
Abstract
Care-experienced children and young people (CYP), for example, those who have been under state care through foster, kinship, or residential placements, or adopted from care, experience disproportionately high levels of mental health difficulties. Yet little is known about the forms of social support that may protect or promote their mental health and well-being (MHW). This scoping review mapped the international evidence on the types, sources, and quality of MHW-related social support for this population. Seven bibliographic databases were systematically searched for English-language, peer-reviewed studies published from 2008 onward in high-income countries. Eligible studies included quantitative, qualitative, mixed-methods, and intervention designs that examined social support for care-experienced CYP aged ≤25. Study selection followed scoping-review methodology and PRISMA-ScR guidelines. Data were summarised using descriptive numerical mapping and qualitative thematic synthesis. Young people with lived experience contributed to interpretation and identification of priorities. A total of 246 study reports met the inclusion criteria, representing research from 13 countries, most commonly the United States (60%) and United Kingdom (13%). Emotional support was the most frequently examined type, followed by tangible, esteem, and informational support. Foster carers, birth families, peers, and professionals were the most common sources. High-quality support characterised by trust, empathy, and stability was consistently associated with better MHW, though many relationships were shaped by complexity. Evidence was limited regarding special guardianship and romantic partners. Findings highlight the need for holistic, relationship-centred approaches to promote the MHW of care-experienced young people.
Introduction
Improving the mental health of children and young people (CYP) is a public health priority, due to its association with distress, impairment and poor long-term outcomes (Anthony et al., 2024). There has been a marked rise in the prevalence of emotional problems among adolescents (Armitage et al., 2023; Collishaw, 2015). Children with a mental health disorder in 2017 experienced more severe difficulties and greater impact on functioning at school, home and in their daily lives, compared to children in earlier decades (Armitage et al., 2025). Certain groups of CYP are at an elevated risk of experiencing mental health issues, such as those who have experienced the care system are.
Care Experience
A child or young person is ‘care experienced’ if they have received statutory involvement, and in the U.K. context, it means that legal responsibility has transferred to local authorities. This includes individuals who have experienced, or are currently, living in residential care, foster care, kinship care, or at home with a supervision order. Adopted children who were previously looked after are also care-experienced. In 2022/2023, there were approximately 107,000 children in care in the United Kingdom, an increase of 8% over the last 5 years (Department for Education, 2023; Department of Health Northern Ireland, 2024; Scottish Government, 2024; Welsh Government, 2025), with a larger proportion experiencing care sometime during their lifetime (Devaney et al., 2023). Most CYP are placed with a relative, friend or approved carer, with non-relative foster care being the most common placement in the United Kingdom (Department for Education, 2023). Many CYP experience multiple placements, for example, In England, Wales and Scotland around 4% to 11% of CYP had three or more placements during the year 2022/2023 (NSPCC, 2024). In England and Wales, 3,234 looked-after children were adopted during the year ending March 31, 2024 (Coram BAAF, 2025; Welsh Government, 2025).
The Mental Health and Well-Being of Care-Experienced CYP
Compared to non-care-experienced populations, CYP who have experienced care are at increased risk of poor subjective well-being (Wijedasa et al., 2022). They experience rates of mental health difficulties approximately five times higher than their peers; and almost half of children in care meet the criteria for a diagnosable mental health condition (Dubois-Comtois et al., 2021; Engler et al., 2022). CYP adopted from local authority care are also at greater risk of mental health difficulties compared to their non-adopted peers (Paine et al., 2021). Conduct disorder, depression, and post-traumatic stress disorder appear to be the most common difficulties experienced (Engler et al., 2022), and comorbidity is common. Suicide attempts are more than three times as likely in CYP placed in care compared to non-care populations (Evans et al., 2017).
There are a number of explanations why this population may experience poorer mental health. Numerous studies confirm that care-experienced CYP have faced more adversity than their non-care-experienced peers (Lester et al., 2020; Turney & Wildeman, 2017), including adopted children (Anthony et al., 2019). In addition to experiences prior to entering care, all CYP in care will have experienced separation from family and other connections. Whilst in care, they may have experienced placement moves and changes of school and community (Cameron et al., 2018). Other aspects which may amplify their risk of poorer mental health and well-being (MHW) include difficulty accessing mental health support and appropriate diagnosis and treatments (McGuire et al., 2022).
Social Support and Mental Health
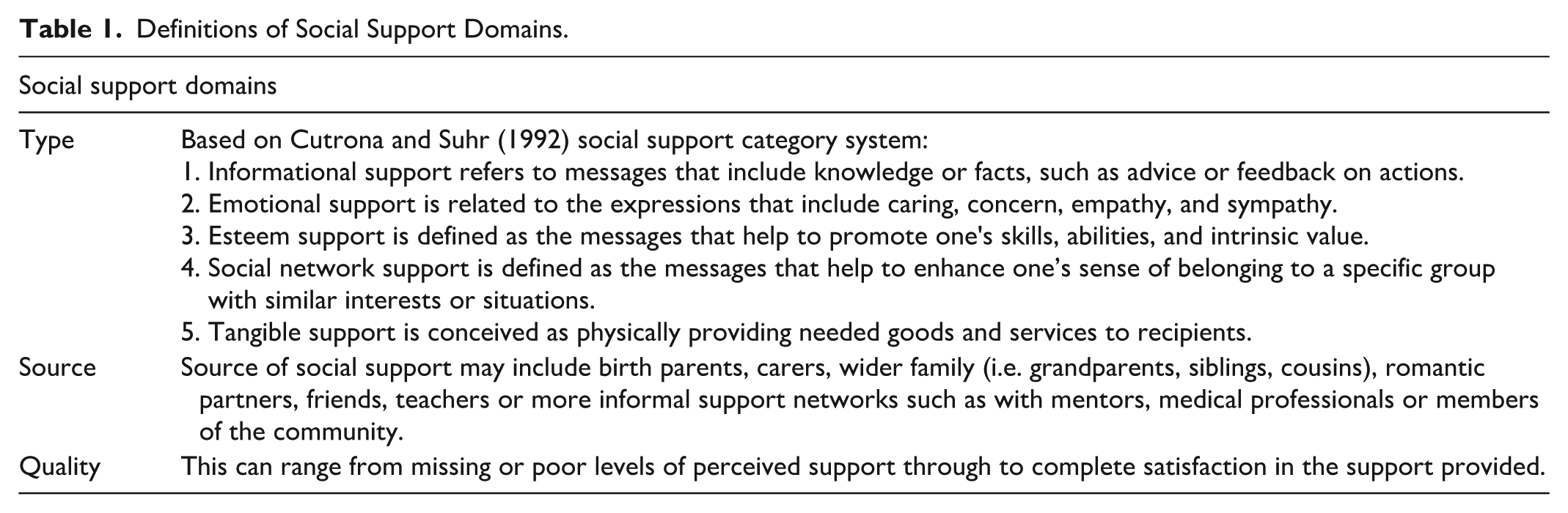
CYP are most likely to thrive in an environment where adversity is minimised and protective factors, such as social support, are enhanced (Buchanan et al., 2023). Social support can be understood as behaviours that communicate to an individual that they are valued and cared for (Barnes & Duck, 1994). Social support is commonly conceptualised in the following categories: emotional support (the care, appreciation, comfort, love, acceptance, and empathy others offer us), informational support (e.g. advice, guidance, and problem-solving), and tangible support e.g. practical help, assistance, and material aid (Feeney & Collins, 2015; Goldsmith, 2004). Other categories of support considered by different theoretical models include esteem and social network support (Cutrona, 1990). Esteem support is defined as messages that help to promote one’s skills, abilities, and intrinsic value. Social network support is defined as messages that help to enhance one’s sense of belonging to a specific group with similar interests or situations.
Numerous evidence including systematic reviews demonstrate that perceived social support is associated with a reduction in stress and improved MHW outcomes (Benca-Bachman et al., 2020; Heerde & Hemphill, 2018; Rueger et al., 2016). Two theories on the mechanism between social support and mental health are the stress-buffering and main-effects models (Kawachi & Berkman, 2001; Lakey & Cohen, 2000). Whilst the stress-buffering model suggests that social support reduces the impact of negative life events on a person’s health, the main effects model hypothesis that there are benefits inherent to social relationships irrespective of the stress experienced by a person. Mechanisms proposed include feelings of belonging, security and self-worth; developing trustful and intimate relationships; and improving access to resources and opportunities (Okland & Oterholm, 2022; Vila, 2021).
Social support is a multi-dimensional construct that varies by type, source, quantity, and quality of assistance (Morelli et al., 2015). Social support can come from a variety of sources, including, but not limited to, family, friends, romantic partners, community ties, and colleagues (Li et al., 2021). Sources of social support can be innate (e.g. family and friends) or more formal (e.g. providers of mental health interventions or housing). The quality of the perceived support is also important, with evidence suggesting that support perceived with a high level of satisfaction can make a significant contribution to overall health (Vandervoort, 1999). Theories of social support take into account that not all sources of social support are necessarily supportive and that some relationships can be burdensome and create problems (Feeney & Collins, 2015).
Social Support for Care-Experienced CYP
The importance of supportive relationships for care-experienced individuals was highlighted by the Care Inquiry (Boddy, 2013), which stated ‘it is the relationships with people who care for and about children that are the golden threads in children’s lives’ (Boddy 2013, p. 2). The Bright Spots survey of CYP in care in England and Wales stated that it is vital for well-being that every child has a relationship with a trusted adult (Wood & Selwyn, 2017). Studies show that good quality relationships are associated with better mental health and increased stability for care-experienced CYP (Anthony et al., 2019; Furlong et al., 2021); mutually meaningful relationships in adulthood (Ball et al., 2021); and care leaver engagement with support and enhanced self-determination (Hyde & Atkinson, 2019). However, while there is evidence that relationships are associated with better MHW outcomes, we know very little about care-experienced CYP’s perceived social support in the United Kingdom (Evans et al., 2022; Stapley et al., 2021).
Purpose of the Present Study
Care-experienced CYP experience disproportionately high levels of mental health difficulties. Although social support is recognised as a key protective factor, the evidence on mental health-related social support for this population has not been comprehensively mapped. Existing studies are dispersed across disciplines, use varied definitions of support, and span multiple care placements, leaving policymakers and practitioners without a clear picture of what types and sources of support have been examined or how support quality has been conceptualised. A consolidated overview is needed to inform relationship-based practice, identify gaps in provision, and guide policy aimed at reducing mental health inequalities. A scoping review was therefore the most appropriate approach. Scoping reviews map the breadth and nature of research, clarify conceptual boundaries, and identify evidence clusters and gaps in areas where study designs, populations and definitions are heterogeneous (Arksey & O’Malley, 2005; Peters et al., 2015). They also act as precursors to systematic reviews by helping determine whether the evidence base is sufficiently conceptually and methodologically aligned to support future effectiveness syntheses (Munn et al., 2018). As our aim was to describe the landscape of mental health-related social support rather than evaluate effectiveness, a scoping review offered the best-fit design.
Cross-Country Terminology and Operational Definition
Although this review was initiated through U.K. stakeholder consultations, its evidence base spans high-income countries with broadly comparable child-welfare systems, characterised by structural similarities (e.g. state responsibility for children in care, foster/residential care models, transitional support frameworks; Stabler et al., 2022; OECD, 2022). Using a functional-equivalence approach ensures that international samples were conceptually aligned with U.K. definitions of care experience.
The aim of this scoping review is to provide a comprehensive map of the evidence base on MHW-related social support for care-experienced CYP in high-income countries. Specifically, the review addresses the following research questions:
What does the existing evidence tell us about the types of MHW-related social support available to care-experienced CYP?
What does the existing evidence tell us about the sources of MHW-related social support available to this population?
What does the existing evidence tell us about the quality of MHW-related social support as described or measured in the literature?
By systematically mapping these three dimensions, the review aims to identify key evidence clusters and gaps, and priority areas for future research including laying the groundwork for intervention-focused systematic reviews, policy development and practice improvement in the United Kingdom and other high-income contexts.
This review takes a holistic view of MHW, and ‘mental health and well-being related social support’ refers to ‘any type of support to individuals that aims to protect or promote their psychosocial well-being or prevent or treat mental health conditions’ (Tol et al., 2015). A debate is ongoing as to whether MHW are distinct constructs. The single continuum model suggests that well-being is the absence of mental ill-health, whereas the dual continua model proposes that MHW are related but separate constructs, suggesting individuals can experience mental health difficulties while maintaining high well-being (Crinson & Martino, 2017; Gautam et al., 2024). Recent research with a sample of care-experienced CYP found moderate associations between MHW. This association varied by age; many early adolescents with clinically elevated mental health reported average well-being but mental health was closely related to poor well-being in the older adolescent age group (Carter et al., 2025).
Social support will be considered according to three domains: type; source; and quality. These terms are explained in Table 1. This will identify key evidence clusters, gaps and uncertainties (Armstrong et al., 2011), inform policy and practice and provide recommendations for the direction of future research.
Definitions of Social Support Domains.
Method
Study Design
This study employed a scoping review methodology, a type of knowledge synthesis approach used to map the main sources and types of evidence available. It was supported by best practice methodology (Arksey & O’Malley, 2005; Mak & Thomas, 2022; Peters et al., 2015). The review is reported in accordance with the Preferred Reporting for Scoping Reviews (PRISMA-ScR) checklist (Tricco et al., 2018). The protocol was developed by RA and registered at the Open Science Framework on January 30, 2024 (https://osf.io/mg9td).
Stage 1: Identification of the Research Questions
The review need was initially identified and then developed in response to a ‘Window into our Priorities document’ (ExCHANGE, 2020) produced by CASCADE Voices – a group of young people associated with Voices from Care Cymru, Youth Fostering Ambassadors – a group of young people associated with The Fostering Network, Tribe – a group of young people involved in the Reaching Wider ‘Diamond Project’ at Swansea University, and other care-experienced CYP. The voices of those with lived experience highlighted the importance of feeling loved and appreciated. A scoping search showed that no previous studies had been undertaken to map what is known about care-experienced CYP’s perceptions of social support.
Stage 2: Identifying Relevant Studies
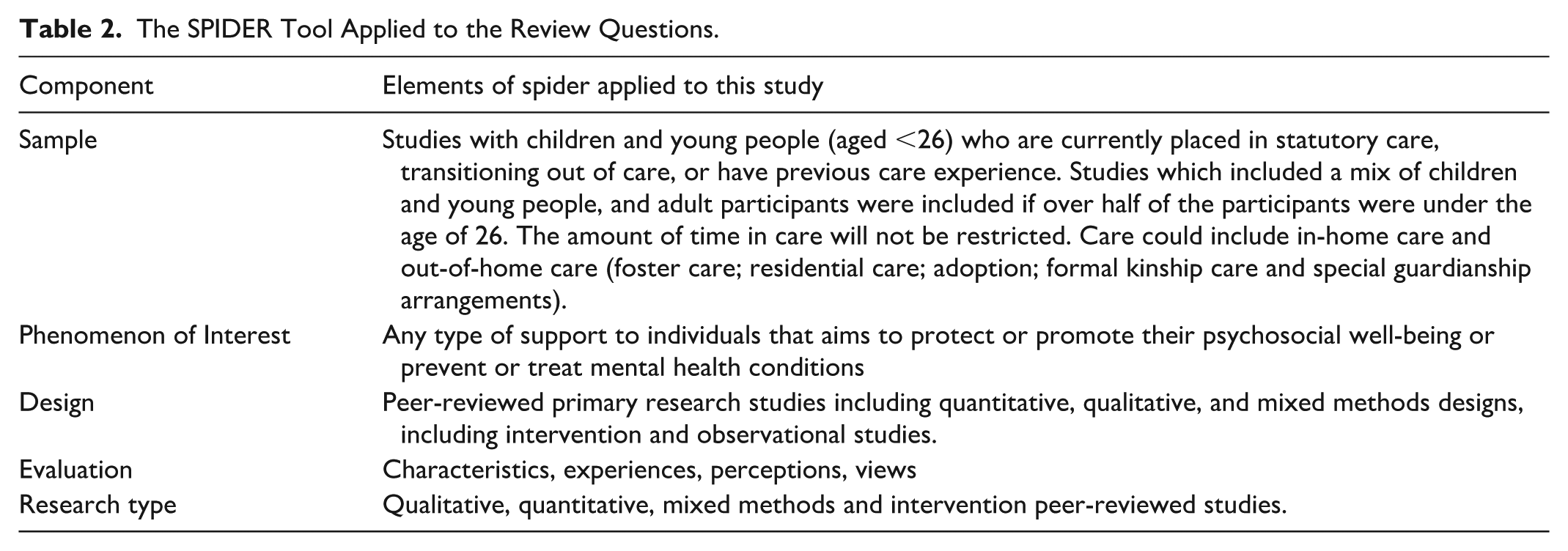
The inclusion criteria were developed in accordance with the Sample, Phenomenon of Interest, Design, Evaluation, and Research (SPIDER) framework, as presented in Table 2 (Cooke et al., 2012). We included studies in English published from 2008 onwards. This date was chosen due to the implementation of The Children and Young Person Act 2008, which aimed to ensure children in care receive high-quality care and services and to improve the stability of placements. We defined high-income countries using the World Bank income classification, which categorises countries based on gross national income per capita. Restricting inclusion to countries designated as ‘high income’ assisted comparability with the U.K.’s child welfare system. Where studies included samples from multiple countries, they were included if the majority of the sample was from high-income countries as listed. We applied an upper age threshold of 26 years, consistent with United Kingdom and international definitions of ‘young people’ in child welfare and leaving-care policy, where support is routinely provided up to age 25. This approach ensured that included samples reflected developmental periods in which care systems continue to influence young people’s social support networks and MHW. Studies were included if more than half of the participants were aged under 26, allowing us to capture evidence relating to the transition from care to adulthood.
The SPIDER Tool Applied to the Review Questions.
A comprehensive search strategy was developed by an experienced Systematic Reviewer (SW) in Medline ALL (Ovid; see Supplemental Material A1) and adapted to the functionality of six electronic bibliographic databases: PsycINFO, Scopus, Web of Science (Social Sciences Citation Index and Emerging Sources Citation Index), Cochrane (CENTRAL and Cochrane Database of Systematic Reviews), Social Policy & Practice, and ERIC.
Stage 3: Study Selection
Deduplication and study selection were conducted using Endnote. To ensure high inter-rater reliability, a calibration exercise was conducted at the beginning of the screening process. For calibration, a random sample of 50 titles and abstracts were screened independently in duplicate by two reviewers (RA and ZH) against the predefined inclusion criteria in combination with a screening tool (Polanin et al., 2019). Following this, any discrepancies were discussed with a third reviewer (KM) and amendments were made to the screening tool. Following calibration, titles and abstracts were screened independently by a single reviewer (RA or ZH). Weekly meetings were held to instil a culture of discussion, exploration, and curiosity while decreasing ‘coder drift’ (Lipsey & Wilson, 2001; Polanin et al., 2019). Subsequently, the full text of studies selected for inclusion was identified, and a second calibration exercise was conducted. For this exercise, 10% of full texts were screened independently in duplicate against the inclusion criteria by two reviewers (RA and ZH). Any uncertainties were discussed with the assistance of a third reviewer (KM). Following calibration, full texts were screened independently by a single reviewer (RA). Full texts that did not meet the eligibility criteria were excluded and reasons for exclusion recorded. Since this is a scoping review aiming to map all available evidence, we did not conduct quality appraisal of included studies. This approach is consistent with best practice methodological recommendations (Peters et al., 2015; Tricco et al., 2016).
Stage 4: Charting the Data
A standardised data extraction form was adapted from the template data extraction instrument for scoping reviews provided in the JBI Manual for evidence synthesis (Peters et al., 2015). The data were extracted into Microsoft Excel to collect the following topics: study identification (i.e. title, author(s), and year of publication); sample characteristics (i.e. sample size, gender, age, ethnicity, care placement type, country they experienced care); study design; measures; social support (i.e. type, source, and if quality was assessed); and main findings. We mapped the diversity characteristics reported in included studies onto the PROGRESS-Plus equity framework, which is widely used to conceptualise dimensions of inequity in evidence syntheses. A calibration exercise was conducted to pilot the data extraction form. For calibration, data were extracted from five papers independently in duplicate by two reviewers (RA and ZH). The experiences of the reviewers were discussed with a third reviewer (RE), and the data extraction form revised. Following this, one reviewer (RA) extracted the data independently, with a second reviewer (ZM) checking the accuracy of a random sample of 60 (approximately 25% of included studies).
Step 5: Collating, Summarising, and Reporting the Results
Study characteristics were summarised numerically with frequency and percentage/proportion statistics. We synthesised the data according to the three research questions previously defined. Studies were numerically summarised, with frequencies of different type, source, and quality of social support. Qualitative studies were synthesised using thematic analysis (Auerbach & Silverstein, 2003), a useful and recommended approach in scoping reviews as it investigates and examines patterns that emerge from the research (Elo & Kyngäs, 2008). The main researcher (RA) examined excerpts of text from included qualitative studies, assessed how it related to the research questions and created a code (label) that best reflected that text. A list of tentative codes (a codebook) was created and modified iteratively as RA engaged in data analysis. Once codes were developed, a review of the codes and how they related to each other helped to identify patterns, which led to themes. Microsoft Word software stored excerpts from the studies, and NVivo software (Dhakal, 2022) was used to identify themes. The results were reported using a narrative summary for each research question that integrated qualitative and quantitative findings and associated infographics that present the evidence gaps and clusters according to research questions.
Stage 6: Stakeholder Involvement
In addition to the prioritisation exercise, which inspired the review, following preliminary synthesis, we held a structured public involvement session with members of CASCADE Voices (https://cascadewales.org/engagement/cascade-voices/), an established group of care-experienced young people (N = 4). The lead researcher presented the emerging evidence map and thematic findings in an accessible format and facilitated discussion focused on how the results aligned with participants’ lived experiences, where they identified gaps, and what they felt should be prioritised in future research and practice. The session was conducted face-to-face over 2 hours, and participants received a £25 voucher for their contribution. Their feedback was documented and used to refine the interpretation of the findings and shape the implications for research, policy, and practice.
Changes to Protocol
Due to initial searches indicating significant sensitivity and a high retrieval rate, the review focused on the mapping of these retrievals. Unpicking relevant systematic reviews and forward and backward citation tracking was not achievable within the timescales.
Results
Study Characteristics
A total of 5,943 individual study reports were identified, and titles and abstracts were screened (see Figure 1 for the flow of studies through the scoping review). Of these, 507 were included and screened at full text resulting in 246 studies (see Supplemental File Table 2 for full list of included studies). Table 3 provides an overview of the characteristics of included studies.
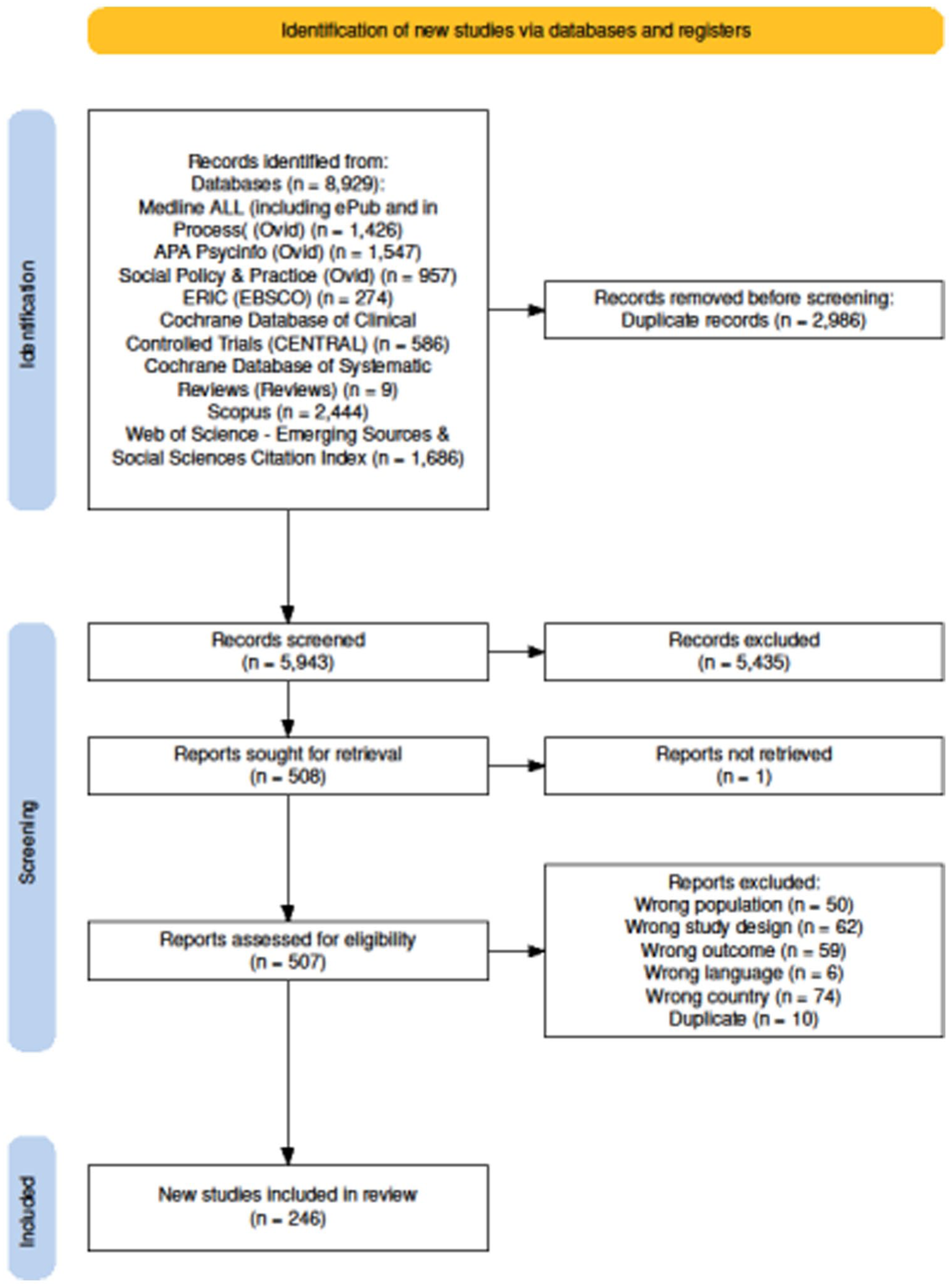
PRISMA flow diagram.
Descriptive Information About the Included Studies.
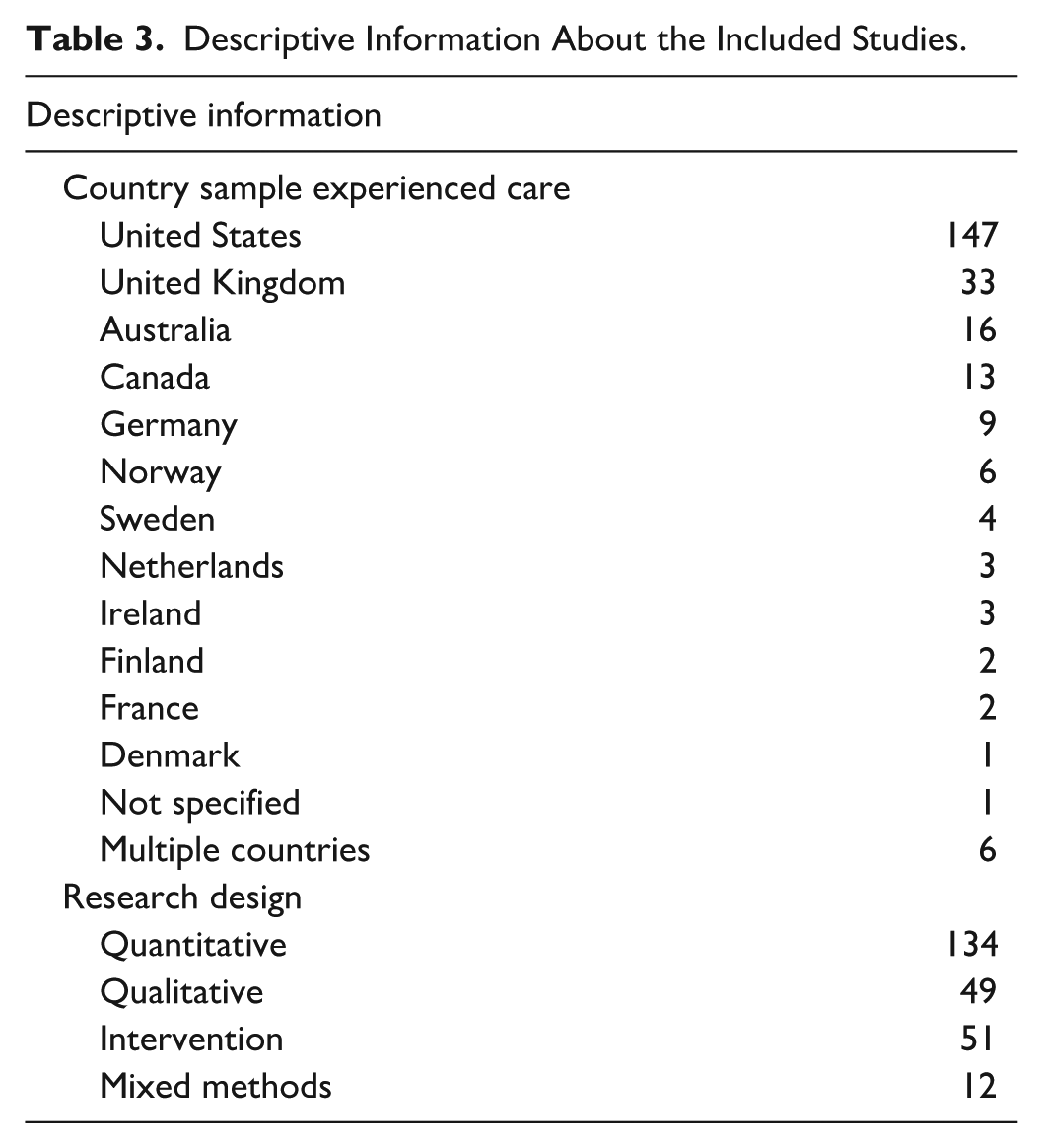
Studies were published between 2008 and 2024 with an upward trend in studies on this topic. The majority of studies were published in the last decade, with 94 studies published since 2020 (Figure 2). Studies included CYP with experience of care in 13 different countries. The vast majority of studies were from the United States (N = 147, 60%); the United Kingdom (N = 33, 13%) and Australia (N = 16, 7%). There were six studies where the sample was from multiple countries, including United States and Australia (Waid et al., 2024); England and Finland (Törrönen et al., 2023); Germany and Georgia (Spangler et al., 2019); United States, Australia and Canada (Hambrick et al., 2018) and Germany, Austria, Croatia, Spain, and France (Garcia-Molsosa et al., 2019, 2021). See Table 3 for the full country breakdown.
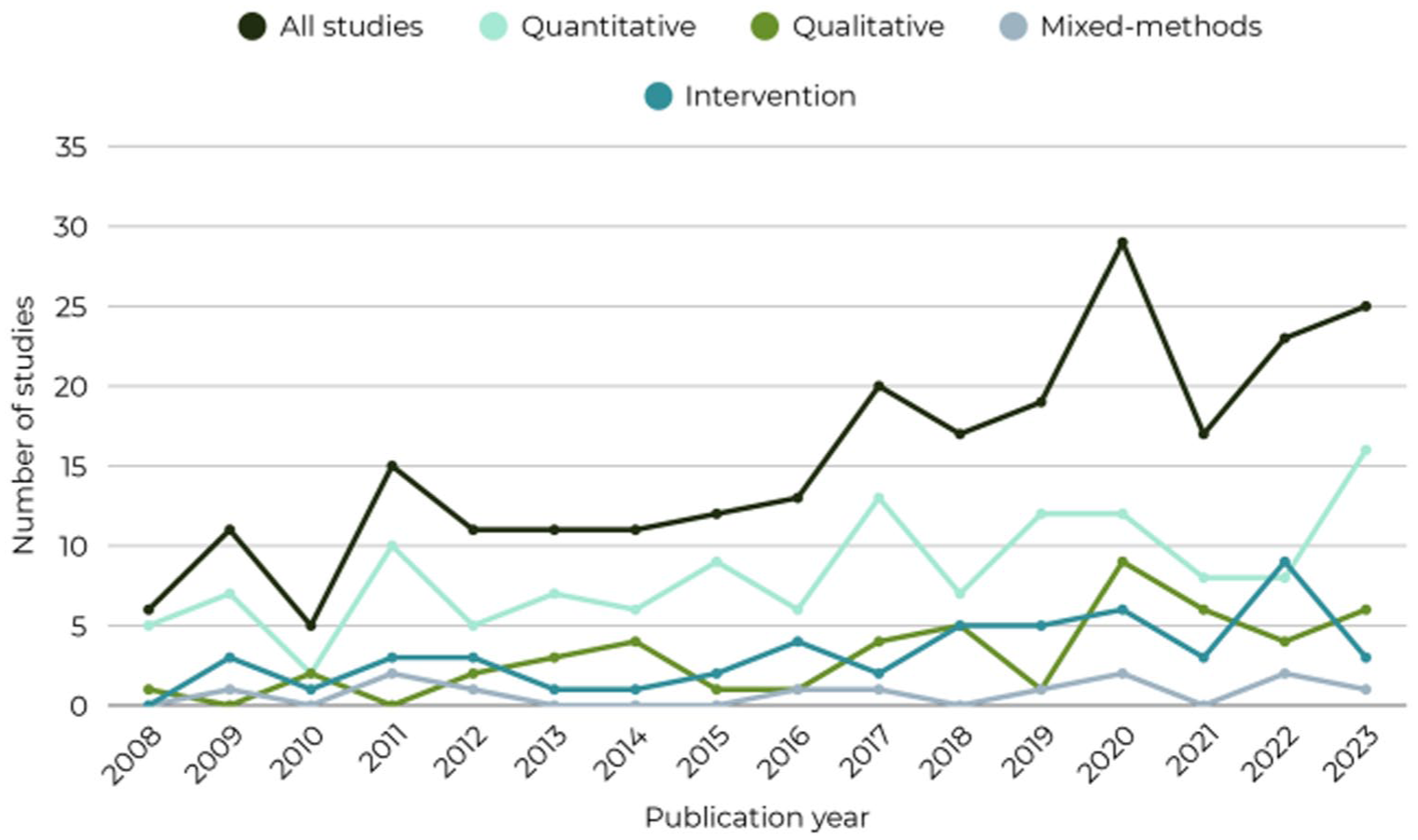
Peer-reviewed studies published per year since 2008, total publications and by method.
Population Characteristics
Age of individuals in care was recorded in most studies (N = 235, 96%), ranging from 1 to 37 years old. The mean age was reported in N = 163 studies, and the derived mean age for those samples was M = 10.43 years old. Gender was recorded in 228 studies, with only eight studies including categories other than ‘male/boy’ and ‘female/girl’. These studies gave the proportion who were ‘non-binary’, ‘trans’ or noted they identified as ‘other’ or did not want to disclose this information. There were six studies that targeted only one gender, with an equal mix of all boys and all girls studies. Race and/or ethnicity were reported in 174 studies (70%). This varied across studies; from detailed population descriptions to reporting the proportion of ‘White’ and ‘non-White’ participants. Of studies that provided information about ethnicity, the most common ethnicity was White/Caucasian (N = 74, 43%) followed by Black/African American (N = 54, 31%).
Research Design
The majority of included studies used quantitative methods (N = 134, 54%), with 49 (20%) qualitative studies and 12 mixed-method studies. There were an additional 51 (21%) studies which used a range of qualitative and quantitative methods to evaluate an intervention. There was a clear upward trend in the number of studies published for all types of study design, except for mixed-methods studies, which remained fairly stable (Figure 2). The split of research designs demonstrates a preference for quantitative methods. Out of the 134 quantitative papers, the majority (N = 86, 64%) were cross-sectional, with 48 (36%) longitudinal studies. Of the longitudinal studies, there was an equal mix of studies using 2 time points and ‘3 or more’ time points. The most prevalent dataset used was the National Longitudinal Study of Adolescent Health (Harris & Udry, 2022).
Care Placement
A large proportion of studies included samples of CYP who had experience of more than one type of placement (N = 100, 41%). The majority of studies (N = 156) collected data from CYP who currently or previously lived in foster care, second to residential care (N = 90) and care with extended family, that is, kinship care (N = 82). There were 41 studies of adopted CYP, and these samples were made of private adoptions (N = 5), adoption from care (N = 25) and mixed samples of private adoptions and those adopted from care, or where this information wasn’t clear or reported (N = 11). Other placements included: those living in or had previously lived in independent living (N = 12); those living at home with parents under a care order (N = 12) and special guardianship (N = 1). There were 10 studies classified as ‘other’ and these included young people who were homeless, in ‘transitional living programs’, as well as descriptions such as ‘other out of home arrangements’ or ‘use of a public system of care’.
Mental Health and Well-Being
The review extracted MHW outcomes as reported by included studies, but these were usually broad, non-diagnostic measures (details can be found in Supplemental Table 2). The majority of studies examined ‘mental, behavioural or neurodevelopmental disorders’ (N = 204), and the most prevalent measures used to assess mental, behavioural, or neurodevelopmental disorders were the Child Behaviour Checklist (Achenbach, 1999) and the Strengths and Difficulties Questionnaire (Goodman & Goodman, 2009). Approximately 1 in 4 studies (N = 65) focused on multiple aspects of MHW, for example, mental health and quality of life together. The second most common aspect of MHW studied was ‘subjective well-being, life satisfaction or quality of life’ (N = 57); with N = 32 studies examining ‘well-being’, N = 11 studies examining quality of life and N = 10 studies examining life satisfaction. A smaller number of studies examined self-harm, suicide ideation or suicide (N = 10). Positive aspects of mental health related to ‘resilience’ were captured in N = 36 studies.
MHW constructs were captured using a variety of methods, including validated measures (N = 172), unvalidated measures (N = 9 studies), qualitative interviews (N = 56 studies), diagnostic clinical interviews (N = 16 studies), clinical data of mental health service use or diagnoses (N = 7) and observational tools (N = 4). A small proportion of studies (N = 18) used two methods of assessing MHW, which generally took the form of validated measures alongside diagnostic interviews (N = 12 studies).
Social Support
The Type of MHW-Related Social Support
Most studies (N = 242) reported on or provided enough information to classify the type of support examined. Table 1 gives an overview of the types of social support. Emotional support was the most frequently studied domain of social support (N = 240, 98%). The next most prevalent type of support was tangible support (N = 67), with a focus on housing and financial support. Esteem support was included in 54 studies, with many studies examining the role of mentoring and included aspects such as compliments, teaching ‘life skills’ such as budgeting. Informational support, such as advice or feedback on actions, was examined in 35 studies. Thematic analysis of qualitative studies suggested that in addition to this care-experienced CYP required specific informational support relating to their life history, medical information and vital documents (e.g. identification). The least prevalent type of support examined was social network (N = 16 studies). These studies had mixed findings – for some young people it wasn’t important that people knew of their background/care experience or they did not want to disclose due to the sense of stigma or shame associated with being in care, whereas for others it was important that they had ‘like people’ who had similar experiences. Other social network aspects included relationships with people of the same ethnicity/race, for example, or others experiencing mental health difficulties.
A large number of studies (N = 84) examined multiple types of support, most frequently emotional support was studied in conjunction with other types. Qualitative studies were more likely to look holistically at the child or young person to explore social support they receive or would like to receive, whereas most quantitative studies used specific measures decided in advance to assess types of social support. A small number of studies (N = 3) did not specify or give a description of the type of support examined and instead focused on social network that is, the number of people the child or young person had in their life. Thematic analysis suggested that for most CYP, it wasn’t enough to have one ‘type’ of support. For example, there was a strong theme that emotional support alongside tangible support such as housing and financial assistance was needed for good MHW. An overarching theme was that CYP were aware of inequities in the types of support they experienced compared to peers who had not experienced care. They spoke of adversity they experienced as children including moving homes, changing schools and the losses of support from friends, family and community that go along with these moves. They also reflected on specific aspects that impacted them such as having to leave home at an earlier age than their peers who had not experienced care and the lack of a ‘safety net’ to fall back on for financial or housing help. Themes also included having to budget for rent and living costs which many of their peers did not have to do. For care-experienced young people at university, they spoke about having to gain employment alongside their studies or not having a ‘home’ to return to in the holiday periods.
The Source of MHW-Related Social Support
Most studies (N = 240, 98%) reported on the source of support. We were not able to ascertain the source of support in six studies where they measured quantity of sources for example, a count of how many people the young person had in their life. Over half of the studies (N = 147, 60%) examined multiple sources of social support for care-experienced young people together.
Carers and Family
The most prevalent (N = 139) was support from carers (foster carers and adoptive parents). Thematic analysis of qualitative studies showed mixed findings, with some young people experiencing very positive relationships with carers and others not feeling loved or cared for. Birth parents were examined in 79 studies. Thematic analysis suggested that relationship with birth parents was a complex topic, for some CYP they provided a constant source of support (e.g. ‘blood ties’) which they could turn to, whereas for others birth parents were a source of conflict. Support from relatives providing kinship care was examined in 53 studies and suggested mixed findings. Wider birth family that is, not birth parents or relatives providing kinship care as a source of support was examined in 50 studies, with sibling and grandparent relationships generally focused upon. Studies had mixed findings and highlighted the often-complex dynamics, linked by biology and shared experience. In addition, wider carer family for example, adoptive parent or foster carer biological children or parents was examined in 11 studies.
Friendships
Another common source of support was from friendships and peer acquaintances (N = 79), which included positive experiences including the sharing of personal issues, getting and giving advice, as well as negative experiences of bullying. Thematic analysis revealed positive aspects of friendships such as playfulness in interactions, as well as mutuality (equal power dynamics), reciprocity and autonomy in terms of ‘choosing’ friendships. However, in contrast, some CYP found making friends difficult. Other CYP were hesitant to invest in making friends due to frequent moves, restrictions in being able to spend time with friends, as well as experiences of threats to safety.
Professional Support
Support provided by social workers and other child welfare professionals was examined in 40 studies. Other common professional sources of support include medical professionals (N = 38 studies), which generally included psychologists, psychiatrists or professionals such as school counsellors who helped manage MHW. While relationships with teachers were specifically examined in 32 studies, thematic analysis of qualitative studies suggested that for many CYP ‘school’ in the wider sense was important. School support wasn’t necessarily from teachers and could be from other adults such as teaching assistants, school counsellors or behaviour mentors. Similarly, studies of care leavers who studied at university mentioned university staff and those in professional roles. Smaller numbers of studies examined residential care workers as sources of support (N = 26), mentors (N = 22), and members of the community (N = 21). Thematic analysis of qualitative studies highlighted that members of the community were generally adults who provided extracurricular activities such as sports coaches, those who run youth or holiday clubs or places CYP could partake in hobbies such as gaming and music. Other support in the community came from religious groups and/or attending church. A small number of studies examined romantic partners (N = 15), and these had mixed findings, with some studies showing that romantic partners were an important source of support they could depend on and other studies showing they could be a source of violence and/or conflict.
‘Other’ Sources
For those old enough to gain employment, support from employment specialists, personal advisers and work colleagues was helpful. Youth workers were also mentioned in a small number of studies. Two studies of care-experienced mothers examined the relationship with their own child(ren). Thematic analysis of qualitative studies suggested that for many CYP, it would be hard to pinpoint exactly the ‘source’ but that some people in their lives just felt ‘like family’. Many spoke about having ‘role-models’ in their lives who they aspired to and provided social modelling. One aspect that came up often was advocacy, a source of support who ‘had their back’ and could help them prepare for meetings and make sure their voice was heard in decision-making. An overarching theme around support from professionals was the need and value of coordinated services and a shared understanding of a young person’s experience. There was an overall sense from the qualitative studies that most needed a ‘tribe’ of people in their lives.
The Quality of MHW-Related Social Support
Nearly two-thirds of the studies (N = 159, 65%) examined some aspect of the quality of social support in relation to the child or young person’s MHW. Generally, social support was assessed using a measure or within a qualitative interview. In some studies, the quality of the relationship was assessed using observational tools. The most popular scales to measure social support included the Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 2016) and the original or modified version of the Medical Outcomes Study social support scale (Moser et al., 2012).
Overall, studies suggest that good quality social support can act as a protective factor for MHW outcomes, tested statistically using longitudinal data in 17% of included studies (N = 42). The majority of these studies (N = 39, 93%) found a statistically significant association between social support and MHW. Thematic analysis of qualitative studies highlighted a number of important qualities depicting ‘good quality’ emotional support. The most important factor for emotional support was that CYP felt loved and cared for, and aspects that helped the CYP to feel this way include empathy and acceptance, trust and stability, mutuality and authenticity, and a genuine bond/connection. Quality of tangible support was also cited, particularly the need for improved availability of housing and better-quality living conditions. Quality of informational support was mentioned in terms of wanting professionals/sources (i.e. websites) to have accurate and up to date information.
Discussion
The present review offers the first comprehensive evidence map scoping the international evidence base on MHW-related social support for CYP who have experienced care. A large number of studies (N = 246) were included, highlighting the extent of research in this area, with a clear upward trend in the last decade indicating the momentum for studying this important field. In providing a rich compendium of research illustrating the different types, sources and quality of social support experienced by care-experienced CYP (see Figure 3), this study offers a clear agenda for future research, policy, and practice (see Table 5).
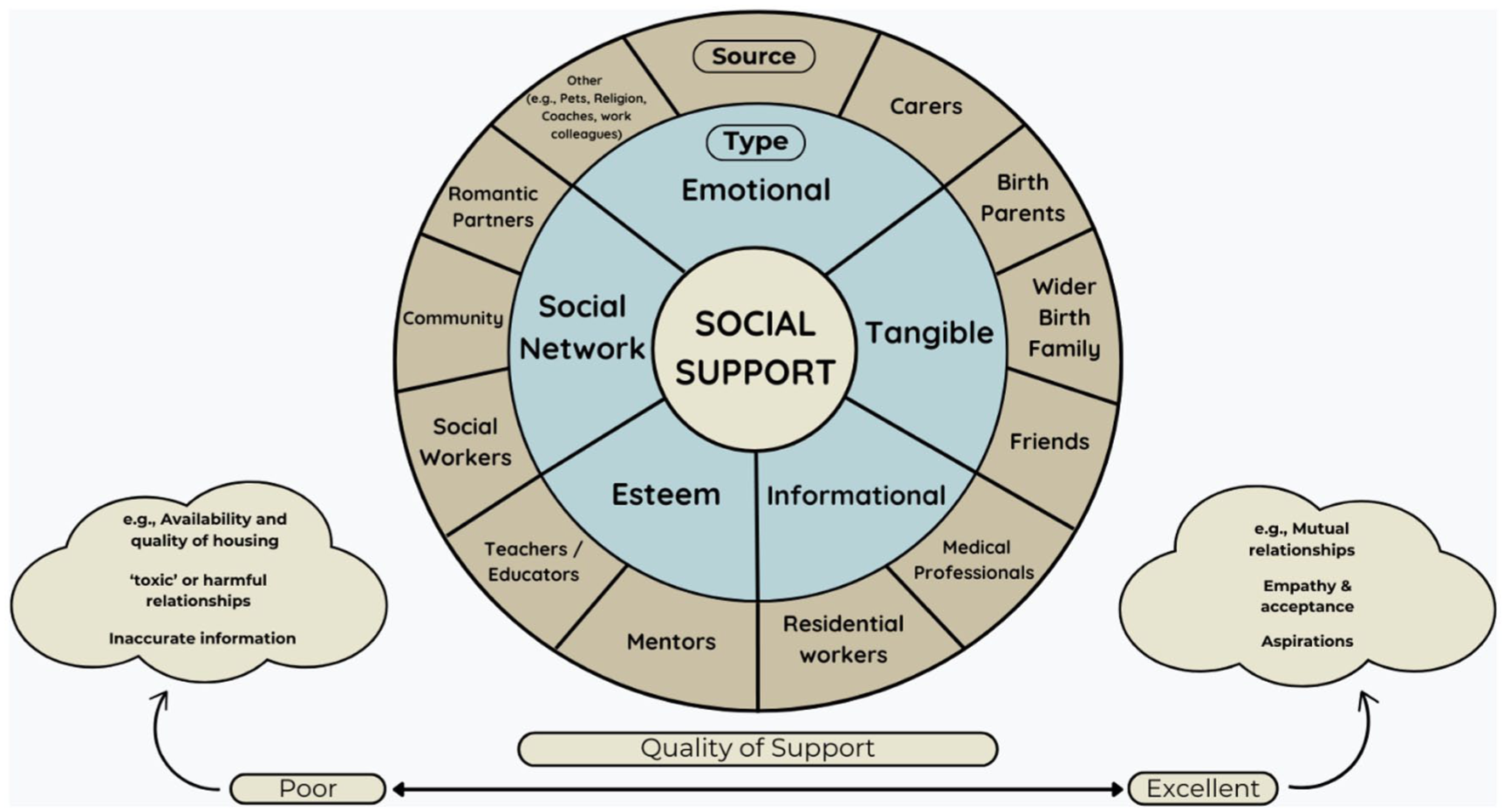
A model of type, source, and quality of social support for care-experienced children and young people.
Limitations of the Existing Evidence Base
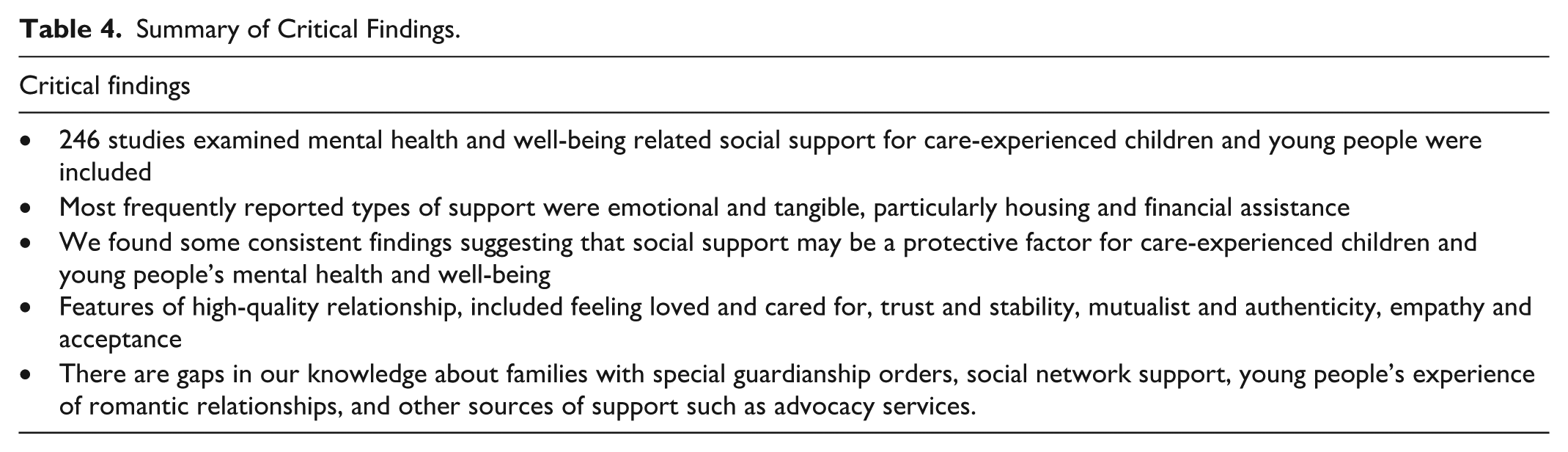
Across the included studies, several limitations in the evidence base should be acknowledged. First, the majority of studies was carried out with CYP in foster care placements, with limited consideration of young people living under a special guardianship arrangement, despite the rising trend of this type of placement (Simmonds & Harwin, 2020). Placement types were often inconsistently described, and there were challenges classifying the care placements in the sample, with international variations in nomenclature (e.g. ‘foster care’ often including non-relative, kin and group homes). Important distinctions such as differences between domestic, private, and international adoptions were frequently absent (Table 5). Moreover, many studies grouped participants under broad labels such as ‘in care’ or ‘care leavers’, with limited consideration of placement histories. This makes it difficult to understand the heterogeneity of samples, and the cumulative losses of and shifting social support needs (Tables 4 and 5).
Summary of Critical Findings.
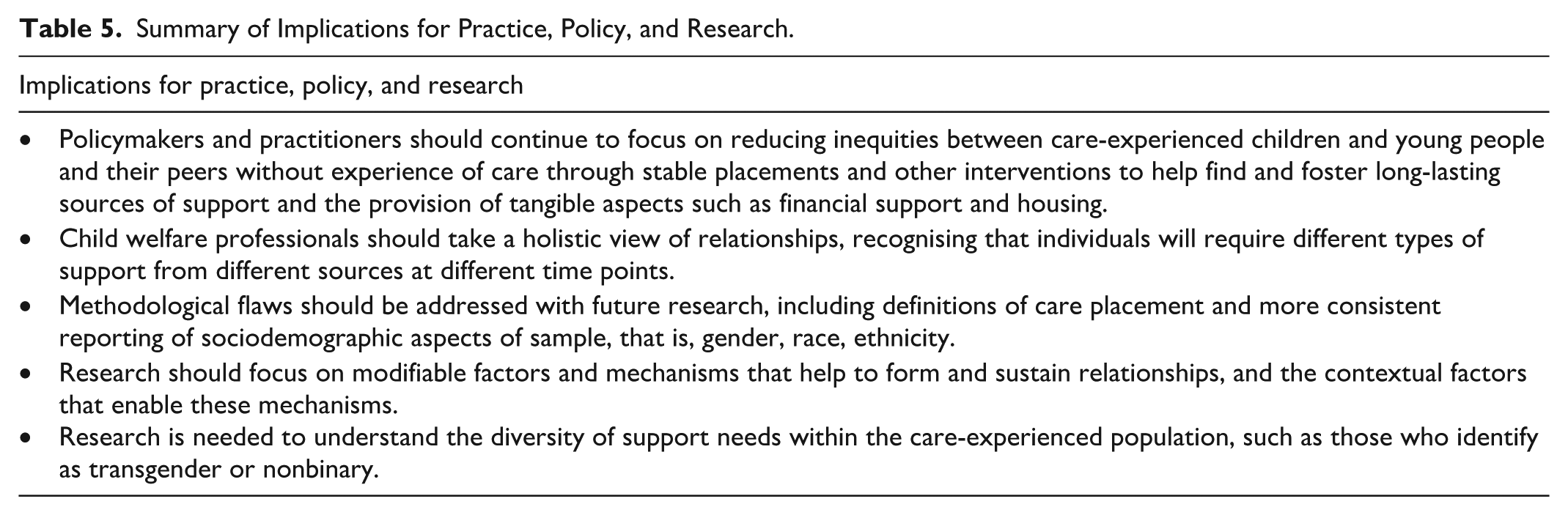
Summary of Implications for Practice, Policy, and Research.
Second, many studies assessed only one dimension of social support, most commonly emotional support, while tangible, informational, esteem and social-network forms of support were less frequently or inconsistently examined. However, it is important to note that many of the studies examining carers used measures and/or observational tools which assessed only emotional support aspects (e.g. attachment, warmth, empathy). Whereas in reality, support from carers is likely to encompass a range of support not measured, including esteem, informational and tangible support, in addition to emotional.
A further limitation of the current evidence base is the lack of diversity in study samples. Although care-experienced youth are themselves a heterogeneous group, most studies provided limited detail on key socio-demographic characteristics, and few explicitly examined whether experiences or effects of social support varied across diverse subgroups. The PROGRESS-Plus equity framework helped highlight that reporting of race and ethnicity was inconsistent, supporting a review on this topic (Javed et al., 2025). Very few studies meaningfully explored how minoritised young people navigate social support within care systems that may not reflect their cultural backgrounds. Similarly, there was minimal representation of LGBTQ+ youth, despite evidence that they face heightened discrimination and identity-related stress. There was also very limited research focusing on disabled or neurodivergent young people, groups that may require distinct support. Future research should purposively recruit and analyse diverse subgroups and use approaches that recognise overlapping identities. This would enable a more nuanced understanding of how social support is accessed and experienced across contexts, and help ensure that interventions are responsive, culturally safe, and equitable.
Social Support
Types
Previous research in both general youth populations and care-experienced samples has consistently identified emotional, tangible, and informational support as core domains of social support (Okland & Oterholm, 2022; Phillips et al., 2024; Teer, 2021). The studies included in this review most frequently examined emotional support, followed by tangible support, particularly housing and financial assistance, which is unsurprising given that care-experienced young people face heightened risks of poverty and housing precarity (Stirling, 2018).
While emotional support has been well-documented in previous studies, our review shows that informational support for care-experienced CYP encompasses a set of distinct, population-specific needs. These include understanding reasons for being in care, access to life-history, medical records and key documents (e.g. ID), supporting previous studies which highlighted these systemic gaps (Clarke & Kent, 2017; Staines & Selwyn, 2020).
Findings relating to esteem support and life skills (e.g. budgeting, navigating services) suggest that these skills are often required earlier than for peers without care experience. Social network support, a domain more commonly studied in general youth mental-health research, remains comparatively under-examined for care-experienced youth. Our findings echo earlier research showing mixed effects: connections with others who share care experience or similar identities can foster belonging, yet stigma, shame and fear of judgement can discourage engagement.
Sources
Research on care-experienced CYP has long emphasised the importance of carers, birth families, peers, and professionals as central sources of support. Our review confirms these established patterns while providing greater nuance regarding variability and complexity. Carers and adoptive parents were frequently identified as sources of support, but experiences varied widely. For some CYP, carers provided stable and nurturing relationships; for others, relationships lacked emotional warmth or were marked by instability. Birth parents remained a meaningful, though often complex, source of support for many. Extended family, including siblings and grandparents, played a significant role, though these relationships were sometimes shaped by past trauma and disrupted connections.
Previous research on peer support for adolescents in general populations highlights its vital contribution to belonging and identity. In line with an earlier review of young people transitioning from care (Teer, 2021), studies included in this review suggest some friendships involved mutuality, playfulness, and companionship, while others involved bullying or the perpetuation of negative/risky behaviours. The threat of violence and not feeling safe among peers was reported particularly by young people living in residential care, consistent with findings from a previous review (Cameron-Mathiassen et al., 2022). It is also important to note that many CYP faced barriers to forming and sustaining friendships due to placement moves, safety concerns, or limited freedom to socialise.
Teachers and school environments were often described as stabilising influences, offering routine, belonging, and access to broader support networks. Professionals such as social workers, mental health practitioners, and personal advisers were frequently cited as important sources of support, yet the quality of these relationships varied substantially. Community-based adults including sports coaches, youth workers, religious leaders, and club organisers emerged as meaningful figures who supported young people’s interests, such as sports, music and gaming, as well as support their religious beliefs, aiding young people’s competence, and identity development consistent with a previous review (Okland & Oterholm, 2022). Our synthesis suggests that both formal and informal mentoring remains a promising yet under-evaluated source of support, especially for older youth. We also identified persistent gaps in research on romantic partners, who are well-studied in general adolescent populations but scarcely examined among care-experienced populations. Overall, qualitative findings suggested that many young people relied on a ‘tribe’ of supportive individuals across multiple domains, rather than a single consistent source. Similar to other reviews (Teer, 2021), we highlight that due to multiple complex factors, including early adversity and instability, CYP who have experienced care may have less opportunity, ability to trust or desire to develop and keep important relationships.
Quality
Quality of support was assessed or measured in the majority of studies, either through qualitative interviews, measures, or observational tools. Studies highlighted a continuum of quality of support from poor through to excellent. High-quality perceived social support is generally associated with better outcomes across ‘general population not in care’ and care-experienced populations (Phillips et al., 2024; Pinheiro et al., 2022; Teer, 2021). Conversely, poor-quality or inconsistent relationships could exacerbate distress. As noted in a previous review on foster versus kinship care, higher contact with family does not necessarily equate to higher relationship quality’ (Hassall et al., 2021). Our findings reaffirm this pattern, with included studies highlighting mixed findings.
In line with broader relationship-science literature (Feeney & Collins, 2015), our synthesis indicates that empathy, trust, reliability, and reciprocity underpin high-quality support. A previous review of young people who ‘Aged Out’ of the child welfare system (Phillips et al., 2024) highlighted the importance of reciprocity and stability for emotional support. Our findings build on this work, suggesting that empathy, trust, and a genuine bond/connection are also important.
By drawing together a large and diverse body of evidence, this review reinforces that high-quality social support is not defined solely by availability but by the extent to which relationships are stable, predictable, responsive, and rooted in genuine care. Included studies highlight that for care-experienced youth, the quality of support is shaped not only by interpersonal dynamics but also by system-level instability, including placement moves, inconsistent professional involvement, and fractured family contact. High-quality support is therefore dependent on both relational and structural conditions.
Implications for Research Policy and Practice
We integrated the review findings with the CASCADE Voices consultation to further refine our understanding of the evidence, policy and practice priorities and gaps that require further research.
Implications for Research
The review identifies several critical gaps that require targeted investigation. First, a notable gap in the existing literature is the limited attention given to support outside of emotional, such as tangible and informational, despite their clear importance. Future research must move beyond emotional-support frameworks to develop more precise definitions, measures, and intervention models for these forms of support. Co-produced research with care-experienced CYP is essential to identify the range of supports to measure, the adults or systems, and what delivery formats are feasible, accessible and acceptable. We suggest that empirical studies should directly operationalise tangible support aspects (including housing stability, financial assistance, transportation).
Second, research is also needed to examine understudied sources of support, such as romantic partners and colleagues, which remain largely absent from the current evidence base. Although romantic relationships are well-established contributors to social support and MHW in young people, the small number of studies involving care-experienced CYP highlight potential benefits and risks. This gap is notable given that relationship histories, and experiences of instability may shape how care-experienced young people form and sustain romantic and workplace relationships. Understanding these dynamics is essential for identifying whether these sources function as protective, neutral, or harmful forms of support within this population.
Third, by mapping how social support has been defined and studied across different contexts, this review lays the groundwork needed to design a future systematic review. Given that a high frequency of studies report positive outcomes regarding relationship-based approaches, a review of effectiveness, mechanisms, and economic outcomes of relationship-focused interventions would be useful, in line with Cochrane guidance for reviews of complex interventions. Fourth, in line with other studies (Pinheiro et al., 2022), our findings highlight a need for studies that examine both positive and negative indicators of adaptation and well-being, moving beyond a predominant focus on mental health difficulties. Consistent with stakeholder recommendations, we highlight the importance of routinely collected relational data that capture the structure and quality of young people’s support networks as previously suggested (Luke, 2024). Such data would enable longitudinal analyses of how relationships evolve over time and how they shape MHW trajectories.
Policy Implications
While implications are drawn for the United Kingdom, we note that international readers may also apply these findings to their own systems. Differences between national care systems – for example, the prevalence of kinship care, the length and availability of leaving-care support, or how services are organised may influence the types of social support available to young people. Stakeholder-engaged approaches to assessing applicability, such as TRANSFER (Munthe-Kaas et al., 2020), support adapting international evidence to local contexts.
The findings underscore the need for policy frameworks that prioritise relational stability and equitable access to support. Within this, funding should be available for the development of evidence-based relational approaches, as suggested in the research implications section. Policy initiatives that promote extended care such as the ‘when I am Ready’ scheme in Wales (Welsh Government, 2016), allow young people to stay with their carer for longer, with the potential to maintain relational continuity, but uptake remains low, and options vary across placement types (Stabler et al., 2023). Policymakers should seek to understand and address the barriers that limit engagement with such programmes. Similar policies are used internationally, such as the ‘Transition Support Service’ in New Zealand (Orangata Mariki, 2023) and the Better Futures and Home Stretch programmes in Victoria, Australia (Victoria State Government, 2025).
Financial and housing insecurity emerged as fundamental obstacles to building stable social support networks. A multinational comparison of care-leaving legislation across 36 countries found that few nations maintain well-developed aftercare frameworks, and most provide minimal financial support beyond age 18, despite clear evidence of vulnerability during this period (Strahl et al., 2021). One important development is the Basic Income for Care Leavers pilot introduced by the Welsh Government, which is currently undergoing a quasi-experimental evaluation. This scheme represents one of the most ambitious efforts globally to address financial insecurity among care-experienced young people (Westlake et al., 2024). Beyond Wales, OECD countries have experimented with a range of transition supports, including housing subsidies, financial allowances, and extended care arrangements up to age 21 to 25. These policies are identified as promising practices that help bridge the gap between care and adulthood, though implementation remains uneven and evidence of effectiveness varies (OECD, 2022). Evidence outside of care-experienced populations demonstrates that unconditional and targeted cash transfers are effective in improving financial security and MHW among vulnerable populations (Crosta et al., 2024; Gassmann et al., 2023; Nunnenmacher, 2023). These established financial-support mechanisms highlight opportunities to extend similar evidence-based approaches to care-experienced young people.
Finally, improved national standards for record-keeping, life-story documentation, and data-sharing practices are essential. Young people require complete, accurate, and timely information about their own histories, and systems must be accountable for ensuring this.
Practice Implications
Traditionally, in social work practice, there has been a focus on independent living skills over social connections (Frimpong-Manso, 2017; Thompson et al., 2016). Our findings point to the importance of adopting a holistic, relationship-centred approach to assessment and support planning. Social workers and other professionals should map young people’s social support networks at key transition points such as entering care, moving placements, transitioning between services (particularly child to adult), or preparing to leave care, to identify gaps and opportunities for strengthening connections. Our review highlighted a number of validated assessment tools available to support professionals in evaluating social support. Several tools were identified within our review, including The MSPSS (Zimet et al., 1988) and The Child and Adolescent Needs and Strengths tool (Lyons, 2009). In addition, relationship-mapping worksheets and eco-maps can help practitioners identify informal and formal supports, relationship gaps, and youth preferences (McCormick et al., 2008), an approach that aligns with stakeholder priorities identified in the CHIMES review (Evans et al., 2024). Integrating these tools into routine assessment could allow workers to monitor the quality, and stability of support networks over time and to plan interventions accordingly.
This review maps existing evidence on how natural mentoring may contribute to young people’s social support networks, including studies that report associations between consistent mentoring relationships and increased perceived support (Bauer et al., 2021; Langeland & Wahl, 2009). For example, therapeutic mentoring models evaluated with foster youth indicate improvements in family and social functioning, school engagement, and reductions in trauma symptoms (Johnson et al., 2011). Although it’s worth noting that inconsistent or short-term mentoring may be associated with poorer outcomes. Other mentoring interventions developed specifically for children in out-of-home care, such as Fostering Healthy Futures, have demonstrated improvements in mental health outcomes (Weiler et al., 2022). These findings align with evidence from general population programmes, such as Big Brothers Big Sisters, which demonstrate improvements in behavioural outcomes, reductions in risk behaviours, and stronger social connections (Herrera et al., 2023). The CHIMES review (Evans et al., 2024) also highlights mentoring as a priority among young people, carers, and professionals, particularly when mentors share lived experience or receive substantial training and supervision.
Collectively, these findings suggest that mentoring may represent a viable approach for strengthening social support, provided interventions are designed to promote relationship continuity, adequate training and supervision, and address the systemic conditions that commonly disrupt supportive adult–child relationships. However, while our scoping review identified mentoring as a frequently described source of support, evidence of effectiveness derives from external evaluations and systematic reviews rather than from the studies mapped here. Social care practice needs more investment (both at the financial and capacity level) to help find and support the development and maintenance of key interpersonal relationships (Nesmith & Christophersen, 2014; Teer, 2021). Facilitating young people’s participation in hobbies, community activities, and peer groups may help foster natural mentoring relationships that support identity development, belonging, and resilience (Bjørlykhaug et al., 2022; Topor et al., 2011).
Given the centrality of informational support, professionals should ensure that young people receive clear, consistent, and accurate communication about their care history, entitlements, and future pathways. This includes proactive advocacy to ensure young people’s voices are heard and respected in decision-making processes.
Strengths and Limitations of This Scoping Review
We followed a rigorous and systematic approach to this scoping review of the literature; however, there are limitations that should be taken into consideration when interpreting the findings. First, this review did not assess the methodological quality of the studies included, as is common practice with scoping reviews. As such, there may be significant variation in the quality of studies contributing to the findings. Second, searches were restricted to English and high-income countries with a similar social care system to the United Kingdom, which may limit generalisability to middle- and lower-income countries. Third, our review was limited to studies indexed in bibliographic databases and as such, we are likely to have missed relevant reports from grey literature and other repositories.
Conclusion
This scoping review highlights the importance of high-quality, stable, and multidimensional social support for care-experienced CYP. While emotional support remains central-tangible, informational, and esteem-related supports are equally critical, particularly as young people navigate the unique challenges associated with being in care. Strengthening relational networks, improving policy frameworks, and enhancing practice approaches have the potential to reduce longstanding MHW inequities and promote more positive, long-term outcomes for this population.
Supplemental Material
sj-docx-1-tva-10.1177_15248380261437098 – Supplemental material for Mental Health and Well-Being-Related Social Support for Care-Experienced Children and Young People: A Scoping Review of Type, Source, and Quality
Supplemental material, sj-docx-1-tva-10.1177_15248380261437098 for Mental Health and Well-Being-Related Social Support for Care-Experienced Children and Young People: A Scoping Review of Type, Source, and Quality by Rebecca Anthony, Simone Willis, Zoe Haslam, Kelly Morgan and Rhiannon Evans in Trauma, Violence, & Abuse
Footnotes
Author Note
The idea for the scoping review was conceived by RA and RE. All authors contributed to the design and the development of the protocol. The manuscript was drafted by RA.
Ethical Considerations
As this study involved the collection and analysis of data from publicly available literature and did not involve human participants, animals, or identifiable personal data, ethical approval was not required. All sources included in this review were properly cited and referenced to ensure academic integrity and transparency. The authors affirm that the review was conducted objectively and without any conflicts of interest.
Consent for Publication
All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author, RA, received Social Care Research Fellowship funding from Health and Care Research Wales, grant number SCF-22-04. The work was also supported by DECIPHer, which is funded by the Welsh Government through Health and Care Research Wales, and the Wolfson Centre for Young People’s Mental Health, established with a grant from the Wolfson Foundation. The funder had no role in developing this protocol.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This scoping review is based on data extracted from publicly available literature sources. All data generated or analysed during this study are included in this published article and its ![]() (if applicable). No new datasets were created or analysed specifically for this study. As such, data sharing is not applicable.
(if applicable). No new datasets were created or analysed specifically for this study. As such, data sharing is not applicable.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.