
Abstract
While a small body of work focuses directly on young people’s experiences of psychotherapy following sexual abuse, to our knowledge, there are no existing reviews of this literature. This systematic review was conducted using Siddaway et al.’s guidelines. Inclusion criteria were: published between 2000 and 2022; used qualitative methodologies; and captured adolescents’ perspectives. Eleven studies were identified, representing an aggregated sample size of 72 young people aged 12 to 18. Methodologies used included thematic analysis, content analysis, conversation analysis, and narrative analysis. A total of 9 of the 11 studies addressed experiences of individual therapy using semi-structured interviews; 2 studies explored experiences of group therapy through focus groups. The review identified three key processes that reflect adolescents’ experiences: engagement, ambivalence to trust; painful processing: exercising agency; and integrating: taking responsibility. Young people struggled to engage in therapy, and it took time to build trust; they experienced improvements in mood and general well-being, facilitated by psychoeducation, talking about the abuse, experiencing difficult emotions, and learning coping skills. They described integrating their abuse experience into their life story, discovering their inner strength and resilience. The therapeutic experience was underpinned by two key support processes: the therapeutic relationship and a supportive environment outside of therapy. This review supports the components of trauma-focused therapy alongside personalizing psychotherapy to the needs of adolescents for agency and autonomy.
Keywords
Introduction
Adolescents are a particularly vulnerable group in terms of mental health due to the complex developmental changes experienced during these years (Starrs, 2019). It is a developmentally crucial time for intervention, given the peak onset of many psychiatric disorders during this period of development (McGorry et al., 2024). The experience of sexual abuse exacerbates this vulnerability. Strong associations have been found between childhood adversities, including sexual abuse, and the first onset of a range of these disorders (Green et al., 2010). Intervention with this group is critical, yet studies report poor access to services (Allnock et al., 2012; Pattison & Cooper, 2024) and concerns about dropout rates among the adolescent population in general (O’Keeffe et al., 2020). According to de Haan et al. (2013), dropout rates for adolescents can range from 28% to as high as 75%.
Several studies attest to the effectiveness of psychotherapy for children and adolescents who have experienced sexual abuse (Hetzel-Riggin et al., 2007; Sánchez-Meca et al., 2011); however, many young people who have been asked their views about therapy have not described it as helpful (Allnock et al., 2015; Jessiman et al., 2017). Where research has involved directly asking young people about their experiences, the analysis has conflated both children’s and adolescents’ experiences, within the one study for example, including young people as young as 6 with older children of 17 or 18 (Capella et al., 2018; Foster & Hagedorn, 2014), thus neglecting to appreciate the distinct developmental phase of adolescence and accompanying developmental tasks. Increased sensitivity to relational power dynamics, the need for growing agency and autonomy, a greater cognitive ability to evaluate relationships and changing boundaries in the parent-child relationship, all influence how therapy is experienced for adolescents (Cook & Monk, 2020). Older adolescents (over 16) have spoken of the need for collaboration in the therapeutic relationship, and not being treated like a child (Harper et al., 2013). It is important that research that endeavors to better understand adolescent experiences also attends to adolescence as a distinct developmental period.
There is now a small but growing body of work that focuses on adolescents’ (aged 12–18 years) experiences of psychotherapy following sexual abuse, in their own words. The objective of this paper is to review these studies to identify if there are common themes emerging from this literature that could help enrich our understanding of what young people find helpful from psychotherapy and offer clinicians and researchers guidance as to how best to serve the needs of young people when presenting to therapy following the experience of sexual abuse.
Child Sexual Abuse and Its Impact
Child sexual abuse (CSA) is defined as: The involvement of a child or an adolescent in sexual activity that he or she does not fully comprehend and is unable to give informed consent to, or for which the child or adolescent is not developmentally prepared and cannot give consent, or that violates the laws or social taboos of society (World Health Organisation, 2017).
Due to its prevalence and impact, it is considered a public health issue (Letourneau et al., 2014). The World Health Organization (WHO, 2017) estimates that 1 in 5 women and 1 in 13 men report experiences of sexual abuse under the age of 17 with 120 million girls and young women under 20 across the globe having suffered some form of forced sexual contact. Most studies on which these estimates are based do not include online sexual abuse. Finkelhor et al. (2024) added questions about online abuse in childhood or adolescence to their survey of respondents aged 18 to 28 and found that prevalence rates increased from 19.8% to 31.6% (females) and 6.2% to 10.8% (males). Such experiences can be diverse and long lasting, impacting on psychological, social, emotional, physiological and behavioral development (Tichelaar et al., 2020). Narang et al. (2019) categorize the impact of sexual abuse on child and adolescent survivors as in the following domains: physical (e.g., sexually transmitted infections); behavioral (e.g., aggression); psychological (e.g., altered sense of self); cognitive distortions (e.g., beliefs such as self-blame); interpersonal and social difficulties (e.g., lack of trust; peer relationship difficulties); body and sexuality (e.g., “damaged goods syndrome”); and mental health disorders (e.g., PTSD). Although Narang et al. and other authors (Carpenter et al., 2016; WHO, 2017) acknowledge that impact varies according to developmental stage, references to impacts that are clearly associated with adolescence, for example, “teenage pregnancy,” “substance abuse disorders” (Narang et al., 2019, p. 1) are presented together with impacts on younger children. According to Allnock et al. (2012), “increasing the provision of and access to treatment is a vital step in reducing the long-term individual and societal consequences of sexual abuse” (p. 320). Adolescents are seen as a challenging group to engage (Cook & Monk, 2020). As young people are typically brought to therapy rather than self-refer, the high dropout rates noted above may be their only way of exercising their autonomy. Voting with their feet through dropping out of therapy may be particularly salient for young people who have experienced sexual abuse with its associated sequelae of disempowerment and helplessness.
Young People’s Voices in Psychotherapy Research Literature
While there has been a growth in qualitative research in psychotherapy, such research has mostly focused on adults’ experiences. In a systematic review of qualitative studies on how young people affected by adverse childhood experiences experience support and services in the United Kingdom, only three studies on sexual abuse were included, all of which relied on samples of adult survivors (Lester et al., 2020). Concerns have been highlighted that participation in such research may be re-traumatizing and distressing for children and young people, however, children and young people have spoken about the benefits of participating in such research (Dittman & Jensen, 2017). Excluding children and young people from such research is also ethically questionable (Eliffe et al., 2020); their views provide valuable information that informs service development (Carlberg et al., 2009), while excluding them prevents them exercising their rights as outlined in the United Nations Declaration on the Rights of the Child (United Nations General Assembly, 1989). Young people who have been sexually abused have been disempowered through the experience of abuse; excluding them from research that impacts their lives can further disempower them, particularly in adolescence, at a time when empowerment and growing autonomy are key developmental tasks (McConville, 1995; Starrs, 2019). Recent qualitative studies have attempted to address the relatively hidden and unacknowledged voices of young people in psychotherapy research (Fiorini et al., 2024). As they navigate this distinct developmental stage, they warrant specific attention.
The Current Study
Several authors have highlighted the need for tailored interventions for young people (Carpenter et al., 2016; McElvaney & Moorhouse, 2022; Midgley et al., 2017). However, to better understand what young people need from therapy, it is necessary to explore with them directly what they found helpful or unhelpful. Qualitative studies, while offering rich detail of in-depth experiences and the phenomenology of the individual, rely on small sample sizes, using purposive sampling. A rigorous, broad overview of the existing evidence can inform practice and policy decisions. Thus, drawing on the aggregated findings of small-scale in-depth studies, it is possible to capture a more comprehensive illustration of young people’s experiences. Prior to 2000, few studies existed that explored children and young people’s experiences of therapy. The last 2 decades have seen a slow but steady increase in studies involving young people being asked directly about their experiences of therapy following sexual abuse. This study, therefore, aimed to conduct a systematic review of qualitative studies capturing adolescents’ (aged 12–18 years) experiences of psychotherapy following sexual abuse. Exploring young people’s experiences where they have accessed therapy may assist our understanding of how we can improve engagement in therapeutic work following sexual abuse and how we can support their continued engagement to enable them to address the many negative impacts of sexual abuse.
Method
Systematic reviews are characterized as “methodical, comprehensive, transparent, and replicable” (Siddaway et al., 2019, p. 751). Qualitative meta-analysis provides a comprehensive representation of the phenomenon under investigation by using the findings of primary qualitative studies as data for further analysis (Schreiber et al., 1997). Thus, a rigorous qualitative analysis of raw data from previous studies can provide “a comprehensive empirically based conceptualization of the processes” (Timulak & McElvaney, 2013, p. 134). Siddaway et al.’s (2019) six stages of conducting a systematic literature review were followed in this study: scoping, planning, identification, screening, eligibility, and study quality. Scoping involved identifying the research question and deciding on the parameters of the review. The research question was: how do young people experience psychotherapy following sexual abuse? As most of the qualitative studies on this phenomenon have been conducted in the past 2 decades, a timeframe of publications between 2000 and 2022 was identified. Planning involved identifying appropriate search terms, inclusion and exclusion criteria with justification, recording decisions regarding searches, using a PRISMA (Page et al., 2021) flow chart to document search results, and completing CASP checklists (https://casp-uk.net/casp-tools-checklists/CASP tool for evaluating qualitative research papers) to evaluate the quality of studies identified.
Search Strategy
The Population Intervention Comparison Outcome Model (Schardt et al., 2007) informed the search strategy: Population, child or adolescent; Intervention, child sex abuse OR child sex assault OR child maltreatment, Context, therapy OR treatment OR intervention, and Outcome, narrative OR feedback OR experience OR perspective AND qualitative research. Inclusion Criteria were primary qualitative studies published in English between 2000 and 2022 that presented raw data (quotes) from adolescents aged 12 to 18 years who had experienced sexual abuse and focused on their experiences of therapy. Exclusion criteria were quantitative studies on outcomes, data from professionals or parents, data from children under 12, and literature reviews or commentaries.
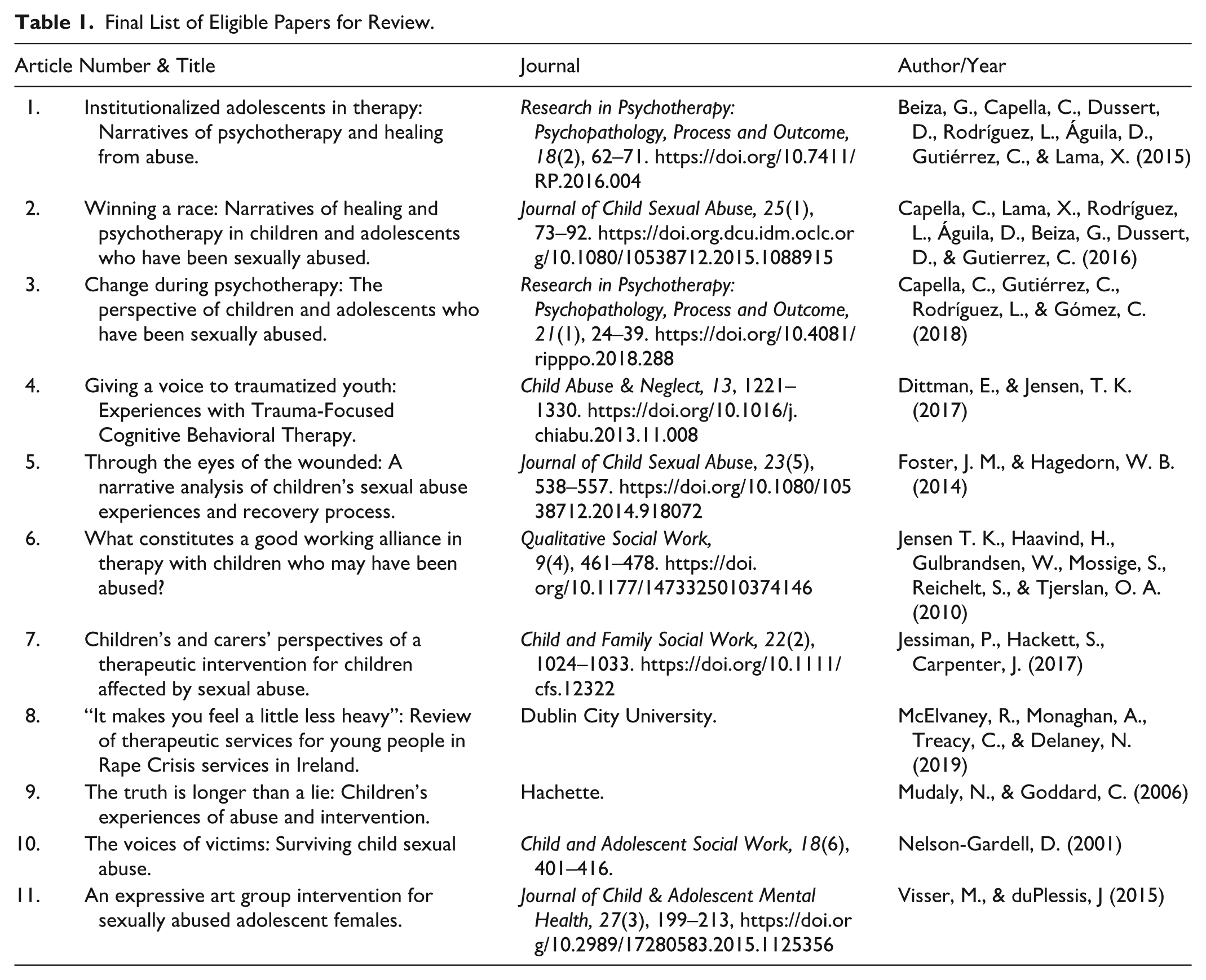
Five databases were searched: Web of Science, PsycINFO, CINAHL, Medline, and Sage Online, using various combinations of the key terms using Boolean operators (i.e., AND, OR). The limiters were: age, qualitative research, and articles published between January 2000 and June 2022. Figure 1 depicts a PRISMA flowchart (Page et al., 2021) illustrating the various stages of the search process. A total of 1,420 papers were identified across the 4 databases, and an additional 17 papers were added through manual searching, primarily through perusing bibliography sections of the relevant papers identified, resulting in a total of 1,437. The titles of these 1,437 papers were read, and where titles were ambiguous, abstracts were read. The removal of duplicates resulted in 49 papers, 32 from the databases and 17 from manual searches. Eligibility involved evaluating the remaining 49 papers by reading the full text of the articles and assessing them against the inclusion and exclusion criteria. This process was conducted independently by the first author and a research assistant. A final sample of 11 papers was identified for thematic analysis, 6 from online databases and 5 from hand searching (reviewing bibliographies and authors’ other publications). Table 1 presents the final sample of 11 papers.
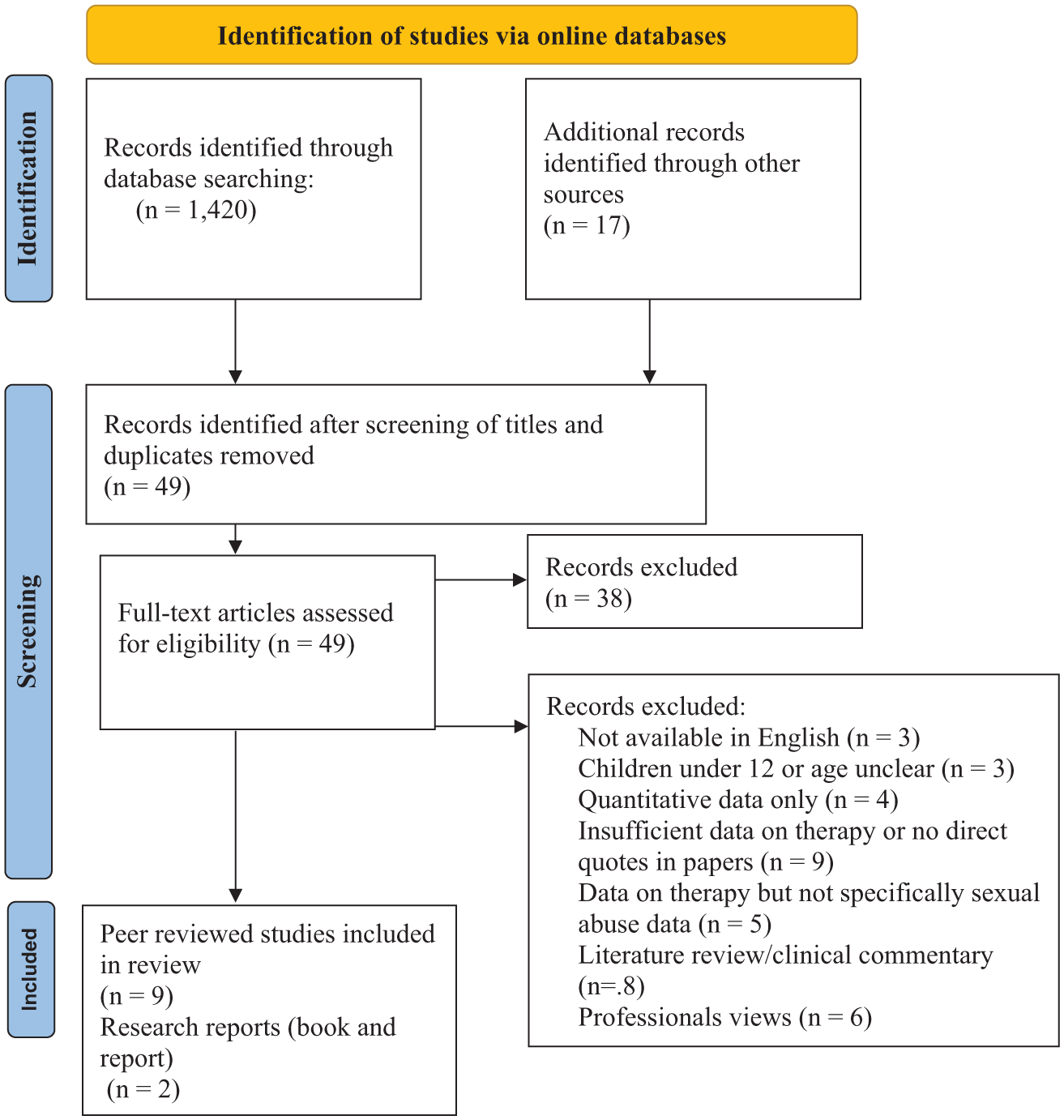
PRISMA (Page et al., 2021) flow diagram.
Final List of Eligible Papers for Review.
Quality Appraisal
The study quality of the 11 was investigated using the Critical Appraisal Skills Program qualitative checklist 2018 (https://casp-uk.net/casp-tools-checklists/CASP tool for evaluating qualitative research papers). Many of the studies were conducted by research teams using parallel coding of the data and discussion of any discrepancies in analysis. Overall, studies were found to be robust in adhering to good practice in conducting qualitative research (Yardley, 2000).
Reflexivity
Few papers discussed reflexivity or the relationship between the researcher and the participants and the issue of potential researcher bias, an important consideration in qualitative research (Creswell & Poth, 2018). Olmos-Vega et al. (2023) discuss the multifaceted nature of reflexivity, how personal, interpersonal, methodological, and contextual factors influence the research process. The first author of this review is a clinical psychologist and integrative psychotherapist with extensive experience of CSA across clinical and academic settings. The second author is a gestalt adolescent psychotherapist and mental health consultant. Both have worked as trainers of psychotherapists. As academics and practitioners, both authors were passionate about privileging adolescent voices in research and finding a way to allow such voices to inform service developments. This stance influenced the decision to focus on adolescents specifically and excludes the voices of younger children, parents, and professionals from the analysis. It may also have influenced the analysis insofar as the findings of the review highlighted the importance of choice and supporting the agency of young people in how therapy is conducted. Both authors work clinically with adolescents and were aware of the challenges of engaging adolescents in therapy. Awareness of these challenges motivated the authors to explore what adolescents found helpful in their experience. Through professional networking, the first author was familiar with the authors of five of the papers reviewed. The involvement of a research assistant, who was unfamiliar with the literature in this field, in the identification of the 11 papers included in the review contributed to the robustness of the process. The first author’s familiarity with the literature and experience of conducting similar studies were an advantage in developing the search terms and consulting gray literature. However, cognizant of potential bias, regular reflexive consultations were held whereby the analysis process, as well as the choice of quotes to illustrate themes, was rigorously interrogated.
Data Collection
Raw data (in the form of quotes) from young people aged 11 to 18 that specifically referred to their experiences of therapy were extracted from published papers and placed in individual Word documents, one document for each study, which were then uploaded to NVivo 12 (QSR International, 2018), a data management software package. Quotes presented without specifying the age of the participant were not included in the dataset. The decision to extract raw data, in the form of participant quotes, was made in an effort to retain as much as possible the essence of young people’s experiences of therapy. As Timulak (2009) notes, in qualitative meta-analyses, the meta-analyst must decide what constitutes data for analysis while retaining their meaning from the primary studies. While some meta-analyses include themes as data, this study only included the raw data – quotes – as data, to foreground the voices of the young participants in these studies and set aside the interpretation offered in the primary papers. The analysis thus focused on young people’s accounts of their experiences, rather than the interpretations of the primary authors. The various papers reviewed addressed a range of research questions, not only the research question of this review, and themes were developed in some papers from interviews with children, adolescents, parents/carers, and professionals. It was therefore considered prudent to rely only on the quotes from adolescent participants in capturing young people’s experiences of therapy. However, it is acknowledged that the primary authors selected these quotes from their own dataset to illustrate their own analysis; more data are likely available from these studies that directly address the research question of this review.
Data Analysis
Reflexive Thematic Analysis (Braun & Clarke, 2019) was used as the guiding analytic framework for conducting this review. Firstly, the extracted data were read and re-read to ensure data familiarization before engaging in identifying codes. The second step involved generating codes guided by the research question of young people’s positive experiences of psychotherapy. An example of such a code is “skills to help me with anxiety.” The third step, identifying initial themes, involved a process of identifying similarities and differences between the open codes and creating a table depicting each initial theme (e.g., coping skills) with the corresponding codes that illustrated each theme, and accompanying quotes to evidence these themes. This table was reviewed with the second author, whereby the fourth and fifth steps, theme definition and naming, and theme review, were followed to clarify the meaning of each initial theme and reach consensus on the final themes (e.g., processing: speaking about the abuse and managing distressing emotions), again through a process of comparative analysis. The sixth step, report production, resulted in the first author preparing a draft results section, which was reviewed by the second author.
Results
Methodological Features of Primary Studies
Table 2 provides an overview of the details of each study. The 11 studies in this review, published in English, represent a total minimum sample size of 72 adolescents, ranging in age from 12 years to 18 years, 1 spanning a diverse range of countries – 3 studies from Chile, 2 from both the United States and Norway, and 1 from Ireland, the United Kingdom, Australia, and South Africa. Some of the studies were broader in focus with differing samples (children, adolescents, parents/carers, or professionals). Nine studies employed individual semi-structured interviews to explore experiences of individual therapy, while two studies collected data through focus groups about group therapy. Questions asked about therapy were similar across studies. Two studies used drawings, although the authors noted that these were used less by adolescents than by younger children. In some studies, data were collected while young people were still attending therapy, while in others, they had completed therapy. In one case, follow-up interviews were conducted a year after therapy finished. The duration of therapy and the theoretical orientation of therapists were not always noted. Where information was available, this could range from three sessions to weekly sessions for 48 months, reflecting considerable variability. The theoretical orientation of therapists also varied. Many studies noted that therapy was provided by psychologists, psychotherapists, or social workers. Trauma-Focused – Cognitive Behavior Therapy was the orientation noted in two of the studies.
Summary of the Characteristics of Each Study.
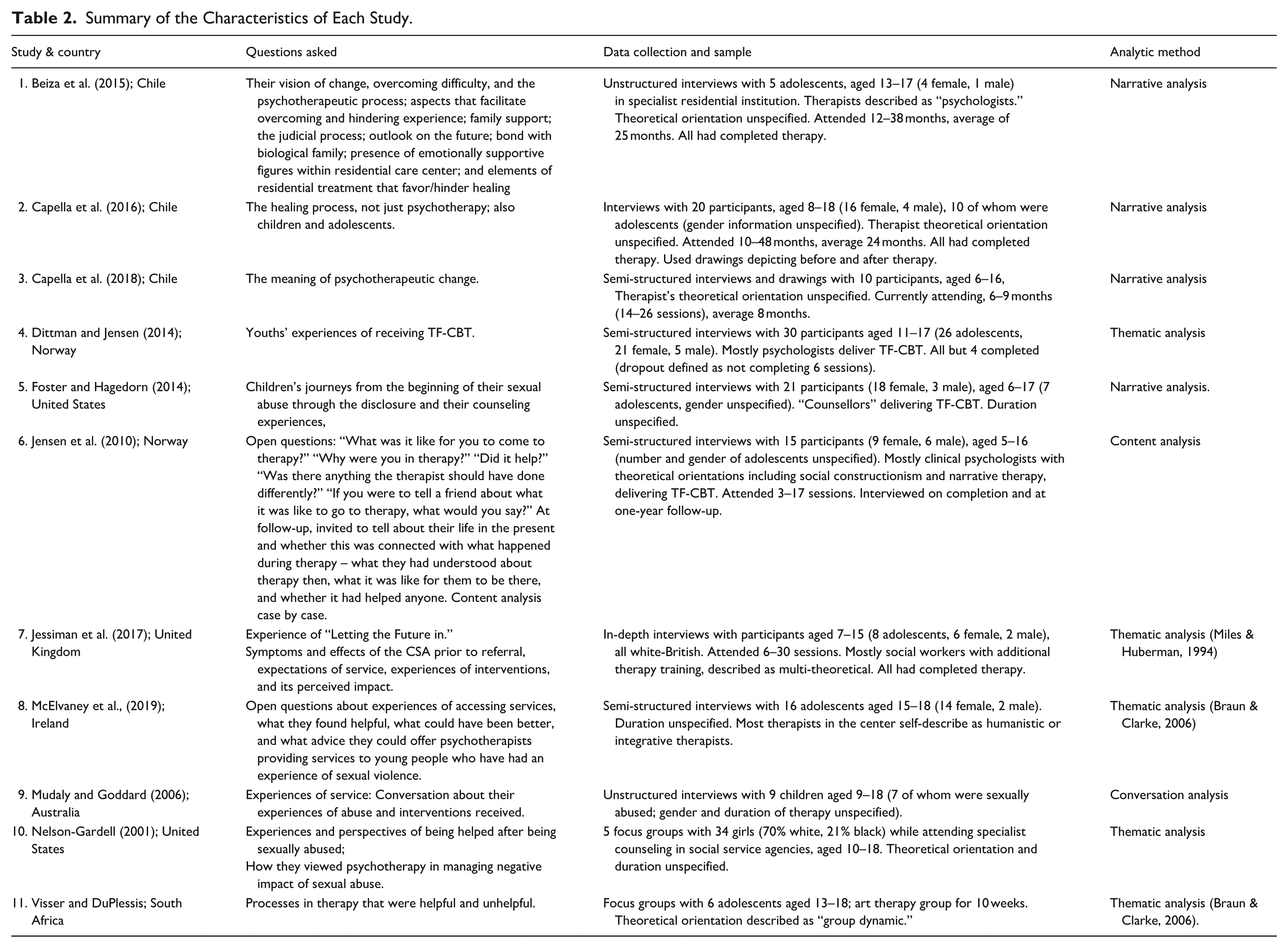
The three studies in Chile involved centers that are part of the Servicio Nacional de Menores (SENAME) network, the principles of which are: “putting a stop to the infringement of adolescents’ rights, re-signifying experiences of sexual abuse and strengthening family and social resources” (SENAME, 2014, cited in Beiza et al., 2015, p. 64) and therapy is provided by psychologists. The U.K. study was conducted in the NSPCC, which uses a specific program, Letting the Future In, a psychodynamically informed approach. One of the U.S. studies noted that therapy was informed by social constructionism and narrative therapy. In the Irish study, participants were attending specialist sexual assault centers where therapists described themselves predominantly (although not exclusively) as humanistic and/or integrative psychotherapists. The remaining three studies did not specify the theoretical orientation of the therapists. It is noteworthy that similar themes were identified across these studies, regardless of the therapeutic orientation of the therapists involved, where this information was noted, and despite different contexts (i.e., individual versus group therapy; generic versus specialist sexual abuse center). While the provision of therapeutic services for those who have experienced sexual abuse may vary from country to country, this was not evident in these papers.
The data analysis methods included narrative analysis, conversation analysis, thematic analysis, and content analysis. Several studies used a team of researchers where triangulation was used in the analytic process. Results were presented in varying formats. In some cases, the “theme” was simply “experiences of therapy.” In other cases, themes focused on change processes in psychotherapy, what experiences of psychotherapy represented, or the therapeutic relationship. Studies used a range of techniques to ensure adherence to good practice in conducting qualitative research. Limited information was provided on the researchers’ background and how the researchers’ own biases may have impacted the analyses.
Experiences of Psychotherapy
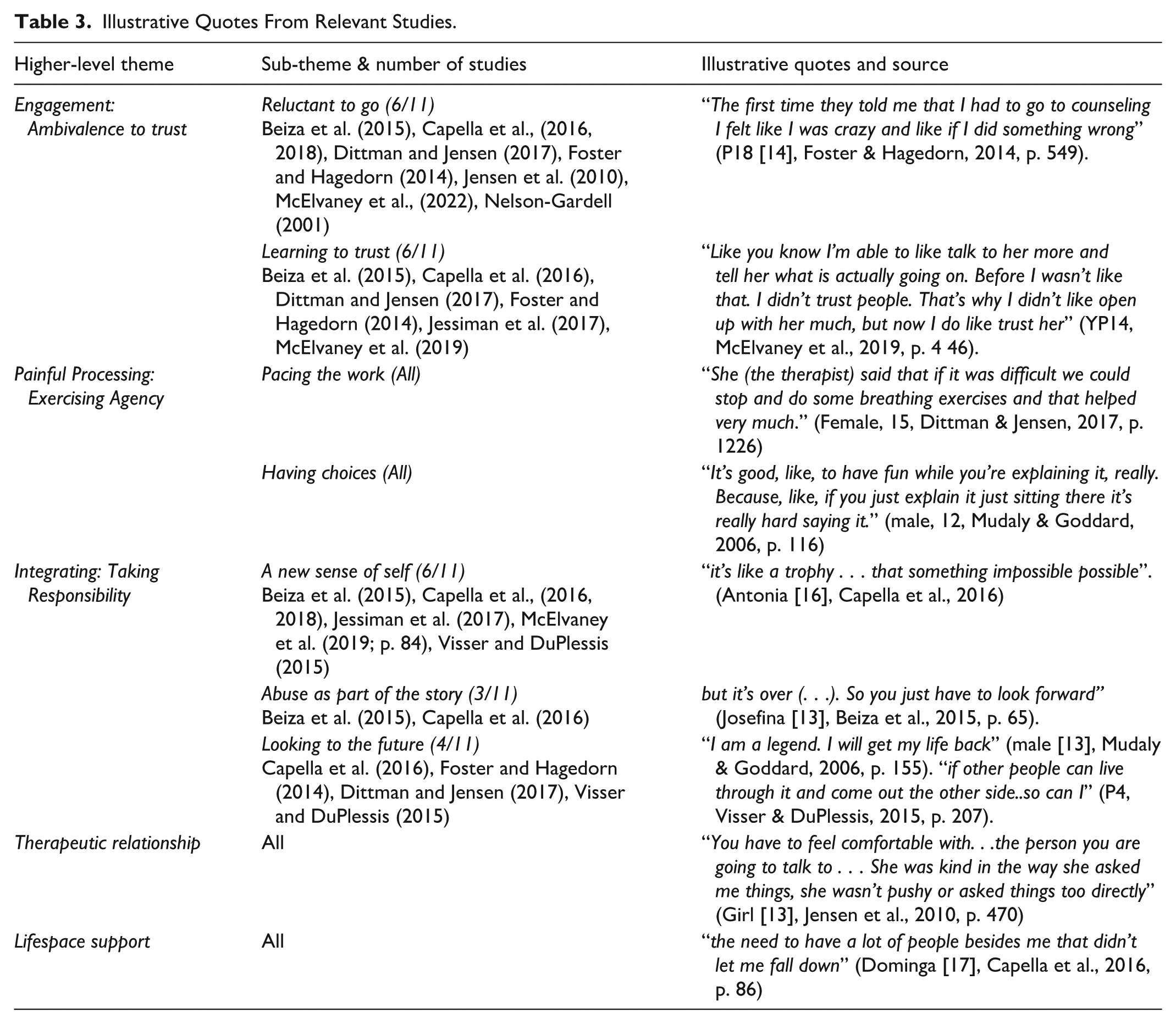
Three key themes were identified that depict the experience of psychotherapy, supported by two accompanying themes. The first theme, engagement: ambivalence to trust, is reflected in reluctance to attend therapy, and learning to trust, when young people have little knowledge of what to expect, how it will help, and have experienced something that they often do not wish to talk about. Painful processing: exercising agency is illustrated by the pacing of the therapeutic work and young people being given choice, thus supporting their agency. The third theme, integrating: taking responsibility, captures the experience of a new sense of self, putting the abuse in its place, and looking to the future, within the broader life story of the young person, acknowledging that the work of healing continues beyond the therapy and the therapeutic relationship. The therapeutic relationship and lifespace supports, such as family and friend networks, were experienced as central to the young person at all stages of the healing journey. Table 3 below presents illustrative quotes for each theme and sub-theme.
Illustrative Quotes From Relevant Studies.
Engagement: Ambivalence to Trust
Engaging in therapy was experienced by young people in these studies as challenging, illustrated by two interrelated sub-themes: avoidance, as seen in young people’s reluctance to attend, and overcoming ambivalence as they gradually learned to trust their therapist.
Reluctance to Attend
In six studies, young people spoke of being reluctant to attend or engage in therapy. A range of reasons were offered: nervousness, anxiety, feeling distrustful of the therapy or therapist, not knowing what therapy was about, and what to expect from therapy. The idea of talking to an unfamiliar person and not knowing if they would like their therapist contributed to their initial anxiety. For others, it was because they did not want to talk about what happened and feared that they would be pressurized into doing so. Some felt that being brought to therapy signified it was their fault. Others did not feel they needed it.
For some, this initial feeling of not needing therapy changed as they became more distressed and realized they needed help. The ambivalence experienced by some young people is illustrated by one participant in wanting and not wanting to come, I didn’t want to come here . . . there were times when I just didn’t want to talk about anything. But I wanted to be here because I felt safer and cared for and all that kind of thing (18 year old female, Mudaly & Goddard, 2001, p. 116).
Learning to Trust
For many of the young people in these studies, learning to trust the therapist resolved their ambivalence about attending. Trusting the therapist enabled the young person to open up and talk about things that they were unable to talk about elsewhere. This second sub-theme was identified in quotes from six studies and reflects young people’s gradual building up of trust in the therapist and other people over the course of therapy. The importance of the first visit and first impressions for the young person was highlighted by one young person’s experience: But I was just so, so scared . . . they introduced themselves and they were just so lovely, offered me tea and biscuits . . . (Counsellor) came out and introduced herself and she was so lovely. And I knew straight away that I was in like a safe place and that they were not going to judge me . . . So I think that first half an hour with her was really important for me to build my trust with her and let her know the type of person I was and let her get to know me and me to get to know her” (YP02,
2
female adolescent, McElvaney et al., 2019, p. 46).
In Jessiman et al.’s (2017) study, young people spoke of the confidential nature of the relationship and lack of pressure, facilitating this feeling of safety and trust in the therapist. This was particularly important for young people who spoke of previous experiences with child protection and law enforcement professionals where they felt their trust had been broken. In other studies, young people spoke of the importance of the therapist explaining how therapy works in order to build trust (Jensen et al., 2010; McElvaney et al., 2019). Being skilled and knowledgeable about sexual abuse and trauma reactions helped young people feel understood (Dittman & Jensen, 2017; McElvaney et al., 2019).
The challenge for young people whose trust has been breached so severely is captured well by Fernanda (15). She struggled to trust due to a constant change of therapists. Her advice to other young people was, “That they let themselves be helped . . . There are people who want to help you, but if you don’t know how to take advantage (of that help) you push them away” (Beiza et al., 2015, p. 67). Gaining the trust of young people was also influenced by parents and carers. In Jessiman et al.’s (2017) study, young people noted that if their carers trusted the therapist, the young people trusted them.
Painful Processing: Exercising Agency
Young people across all the studies spoke of two key aspects of processing their experiences of abuse that they found helpful in therapy: saying the words and managing the feelings. In both aspects of processing, they highlighted the importance of respecting their agency and autonomy through pacing the therapeutic work and giving them choices. In talking about the abuse, various metaphors captured the cathartic nature of the narrative expression of their experiences – “get something off my chest” (Capella et al., 2016), “get it all out” (Nelson-Gardell, 2001), “letting go of everything” (McElvaney et al., 2019). “It’s like a big weight off your shoulders” (Jessiman et al., 2017), “offloaded a lot of weight” (Visser & DuPlessis, 2015). Similarly, many young people spoke of the relief they felt as a result of being able to express their emotions in therapy (Nelson-Gardell, 2001; Visser & DuPlessis, 2015) and how therapy helped them to see it was not their fault (Jessiman et al., 2017). For others, being in a group where they knew others had been through a similar experience also helped young people talk about their experiences (Visser & DuPlessis, 2015). Talking about the abuse was valued but experienced as necessary: If that person had, for example, experienced the same thing as me, then I would have recommended that they found someone to talk to right away, because it helps so much. Because it is almost dangerous in a way to be by yourself and think . . . I used to cut myself and if I hadn’t found someone to talk to, I could have . . . cut myself again. (Female (15), Dittman & Jensen, 2017, p. 1227).
Young people in Mudaly and Goddard’s (2006) study acknowledged that they were helped to overcome the trauma by talking about it, but also noted that this was the hardest part of the work. They described it as emotionally distressing at the beginning, but felt less upset as they engaged in this process.
Pacing the Work
The pacing of therapy (Capella et al., 2016, 2018; McElvaney et al., 2019) was particularly important in facilitating the unfolding of the young person’s story. While some young people spoke of needing their therapist to push a little as they tended to avoid talking about their experiences, others spoke of the importance of not being pressurized to talk when they didn’t feel comfortable or didn’t want to talk about details of the abuse (McElvaney et al., 2019; Visser & DuPlessis, 2015). Young people spoke of feeling confident that the therapist would stop if they wanted a break or they felt upset (Jessiman et al., 2017; McElvaney et al., 2019).
Some dropped out of the therapy at this point and referred to not feeling heard when they expressed their desire not to speak about the trauma, It was the fact that I had to drag up the things that had happened and that I didn’t have time to think about it and that I felt pressured to talk about it when I didn’t feel ready. . . . And when I said “no” many times and that I couldn’t do it, she didn’t listen to me so at the end I had to say it to her. That was difficult for me. (Girl [17], Dittman & Jensen, 2017, p. 1226).
In several studies, young people referred to how the therapist helped them cope with this part of the work by offering reassurance, choice, and engaging in exercises to support emotion regulation. As another young person noted, “she wouldn’t hit me with difficult questions. She’d suggest something else if talking became difficult (age 15, Jessiman et al., 2017, p. 1030).
Having Choices
Young people valued being given a choice over what they talked about, what activities to engage in, whether to take a break from therapy, or change therapists if it was not working for them. “(Therapist) always said you’re here because you didn’t have a choice. So now it’s your choice what you want to talk about” (YP02, McElvaney et al., 2019, p. 42). Gaining control and exercising their agency was also evident in how young people spoke about becoming more aware of and managing their feelings better. Across the studies, young people described this as a reduction of symptoms such as headaches, sleeping difficulties, anxiety or depressive symptoms, intrusive thoughts, self-harming, and aggressive behavior, feeling better or happier, not thinking about the traumatic incident as much, and general improvement in well-being.
These changes were attributed by young people to speaking about the abuse and learning coping skills such as grounding techniques to cope with emotions, particularly anxiety, anger and aggression, “she’d say, put your feet on the floor, tap something and knock on your knee. You’re not there, you’re in a safe place, I know it’s you’ and that really really helps with it” (age 16, Jessiman et al., 2017, p. 1030). Young participants in Visser and DuPlessis’ (2015) study who had received a group intervention said that it made them feel stronger to realize there were others who had been through similar experiences and had managed to cope with their emotions. Young people spoke of the benefits of psychoeducation, for example, how they may have been groomed or manipulated as part of the abuse; for others, it was through the therapist challenging them when they spoke of feeling guilty about the abuse or the impact on their family. They spoke of feeling free to express themselves and of how they were able to be themselves, more authentic.
Integrating: Taking Responsibility
The third theme, integrating through taking responsibility, refers to feeling stronger and growing as a person, contextualizing the experience of sexual abuse into their wider lifespace and becoming more self-reliant as they looked to the future. Participants in the studies reviewed also spoke of feeling sad that therapy was finishing at the same time as feeling a sense of achievement, reflecting an ability to tolerate both the good and the bad of finishing therapy.
A New Sense of Self
In six studies, young people spoke of having a new sense of self-awareness and changes in their perception of themselves (Capella et al., 2016) and awareness of others, illustrated in references to experiencing themselves as stronger individuals, feeling a sense of achievement in being able to complete their therapy (Visser & DuPlessis, 2015) and learning a new way of being in the world. Young people described themselves as having increased reflective and problem-solving skills (Capella et al., 2018) and becoming more reliant on themselves, valuing themselves, and trusting in themselves with improved confidence and self-esteem (Beiza et al., 2015). Many young people highlighted how they felt they were better people. For some, this was facilitated through exercises designed to identify strengths and resources, and they were now being able to rely on these resources for the future. For others, this was explicitly offered through the therapist explaining why they might be feeling anxious, how the legal system works, or how counseling might help the young person,
One young person described how they discovered a strength within themselves they didn’t know they had, It made me realise things about myself..I didn’t realise how strong I was until I came here to this group. It made me proud of myself that I can still stand on my own two feet after everything I have been through (P4, Visser & DuPlessis, 2015, p. 207).
Abuse as part of the story
In three studies, participants spoke of acknowledging that while they remembered the abuse, the memories were less emotionally intense and hurt less, becoming less and less present in everyday memories, that while abuse cannot be forgotten, life can go on with new life plans and goals. It was not central to their lives, even though it was an important part of their story.
Some young people described moving beyond an identity as a victim “that you can be what you are and not what happened to you” (Dominga [17], Capella et al., 2016, p. 82).
The healing journey was seen by some young people as continuing, acknowledging that psychotherapy is part of the healing journey, but the journey continues, as they rely on their own resources, The psychologist is a support, because that (experience) is something that will always be there and everyone has to resolve it..that’s something that I will have forever . . . it’s something that won’t be forgotten and you have to learn to live with it (Karen [18], Capella et al., 2016).
Looking to the Future
Young people spoke of hopes for the future, wanting to pursue a career that involves helping others, “I want to be a psychologist like here, as if, as if I were working here (in the center) . . . that’s my vision of the future” (Capella et al., 2016, p. 80). Others spoke of having a positive outlook, It’s like I left that stage of my life in the past, now I understand that it’s gone, that I can’t erase it, but I can live with it . . . I don’t look back anymore, I don’t focus on the past, I pay attention to my present and my future. (Patricia, 16-year-old female, Capella et al., p. 30).
The ability to speak about the abuse now, after therapy had ended, signified for them their ability to overcome the experience. “I think professionals telling their clients that they will come out of it, that eventually, there is a light at the end of the tunnel. That would help younger people knowing that and could prevent like suicides” (YP07, McElvaney et al., 2019, p. 48). Looking to the future also meant relying on one’s own resources. Mariela noted, “What comes now depends on me. I can’t do anything with my past, but I can with my future” (p. 66, Beiza et al., 2015).
The Therapeutic Relationship
The fourth theme highlighted the importance of the therapeutic relationship as supporting the therapeutic work. Often, young people referred to the personal qualities of the therapist when describing how they built up a relationship. Young people used words like “nice” and “kind” to describe their therapist (Jensen et al., 2010; Jessiman et al., 2017). Experiences of the counselor/therapist included feeling listened to, supported, being believed, and feeling understood. In the group context, the relationship was not just with the therapist but also with other group members, feeling that others cared about them and about what had happened to them (Visser & DuPlessis, 2015). The gradual building of trust was facilitated by a feeling that the therapist understood them and believed that what they said was important (Nelson-Gardell, 2001).
Young people also referred to the specialist nature of the service as helping them trust the therapist (McElvaney et al., 2019; Visser & DuPlesser, 2015), I think the fact that it is a rape crisis, sexual abuse centre, because it feels like I actually am going and getting help for what I need. Like if you’ve a problem with your eyes and you’re going to your GP . . . if you’ve a problem with your eyes, you go to an eye doctor (YP13, McElvaney et al., 2019, p. 46).
Supportive Lifespace
Young people in all of the studies reviewed spoke of the reciprocal relationship between their lifespace and their experience in therapy. Support from parents and friends was seen as an important aspect of the healing journey, but therapy also helped them develop these relationships. Several young people referred to the importance of providing support for family members and carers. Young people spoke of environmental supports such as staff from the residential care center where they lived (Beiza et al., 2015). One young person spoke of how being in a care setting away from her family enabled her to recover, while another noted that being away from her family hampered her recovery. Young people also attributed change to other areas of their lives, such as parents getting help or support from friends, the importance of being able to have fun with their peer group, which helped them forget about the abuse for a time, thus reducing its presence in their everyday lives. One participant spoke of how getting a dog helped her when she was feeling sad (Capella et al., 2018). Several young people, across studies, spoke of how therapy helped them understand others better, particularly parents, leading to improvements in relationships with family and friends (Jensen et al., 2010; McElvaney et al., 2019; Visser & DuPlessis, 2015). They said the group helped them to “treat people better and to start talking about my emotions . . . to have a better relationship with my mother” (P1, Visser & DuPlessis, 2015, p. 208). “and believe in myself so when I see other people I can smile and say hello, rather than staying alone and locked up in my room” (P5, Visser & DuPlessis, 2015, p. 208).
Discussion
The 11 papers reviewed here draw on young people’s experiences of therapy across four continents, conducted in various contexts. Most young people were attending specialist sexual abuse/sexual assault services or programs specifically targeted at young people who had experienced childhood abuse. Theoretical orientation, where information was available, varied, as did the duration of therapy. Nevertheless, there was a remarkable similarity in themes identified. Notwithstanding differences in methodologies, foci of interviews or focus groups, and different cultural contexts, core themes were identified that capture young people’s experiences of the process of therapy following sexual abuse, involving engaging, processing, and integrating, supported by the therapeutic relationship and the life space of the young person.
Reluctance to Attend
The tendency for young people to feel reluctant to attend was prominent; this is not unique to young people who have experienced sexual abuse (see reviews by Gulliver et al., 2010; Radez et al., 2021). Gilmartin et al. (2022) refer to the double stigma for young people in state care, of being in care and needing to attend therapy. For adolescents, this reluctance may be compounded by the need to be self-reliant (Gulliver et al., 2010). For those who have experienced sexual abuse, past experience of having been silenced and silencing themselves, compounded by self-blame, guilt, and shame (McElvaney, 2015; McElvaney et al., 2021), are likely to be contributing factors to the reluctance to speak to a stranger about these intimate and embarrassing experiences. Potential ways of motivating young people to engage in therapy can be found in what young people said about what they found helpful in their therapy, such as providing explanations as to how therapy works and sharing information about sexual abuse and its impact. Jensen et al. (2010) note how therapy is a novel situation and children and young people don’t know what to expect. For young people in these studies, learning to trust their therapist appears to have been an important factor in helping them engage in therapy and sustain their attendance. Psychoeducation about how therapy works appears to have contributed to epistemic trust in this study, an important component of the therapeutic relationship linked to therapeutic change (Fonagy & Allison, 2014). Learning to trust the therapist also paid dividends for young people in their relationships with peers and carers. Positive experiences of therapy, such as feeling understood, not judged, and feeling heard, may contribute to trust building in general for young people (Anwar Jaffrani et al., 2020).
The Therapeutic Relationship
A common theme across all studies was the importance of the therapeutic relationship, in helping the young person feel cared about, in establishing trust, in facilitating painful conversations about the experience of abuse, in expressing and managing distressing feelings, learning coping skills and gaining a sense of hope for the future The therapeutic relationship has received considerable attention in adult psychotherapy research; less attention has been paid to this as a central component of work with children and adolescents (Midgley et al., 2017; Núñez et al., 2022). Núñez and colleagues suggest that while Bordin’s (1979) three components of the working alliance – agreement on goals, collaboration on tasks, and bond between the therapist and client, have been found to be associated with positive outcomes in the adult psychotherapy literature, from children and adolescents’ perspective, the bond or real relationship between the young person (feeling connected) and therapist may take precedence, particularly in the early stages of therapy. Across the studies reviewed, young people described the characteristics of the therapist – as a nice person, as someone they could trust, and as someone they felt comfortable with and felt understood. It may be that Rogers’ (1957) original model of the three core conditions of therapy – congruence, empathy, and unconditional positive regard – is more relevant to how we conceptualize the therapeutic relationship for children and young people. In adult psychotherapy studies, these core conditions have been found to foster trust and emotional safety and are associated with positive therapeutic outcomes (Farber et al., 2018; Kolden et al., 2018; Watson et al., 2014). When asked about what they found helpful from professionals in their recovery from the impact of sexual abuse, adolescents in Schönbucher et al.’s (2014) study identified empathy as an important supportive behavior. According to Jensen et al. (2010), when the therapist appears friendly, supportive, and receptive, this helps the child engage in the therapeutic tasks.
Processing the Abuse Experience
The findings relating to how young people process their experiences in therapy, what helps them feel better, both in terms of psychopathology – low mood, anxiety – but also feeling good about themselves, offer guidance for the field. Young people noted that while it was painful and challenging, it was important to speak about their experience of abuse and allow themselves to experience painful feelings. Learning to cope with difficult emotions, psychoeducation, improved awareness of self and others, understanding relationships better, and feeling stronger in themselves were identified as what they found helpful. They spoke of having their agency and autonomy supported through offering choices that led to improvements in their well-being and sense of self. These findings are aligned with Lavik et al.’s (2018) findings about what adolescents want from therapy – improved emotion regulation, self-awareness, and social connectedness. They are also core components of trauma-focused approaches in therapy (Carpenter et al., 2016; Deblinger et al., 2015; Foroughe, 2023; Paivio & Pascual Leone, 2010), but are clearly core to therapeutic work regardless of theoretical orientation, as many of the studies reviewed worked to general principles (e.g., SENAME, 2014, cited in Beiza et al., 2015, p. 64). The support of parents, other adults, peers, and engagement in other activities outside of therapy supported the therapeutic work for many of the young people interviewed in these studies.
It is noteworthy that young people found it helpful, although challenging, to talk about the experience of abuse. Nelson-Gardell (2001) suggested that talking about the abuse may be “the core of the therapeutic experience” (p. 412), while Beiza et al. (2015) described it as a turning point in the therapeutic work. However, young people also emphasized the importance of not feeling pressurized to talk about the details; for some, this resulted in them terminating the therapy. Jensen et al. (2010) note the importance of the therapists’ sensitivity and timing for the young people in their study. Finding a balance between encouraging the young person to confront this difficult task and respecting their autonomy and agency in when and what they talk about is challenging for therapists and can only be realized through good attunement between the therapist and client, coupled with a willingness on the part of the therapist to push the client outside their comfort zone – something that young people identified as helpful. This resonates with recommendations from other reviews that therapy needs to be tailored to the individual child and family (Narang et al., 2019), as each young person will need different supports and challenges at different moments in their therapeutic journey.
Continuing the Healing Journey Beyond Therapy
Young people in this study acknowledged that their therapeutic engagement was part of their journey to healing and not the outcome of this journey. They spoke of feeling changed and feeling stronger as a person, discovering their resilience, trusting in themselves, and nurturing hope for the future so that they could live the lives they wanted to live.
They described integrating the abuse experience into their wider life story, supported by both the therapeutic relationship and support from others such as friends and family. Capella et al. (2016) noted that in their study, one key difference between younger children and adolescents was that the children believed that healing was achieved on completion of therapy, while adolescents saw their healing as an ongoing process that continued beyond the experience of therapy, underscoring the importance of attending to adolescents as a unique group. Supporting the developing autonomy of the adolescent is thus a key task of the adolescent psychotherapist (Starrs, 2019). In Lavik et al.’s (2018) study, positive outcomes in therapy were conceptualized by young people as achieving a sense of stronger autonomy and safer identity. Young people’s ability to articulate these reflections in the studies reviewed illustrates the resilience and healing capacity, acceptance of both their hurt and their ability to move beyond the experience, “put it in its place,” and hope for the future. Stories of feeling a better person, optimism for the future and ambitions also reflect the posttraumatic growth many adult survivors of childhood trauma have described (Joseph, 2013). The concept of growth through adversity is amply reflected in young people’s stories in this review.
Strengths and Limitations
The key strength of this review is its focus on the direct narratives of adolescents – a developmental phase distinct from that of childhood and young adulthood. To our knowledge, it is the only review to capture the voices of at least 72 adolescents. The findings are limited by the methods and contexts of the studies themselves. Limited diversity was evident with respect to gender, sexual orientation, and familial context. Studies relied predominantly on verbal narratives. Capella and Boddy (2021) have highlighted what can be communicated in silences and the need for the researcher to attend to what is unsaid in the research interview. While limited information was provided on the context in which these studies were conducted, it appears that only one study specifically focused on a marginalized group – young people in residential care (Beiza et al., 2015), a group identified as experiencing double stigma from being identified as “needing therapy” and being in state care (Gilmartin et al., 2022).
Most of the studies reviewed focus on positive experiences of psychotherapy. It may be that young people who had positive experiences were disproportionately more likely to be invited to participate, they were more likely to volunteer for participation, or were reluctant to be critical of their therapist. Studies focusing on more challenging experiences tend to set out to directly explore such experiences, for example, studies on dropout from psychotherapy (O’Keeffe et al., 2020).
Implications for Practice, Policy, and Research
The implications for practitioners include the importance of attending to the therapeutic relationship, both in helping young people engage in the initial phases of therapy and supporting their sustained engagement. Addressing wider lifespace supports, such as relationships with parents/carers and peers, can support the therapeutic work and also contribute to improvement in these relationships. A range of strategies are helpful in supporting young people to process their experience, including psychoeducation, emotion regulation techniques, and encouraging the young person to speak about the experience of abuse. Viewing therapy as only part of the healing journey may be important for therapists in managing their expectations of what can be achieved in therapy and in focusing on the future and how the young person can continue the healing work themselves, with support from their wider lifespace (Table 4).
Implications of Findings.
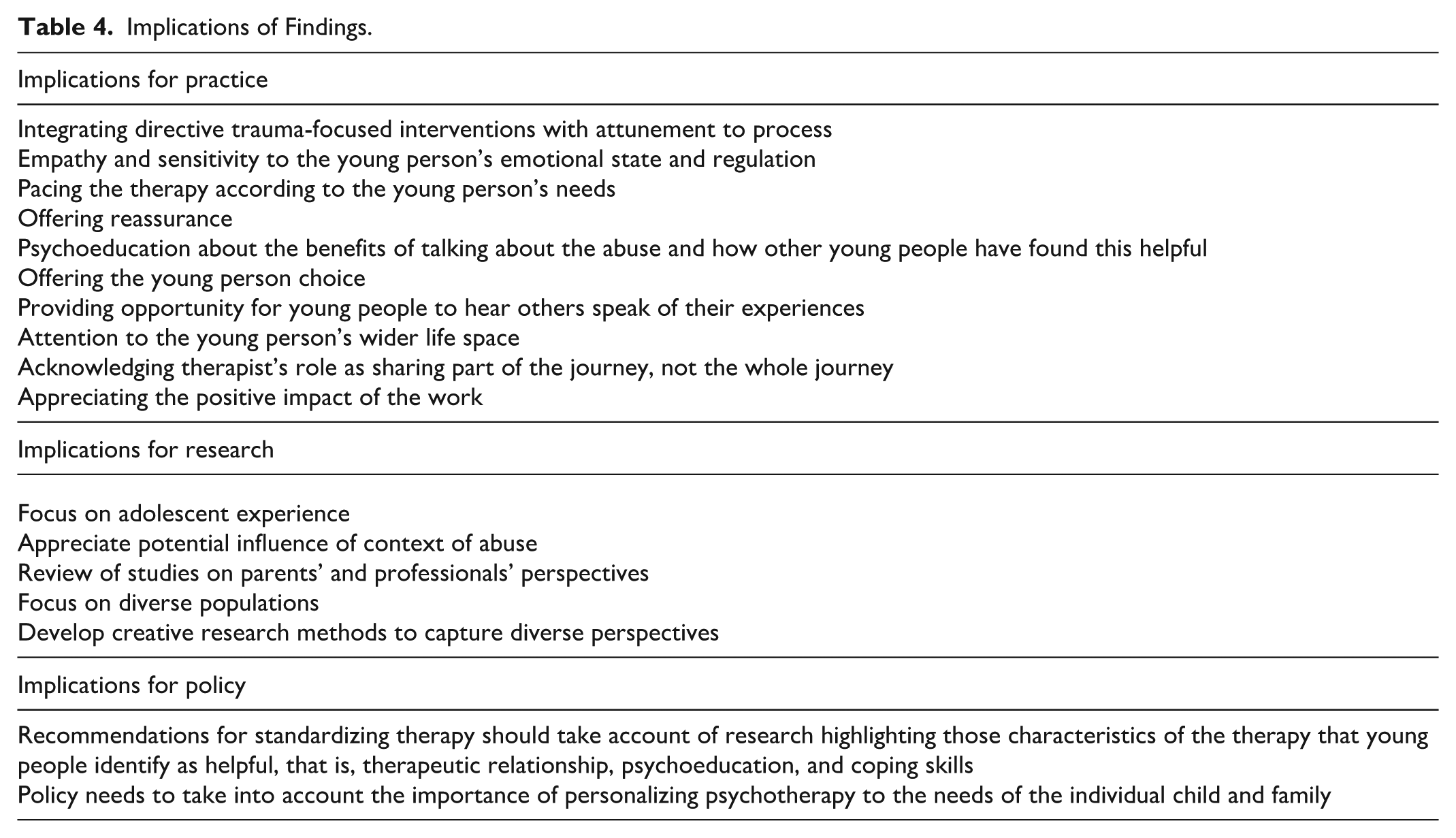
Few studies reviewed referred to the existence of national or international policies informing therapeutic work in this field. Guidelines from WHO (2017) recommend TF-CBT for children and adolescents experiencing PTSD or PTSD symptoms, despite describing the quality of evidence as “very low” (p. 5). Rather than focusing on specific modalities, which the research evidence does not support, policy in this field needs to take into account how therapy is being conducted in real-life settings and how young people are experiencing therapy. In the three Chilean studies, the statutory services were guided by principles such as therapy being part of an interdisciplinary intervention, having the goal of strengthening family resources, protecting the child, and helping the child make meaning of their experience of abuse (Servicio Nacional de Menores, 2012). Focusing on principles, informed by what young people say about their experiences in therapy, rather than policy recommendations for specific therapeutic approaches, appears to be more aligned with the research on children’s and adolescents’ experiences of what they find helpful in therapy.
Demographic information on samples participating in research studies was sparse. Including such information in studies would enable a better understanding of how different contexts of the abuse experience (e.g., peer to peer vs. adult child, online vs. in person, intrafamilial vs. extrafamilial) and different contexts of service provision influence the psychotherapy experience through childhood and adolescence. Studies of parents/carers and professionals’ views and other supportive individuals (e.g., peers, teachers, sports coaches) would be helpful in understanding the challenges they experience and how they support young people on this journey. Cultural differences have been highlighted with respect to CSA prevalence rates (Stoltenborgh et al., 2011), barriers to disclosure (Fontes & Plummer, 2010), and coping following sexual abuse (Tao, 2024). More studies focusing on cultural influences on the recovery process are needed to inform culturally responsive psychotherapy. Finally, the studies reviewed relied predominantly on verbal narratives. Researchers need to consider more creative methods of eliciting young people’s views about their experiences.
Conclusion
To the authors’ knowledge, this is the first review to be conducted of qualitative studies of adolescents’ experiences of therapy following sexual abuse. As adolescents in these studies looked to the future, their growing agency and autonomy were evident. Young people spoke of how adapting the therapeutic work to their needs through pacing, offering choice and supporting their growing independence, was particularly helpful. Sensitivity and attunement to the developmental needs of adolescents empower them to trust in their own ability to confront difficult experiences in therapy, while challenging them to move outside of their comfort zone and respecting their ability to cope.
Recent guidelines on psychotherapy with children and young people emphasize the need for a tailored approach to therapy and personalizing psychotherapy (Narang et al., 2019), acknowledging the idiosyncratic manner in which children respond to the experience of sexual abuse. This review captures the breadth and depth of individuals’ experiences, thus informing the many unique ways that young people can be supported following experiences of sexual abuse, meeting each young person as a unique individual who needs a unique response to assist them on their recovery journey.
Footnotes
Acknowledgements
The authors wish to acknowledge the assistance of Lauren Maguire, School of Psychology, Dublin City University, who assisted with data analysis.
Ethical Considerations
No ethical approval was required for this review as it relied on secondary data available in published studies.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Children’s Health Ireland assisted with funding for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available through published works.