
Abstract
This scoping review examined risk and protective factors that influence the relationship between disclosure of child sexual abuse and suicidal thoughts or behaviours. While child sexual abuse is a well-established risk factor for suicidality, disclosure experiences and suicide risk remain underexplored. Guided by Arksey and O’Malley’s method of scoping, a systematic search of Medline, CINAHL, PsycINFO, and Scopus was conducted for English-language studies published between 2015 and 2025. Grey literature relevant to the Australian context was also reviewed. Ten studies met inclusion criteria, involving qualitative, quantitative, and mixed methods designs. Results, informed by betrayal trauma theory and the interpersonal theory of suicide, suggest that the relational and systemic context surrounding disclosure, rather than disclosure experience itself, contributes to suicide risk. Supportive responses mitigated distress, while negative reactions and unsupportive system responses heightened suicidal ideation and behaviours. Quantitative studies were mixed: while disclosure opportunities appeared protective, their benefits depended on response quality and ongoing support. Mandatory reporting processes, though protective in intent, were sometimes experienced as intrusive or disempowering, adding to distress. Safe disclosure is contingent upon trauma-informed, relationally-attuned systems of care. Integration of suicide prevention and child sexual abuse response frameworks is needed to ensure victims and survivors receive sustained, validating support across family, community, and practice contexts.
Introduction
Child sexual abuse refers to sexual acts involving physical contact and/or non-contact sexual behaviours in which a child under the age of 18 lacks the capacity to provide informed consent (Mathews & Collin-Vézina, 2019). Research has consistently demonstrated that child sexual abuse is a significant risk factor for a wide range of psychopathological outcomes such as suicide or self-harm (Hashim et al., 2025). Child sexual abuse victims and survivors face an elevated risk of suicide attempts even when other variables are accounted for (Evans et al., 2017; Hailes et al., 2019). There is considerable variation across studies in the reported severity and timing of sexual abuse, and the mechanisms or developmental pathways underlying the emergence of suicidal behaviours remain insufficiently understood (Angelakis et al., 2020). Similarly, prevalence of self-harming behaviours, regardless of suicidal intent, has a notable correlation with child sexual abuse (Liu et al., 2018).
Disclosure of child sexual abuse is not a one-off event but a dynamic process that may take place over time, with different people, and can be revisited across the lifespan. This process can represent a turning point that shapes mental health and well-being trajectories (Alaggia et al., 2019; Russell et al., 2021). Supportive responses to disclosure may buffer against suicidal thoughts or behaviours, while negative or delayed responses may intensify distress and compound risk (Canosa et al., 2025; Hindman et al., under review; McPherson, Gatwiri, Canosa, et al., 2025). Despite growing recognition of the relational nature of disclosure, there is limited understanding of which risk and protective factors moderate or mediate the relationship between disclosure of child sexual abuse and suicidal ideation, behaviours, or self-harm.
Research has shown that people who experienced child sexual abuse have higher rates of suicidal ideation and suicide attempts compared to people who were not sexually abused (Devries et al., 2014). Disclosure is not a simple protective or harmful factor in itself; rather the response to disclosure is critical. Belief, validation, and support are generally protective, whereas negative responses like disbelief and blame can increase distress and suicidal risk (McPherson, Gatwiri, Graham, et al., 2025). Several qualitative and quantitative studies emphasise that the disclosure experience partly explains variation in mental health outcomes after child sexual abuse (Alaggia, 2010; Alaggia et al., 2019; Hindman et al., under review). Some population studies have even found that disclosure to certain systems (statutory services) was associated with higher reported lifetime suicidal ideation (Baiden et al., 2017). This finding likely reflects complex pathways, such as legal or process-related stressors, or unsupportive system responses, rather than suggesting that disclosure per se causes suicidality (Baiden et al., 2017). This evidence highlights the need for trauma-informed and supportive responses when abuse is reported (McPherson, Gatwiri, Canosa, et al., 2025). Factors that link child sexual abuse and suicidality include post-traumatic stress disorder, depression, hopelessness, shame, social isolation, substance use, and stigma (Wang et al., 2025). The disclosure process influences many of these mediators and considering the socio-ecological context is important (Latiff et al., 2024). Where responses to disclosure are experienced as supportive, isolation can be reduced and access to therapy increased, whereas hostile or dismissive reactions can heighten shame and hopelessness (Spokas et al., 2009).
This scoping review is informed by two complementary theoretical frameworks that demonstrate the relational and psychological dimensions of child sexual abuse and suicidality. Betrayal trauma theory (Freyd, 2003) explains how child sexual abuse perpetrated within relationships of trust can disrupt attachment, identity, and self-concept, with lasting impacts on personal functioning and self-worth. Interpersonal theory of suicide (Chu et al., 2017; Joiner & Van Orden, 2008; Van Orden, 2014) proposes that suicidal desire arises from social disconnection perceived burdensomeness. Taken together, these frameworks suggest that child sexual abuse-related disruptions in attachment and identify may heighten vulnerability to social disconnection and feelings of being a burden, thereby increasing suicide risk. Within this pathway, disclosure represents a pivotal relational moment: supportive responses may restore connection and reduce risk, whereas disbelief or blame may reinforce betrayal and deepen suicidality. This integrated lens informed the framing of the review.
Despite growing recognition of the relational nature of disclosure, there remains limited understanding on how specific factors may influence the relationship between child sexual abuse disclosure and suicide-related outcomes or self-harm. This scoping review addresses this gap by mapping existing literature to identify protective and risk factors, thereby building the evidence base for the development of trauma-informed, relationally-attuned responses to disclosure.
This work is undertaken in partnership with practitioner experts from the Centre Against Violence in Northeast Victoria, Australia who witness firsthand when disclosures are met with rejection or disbelief and its contribution to suicidal ideation and behaviours. Additionally, practitioners observe how the disempowering nature of mandatory reporting processes may further contribute to psychological distress for some victims and survivors. Developing this work in close partnership with practitioners ensures that the findings are grounded in real-world practice and informed by the lived realities of those working directly with victims and survivors. While the grey literature component was limited to Australia, this context has distinct features, including mandatory reporting frameworks and nationally significant inquiries into institutional responses to child sexual abuse, which shape disclosure processes and service responses. These structural and policy settings may limit direct generalisability to other jurisdictions. However, the relational dynamics identified in this review are likely relevant across contexts where disclosure occurs within interpersonal and systemic environments.
Methods
This paper developed from an Australian-based mixed-methods study that explored helpful and unhelpful practices and responses to disclosures of child sexual abuse, with the aim of improving service systems to facilitate safe and supportive interventions (Canosa et al., 2025; Hindman et al., under review; McPherson, Gatwiri, Canosa, et al., 2025; McPherson, Gatwiri, Graham, et al., 2025). A finding of this overarching study was that the high prevalence of suicidality reported among participants was closely linked to how their child sexual abuse disclosures were received, highlighting the enduring impact of disclosure responses on survivors’ psychological distress and overall well-being. Therefore, a scoping review, including grey literature relevant to the Australian context, was deemed relevant to examine the existing evidence and identify factors that influence safe responses to disclosure. This review was conducted using the Arksey and O’Malley (2005) and Davis et al. (2009) guidelines. The steps in the process involved (a) defining the research question, (b) identifying relevant studies, (c) selecting studies, (d) charting the data, and (e) collating, summarising, and reporting the results.
Step 1: Defining the Research Question
The question guiding this review was: What risk and protective factors influence the relationship between disclosure of child sexual abuse and suicidal thoughts, behaviours, or self-harm?
Step 2: Identifying Relevant Studies
The included studies (a) focused on disclosure of child sexual abuse, (b) had suicidal ideation, suicide attempts, self-harm, or death by suicide as outcomes, (c) used any study design, and (d) were published in English. Conference presentations, reviews, book chapters, theses, and studies focusing on only veterans were excluded. Publication timeframe was set from 2015 to August 2025. This 10-year timeframe was selected to ensure the review captured contemporary evidence, reflecting significant policy reforms, evolving language around stigma and disclosure, and recent advances in suicide prevention and trauma-informed practice (Procter et al., 2023; Tunno et al., 2021). The search strategy was formulated with the assistance of a research librarian. Four electronic peer-reviewed databases (Medline, CINAHL, PsycINFO, and Scopus) were searched using a combination of carefully selected keywords (Table 1).
Search Strategy.
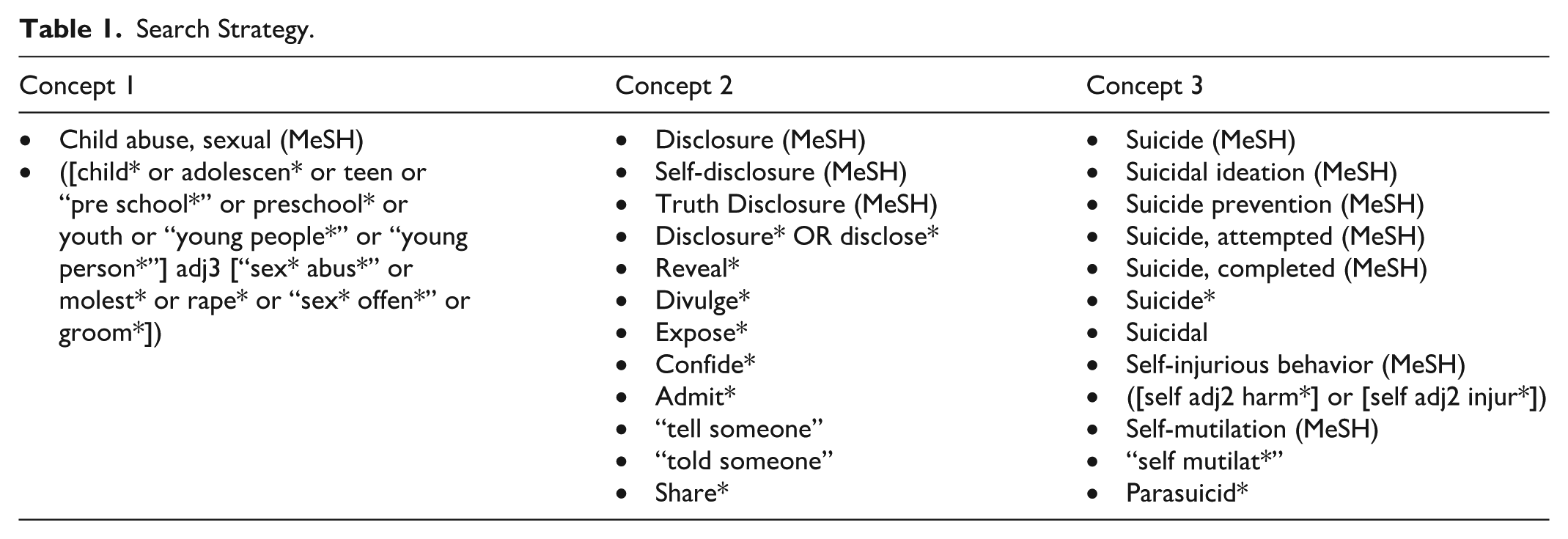
The grey literature search encompassed two databases (Google and Overton) using the string of key terms “‘child sexual abuse’ AND disclos* AND suicid* OR self-harm.” The first 50 results from either database were screened. In addition to the abovementioned inclusion criteria, the grey literature searches were further limited to PDF documents published in Australia. Duplicate or invalid results were removed, and the remaining documents were screened for inclusion. Child protection policies and manuals available on the Australian state governments’ websites were also reviewed.
Step 3: Selecting Studies
Covidence™ was used to screen peer-reviewed studies. Two researchers screened 431 studies for relevance based on the information provided in the title and abstract. Records that did not match the inclusion criteria were excluded (n = 287), and any citations that were not agreed upon were reviewed by a third researcher for a final decision. Full articles (n = 62) were retrieved for citations that had been approved. Two researchers examined these articles to decide if the citations conformed to the inclusion criteria. The third researcher resolved any disagreement, resulting in nine studies being included. Grey literature screening was performed by one researcher. Out of 114 search results, one document met the inclusion criteria. The remaining documents were excluded due to the lack of primary data, or lack of focus on disclosure and suicidal outcomes. In total, 10 documents were included (Figure 1).
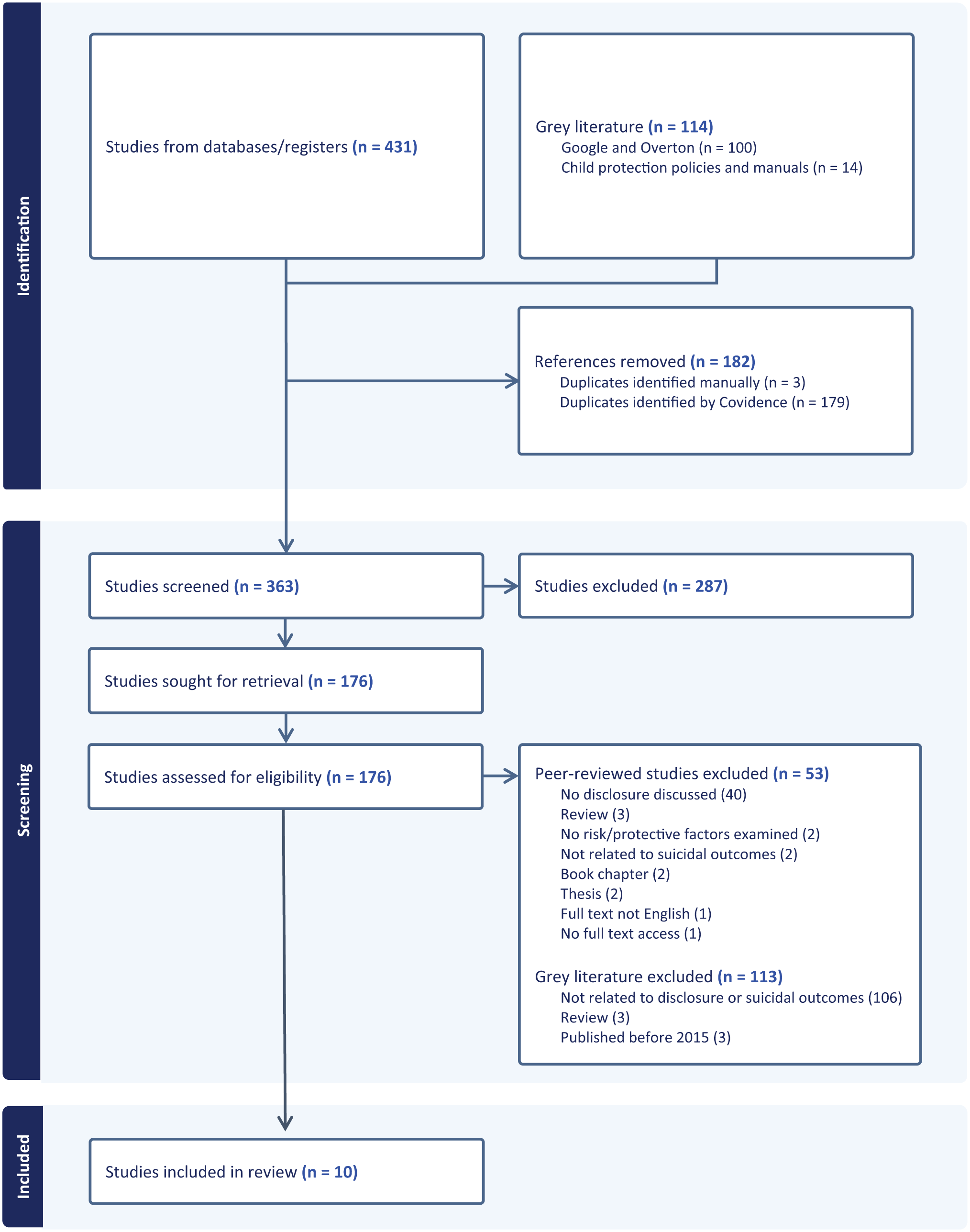
PRISMA flowchart.
Step 4: Charting the Data
An extraction template was developed by the study team. Extraction was performed by one researcher and checked by another. Quality assessment of included studies was performed by two researchers. Since the studies involved qualitative and quantitative methodologies, the Quality Assessment with Diverse Studies (QuADS) tool was used (Harrison et al., 2021). Scoping reviews do not require formal quality appraisal; however, to support transparency and contextualise the evidence base, a light-touch quality assurance process was incorporated. This appraisal was not used to exclude studies but to provide insight to the strength and limitation to the available evidence. Overall, the research was conducted and reported to a medium to high standard according to the QuADS tool. A small portion of studies critically discussed the limitations related to the research they reported on. Notably, only one study involved stakeholder input in its research design and conduct. While all studies reported on suicidality in the context of child sexual abuse, only a subset specifically examined the relationship between disclosure and suicidal or self-harm behaviours. This distinction has been reflected in Table 2, where all results relating to disclosure and suicidality are included, regardless of the level of detail reported.
Overview of Included Studies.
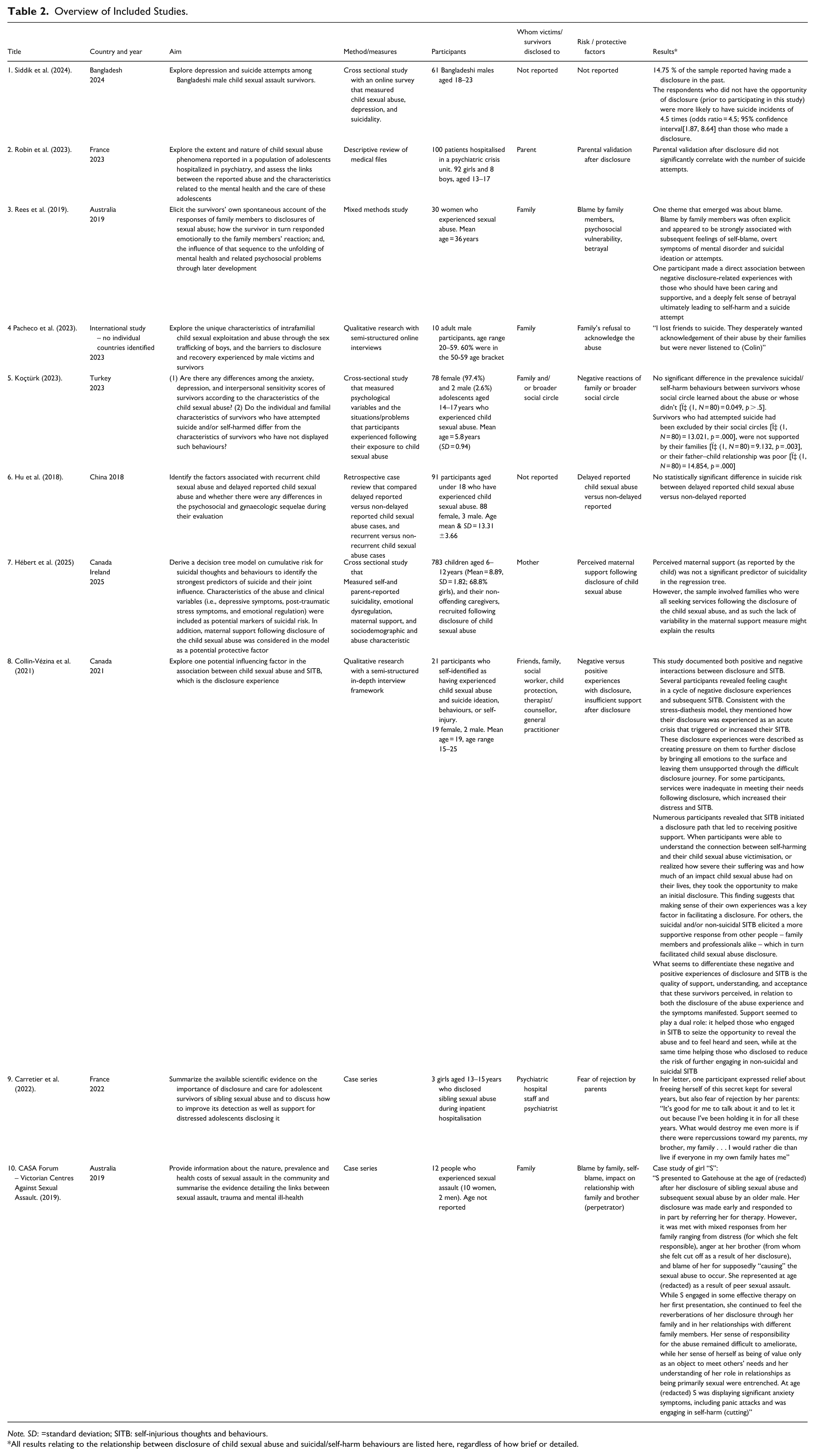
Note. SD: =standard deviation; SITB: self-injurious thoughts and behaviours.
All results relating to the relationship between disclosure of child sexual abuse and suicidal/self-harm behaviours are listed here, regardless of how brief or detailed.
Step 5: Collating, Summarising, and Reporting the Results
The data from the included literature were collated based on the Preferred Reporting Items for Systematic reviews and Meta-Analyses – Scoping Reviews (PRISMA-ScR)guidelines for reporting results (Tricco et al., 2018). The researchers and practitioners conducted reflexive consultations both collectively and independently to enhance the overall research process. This critical process involved three authors screening, charting, and collating data. By incorporating this reflexive consultative approach, these authors ensured continuous reflection was undertaken on search strategies and methodological choices. This method was not linear but iterative within each stage of the scoping review. We begin our reporting of the results by study design, location, sample size, and participants. A narrative synthesis of the included articles was conducted using a thematic approach, and patterns were reviewed and revised by the researchers (Braun & Clarke, 2014). Study aims of included studies generally focused on (a) the relationship between child sexual abuse disclosure and suicidal or self-injurious thoughts and behaviours, (b) psychosocial correlates of suicidal behaviours following child sexual abuse, and (c) barriers and facilitators to disclosure and recovery.
Results
Study design: Included studies represented diverse designs including qualitative interview studies (Collin-Vézina et al., 2021; Pacheco et al., 2023), mixed-methods research (Rees et al., 2019), cross-sectional surveys (Herbert & Bromfield, 2021; Koçtürk, 2023; Siddik et al., 2024), retrospective case reviews ((Hu et al., 2018), descriptive file reviews (Robin et al., 2023), and case study series (Carretier et al., 2022; CASA Forum, 2019).
Location: Studies were conducted across multiple locations including Canada and Ireland (Collin-Vézina et al., 2021), Canada (Hébert et al., 2025), Australia (CASA Forum, 2019; Rees et al., 2019), France (Carretier et al., 2022; Robin et al., 2023), Bangladesh (Siddik et al., 2024), China (Hu et al., 2018), Turkey (Koçtürk, 2023), and one international study (Pacheco et al., 2023).
Sample size and participants: Sample sizes ranged from small qualitative samples of three people (Carretier et al., 2022) to large clinical cohorts of 783 participants in a cross-sectional study (Hébert et al., 2025). Participant groups varied across studies and involved children (Hébert et al., 2025), adolescents (Carretier et al., 2022; Hu et al., 2018; Koçtürk, 2023; Robin et al., 2023), combination of adolescents and adults (Collin-Vézina et al., 2021), and adults reflecting retrospectively on child sexual abuse (CASA Forum, 2019; Pacheco et al., 2023; Rees et al., 2019; Siddik et al., 2024). Two studies focused exclusively on males (Pacheco et al., 2023; Siddik et al., 2024), and two on females (Carretier et al., 2022; Rees et al., 2019). The rest had mixed gender samples, with a higher proportion of women in all of them. No study reported having gender-diverse participants.
Whom Victims and Survivors Disclosed To
Across studies, parental or familial disclosure were most commonly reported, though several studies also documented disclosures to practitioners, including therapists, psychiatric staff, or child protection workers (Collin-Vézina et al., 2021; Hébert et al., 2025; Koçtürk, 2023; Robin et al., 2023). Suicidal or self-harming behaviours sometimes preceded disclosure, suggesting a reciprocal rather than linear pathway (Collin-Vézina et al., 2021). Several clinical and qualitative studies explicitly recorded disclosure to mothers or parents (Hébert et al., 2025; Robin et al., 2023), while others described disclosures to psychiatric staff during inpatient care (Carretier et al., 2022). In broader community and adult retrospective samples, disclosure was made to family members and friends (CASA Forum, 2019; Collin-Vézina et al., 2021; Rees et al., 2019). One study described that male survivors who attempted disclose to their families were met with a refusal to acknowledge the abuse (Pacheco et al., 2023).
Impact of Disclosure Responses on Suicidality
A consistent theme is that the quality of the response following disclosure, whether characterised by validation and support or by blame and disbelief, profoundly shaped survivors’ subsequent psychological distress and risk of suicidal or self-injurious thoughts and behaviours (CASA Forum, 2019; Collin-Vézina et al., 2021; Koçtürk, 2023; Pacheco et al., 2023; Rees et al., 2019). Supportive and validating responses were described as reducing isolation and aiding help-seeking (Collin-Vézina et al., 2021), whereas negative family reactions, including explicit blame (CASA Forum, 2019; Rees et al., 2019), refusal to acknowledge the abuse (Pacheco et al., 2023), or exclusion by the family or social circle (Koçtürk, 2023), were associated with elevated self-blame, deterioration in mental health, and suicidal ideation or attempts. Cultural and gender norms shaped both disclosure likelihood and stigma, particularly among male survivors (Pacheco et al., 2023; Siddik et al., 2024). Participants in several qualitative studies explicitly linked experiences of family blame or non-acknowledgement with later self-harm or suicide attempts (Pacheco et al., 2023; Rees et al., 2019). System-level responses were inconsistently protective, with disclosures to practitioners not always reducing risk (Collin-Vézina et al., 2021; Hu et al., 2018).
Quantitative Associations Between Disclosure and Suicidal Outcomes
Several quantitative studies examined the association between disclosure and suicidal outcomes, presenting mixed results. Respondents who lacked an opportunity to disclose were 4.5 times more likely to report suicide attempts than those who had disclosed (Siddik et al., 2024). Conversely, another study found no significant difference in the prevalence of suicidal behaviours between adolescent survivors whose social circle learned about the abuse and whose did not (Koçtürk, 2023). There was no difference in suicide risk between people who delayed their disclosure and those who did not (Hu et al., 2018).
There was also mixed evidence regarding the impact of family reactions to disclosure and subsequent suicidality. Two studies reported that parental validation (Robin et al., 2023) and maternal support (Hébert et al., 2025) were not significantly associated with suicidal thoughts or attempts. Conversely, another study demonstrated a link between suicide attempts and being excluded by one’s social circle, not being supported by family, or having a poor father–child relationship (Koçtürk, 2023). Overall, these findings suggest that the presence or timing of disclosure is not consistently associated with suicidal outcomes. However, where this association is present, non-disclosure or negative consequences following disclosure may lead to increased suicide risk.
Support as a Protective Factor
High-quality support from caregivers, peers, and practitioners played a protective role, reducing suicidality or facilitating recovery (Collin-Vézina et al., 2021; Hébert et al., 2025; Rees et al., 2019). However, there was also a substantial variation in the accessibility and consistency of that support. A large clinical cohort recruiting families after disclosure found limited variance in maternal-support measures (Hébert et al., 2025). Since mother–child duos in this study were actively seeking support services, this likely means that maternal support was already high. In qualitative studies, when disclosure triggered appropriate responses – characterised by understanding and referral to services – participants experienced relief and reductions in suicidal thoughts or behaviours (Collin-Vézina et al., 2021; Rees et al., 2019). Inadequate practitioner responses or service gaps increased distress and perpetuated suicidal ideation (Collin-Vézina et al., 2021).
Influence of Family Dynamics on Post-Disclosure Well-Being
Several studies highlighted family dynamics, particularly poor father–child relationships, family exclusion, or parental non-support, as noticeable correlates of suicidal behaviours (CASA Forum, 2019; Koçtürk, 2023; Pacheco et al., 2023; Rees et al., 2019). Quantitative analysis in an adolescent sample showed that family exclusion, lack of support, and negative paternal relationships were strongly associated with suicide attempts (Koçtürk, 2023). Qualitative accounts similarly emphasised the profound harm caused when families responded to disclosure with rejection or denial (CASA Forum, 2019; Pacheco et al., 2023; Rees et al., 2019), demonstrating the role of family relationships in shaping the trajectory of post-disclosure well-being.
Discussion
This scoping review explored the risk and protective factors influencing the relationship between disclosure of child sexual abuse and suicidal thoughts and/or behaviours. Within the small body of included studies, disclosure emerged as a critical relational moment: a potential for connection and validation or renewed betrayal and isolation. The results suggested that the interpersonal and systemic context surrounding disclosure, rather than disclosure itself, is central to understanding victims’ and survivors’ lived experiences. In this context, unsupportive disclosure responses can be understood as a form of secondary betrayal that heightens the original relational harm (Freyd, 2003), while social exclusion and blame reflect the disconnected belongingness and perceived (Van Orden, 2014).
Across studies, unsupportive disclosure responses, social exclusion, and family dysfunction were repeatedly associated with heightened suicidal ideation and behaviour. Negative family responses, lack of acknowledgement, blame, and absence of opportunities for disclosure each increased the risk of suicide attempts. One study suggested that the disclosure opportunity itself can be protective; those who never disclosed were at a substantially higher suicide risk (Siddik et al., 2024). However, other factors that may have contributed to these participants’ suicidality, or their reasons for not disclosing the abuse, were not examined in this study. Regardless, the protective effect of making a disclosure was conditional on receiving validating support (Hébert et al., 2025). From a betrayal trauma perspective, such responses may reinforce children’s expectations that attachment figures are unsafe or unavailable. Simultaneously, experiences of blame or silencing may intensify feelings of isolation and burdensomeness, thereby strengthening suicidal desire.
The results also extend the current understanding of the link between disclosure of child sexual abuse and suicidality by identifying bidirectional processes: self-harming or suicidal behaviour sometimes preceded disclosure and acted as a precipitating factor for help-seeking (Collin-Vézina et al., 2021). This may suggest that disclosure and suicidality exist in a reciprocal cycle, rather than a simple linear sequence. Furthermore, cultural and gender norms shaped disclosure patterns and stigma, with male participants describing particularly profound silencing and family denial. These results emphasise that social scripts of masculinity and honour influence not only disclosure likelihood but also survivors’ capacity to seek and receive support. This bidirectional pattern also aligns with interpersonal theory, whereby escalating distress and perceived disconnection may precipitate suicidal behaviour prior to disclosure, positioning self-harm as an expression of unmet relational needs rather than solely an outcome of disclosure failure.
Protective factors centred on the quality and authenticity of support. Victims and survivors who encountered compassionate and sustained responses experienced reduced distress and suicidality (Collin-Vézina et al., 2021; Rees et al., 2019). Findings from these two studies reinforce the notion that the quality of support, rather than its mere presence, are what mitigate risk. Interestingly, in Hébert et al.’s (2025) large clinical cohort, maternal support did not predict suicidal outcomes, likely due to limited variability in the already service-engaged sample. Peer and community responses also played an underacknowledged role. Koçtürk (2023) found that social exclusion from peers independently increased suicide risk, even when family support was present. Collectively, these studies show that relational safety that includes family, peer, and professional systems, is important in protecting against suicidality. Where systems failed to respond appropriately, victims and survivors experienced renewed feelings of isolation and despair (CASA Forum, 2019; Rees et al., 2019). Supportive and sustained responses may interrupt this trajectory by restoring relational safety and belonging, thereby counteracting both the attachment disruptions and the interpersonal risk states associated with suicidality.
These results carry implications for prevention and intervention. Although this review involves Australian grey literature, the included studies are geographically diverse and thus, the findings are applicable worldwide. Well established in the literature, disclosure should be conceptualised as a process, not a one-off event (Alaggia et al., 2019; McPherson, Gatwiri, Graham, et al., 2025). Support must be sustained over time and embedded in trauma-informed systems that can respond flexibly to victims’ and survivors’ evolving needs across the lifespan. Family-based interventions that promote acknowledgement and open communication may help repair relations and reduce suicide risk. Finally, from a policy perspective, service frameworks should integrate suicide prevention and disclosure of child sexual abuse response systems, recognising the overlap between disclosure distress and suicidality. Interventions should therefore prioritise strengthening belongingness, countering perceived burdensomeness, and avoiding institutional forms of betrayal that may inadvertently replicate earlier relational harms.
There are limited studies from diverse cultural contexts. Given that attitudes towards suicide vary across cultures, it is possible that the factors affecting the relationship between abuse disclosure and suicide-related outcomes will vary accordingly. Similarly, the underrepresentation of male and gender-diverse victims and survivors narrows the scope of perspectives that are reflected in this evidence base. In line with this, professional responses require strengthening, particularly through training in trauma-informed and culturally responsive practice. Socio-cultural factors influence child sexual abuse disclosure, so examining how aspects such as acculturation and minority identity shape disclosure in multicultural settings with racially and culturally minoritised communities would be valuable (Latiff et al., 2024).
Overall, the literature that provides detailed examinations of disclosure of child sexual abuse and subsequent suicidality is scarce. In a significant portion of the included studies, suicidality was measured as a single-item variable or described in vague terms. The stigma around suicide is prominent across research and practice, which may explain the lack of focus and detail. This review highlights the gap in current understanding relating to how individuals and services can respond to disclosure in a way that promotes victims’ and survivors’ well-being and reduces suicide risk.
Strengths and Limitations
This review has several strengths. It is the first to investigate both risk and protective factors related to disclosure of child sexual abuse and suicidality. We searched not only peer reviewed sources but also Australian grey literature, which allowed us to capture relevant research that would have otherwise been missed. Furthermore, practitioner experts who work directly with victims and survivors were involved in this study, enhancing the interpretation of findings through the lived experience perspective. However, there are several limitations. Firstly, the evidence base featured methodological heterogeneity and predominantly retrospective and cross-sectional designs, which limits the ability to draw conclusions and generalise across contexts. Future research should examine multi-level factors (individual, relational, and systemic) through mixed-method or longitudinal designs. Secondly, the included studies provided little information on how disclosure was defined or performed. These varying operational definitions of “disclosure” may have contributed to the discrepancies in findings. Future work should ensure that disclosure, and responses to disclosure, as study variables are well defined and operationalised. Thirdly, the relationship between child sexual abuse, suicidality, and associated factors is complex and likely not linear. For example, negative family relationships may predate (or be a contributing factor to) the abuse in the first place, increasing suicidal outcomes regardless of whether or how any disclosure took place.
Conclusion
This scoping review highlights the risk and protective factors between child sexual abuse disclosure and suicidality, emphasising that it is not disclosure alone, but the responses surrounding it, that shape victims and survivors’ lived experiences. Across diverse contexts, the relationship between disclosure of child sexual abuse and suicidality is profoundly shaped by how others respond. Supportive and contextually attuned responses across family, peer, professional, and policy domains, are critical in mitigating suicidal distress. By mapping existing evidence and identifying protective and risk factors, this review lays the groundwork for relational and trauma-informed approaches to suicide prevention and disclosure support.
Footnotes
Acknowledgements
We thank Ms Johnson, research librarian at La Trobe University Bendigo, for her support in developing and undertaking the search strategy.
Ethical Considerations
Ethical approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.