
Abstract
Disabled women experience disproportionately high rates of gender-based violence (GBV), yet their unique experiences remain understudied. This qualitative meta-synthesis examined the lived experiences of disabled women who have encountered GBV. Following a structured review process, 49 qualitative studies met the inclusion criteria, focusing on disabled women’s first-hand accounts of GBV. Studies were identified through a comprehensive search of multiple academic databases using predefined search terms and selection criteria. The findings revealed several intersecting challenges that disabled women faced when experiencing and navigating GBV. Systemic neglect and institutional harm were identified as significant barriers, as women encountered structural failures that limited their ability to seek safety, protection, and justice. Many survivors described experiences of revictimization, in which inadequate institutional support and mistreatment by service providers perpetuated ongoing cycles of violence. Dehumanization and oppression were also central to survivors’ narratives, with ableism, infantilization, and intersecting forms of marginalization shaping their experiences of violence. Despite these challenges, disabled women demonstrated resilience and resistance by employing various survival strategies and advocating for themselves and others within systems that frequently failed to protect them. These findings underscore the urgent need for intersectional, disability-inclusive GBV policies, improved access to services, and survivor-led approaches to intervention to ensure that disabled women can seek support without fear of further marginalization.
Introduction
Gender-based violence is a widespread global issue that demands further attention. Globally, an estimated 736 million women have experienced physical or sexual violence by an intimate partner or non-partner at some point in their lives (World Health Organization [WHO], 2024). Gender-based violence encompasses various forms of violence, including emotional, sexual, physical, psychological, and financial abuse (Savage, 2021). Although this violence affects women of all backgrounds, women with disabilities face additional barriers at the individual, relational, community, and societal levels that impede their ability to seek help and find safety (D’Costa, 2025). Despite these heightened vulnerabilities, the literature has underexamined the distinct and often overlooked realities faced by women with disabilities who have experienced violence.
Disabled Women’s Experiences of Gender-Based Violence
Research has consistently shown that disabled women experience gender-based violence at significantly higher rates than non-disabled women. They are also more likely to experience abuse from more than one intimate partner over their lifetime (Savage, 2021). Studies have demonstrated that disabled women experience unique forms of abuse compared to non-disabled women (Shah et al., 2016). These forms of abuse include withholding medications, disability equipment, and mobility aids, as well as positioning women in physically uncomfortable or precarious positions (Olkin et al., 2019). When facing gender-based violence, defined as violence rooted in power inequities linked to gender, gender identity or expression, or perceived gender (Wirtz et al., 2020), disabled women who have sought help often encountered limited assistance. In some cases, these responses resulted in serious consequences, including the apprehension of children or the worsening of abusive behaviors (Walter et al., 2024). Ruiz-Pérez et al. (2018) noted that abusive partners often exploited women’s disabilities to cause further harm, increasing their isolation and dependence on the abusive partner.
Beyond these overt forms of violence, disabled women also faced subtle forms of discrimination that were pervasive and negatively affected their mental health and overall well-being. Kattari (2020) described ableism as a system that values certain abilities over others and operates through discriminatory behavioral, cultural, and structural norms that harm disabled people. These harms have often manifested as ableist microaggressions, which are subtle interactions that reinforce stereotypes and inequality, including infantilization, where others treat women as childlike or assume they need caretakers (Olkin et al., 2019). Research has shown that the intensity of this discrimination varies depending on the visibility and type of disability (Hamby et al., 2023). Social stigma reinforces these harms by isolating disabled people and subjecting them to derogatory treatment and humiliation (Meer & Combrinck, 2015). D’Costa (2025) identified significant gaps in research representation, noting that many studies focused predominantly on White, heterosexual women, leaving disabled women with multiple marginalized identities largely invisible.
Disabled women situated in marginalized communities have experienced higher rates of gender-based violence and more severe impacts of abuse, including invisibility, limited access to targeted support, and reduced legal protection (Statistics Canada, 2020). These experiences reflect women’s navigation of multiple, interconnected systems of oppression (Wright & Manuel, 2025). Accordingly, the risks and lived experiences of gender-based violence among disabled women vary across populations. Intersectional factors, including age, race, immigration status, type of disability, and sexual orientation, shape women’s vulnerability to violence and access to support (Collins, 2019; Cotter & Savage, 2019; Crenshaw, 1991).
Although scholars have described gender-based violence among disabled women as globally endemic (McConnell & Phelan, 2022), qualitative research situating women’s lived experiences within the intersecting contexts of violence and disability has remained limited. While the literature has grown, limitations in scope, intersectional analysis, and representation have continued to marginalize disabled women’s experiences in both research and practice (Dowse et al., 2016). D’Costa (2025) and Walter et al. (2024) found that many disabled women avoid engaging with organizations due to persistent accessibility barriers. As a result, first-hand survivor perspectives, often referred to as first-voice experiences, have remained largely absent from the development of community-based interventions, social responses, and policy initiatives. This absence is closely linked to the structural barriers disabled women encounter when attempting to leave relationships, including restrictive policies regarding service animals, the absence of assistive technology, and restrictions on children within shelter spaces (Alhusen et al., 2020). Consequently, organizations that support women with disabilities experiencing gender-based violence increasingly seek survivor-informed evidence to better understand the issues facing this population.
The Current Study
Centering survivors’ voices is essential for creating inclusive, accessible, and barrier-free support systems. In response to these gaps, this qualitative meta-synthesis aimed to synthesize existing research to deepen understanding of the lived experiences of gender-based violence among disabled women, many of whom also occupy multiple marginalized social locations (e.g., women of color, women living in poverty, and sexual and gender minority women). This study addressed the following research question: How do disabled women experience gender-based violence, and what are their formal and informal needs? In this paper, we used both person- first and identity-first language when discussing disability, recognizing the evolving nature of disability-related terminology and the lack of consensus regarding the most affirming language (Kattari, 2020). By integrating both approaches, we aimed to respect the diverse viewpoints within disabled communities (American Psychological Association, 2015). We conceptualized disability as a personal, social, cultural, and political identity (Dupré, 2012) and as a continuum of human variation in which individuals have unique voices and complex experiences (Rocco, 2005). Hence, the term disability encompasses developmental and physical impairments, neurodiversity, chronic illness, chronic pain, and mental illness, among others.
Methods
We conducted this qualitative meta-synthesis to explore and synthesize the lived experiences of disabled women who had experienced gender-based violence. Unlike quantitative research, which often focuses on statistical trends, qualitative meta-synthesis provides deeper insight into first-voice survivor experiences by integrating qualitative findings across multiple studies. In this review, we treated participant quotations reported in the included studies, rather than authors’ interpretations or summaries, as the primary analytic material. We engaged in an interpretive analysis of these quoted accounts. This approach allowed us to re-examine survivor voices across diverse contexts and study designs and to synthesize nuanced accounts of disabled women’s experiences of gender-based violence that may not be readily accessible through other research methods.
We followed a published meta-synthesis protocol previously developed (Goulden et al., 2023), in collaboration with a community group and a service provider working within local gender-based violence response systems. This collaboration ensured relevance and alignment with the lived experiences of disabled women. We used the PRISMA 2020 framework to guide transparent reporting of the systematic search, screening, and selection processes. Our methods included database and gray literature searches, dual screening, and quality appraisal using the Critical Appraisal Skills Programme (CASP) checklist.
We conducted the analysis using a thematic synthesis approach (Dixon-Woods, 2011; Douma et al., 2021). We extracted participant quotations verbatim from the included studies and treated them as secondary qualitative data. We familiarized ourselves with the data, developed a thematic framework, indexed and charted findings, and mapped and interpreted key themes. Quotations are presented in the findings section to illustrate cross-study themes and survivor perspectives.
Search Strategy
An academic librarian (KR) designed the search strategy in consultation with other team members. The search strategy included text words and controlled vocabulary terms aligned with the SPIDER eligibility criteria (Cooke et al., 2012), specifically the sample (women and nonbinary people with disabilities), the phenomenon of interest (gender-based violence), and the study designs of interest (qualitative literature). We adapted portions of the search strategy from published knowledge syntheses on disability (Irvin et al., 2023; Small et al., 2022) and gender-based violence (Farmer et al., 2023).
We searched the following academic databases on April 4, 2023: MEDLINE (Ovid), APA PsycINFO (EBSCO), Criminal Justice Abstracts (EBSCO), Social Work Abstracts (EBSCO), Sociological Abstracts (ProQuest), Social Services Abstracts (ProQuest), SocINDEX (EBSCO), International Bibliography of the Social Sciences (ProQuest), Applied Social Sciences Index and Abstracts (ProQuest), Women’s Studies International (EBSCO), LGBTQ+ Source (EBSCO), and Scopus (Elsevier). No date or language limits were applied. Supplemental Appendix B includes the full search strategy. Additionally, we conducted a hand search of the Canadian Journal of Disability Studies because it is not indexed in the databases we searched. No additional studies were added to the sample from the hand search. To identify gray literature, we searched ProQuest Dissertations and Theses Global, Google, and Google Scholar and screened the first 50 results from each search. We also searched the Community Health Online Digital Archive and Research Resource and the Global Database on Violence Against Women. These searches did not identify additional studies. Due to time and resource constraints, we did not conduct citation searching.
Study Inclusion
To be eligible for inclusion in this review, studies needed to report primary qualitative research involving data collection through interviews or focus groups with disabled women who had experienced gender-based violence. We included studies with mixed samples of disabled and non-disabled participants only when authors clearly identified findings specific to disabled women. Given the emphasis on disability, we excluded studies that focused exclusively on mental health disabilities because prior systematic reviews had already examined the intersection of mental health and gender-based violence in depth (Golding, 1999; Sparrow et al., 2017). Following previous reviews (e.g., Campbell et al., 2022), we also excluded studies focused on HIV to maintain emphasis on disabilities disproportionately experienced by women.
We included mixed-methods studies only when they contained sufficient qualitative data to contribute meaningfully to the synthesis. We excluded studies that did not involve direct data collection with survivors (e.g., discourse analysis of secondary data). Eligible studies included broad definitions of gender-based violence, which encompassed physical, sexual, emotional, psychological, or structural violence, as well as intimate partner violence, neglect, and harassment. We imposed no restrictions on publication year to ensure a comprehensive synthesis of available research. Due to resource constraints, we included only studies published in English. We summarized inclusion and exclusion criteria in Supplemental Appendix A.
We imported all database search results into Covidence systematic review software (Covidence, 2023), which identified and removed 3,000 duplicates. Two independent reviewers then screened the remaining 4,045 studies at the title and abstract level and excluded 3,913 studies that did not meet inclusion criteria. Reviewers conducted full-text screening on 132 studies, and a third reviewer resolved disagreements. After full-text screening, 49 studies met eligibility criteria and were included in the final synthesis. We outlined the screening and selection process in the PRISMA flow diagram (Figure 1).
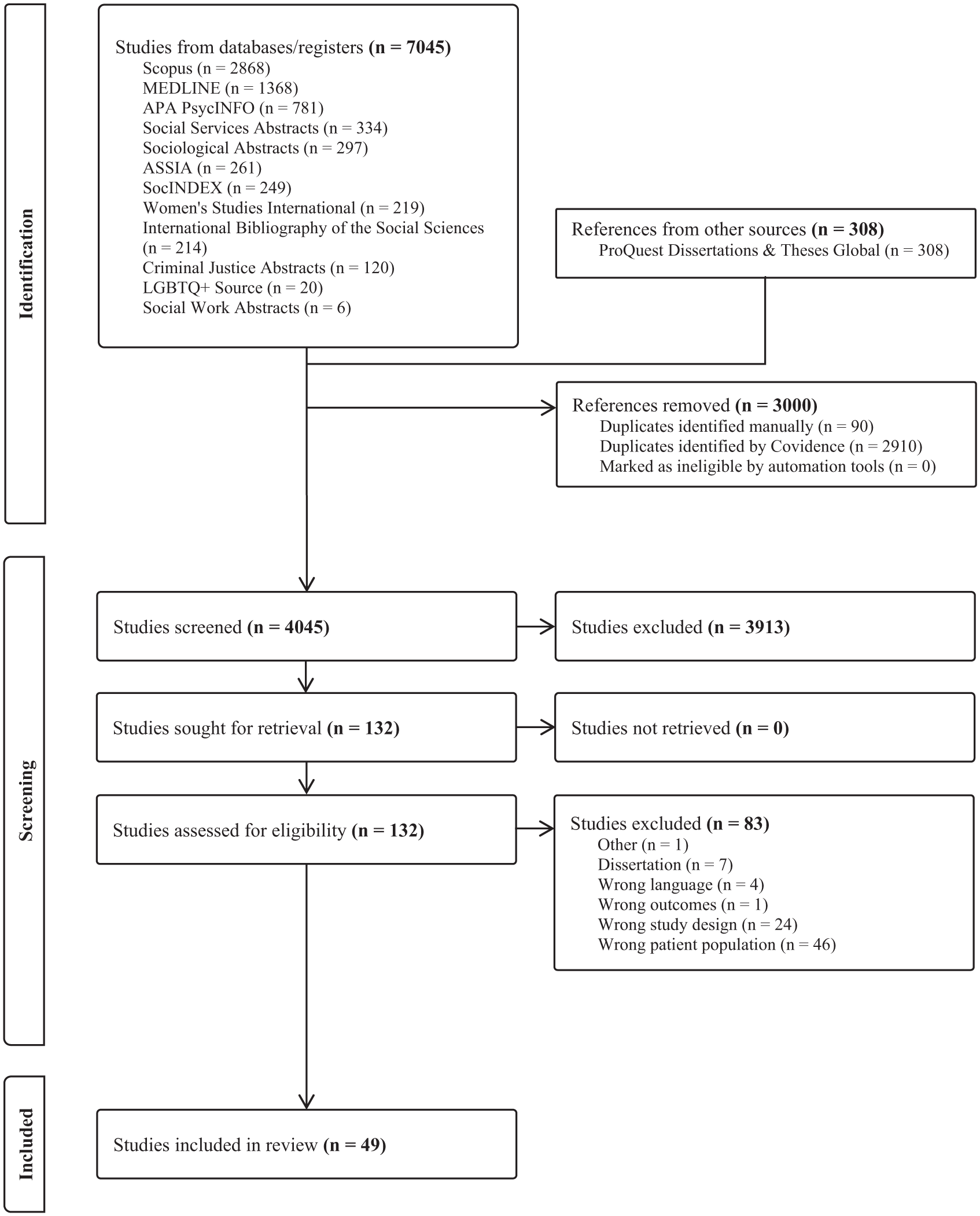
PRISMA flow diagram.
Quality Appraisal
As illustrated in the summarized quality appraisal diagram (Figure 2), we assessed all included studies using the Critical Appraisal Skills Programme (CASP) qualitative checklist (CASP, 2018). Two independent reviewers completed the appraisal, and a third reviewer resolved disagreements to reach consensus. Rather than excluding studies, we used the CASP checklist to identify methodological strengths and potential limitations. Limited reflexivity was identified as the most common issue, as several studies lacked sufficient detail regarding the relationship between researchers and participants. Other areas with reduced methodological clarity included study rigor, ethical considerations, and participant recruitment. We have provided a full summary of the quality appraisal results in Supplemental Appendix D.
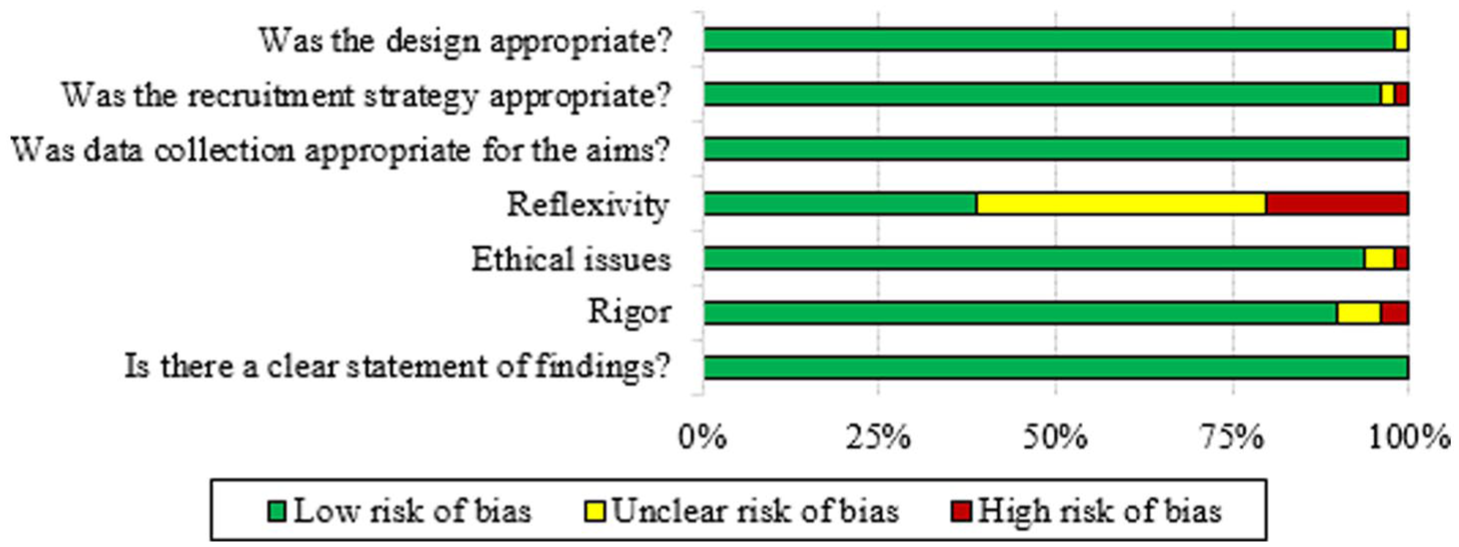
CASP quality appraisal diagram.
Data Synthesis
We followed the five-stage thematic synthesis approach outlined by Dixon-Woods (2011) and adapted by Douma et al. (2021). This structured method supported in-depth interpretation across studies.
Stage 1: Familiarization With the Data
During the first stage, our team reviewed each study to identify key themes and patterns. The lead author (AG) distributed studies among team members, who extracted data using Covidence systematic review software (Covidence, 2023) and recorded findings in a pre-designed data extraction form. We extracted data into Excel for further review. Our team members conducted multiple readings of each study to ensure deep engagement with the data. We met regularly to discuss initial observations and identify recurring patterns.
Stage 2: Identifying the Thematic Framework
In the second stage, our team developed an initial coding framework to categorize identified themes. The lead authors (AG, SLB) refined this framework iteratively through consultation with our team as new insights were identified.
Stage 3: Indexing
During the third stage, we applied the coding framework across all extracted data. We coded and categorized each study to ensure that the analysis captured all relevant themes across diverse methodological approaches. Our team treated indexing as a dynamic and iterative process, engaging in ongoing revisions and discussions to maintain conceptual clarity and consistency.
Stage 4: Charting
In the fourth stage, our team organized themes and sub-themes into analytic tables to facilitate cross-study comparison. This process supported a nuanced understanding of how gender-based violence manifested in the lives of disabled women. We developed two organizational tables: the Study Details Table (documenting study focus, location, sample size, type of disability, and type of violence) and the Study Methods and Findings Table (summarizing study methodology, data collection methods, and key findings). Both tables are included in Supplemental Appendix C.
Stage 5: Mapping and Interpretation
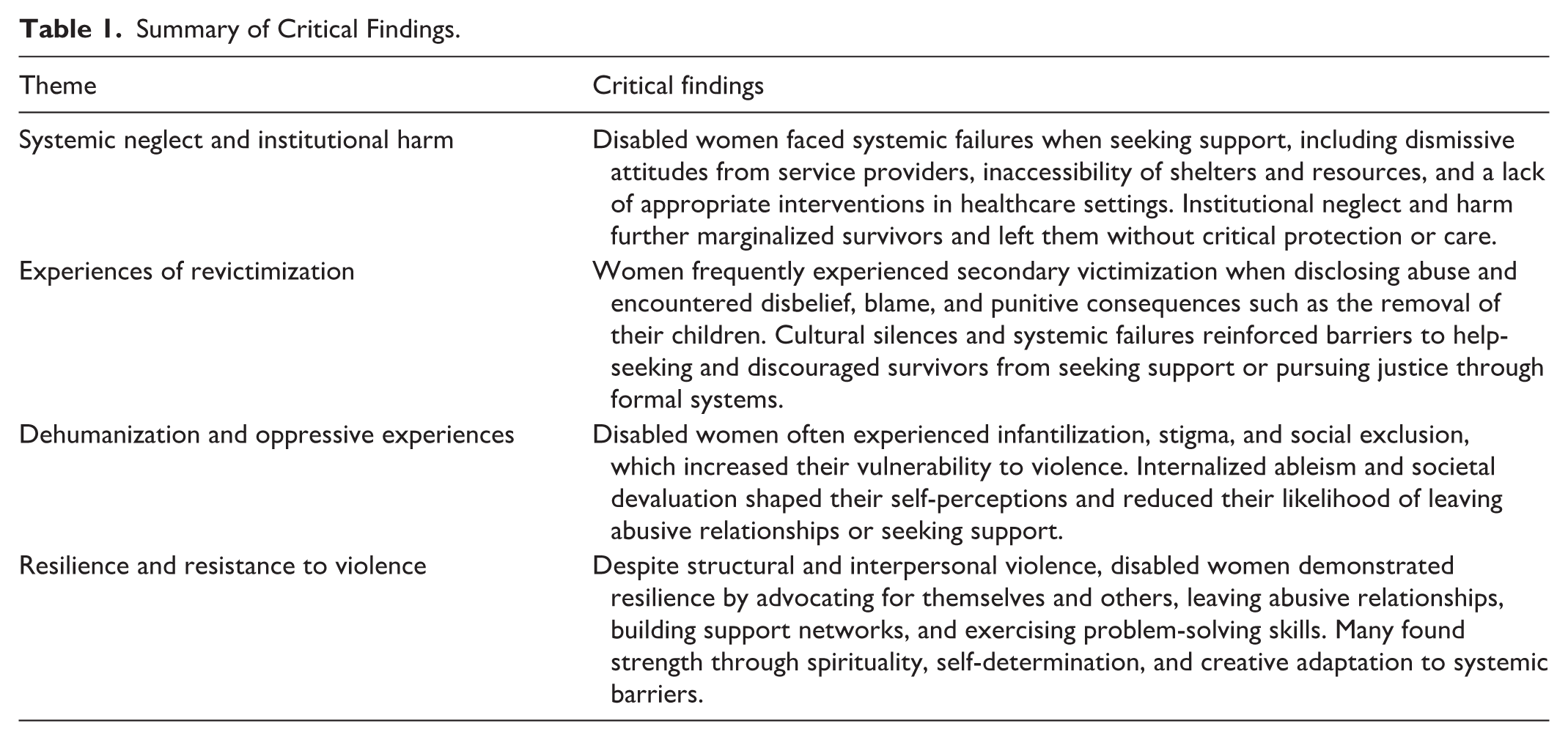
In the final stage, our team explored relationships among themes, sub-themes, and study contexts through repeated discussion. This stage supported a critical synthesis of disabled women’s experiences of gender-based violence. We developed a final Summary of Critical Findings table to present key themes and insights (see Table 1).
Summary of Critical Findings.
Researcher Positionality and Reflexivity
Our team consisted of four social workers with extensive practice experience supporting survivors of gender-based violence. Three team members currently hold academic positions, and two are doctoral students. Several team members self-identify as disabled or living with disabilities, bringing embodied knowledge of accessibility barriers, systemic exclusion, and the complexities of navigating care and support systems. We embedded reflexivity throughout the analytic process. Our team members engaged in ongoing conversations about positionality, assumptions, and interpretive responsibility while analyzing and synthesizing findings. We discussed the potential for our positionalities as researchers to shape interpretation and representation, and we approached the synthesis with care, humility, and a commitment to justice.
Findings
The included studies examined the experiences of gender-based violence among approximately 600 disabled women across 49 studies. We have summarized each study’s focus, location, sample size, type of disability, and type of violence in tables found in Supplemental Appendix C. Most studies were conducted in the United States (15), followed by the United Kingdom (7) and Australia (4). Other studies took place in Ghana (3), Ethiopia (3), South Africa (3), Bangladesh (2), Zimbabwe (2), Spain (2), Austria (1), Brazil (1), Croatia (1), Finland (1), India (1), Iran (1), Nepal (1), and Sierra Leone (1). The studies included diverse disability identities and captured the heterogeneity of disabled women’s experiences. Many studies examined co-occurring disabilities, including physical disabilities (34), sensory disabilities (23), cognitive disabilities (18), cancer-related disabilities (4), and chronic illnesses (3). A smaller number of studies examined specific conditions such as fibromyalgia, endometriosis, podoconiosis, and chronic maternal disabilities. Participants reported a wide range of gender-based violence experiences. Physical violence (39) and sexual violence (39) appeared most frequently, followed by psychological violence (27), emotional abuse (19), financial abuse (17), neglect (9), and verbal abuse (7). Some studies also examined institutional violence (4), disability-specific abuse (4), obstetric violence (2), and other forms of harm, including animal abuse, isolation, occupational deprivation, and reproductive coercion. The studies represented participants across early to late adulthood, reflecting the lifespan experiences of disabled women navigating violence.
We have summarized the methodological approaches used across the included studies in Table 4 in Supplemental Appendix C. Most studies relied on individual interviews (36), while others used focus groups (2) or mixed-methods designs (7). A small number used alternative qualitative methods, such as ethnographic observation or case studies (4). The analytical approaches varied across studies. Researchers most frequently used thematic analysis (18), followed by phenomenology (7), content analysis (6), grounded theory (4), and other approaches, such as paradigmatic or narrative analysis.
We identified four overarching themes (summarized in Table 1) that captured disabled women’s experiences of gender-based violence. These themes highlighted systemic, interpersonal, and personal challenges, and strategies for survival and resistance. The themes are presented in an order that reflects a conceptual and narrative progression from systemic and institutional harms through interpersonal and social experiences of violence to women’s responses of resilience and resistance.
Systemic Neglect and Institutional Harm
Findings from 32 studies contributed to this theme, demonstrating the pervasive role of systemic neglect and institutional harm in disabled women’s experiences of gender-based violence. Disabled women described encountering systemic neglect and institutional harm when seeking support from social services, healthcare, and justice systems. Participants described dismissive attitudes from service providers, inadequate accommodations, and institutional failures to recognize or respond appropriately to violence (Budu-Ainooson, 2020; Hasan et al., 2014). Restrictive shelter policies, particularly those limiting access for women with service animals or children, further limited women’s ability to escape abusive situations (Alhusen et al., 2020).
A lack of tailored resources and limited service flexibility constrained access to appropriate support (Budu-Ainooson, 2020; Hasan et al., 2014). One of the most concerning findings involved the failure of systems to proactively identify abuse. Healthcare providers often failed to screen for violence or provide appropriate interventions (Alhusen et al., 2020). In a study examining screening practices during pregnancy, eight out of nine participants (89%) reported that healthcare providers never asked about intimate partner violence despite being at high risk (Alhusen et al., 2020). One participant described attempting to signal distress while providers avoided engagement:
In my opinion, [they] missed every red flag I was trying so desperately to wave. I felt like they couldn’t get out of the room fast enough. I was never asked. I feel lucky to be alive. . .but it didn’t have to be this difficult. (Alhusen et al., 2020, p. 3)
Seeking help was described as daunting, particularly in contexts marked by fear of retaliation, lack of follow-up after reporting violence, and feelings of shame, embarrassment, and self-doubt (Budu-Ainooson, 2020; Hasan et al., 2014; Robinson et al., 2021). These barriers reinforced cycles of neglect and left many survivors without access to essential support services.
Institutional violence within healthcare settings was also documented. Participants described experiences of insidious or direct silencing, humiliation, and dehumanization by healthcare professionals and service providers (São Bento & Moreira, 2017). This violence took both overt forms, such as direct mistreatment, and more subtle forms, including disregard for women’s health and autonomy (Hassouneh-Phillips, 2004). Some women reported obstetric violence, where providers made medical decisions without consent, reinforcing deeply unequal power dynamics (Wudneh et al., 2022). One survivor shared a story about coercive reproductive control during childbirth:
I arrived at the delivery room in a wheelchair. I was 24 years old, a mother of a young child, and expecting twins. . .A male surgeon enters the operating room and inquires about the number of children I have. “No one,” I replied. The surgeon asks me flatly if I want to be tied this time. When I said no, the surgeon looked at me and said, “You must be tied because of your disability. . .” (Wudneh et al., 2022, p. 9)
Beyond healthcare settings, personal care providers were identified as perpetrators of abuse (Hague et al., 2011a). Participants described boundary violations, including inappropriate physical contact, neglect, and psychological manipulation (Hague et al., 2011a; Saxton et al., 2001). Research conducted in care facilities showed that staff sometimes denied women dignity and autonomy and failed to meet basic care needs (van der Heijden et al., 2019). One survivor described how medical professionals undermined her sexual and bodily autonomy:
And even when I went to have my abortion, I went to this one hospital, and this nurse says to me: “How did you get pregnant? I didn’t know you could ‘do it’ [have sex] in wheelchairs?” (van der Heijden et al., 2019, p. 835)
Caregiving relationships often blurred boundaries between care and coercion, making it difficult for disabled women to identify when support became control. Survivors described how caregivers reinforced power imbalances through neglect, including leaving women unattended or ignoring basic needs (Saxton et al., 2001). One woman reflected on how this mistreatment operated as a form of control within her caregiving relationship, capturing how caregiving relationships were shaped by unequal power and institutional structures:
Being left in the shower and then she doesn’t come back like for five minutes. It kind of changes the relationship, shifts the balance of power to her when she does that because then she knows that I’m usually nice to her after that. (Saxton et al., 2001, p. 402)
Overall, the findings showed that systemic neglect and institutional harm sustained cycles of violence by failing to recognize, prevent, or adequately respond to abuse. Inadequate screening, inaccessible services, and abuse perpetuated by professionals and caregivers collectively reinforced disabled women’s vulnerability and limited their access to meaningful protection and support.
Experiences of Revictimization
Findings from 33 studies contributed to this theme, highlighting how disabled women often encountered systemic failures when seeking support, resulting in cycles of revictimization. In this context, revictimization referred to the ways survivors were retraumatized by the very systems meant to support them. The concept of institutional betrayal outlined the failure of institutions to protect, support, or appropriately respond to individuals who depended on them (Corbett et al., 2025). Institutional betrayal included dismissive attitudes, victim-blaming responses, inadequate policies, and systemic negligence (Corbett et al., 2025).
Women reported feeling ignored, dismissed, or even punished when disclosing their abuse to institutions (Opsahl & Pick, 2017). Rather than receiving safety or support, some survivors described mistreatment by the very services intended to help them, which left them feeling responsible for their own victimization (Walter-Brice et al., 2012). This theme captured these dynamics, illustrated further through three related sub-themes. The silencing and social stigma that participants described as preventing disclosure and enabling abuse to persist are outlined in A Wall of Silence. The systemic inaccessibility and economic insecurity that deepened survivors’ vulnerability and limited their options for escape are highlighted in Entrapment Through Dependence. Finally, the long-term emotional, physical, and psychological consequences of living through repeated harm without support that participants described are summarized in The Toll of Revictimization. Together, these sub-themes illustrated that revictimization is not solely the result of individual experiences of violence, but also of broader social, cultural, and institutional failures.
Women described negative experiences with social workers, legal professionals, and community leaders, who either failed to provide meaningful assistance or actively discouraged them from seeking justice (Hasan et al., 2014; Robinson et al., 2021). Some shared how ineffective responses from service providers retraumatized them, leaving them feeling unsupported or unsafe in therapeutic settings:
I had some counselling. . .I only went to two sessions because the first time I went the lady said, “Well, tell me your story,” and I told her, and she just sat there and cried and then. . .I went back. . .and I told her what was going on and she just sat there and cried and in the end. . .I thought, no, this is not good for me. (Jordan, 2022, p. 3693)
Legal and financial barriers were also common, with survivors reporting that they were denied representation unless they could afford high legal fees (McCulloch et al., 2021). Disabled mothers, in particular, described being blamed and punished for the violence they experienced through the removal of their children rather than the provision of support (McCulloch et al., 2021): “When we ask for help, there’s no one to help us. They seem to take your children away instead of helping you [sobbing]” (McCarthy et al., 2017, p. 276). These failures left survivors feeling trapped, silenced, and retraumatized by the very systems that should have supported them.
A Wall of Silence
Women with disabilities described their experiences of abuse as being met with silence from service providers, family members, and the wider community (Robinson et al., 2021). This silence reinforced the invisibility of gender-based violence and created conditions in which abuse persisted without intervention (Sallinen & Kukkurainen, 2015). Silence also functioned as a barrier to disclosure, making it more difficult for survivors to seek help (Hasan et al., 2014). Here, silence reflected not only a personal coping strategy but also broader cultural stigma that discouraged disclosure and isolated survivors:
Our neighbours do not know anything about this. I did not tell them. . .If people can find a deficiency, they will castigate me (khota dibo). During quarrels, they will take the upper hand and stigmatize me (shorom dibo). This is why I don’t discuss this with anyone. (Naved et al., 2012, p. 189)
Families also imposed silence by denying the violence or blaming disabled women for their experiences (Daruwalla et al., 2013). Women with disabilities reported being ostracized or disbelieved by family members when they disclosed abuse. Cultural expectations and social stigma surrounding disability and gender-based violence pressured many women to remain silent, even when their safety was at risk (Ruiz-Pérez et al., 2018).
Entrapment Through Dependence
Disabled women often faced additional barriers to leaving abusive situations due to reliance on others for mobility, care, or financial stability (Rugoho & Maphosa, 2015). Abusive partners exploited these vulnerabilities to deepen women’s dependence and isolation (Ruiz-Pérez et al., 2018). Survivors described feeling powerless due to the physical and economic control exerted by abusive partners:
I felt so tired and I had no energy but he wasn’t going to take no for an answer so I didn’t feel like I had a choice. . .He knows I can’t fight back. I mean what can I do? Women like me [in a wheelchair], we’re vulnerable to violence. (Alhusen et al., 2020, p. 3-4)
Economic dependence was cited as a reason for remaining in abusive relationships, with some unable to leave due to financial constraints. One woman’s story exemplified how the lack of economic opportunities reinforced entrapment and undermined self-efficacy:
He used to threaten me. “Go to a lawyer! Report me! Report me! You’re useless! What are going to do? What are you going to do, work as a cleaner? How?” (Ruiz-Pérez et al., 2018, p. 1061)
Reliance on caregivers and partners for basic needs entrapped many disabled women in cycles of violence, making it difficult to leave abusive relationships (van der Heijden et al., 2019). When abusive partners or caregivers controlled access to mobility aids, transportation, or financial resources, survivors often felt they had no viable means of escape (Ballan & Freyer, 2020). For some, fear of worse conditions outside the relationship, such as institutionalization or homelessness, forced them to endure ongoing abuse:
I knew I needed to get out. . .but that’s easier said than done when you’re reliant on [abusive partner] to get you everywhere. I needed to know where I could go, and not worry that it would be worse. (Alhusen et al., 2020, p. 4)
This quotation illustrated the importance of accessible, independent transportation for survivors seeking to escape abuse, and the critical role of functional independence in leaving violent relationships.
The Toll of Revictimization
The cumulative impact of violence and systemic neglect led to profound emotional, psychological, and physical consequences. Women described depression, anxiety, chronic pain, and post-traumatic stress disorder (PTSD) as direct results of prolonged exposure to abuse (Copel, 2006; Hague et al., 2011b). Women also reported that stress worsened existing health conditions or that trauma contributed to the onset of new disabilities (Freeborn & Curry, 2009; Sawin et al., 2009). The psychological toll of revictimization was linked to exhaustion, hopelessness, and despair, with descriptions of abuse slowly eroding their sense of self-worth and identity (Divin et al., 2013). Studies reported suicidal ideation and self-harm among women who endured long-term violence as accumulated trauma left them feeling that escape was impossible (Freeborn & Curry, 2009; McCarthy, 2019). One participant described the emotional devastation caused by years of mistreatment: “I wasn’t getting no help or anything during my court proceedings. . .I took an overdose” (McCarthy, 2019, p. 16). Abuse also exacerbated their physical conditions, leading to further disability, increased pain, and long-term functional decline (Hassouneh-Phillips & McNeff, 2005; Poleshuck et al., 2018). Sexual and emotional abuse also placed some women at heightened risk for reproductive health complications. Chronic maternal violence resulted in unwanted pregnancies, increased strain on existing disabilities, and reproductive health issues stemming from coerced or forced sexual activity (Naved et al., 2012).
The intersection of gender-based violence and disability intensified the impact of revictimization, and many survivors reported complex trauma, unaddressed health concerns, and a sense of isolation. Despite these challenges, proactive and disability-informed healthcare interventions were proposed as ways to mitigate harm. Aguillard, Hughes, et al. (2022) reported that when healthcare providers used a trauma-informed approach and screened proactively for PTSD and depression, survivors were more likely to receive the support they needed.
Dehumanization and Oppressive Experiences
This theme relied on findings from 44 studies included in the synthesis and captured the prominence of dehumanization and systemic oppression in disabled women’s experiences of gender-based violence. These experiences shaped their interactions with partners, caregivers, service providers, and broader society and reinforced feelings of powerlessness and exclusion. The process of dehumanization manifested in three interrelated ways: infantilization and the stripping of autonomy, which led others to treat survivors as incapable or dependent; internalized ableism, which shaped how survivors viewed their own worth and agency; and intersecting oppressions, which amplified barriers to safety, support, and recognition. These sub-themes demonstrated dehumanization across interpersonal and systemic levels, which increased vulnerability to violence and reduced access to justice and care.
Infantilization and Dehumanization
Disabled women described being treated as childlike, incapable, or dependent, and studies identified this infantilization as a recurring aspect of their experiences of gender-based violence. Societal perceptions of disabled women as defenseless and in need of constant care rendered them particularly vulnerable to control and exploitation (Rugoho & Maphosa, 2015). This vulnerability intensified when communities overlooked or dismissed disabled women’s lived realities, leading to limited recognition and support when abuse occurred (Daruwalla et al., 2013). Several studies found that some men perceived disabled women as sexually available and lacking agency, which heightened risks of sexual violence (Daruwalla et al., 2013).
Disabled women’s reliance on others for daily support often reinforced infantilizing attitudes and power imbalances within intimate relationships (Rittmannsberger, 2022). Survivors described how partners used disability as a justification for control, dismissed their autonomy, and minimized their health concerns. One woman explained how her partner used infantilizing and blame-based arguments to undermine her independence and sense of agency, blaming her for her condition and reinforcing dependency and control within the relationship:
He tells me that I am the cause of my illness. Who likes chemotherapy? Chemotherapy is so difficult. Even if I have a headache, he says it is your fault. He says “do not think about everything.” (Sheikhnezhad et al., 2023, p.4)
Infantilization extended beyond personal relationships into broader societal structures that excluded disabled women from valued roles and interactions. Women with intellectual disabilities experienced social invisibility through denial of employment and limited opportunities for social engagement. Perceptions of incapability contributed to gendered power imbalances that increased their likelihood of experiencing intimate partner violence (Pestka & Wendt, 2014). One participant described how an employer’s reaction to her disability reflected these assumptions:
I applied for employment at my current employer. I passed the interview and then after that, it was my first day at work. My supervisor at that moment was not aware of my disability. So, when she first saw me, she was angry because in her mind I could not perform the duties because of my disability. (Muruzi & Gutura, 2022, p. 19369)
Survivors described the stigma associated with disability and the resulting social exclusion as an extension of the violence they endured (Daruwalla et al., 2013). Societal failure to recognize disabled women as whole individuals deserving of respect, autonomy, and support enabled abuse and reinforced its lasting effects.
Internalized Ableism
Studies reported that many women with disabilities internalized societal devaluation of disabled bodies and identities, shaping perceptions of self-worth, desirability, and autonomy within relationships. Research highlighted how deeply ingrained messages portrayed disabled women as inadequate or flawed, which influenced their decisions about seeking support or leaving abusive relationships (Aguillard, Gemeinhardt, et al., 2022). Societal norms that framed disabled individuals as undesirable sexual partners or incapable parents contributed to this internalized ableism. Hassouneh-Phillips and McNeff (2005) found that negative societal attitudes toward disability shaped disabled women’s self-perceptions and led many participants to believe they were unworthy of fulfilling romantic relationships. These beliefs often eroded sexual self-esteem and increased the likelihood that women remained in abusive relationships (Hassouneh-Phillips & McNeff, 2005). One woman described how community members questioned the legitimacy of disabled women’s roles as mothers, reinforcing internalized ableism:
“Whose are these children? Are they yours? Amazing. . .how did you get pregnant. . . how did you deliver all four. . .almighty God.” These are common expressions from the community. (Hirpa, 2022, p. 13)
Studies also showed that women internalized the lack of appropriate institutional responses to abuse and interpreted these failures as reflections of their own worth or limitations (Walter-Brice et al., 2012). Others described profound isolation related to disability and expressed beliefs that non-disabled people could not understand their experiences (Aguillard, Gemeinhardt, et al., 2022). These internalized messages reduced their willingness to challenge abuse and strengthened cycles of violence and dependence.
Compounding Oppressions
Findings showed that gender-based violence intersected with additional forms of oppression related to race, class, poverty, and social exclusion. Disability combined with other marginalized identities created layered disadvantages that increased vulnerability to violence and generated additional barriers to support (Hague et al., 2011a). Women who experienced multiple forms of marginalization were more likely to live in poverty, rely on informal housing arrangements, and lack access to safe and accessible shelters (van der Heijden et al., 2019). Intimate partner violence occurred more frequently among women facing systemic barriers, such as rural residence, lower income, and membership in historically marginalized communities (Tsegay et al., 2018). Disabled women from minority communities reported increased isolation and lower engagement with formal support services (Hague et al., 2011b). One participant reflected on how gendered power dynamics shaped women’s treatment:
Women have always been looked at as being “lessive” [lesser] beings than men are. And I know that there are some things about women and their personality and how they deal with things that make it easy for men to joke and to just treat women more lightly. I think that definitely has a part to play in how any person is treated. (Freeborn & Curry, 2009, p. 562)
Dehumanization and oppression took multiple forms and reinforced disabled women’s vulnerability to violence while limiting their ability to seek safety and justice. Infantilization and social exclusion reduced autonomy, while internalized ableism shaped self-perceptions. Intersecting oppressions further intensified social and economic barriers to support. The studies illustrated that systemic change is needed to stop these factors from sustaining environments in which violence against disabled women is tolerated, ignored, or rendered invisible.
Resilience and Resistance to Violence
This theme drew on findings from 28 studies included in the synthesis and illustrates how disabled women exercised resilience, agency, and resistance in the context of gender-based violence. Despite widespread portrayals of disabled women as passive victims, the reviewed studies highlighted women’s strength, agency, and resistance in the face of violence. Rather than defining themselves solely through experiences of harm, many disabled women actively challenged oppression by drawing on internal resilience, social networks, and acts of self-advocacy to reclaim autonomy (Aguillard, Gemeinhardt, et al., 2022). The findings demonstrated that survival involved not only enduring violence but also resisting it in ways that affirmed dignity and humanity. In doing so, survivors resisted not only individual acts of violence but also the societal structures that sought to marginalize them.
Disabled women described numerous ways they resisted violence, including confronting abuse, leaving harmful relationships, and seeking justice through legal or community-based support systems (Walter-Brice et al., 2012). These acts of resistance often reflected women’s commitment to protecting themselves and others, as well as their determination to challenge the social structures that rendered them vulnerable. One survivor reflected on her resilience and adaptability:
I’ve always had to think out of the box because the box wasn’t my box, it was everybody else’s box. I was already out of the box. (laughs) So anyway I had that creativity going for me and I think that, I think I’ve done very well and I think that I rarely say “Can’t.” So there’s always a way to do it. (Aguillard, Gemeinhardt, et al., 2022, p. 15602)
Women also found strength from faith, spirituality, and personal coping strategies. Prayer was identified as a vital source of emotional support that provided comfort during periods of despair and reinforced women’s sense of self-worth (Divin et al., 2013). Other women relied on problem-solving skills developed through years of navigating environments not designed for them. The resilience they developed while managing everyday challenges, such as accessibility barriers, discrimination, and social exclusion, often formed the foundation for resisting violence and reclaiming control over their lives (Aguillard, Gemeinhardt, et al., 2022).
Resilience and resistance were identified as processes that required time, support, and recognition of one’s worth. Disabled women’s survival and perseverance represented not only individual acts of endurance but also forms of defiance against systems that sought to silence and marginalize them. By continuing to resist, disabled women asserted agency and challenged the conditions that enabled gender-based violence.
Discussion
The findings of this qualitative meta-synthesis demonstrate how structural barriers, power imbalances, and systemic neglect prevent women with disabilities from leaving abusive relationships and accessing necessary support services. These findings extend prior research on multi-level barriers to safety for disabled women (Meer & Combrinck, 2015; Walter et al., 2024; Wright & Manuel, 2025) by showing how women experience these barriers globally. Inaccessible shelters and environmental obstacles can reinforce isolation, while dependence on caregivers and institutions can limit disabled women’s autonomy. The pervasiveness of violence across childhood, adolescence, and adulthood underscores the chronic nature of victimization. Disabled women frequently experience gender-based violence from multiple people, including intimate partners, family members, caregivers, and service providers. Abusive tactics often include disability-specific forms of abuse, such as withholding assistive devices or medication, exploiting physical limitations, and humiliating women based on their disabilities. Regardless of who perpetrates the violence, this meta-synthesis identifies infantilization as a core aspect of abuse throughout the lifespan, as Olkin et al. (2019) previously articulated. Across the included studies, infantilization emerges as a central dynamic shaping both interpersonal abuse and institutional responses. This dynamic reinforces women’s powerlessness.
These findings further highlight the intersection of systemic and interpersonal violence. Disabled women experience dehumanization and marginalization not only from those perpetrating the abuse but also from institutions. Healthcare, social service, and legal systems often perpetuate abuse and neglect through institutional betrayal, a process in which institutions fail to protect those who depend on them (Corbett et al., 2025). Research across marginalized populations has documented institutional betrayal as a mechanism through which institutions harm the very people they intend to support (Hamby et al., 2023). The findings of this meta-synthesis demonstrate how institutional betrayal operates as an extension of interpersonal abuse. It reinforces isolation and limits pathways to safety. At the same time, participants emphasized the importance of community collaboration and peer support networks in fostering empowerment and resilience. Despite significant structural and interpersonal oppression, women with disabilities demonstrate persistence and self-advocacy. They resist violence through collective action, mutual support, and personal agency.
One of the most concerning findings centers on the revictimization disabled women experience when seeking help. Consistent with earlier research (Meer & Combrinck, 2015; Walter et al., 2024), many women encountered attitudinal barriers and social stigma within social and legal systems. Professionals often responded with disbelief, blame, or punitive consequences. As McCarthy et al. (2017) identified, some social service providers removed children from mothers experiencing abuse instead of offering meaningful support. These responses reinforced survivors’ trauma and discouraged future help-seeking. This meta-synthesis extends prior work by showing that revictimization does not operate as an isolated incident. Instead, it functions as a systemic pattern embedded in service responses that prioritize risk management over survivor-centered care. The “wall of silence” described in earlier research (Sallinen & Kukkurainen, 2015) appears across multiple studies in this synthesis. It functions as another mechanism of institutional betrayal. This silence operates not only at the institutional level but also within families and communities. It further isolates survivors and discourages disclosure and efforts to seek justice (D’Costa, 2025; Walter et al., 2024). D’Costa’s (2025) research identified how disabled women experiencing intimate partner violence encountered obstacles across multiple domains of their lives. This work provides another example of systemic neglect and failure across levels, as illustrated in this meta-synthesis. Although gender-based violence remains historically and culturally pervasive, it is often concealed by systemic inaction and cultural norms that privilege secrecy over survivor-centered responses. These dynamics create the forms of entrapment described in the studies included in this synthesis.
Moreover, the meta-synthesis findings illustrate how ableism reverberates across multiple systems in the lives of disabled women who experience gender-based violence. As Olkin et al. (2019) noted, ableist microaggressions, such as minimizing disability-related needs or questioning credibility, carry serious consequences. These consequences become especially severe when medical professionals fail to refer disabled women to appropriate treatment and support. Kattari’s (2020) description of ableism as operating through behavioral, cultural, and structural norms closely aligns with the internalized ableism evident across the studies included in this synthesis. Survivors often internalized societal messages that framed them as burdensome, incapable, or undeserving of care. These messages shape self-perceptions and influence decisions to remain in abusive relationships.
Overall, this meta-synthesis underscores the importance of applying an intersectional lens (Collins, 2019; Crenshaw, 1991) to address ableism within gender-based violence. It also situates disabled women’s experiences within broader systems of compounded oppression (Wright & Manuel, 2025). Disability does not exist in isolation. It intersects with race, ethnicity, sexual orientation, socio-economic status, and other marginalized identities, shaping women’s lived realities in unique ways. This meta-synthesis demonstrates how women with disabilities from marginalized communities experience double stigma, heightened isolation, and additional barriers to accessing support (Hague et al., 2011a). Yet, research continues to show that disability remains marginalized even within intersectional anti-violence efforts (Wright & Manuel, 2025). This gap highlights the critical need to center disability in research, policy, and programming to create more inclusive and effective responses to gender-based violence.
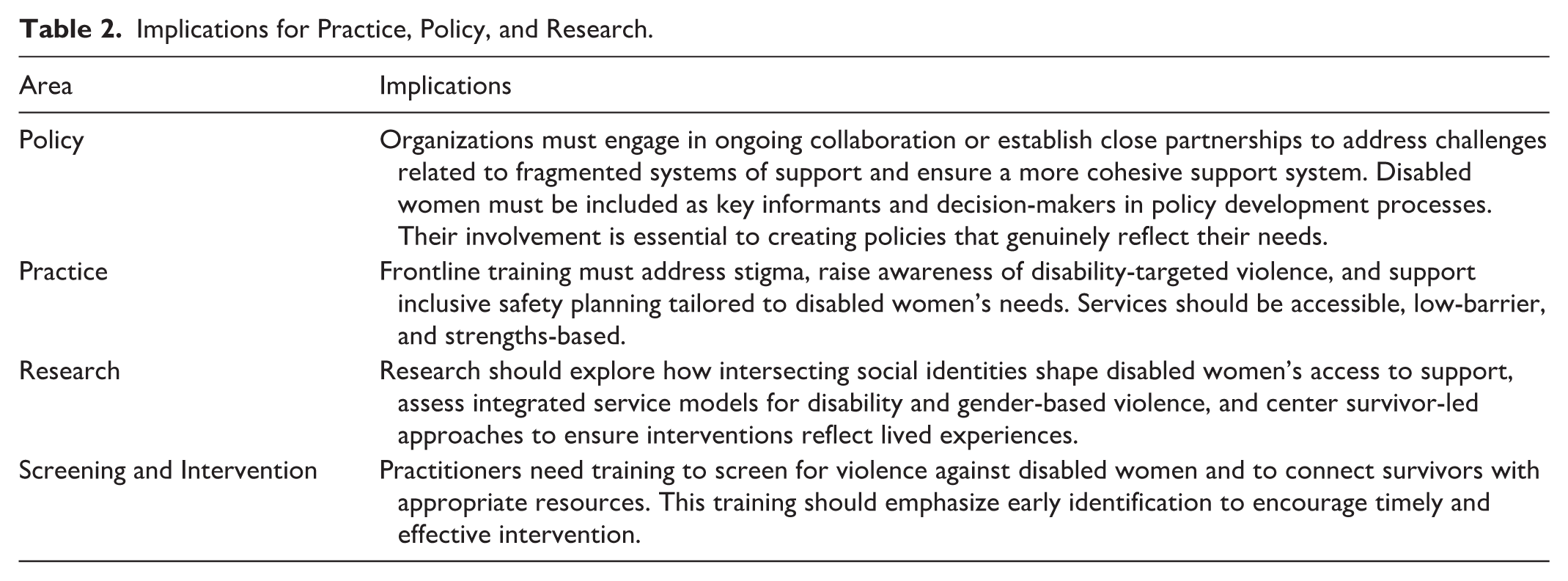
The findings of this meta-synthesis reinforce the urgent need for structural changes across research, policy, and service provision to address the unique experiences of disabled women affected by gender-based violence. Key implications for practice, policy, and research are outlined in Table 2.
Implications for Practice, Policy, and Research.
Limitations and Future Directions
While this qualitative meta-synthesis provides a comprehensive examination of the experiences of disabled women who survive gender-based violence, several limitations should be acknowledged. First, although the aim is to capture diverse lived experiences, the synthesis is limited by the scope of available research. The final set of included studies reflects only those that met our inclusion criteria. As a result, perspectives from some populations, particularly Indigenous disabled women and women from underrepresented regions, may be absent. Additionally, despite using a comprehensive search strategy, variations in terminology and indexing practices across databases may have led us to inadvertently exclude relevant studies. Second, most studies included in this meta-synthesis originate from high-income countries, particularly the United States, the United Kingdom, and Australia. This geographic concentration may limit the applicability of the findings to disabled women living in low- and middle-income countries, where structural, cultural, and service-related barriers to help-seeking may differ. Relatedly, as with most qualitative syntheses, this review depends on the scope and depth of reporting in the original studies. The original authors may not have captured or emphasized certain dimensions of participants’ identities or experiences. This limitation may shape the themes identified in this synthesis. This synthesis also does not provide detailed counts of how frequently specific findings appear within or across sub-themes. Because individual studies often contribute to multiple themes and analytic excerpts, this level of detail was not included. This decision represents a limitation for readers seeking frequency-based comparisons. Finally, publication bias may influence the studies available for inclusion, as less visible or unpublished community-led research may remain excluded.
While this analysis highlights systemic barriers, revictimization, and institutional harm, further research should examine effective interventions and best practices for supporting disabled survivors. Future studies should amplify the voices of disabled women through participatory and community-led research approaches. Despite these limitations, this study offers critical insights into how disabled women experience and resist gender-based violence. It also underscores the need for accessible, survivor-centered interventions that recognize both vulnerability and strength.
Conclusion
This qualitative meta-synthesis highlights the distinct and complex challenges women with disabilities face when experiencing gender-based violence. Across the included studies, disabled women described neglect by systems intended to protect them, repeated exposure to violence, and deeply dehumanizing and oppressive conditions. At the same time, survivors articulated resilience and resistance. They actively challenged the harms they experienced. A common thread across the themes is institutional betrayal. Institutions that women turned to for safety and support often exacerbated trauma rather than alleviating it. These patterns reinforce the need for survivor-led initiatives, policies, and programs grounded in first-voice knowledge and lived experience.
Addressing these issues requires a multi-pronged response involving governments, social service organizations, healthcare systems, and community networks. Structural investments must reduce gender inequality, improve accessibility within support services, and foster inclusive environments where disabled women feel safe seeking help. Both formal and informal support play critical roles in preventing and responding to violence. Without coordinated, well-resourced, and inclusive systems of care, however, survivors remain underserved and at risk.
Future research must prioritize an intersectional lens to examine how disability interacts with race, ethnicity, sexual orientation, and socio-economic status in shaping experiences of violence and help-seeking. Research should also move beyond documenting barriers and focus on identifying specific protective factors and interventions that improve safety and access to justice for disabled survivors. Because the findings demonstrate survivors’ resilience and resistance, future studies should expand participatory and community-led approaches. These approaches can ensure that women with disabilities are not only research participants but also active contributors to shaping solutions.
Ultimately, survivors of gender-based violence require inclusive, anti-ableist interventions that recognize their needs, strengths, and identities. Many existing services remain inaccessible and continue to reinforce cycles of marginalization and exclusion. Organizations and researchers must take intentional action to create safer, more accessible spaces where disabled survivors can share their experiences without fear of further harm. By amplifying survivor voices and addressing systemic inequities, a more just and inclusive response to gender-based violence becomes possible. These efforts are essential to ensuring that disabled women receive the support and protection they deserve.
Supplemental Material
sj-docx-1-tva-10.1177_15248380261433014 – Supplemental material for Experiences of Gender-Based Violence Among Disabled Women: A Qualitative Meta-Synthesis
Supplemental material, sj-docx-1-tva-10.1177_15248380261433014 for Experiences of Gender-Based Violence Among Disabled Women: A Qualitative Meta-Synthesis by Ami Goulden, Stephanie L. Baird, Sarah E. Norris, Victoria Lewis and Kristen Romme in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-2-tva-10.1177_15248380261433014 – Supplemental material for Experiences of Gender-Based Violence Among Disabled Women: A Qualitative Meta-Synthesis
Supplemental material, sj-docx-2-tva-10.1177_15248380261433014 for Experiences of Gender-Based Violence Among Disabled Women: A Qualitative Meta-Synthesis by Ami Goulden, Stephanie L. Baird, Sarah E. Norris, Victoria Lewis and Kristen Romme in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-3-tva-10.1177_15248380261433014 – Supplemental material for Experiences of Gender-Based Violence Among Disabled Women: A Qualitative Meta-Synthesis
Supplemental material, sj-docx-3-tva-10.1177_15248380261433014 for Experiences of Gender-Based Violence Among Disabled Women: A Qualitative Meta-Synthesis by Ami Goulden, Stephanie L. Baird, Sarah E. Norris, Victoria Lewis and Kristen Romme in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-4-tva-10.1177_15248380261433014 – Supplemental material for Experiences of Gender-Based Violence Among Disabled Women: A Qualitative Meta-Synthesis
Supplemental material, sj-docx-4-tva-10.1177_15248380261433014 for Experiences of Gender-Based Violence Among Disabled Women: A Qualitative Meta-Synthesis by Ami Goulden, Stephanie L. Baird, Sarah E. Norris, Victoria Lewis and Kristen Romme in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
The authors thank the research assistants and collaborators who contributed to the early stages of this study, including literature searches, data extraction, and preliminary analysis.
Ethical Considerations
Ethical approval was not required for this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Social Sciences and Humanities Research Council (SSHRC) Knowledge Synthesis Grant [872-2022-0007].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study were derived from previously published journal articles and are publicly available through the respective publishers. Researchers interested in accessing the original studies may refer to the citations listed in this paper.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.