated to participate in and think about the topic than others (e.g., community members vs. perpetrators), for different reasons (e.g., being optional vs. mandatory; McNeish et al., 2022; Mora-Pelegrín et al., 2025). Moreover, prevention and intervention efforts should be implemented in various contexts, such as schools and academic settings, through sexual education curricula and psychoeducation (Cole et al., 2020; Collibee et al., 2021; Ferragut et al., 2022; Warren et al., 2015). Psychoeducation is crucial for understanding and preventing sexual violence (Ferragut et al., 2022) and is particularly important for professionals (Koçtürk & Şahin, 2021). The attitudes of professionals, including police officers, are closely linked to the perpetuation of myths in these institutional settings (Murphy & Hine, 2019), often due to insufficient training, which can result in underestimating the severity of sexual violence and impede reporting, especially in cases of child sexual abuse (Al-Saif et al., 2018). Accordingly, training and supervision are essential to preventing secondary victimization arising from potentially maladaptive beliefs. Finally, empathy, as the capacity to understand others’ perspectives, might be a protective factor against the endorsement of myths (Koçtürk & Şahin, 2021; O’Connor et al., 2025), which requires further intervention efforts to foster this skill in both community and professional contexts.
Supplemental Material
sj-docx-1-tva-10.1177_15248380261443213 – Supplemental material for A Systematic Review and Meta-Analysis on Factors Related to Child Sexual Abuse and Rape Myths
Supplemental material, sj-docx-1-tva-10.1177_15248380261443213 for A Systematic Review and Meta-Analysis on Factors Related to Child Sexual Abuse and Rape Myths by Inês Chim, Cláudia Camilo, Nélio Brazão and Eunice Magalhães in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
We would like to thank Catarina Palma for her support in the co-screening process of this systematic review.
Funding
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.