
Abstract
This systematic review examines the role of causal attributions in the maintenance and recovery of PTSD symptoms. Causal attributions, which include dimensions such as locus (internal vs. external), controllability (controllable vs. uncontrollable), and stability (stable vs. unstable), as well as locus of control, learned helplessness, and self-blame, are crucial in understanding the cognitive processes that contribute to PTSD. The review followed PRISMA guidelines and included longitudinal empirical studies on the association between causal attributions and PTSD symptoms over time. A total of 13 articles were included in the review. Attributions were categorised as pertaining to ‘locus’, ‘control’, and ‘consistency’. The findings indicate that maladaptive attributions, whether related to locus, control, or consistency, contribute to the persistence and severity of PTSD symptoms. For attributions regarding the origin of the traumatic event, an external locus of control with another person, as well as internal characterological self-blame, appeared to be maladaptive. In addition, for attributions regarding experiences during the traumatic event, low levels of experienced control, control options that were not (sufficiently) exercised, and high levels of perceived consistency appeared to be maladaptive. The review offers a nuanced and a comprehensive framework that enhances our understanding of how individuals perceive and interpret traumatic events, by recognising that attributions are complementary rather than mutually exclusive. This independency approach acknowledges the complexity of human cognition and highlights the importance of addressing deeply anchored maladaptive attributions in therapeutic interventions.
Introduction
With an estimated lifetime prevalence of 3.9%, post-traumatic stress disorder (PTSD) is a common mental disorder worldwide (Koenen et al., 2006). Patients diagnosed with PTSD suffer from severe trauma-related symptoms, including intrusions, avoidance behaviours, negative alternations in cognition and mood, and marked alternations in arousal and reactivity, following exposure to a traumatic event (American Psychiatric Association, 2013).
According to Ehlers and Clark’s (2000) cognitive model, PTSD develops and persists when individuals process traumatic events in ways that create a sense of perpetual threat. This perception results from excessive negative appraisals of the traumatic event and its consequences, as well as from disturbances in autobiographical memory, including poor elaboration, strong associative memory, and perceptual priming (Ehlers & Clark, 2000). As individuals with PTSD repeatedly relive the traumatic experience, their cognitive appraisals of the traumatic event – such as attributions of controllability and stability – play a central role in maintaining their emotional, behavioural, and physiological reactions. In order to make sense of their traumatic experiences and to regain a sense of control and predictability, especially after unexpected or traumatic events, people are often motivated to make causal attributions (Wong & Weiner, 1981). The first aim of this review study is to conduct a systematic review of longitudinal studies investigating the impact of causal attributions on PTSD symptom development.
The second aim of this review study is to provide a classification system for causal attributions that is useful for reviewing empirical studies on causal attributions and PTSD symptom development over time. The most commonly used dimensions for categorising causal attributions are those of Weiner (1986) and include locus (internal vs. external), controllability (controllable vs. uncontrollable), and stability (stable vs. unstable). These dimensions have proven useful for understanding causal attributions in people with PTSD.
Weiner’s Dimensions of Causal Attributions and Their Relation With PTSD Symptoms
Causal attributions play a significant role in the development and maintenance of PTSD (Massad & Hulsey, 2006). Research suggests that internal, stable, and global attributions are associated with psychological distress in general and are particularly relevant to trauma-related symptoms, including PTSD (e.g. Gray et al., 2003; Joseph et al., 1993; Seah & Berle, 2022). For example, psychology students who blamed themselves for a traumatic event they experienced (internal attribution), identified enduring and unchangeable factors (stable attribution), and perceived those factors as broadly affecting their life (global attribution) reported higher levels of PTSD symptoms (Gray et al., 2003). The role of causal attributions (or attributional style) in the development of PTSD symptoms is further supported by a review by Elwood, Hahn, et al. (2009), who suggest that negative attributional styles – attributions that are internal, stable, global, and uncontrollable – may act as a contributing factor for developing PTSD symptoms. Each of these types of attributions works in conjunction with other processes that further contribute to PTSD symptoms. Attributing trauma to internal causes (e.g. ‘it’s my fault’) was associated with increased shame, which in turn was linked to greater PTSD symptom severity (Seah & Berle, 2022). Moreover, attributing trauma to stable causes was associated with greater PTSD symptom severity, which may contribute to a sense of hopelessness, and hinder recovery (Reiland et al., 2014). Similarly, perceiving the traumatic event as uncontrollable invokes feelings of helplessness and disempowerment, reinforcing the belief that circumstances cannot be changed, thus contributing to chronic distress and the persistence of PTSD symptoms (Hancock & Bryant, 2018; Salcioglu et al., 2017).
Beyond Weiner’s original dimensions, other research has emphasised the significance of global attributions. For instance, perceiving a traumatic event as affecting every area of life has been found to intensify emotional distress (Zinzow & Jackson, 2009) and prolong PTSD symptoms (Gray et al., 2003). These findings suggest that attributional styles that extend beyond Weiner’s framework may also play a critical role in the development of trauma-related psychopathology.
Locus of Control, Learned Helplessness, Self-blame, and Their Impact on Maintenance and Recovery of PTSD Symptoms
In addition to the classic dimensions of causal attribution proposed by Weiner (1986), other attribution tendencies such as locus of control, learned helplessness, and self-blame should also be considered in the maintenance and recovery of PTSD symptoms. Although these concepts share similarities with Weiner’s dimensions in terms of their focus on causality and control, they go beyond his original framework. They reflect broader cognitive processes through which people assign meaning to adverse events, in terms of whether they are perceived as self-caused or externally-driven, controllable or uncontrollable, and stable or changeable. The way people interpret these causes significantly shapes their emotional responses, behavioural patterns, and motivation (Elwood et al., 2009; Janoff-Bulman, 1979). Importantly, these tendencies cannot be fully captured by Weiner’s dimensions. This is why locus of control, learned helplessness, and self-blame will be discussed separately as a distinct dimension. These attribution tendencies are central to understanding how trauma survivors engage with recovery processes, and why certain cognitive styles may hinder or facilitate recovery. Therefore, locus of control, learned helplessness, and self-blame are particularly relevant to PTSD, as they directly influence how individuals perceive and respond to traumatic events.
Locus of Control
Locus of control plays a significant role in the maintenance and recovery of PTSD symptoms. Defined as the extent to which individuals believe they can control the outcomes of their actions (Rotter, 1966), locus of control is aligned with Weiner’s attribution theory, which distinguishes between internal (e.g. effort and ability) and external (e.g. task difficulty and luck) causes of outcomes (Valle, 1974). However, Rotter’s locus of control should not be viewed as a form of causal attribution. While causal attribution is retrospective, explaining past outcomes, Rotter’s is prospective, reflecting expectations about future reinforcement. This distinction establishes locus of control as a distinct concept rather than an extension of the causal attribution framework (Pettersen, 1987). Specifically, an internal locus of control fosters empowerment and control, while an external locus of control is associated with passivity and a diminished self-efficacy (Neeman, 1995). An internal locus of control has been associated with enhanced recovery in patients with chronic pain (Álvarez-Rodríguez et al., 2022) and schizophrenia (Harrow et al., 2009), and similar effects are expected in PTSD. Conversely, a study of undergraduate students found that those with an external locus of control experienced greater difficulty in reducing symptoms because they tended to feel more helpless (Ozment & Lester, 2001).
Learned Helplessness
Learned helplessness, where individuals feel they have no control over outcomes, can contribute to persistent PTSD symptoms (Winterflood & Climie, 2020). When failure is structurally attributed to external, stable causes (e.g. ‘No matter how hard I try, the outcome is beyond my control’), helplessness develops (Abramson et al., 1978). In addition, Alloy et al. (1984) found that those with a global attribution style – blaming negative outcomes on broad factors – experience generalised helplessness, which intensifies their powerlessness in various aspects of life. This may prolong PTSD by impairing coping mechanisms and reducing engagement in treatment (van der Kolk, 2006).
Self-Blame
Self-blame, the tendency to attribute negative outcomes or failures to one’s own actions or characteristics (e.g. ‘I failed because I’m not smart enough’), is another important factor in the maintenance and recovery of trauma-related symptoms, including PTSD (Sinnott et al., 2022). Foa et al. (1999) found that self-blame, as measured by negative trauma-related cognitions, was associated with greater PTSD symptom severity. This suggests that self-blame may hinder recovery by complicating the process.
Reclassification of Attributions
Recent theoretical and empirical work has highlighted the intertwined nature of attributional dimensions such as locus, controllability, and consistency in trauma-related interpretations. Studies have shown that people often attribute traumatic events to causes that are simultaneously internal, stable, and uncontrollable, which intensifies emotional distress and hinders recovery (Reiland et al., 2014; Seah et al., 2023). Constructs such as self-blame, locus of control, and learned helplessness are frequently discussed alongside Weiner’s dimensions; however, they are rarely incorporated into a coherent framework (Elwood et al., 2009).
To organise research on Weiner’s (1986) causal attribution dimensions, as well as research on specific causal attribution tendencies and PTSD, in a meaningful way, we propose grouping the findings into three categories. These are (a) locus-related attributions (Weiner’s dimension of locus, locus of control, and self-blame); (b) control-related attributions (Weiner’s dimension of controllability and learned helplessness); and (c) consistency-related attributions (Weiner’s dimensions of globality and stability). This reclassification clarifies how individuals perceive and interpret traumatic events. Figure 1 provides a visual overview of this proposed reclassification to guide the reader through the conceptual framework that underpins the remainder of this review.
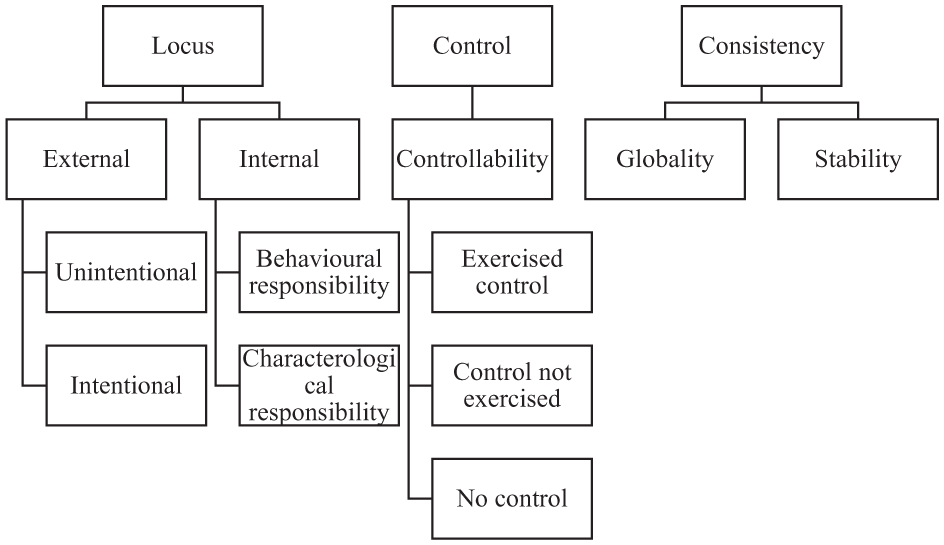
Refined reclassification of causal attributions of traumatic events.
Locus focuses on whether the cause of the traumatic event is attributed to the individual’s own actions (internal) or to external factors beyond the individual’s control (external). Specifically, Weiner’s locus dimension distinguishes between attributing traumatic events to personal characteristics (internal) versus external circumstances. Locus of control expands on this, addressing broader beliefs about whether outcomes are generally determined by internal efforts or external forces. Meanwhile, self-blame focuses on a specific type of internal attribution for negative outcomes.
Controllability, on the other hand, refers to the overall perception during the traumatic event of whether aspects of the traumatic event could have been controlled. When individuals perceive a traumatic event as uncontrollable, they may feel helpless and distressed. Weiner’s controllability dimension and the concept of learned helplessness share a common focus on perceptions of control. Both explain how uncontrollable traumatic events affect individuals, with a lack of control leading to increased distress.
Consistency, which includes Weiner’s stability and globality dimensions, considers the nature and extent of traumatic event causes over time. Stability examines whether a cause for the traumatic event is seen as permanent or temporary, which influences how individuals perceive the likelihood of the event recurring. Globality assesses whether the cause for the traumatic event affects many areas of life or is confined to one area, affecting the perceived scope of the event’s consequences.
The distinctions among locus, controllability, and consistency in causal attributions may have important implications for how individuals cope with traumatic events. Locus influences cognitive processing of the cause of the traumatic event, where internal attributions may lead to self-blame and lower self-esteem, whereas external attributions may protect self-esteem but lead to feelings of injustice or anger and possibly unpredictability or uncontrollability. Perceived uncontrollability leads to helplessness, passivity, and distress, whereas a sense of control during or after the traumatic event fosters empowerment and reduced anxiety. Consistency affects whether people see the causes of a traumatic event as permanent or temporary, and whether they affect many areas of life or just one. Perceiving the causes of one’s traumatic experiences as permanent and affecting many areas of life may contribute to more distress and hopelessness. Understanding these dimensions helps to tailor psychological interventions to increase perceived control, reattribute causes, and address the stability and scope of the event’s impact, thereby promoting effective coping.
Maladaptive Attributions and PTSD Trajectories
Maladaptive attributions have been widely implicated in the onset of PTSD, yet their influence on PTSD trajectories – how symptoms persist, worsen, or remit over time – remains insufficiently understood. Understanding how these dysfunctional cognitive patterns shape the course of PTSD is essential for refining theoretical models and developing targeted interventions. A longitudinal perspective is particularly valuable as it enables us to examine whether maladaptive attributions act as stable vulnerability factors, exacerbate symptom severity, or hinder key recovery processes over time. Despite their theoretical relevance, no comprehensive review has yet synthesised longitudinal evidence on this topic. This review therefore makes a novel contribution by focusing specifically on the longitudinal development of these processes in different trauma-exposed populations.
The Current Study
This review synthesises longitudinal findings on attributional processes in PTSD and proposes a novel classification system based on recurring patterns across studies. Our aim is to bridge the gap between data and conceptual understanding by integrating empirical evidence with theoretical refinement. This review specifically focuses on trauma-related symptoms and attributional processes in adult populations. The purpose of the study is to explore how causal attributions predict the maintenance and recovery of trauma-related symptoms over time. Specifically, the study aims to explore how different types of attributions – such as locus-related attributions, control-related attributions, and consistency-related attributions – affect the course of PTSD symptoms.
We hypothesise
(a) that locus-related attributions (Weiner’s internal dimension, external locus of control, and self-blame) will facilitate prolongation of PTSD symptoms and thus reduce recovery,
(b) that control-related attributions (Weiner’s uncontrollability dimension and learned helplessness) will facilitate prolongation of PTSD symptoms and thus reduce recovery, and
(c) that consistency-related attributions (Weiner’s globality and stability dimensions) will facilitate prolongation of PTSD symptoms and thus reduce recovery.
A key contribution of this review is the proposed reclassification of attributional dimensions into three categories (locus-related, control-related, and consistency-related). This reclassification aims to provide a more nuanced understanding of how attributional processes operate within the context of trauma and recovery. By integrating longitudinal study findings, the review offers a novel framework for conceptualising the role of maladaptive attributions in PTSD, paving the way for new directions in future research and clinical applications.
Method
This study was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009).
Eligibility Criteria
We included empirical, longitudinal studies involving peer-reviewed observational designs that reported on the association among attributions, locus of control, learned helplessness, and self-blame and PTSD symptoms over time (including self-report measures and clinical interviews). Eligible studies had to be written in English or Dutch, published in peer-reviewed journals, and participants had to be adults (age ≥18 years). There were no studies excluded on the basis of participants’ gender, ethnicity, regions/country, or the study’s publication year. Studies that did not report primary quantitative data (e.g. reviews, editorials, book chapters) were excluded.
Search Strategy
For this systematic review, as recommended by Bramer et al. (2017), we searched Embase, Medline, PsycINFO, PTSDpubs, and Web of Science between July 2024 and September 2024. The final search was conducted on September 9, 2024. The following search terms were used in the databases: ‘attribution’ (or ‘attributions’ or ‘attributional style’) OR ‘locus of control’ OR ‘learned helplessness’ OR ‘self-blame’ AND ‘chronic’ (or ‘chronicity’) OR ‘maintenance’ AND ‘PTSD’ (or ‘post-traumatic stress disorder’). Additionally, reference lists of included articles were screened to identify additional articles for inclusion.
Data Extraction
The study selection process consisted of a three-stage process. In Stage 1, we manually searched the databases of Embase, Medline, PsychINFO, and PTSDpubs for eligible studies. Studies were selected based on the title and abstract. Within the title and/or abstract, it was required that the studies reported on control-related, locus-related, or consistency-related attributions (Weiner’s attribution dimensions, locus of control, learned helplessness, and self-blame), chronicity (including maintenance), and PTSD. Additionally, in this stage we used ASReview, an AI tool, to systematically screen all the articles from the Web of Science database. All the studies that had previously been selected from the other databases on the basis of their title and abstract were labelled as relevant in ASReview, which then searched the Web of Science using a search algorithm based on the common denominators of the relevant articles already selected. The results presented by ASReview were then manually labelled as relevant or not relevant by the first author. Articles for which it was unclear whether they met the inclusion criteria were transferred to Stage 2 of the screening process. In Stage 2, the full texts of the articles identified as relevant before and after the ASReview search were assessed to determine whether they met the full eligibility criteria. In Stage 3, references from included papers and manuscripts that cited the included papers were examined to identify additional eligible studies. The study selection procedure was conducted by one reviewer (the first author). A second reviewer conducted a screening of the literature by checking a random sample of 284 screened records. In case of disagreement, consensus on which articles to screen full text was reached by discussion.
Specific information for the systematic review was extracted from the selected studies, which included (a) author, (b) title, (c) year of publication, (d) study design, and (e) follow-up period. In addition, the following descriptive variables were extracted from the studies (if applicable): (f) setting (i.e. country), (g) ethnicity, (h) sample size, (i) age (M; range), (j) sex (%), (k) sample size characteristics, (l) type of trauma, (m) assessment instruments for all attributions, (n) assessment instruments for PTSD symptoms, (o) statistical effect, and (p) main outcomes. The data was extracted by one reviewer (the first author). A second reviewer independently checked 25% of the data extraction by checking a random sample of extracted studies. A comparison of the data extracted by the two researchers showed that there were only a few differences that could be attributed to the sample data. Consensus on the differences in the extracted data was achieved through discussion.
Study Risk of Bias Assessment
The risk of bias was assessed with the Newcastle-Ottawa Scale (NOS) (Ottawa Hospital Research Institute, n.d.). The NOS is a widely used tool for assessing the quality of non-randomised studies, such as case-control and cohort studies, within systematic reviews and meta-analyses. The NOS evaluates studies in three main areas: (a) study population selection, (b) comparability of groups, and (c) determination of outcomes or exposures. The quality of all studies was assessed by the first author. A second reviewer independently checked 25% of the reviews by checking a random sample of the reviewed studies. A discrepancy was found in the quality of one study (low vs. moderate). This discrepancy in the risk of bias assessment was resolved by discussion to reach consensus. As a result of this discussion, the bias assessment of all studies was re-evaluated to ensure accuracy and consistency. Overall, this process contributed to more robust, reliable, and valid results, which ultimately improved the quality of the research assessments.
Results
Study Selection
A total of 94,051 unique eligible articles were generated from a literature search of Embase, Medline, PsycINFO, PTSDpubs, and Web of Science databases. After completing the title and abstract review for the 94,051 articles identified, 94,013 articles were excluded (1,120 manually, 92,893 by ASReview). Most articles were excluded at this stage because the titles and abstracts did not report on attributions, PTSD symptoms over time, or because the study was not longitudinal. A full-text review of the remaining 38 articles was then conducted; 22 articles were excluded because (a) the design of the studies was non-longitudinal (n = 10), (b) the studies did not examine the relationship between attributions and PTSD symptoms over time (n = 5), (c) the studies were dissertations of which the full version could not be retrieved (n = 4), (d) one study was written in a different language (non-English/non-Dutch), (e) one study turned out to be a systematic review, and (f) one study turned out to be a duplicate (the title had been changed with a subtitle). A total of 16 articles met the inclusion criteria. The full text of three of the 16 articles could not be found in the databases. The authors contacted the authors of these articles (all dissertations), but two did not respond. One author replied and sent the abstract of the article, but there did not appear to be a digital version of the article, and the hard copy was too old to scan and/or send. As a result, 13 reports were included. See Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram for a depiction of the search results at each stage (Figure 2).
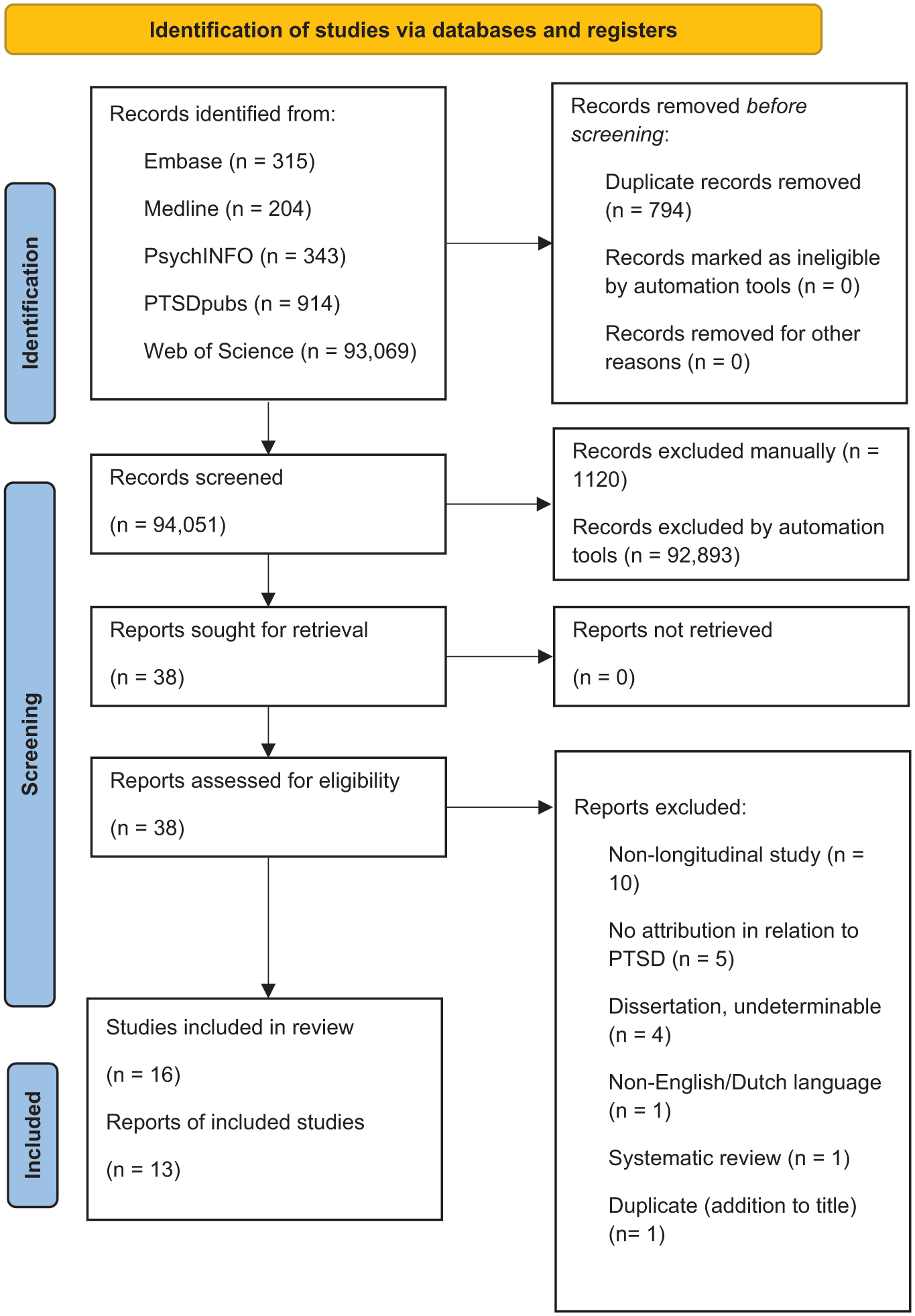
Preferred reporting items for systematic reviews and meta-analyses diagram.
Of these 13 articles, four examined associations between Weiner’s attributional dimensions and the maintenance of PTSD symptoms in different contexts, with three of these studies describing the different dimensions separately, allowing their individual effects to be examined. Five articles examined the relation between locus of control and chronic trauma-related symptoms in different contexts. Only one article examined the association between (learned) helplessness and chronic post-traumatic stress symptoms in a medical context. Eight articles examined the relation between self-blame and chronic PTSD symptoms in survivors of motor vehicle accidents or sexual assault. Note that because some articles examined multiple attribution dimensions, the total number of articles is more than 13.
Study Characteristics
Studies were published between 1988 and 2021 and included a total of 4,637 adult participants across studies. The majority of the studies (n = 8) were conducted in the United States. Most studies focused on sexual assault as the type of trauma (n = 5). In six studies, the sample consisted solely or predominantly of women, and in five studies, the sample was predominantly or mainly White. See Table 1 for a summary of participant characteristics.
Study Characteristics.
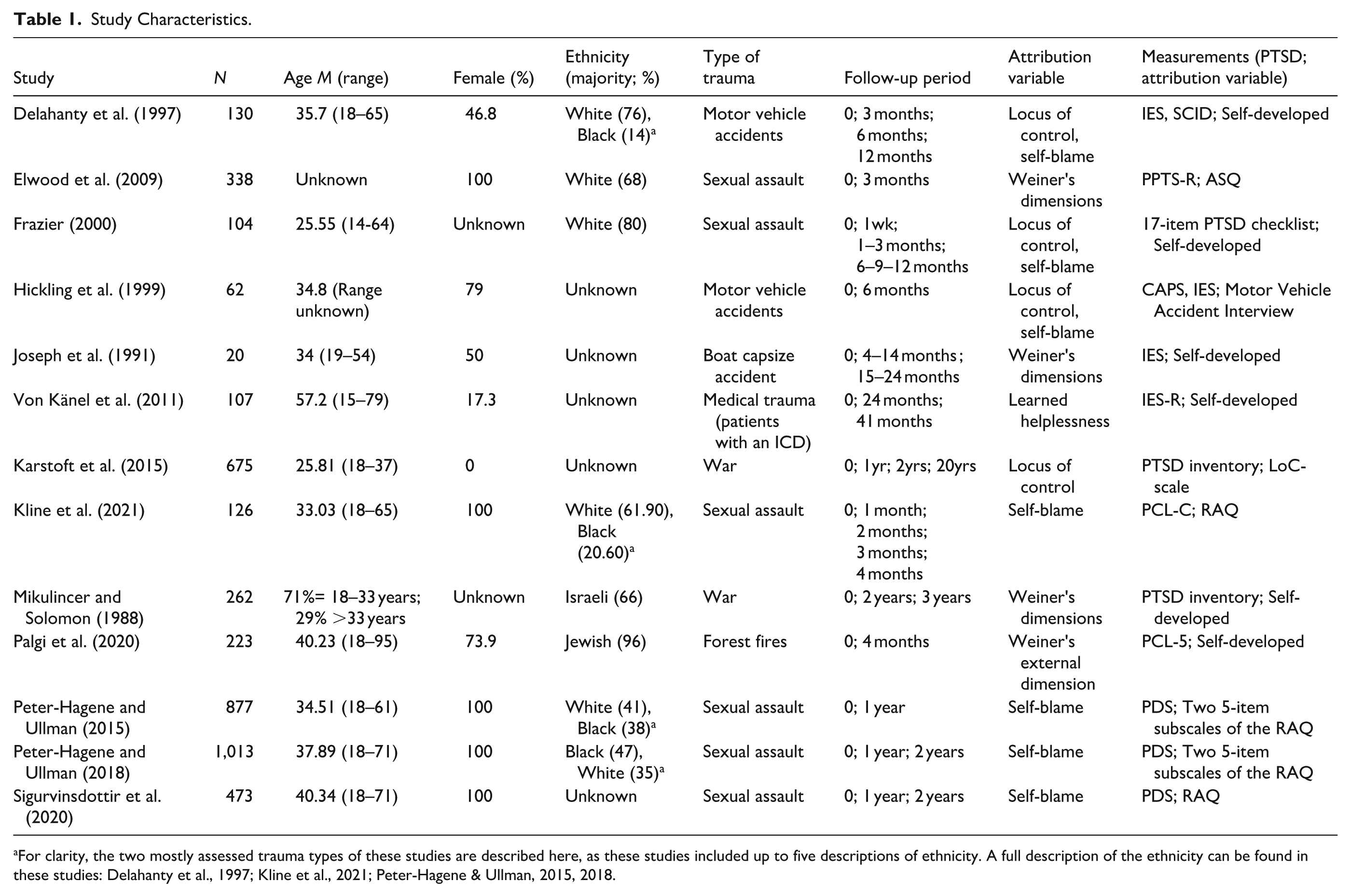
For clarity, the two mostly assessed trauma types of these studies are described here, as these studies included up to five descriptions of ethnicity. A full description of the ethnicity can be found in these studies: Delahanty et al., 1997; Kline et al., 2021; Peter-Hagene & Ullman, 2015, 2018.
All eligible longitudinal studies focused on the relationship between attributions and PTSD symptoms over time. Both the number of follow-up measures and the duration of follow-up varied significantly across the studies, ranging from 1 to 6 measurements and from 1 week to 20 years, respectively. Measurement varied across studies. Weiner’s attributions were measured in the majority of the studies with self-developed questionnaires, asking some questions about attributions related to events. Only one study used a validated self-report instrument (the ASQ; Peterson et al., 1982). Locus of control was measured with a variety of self-report questionnaires, ranging from self-developed questionnaires to validated questionnaires such as the LoC (Rotter, 1966). Learned helplessness was measured using a self-developed questionnaire. Self-blame was measured in the majority of studies using a validated questionnaire for victims of sexual violence (RAQ; Frazier, 2003); the remaining studies either used other validated questionnaires or developed their own questionnaire. Six studies used measures that assessed PTSD criteria in the third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III; American Psychiatric Association, 1987), six studies used measures that assessed PTSD criteria in the DSM-IV (American Psychiatric Association, 1994), and only one study used measures that assessed the DSM-5 (American Psychiatric Association, 2013) PTSD criteria. In most studies, PTSD was measured with a self-report questionnaire (PCL-5; Weathers et al., 2013); only three studies used a semi-structured interview to measure PTSD (CAPS; Blake et al., 1990), which is considered the gold standard for diagnosing PTSD. Both the self-report questionnaires as well as the semi-structured interview used varied considerably. The statistical tests used varied greatly across studies, although linear regression analyses and Multivariate Analyses of Variance (MANOVA) were the most commonly applied. See Table 1 for a summary of study characteristics.
Bias Assessment
Based on the Newcastle–Ottawa Scale (NOS) (Ottawa Hospital Research Institute, n.d.), the highest quality studies in this review were the studies conducted by Delahanty et al. (1997) and Hickling et al. (1999). These studies can be classified as good quality and moderate quality evidence, respectively. All other studies can be classified as low quality evidence.
Study Analyses
All the eligible longitudinal studies examined the relationship between attributions and PTSD symptoms over time. Twelve of the 13 included studies (92,3%) reported statistically significant prospective associations between attributional dimensions and PTSD symptom trajectories. This supports the relevance of attributional processes in the longitudinal course of PTSD.
Locus-Related Attribution
Eleven studies examined the impact of locus-related attributions – such as Weiner’s locus dimension, locus of control, and self-blame – on PTSD symptom severity and persistence. These studies investigated whether traumatic events were attributed to the individual’s own actions (internal) or to external factors beyond the individual’s control (external) (Delahanty et al, 1997; Elwood, Mott, et al., 2009; Frazier, 2000; Hickling et al., 1999; Joseph et al., 1991; Karstoft et al., 2015; Kline et al., 2021; Mikulincer & Solomon, 1988; Palgi et al., 2020; Peter-Hagene & Ullman, 2015, 2018; Sigurvinsdottir et al., 2020). Five studies used Weiner’s internal–external attribution dimension (Joseph et al., 1991; Mikulincer & Solomon, 1988), while three used locus of control frameworks (Delahanty et al., 1997; Hickling et al., 1999; Karstoft et al., 2015). These studies reported that external attributions were associated with a higher likelihood of chronic PTSD, particularly when the cause was human rather than natural (Palgi et al., 2020).
Six studies focused on self-blame. Frazier (2000) found that the three types of self-blame – external (attributing the cause to uncontrollable situational factors), behavioural (believing that different actions could have prevented the event), and characterological (blaming stable personal flaws) – each had detrimental effects at different points in time. Kline et al. (2021) demonstrated that behavioural self-blame was associated with negative outcomes. In contrast, Peter-Hagene and Ullman (2015, 2018) and Sigurvinsdottir et al. (2020) found that characterological self-blame had the strongest negative impact on PTSD symptoms. By contrast, two studies of motor vehicle accident survivors (Delahanty et al., 1997; Hickling et al., 1999) suggested that behavioural self-blame – defined as attributing the trauma to one’s own specific actions – was associated with fewer symptoms and a quicker recovery than blaming others.
In summary, maladaptive locus-related attributions – whether internal or external – tend to prolong and intensify trauma-related symptoms, including PTSD. Characterological self-blame and external locus of control, particularly when the external origin of the trauma is human, appear to be the most detrimental. Similar attributional patterns were observed across studies with varying sample sizes (62–1,013 participants), age ranges (18–71 years), and gender distributions, as well as across diverse trauma contexts, including sexual violence, war, and motor vehicle accidents. However, this apparent consistency should be interpreted with caution given the differences in follow-up periods, measurement instruments, and demographic and trauma-specific variables, as well as differences in age, gender, and cultural background.
Control-Related Attributions
Three studies investigated the impact of control-related attributions – such as Weiner’s controllability dimension and the concept of learned helplessness – on the persistence of trauma-related symptoms, including PTSD (Joseph et al., 1991; Von Känel et al., 2011; Mikulincer & Solomon, 1988). These studies have generally found that a lack of control (Mikulincer & Solomon, 1988) and a sense of helplessness (Von Känel et al., 2011) during the traumatic event are associated with a greater likelihood of developing more severe PTSD symptoms over time. Specifically, individuals who perceive the traumatic events as uncontrollable are more likely to experience prolonged and severe PTSD symptoms, when examined in a military context (Mikulincer & Solomon, 1988). In a medical context, helplessness was associated with more severe PTSD symptoms over time in patients with medical trauma (Von Känel et al., 2011). In contrast, Joseph et al. (1991) found that among survivors of a boat capsize accident caused by human error, higher levels of controllability attributions were associated with greater distress and PTSD symptoms. These attributions also predicted an increase in PTSD symptoms over time. The authors argued that this finding aligns with Foa et al.’s (1989) prediction that perceptions of unexercised control exacerbate PTSD symptoms (Joseph et al., 1991).
Overall, these findings suggest that maladaptive control-related attributions, such as perceived lack of control and helplessness, contribute to the persistence and severity of trauma-related symptoms, including PTSD. However, perceived control during the traumatic event does not always seem to lead to more favourable PTSD symptom development over time. If people perceive that they had the potential for control, but did not (sufficiently) exercise that control, this may lead to worse PTSD symptom development over time. These findings should be interpreted with caution due to a limited number of studies in varying contexts and limitations in sample sizes, sample diversity, varying follow-up periods, and limited use of validated measures.
Consistency-Related Attribution
One study explored the impact of consistency-related attributions, specifically Weiner’s dimensions of globality and stability, on the development of chronic PTSD and barriers to recovery (Mikulincer & Solomon, 1988). Mikulincer and Solomon (1988) found that individuals who attributed the origin of traumatic events to stable and global causes were more likely to experience chronic PTSD symptoms (Mikulincer & Solomon, 1988).
The study suggests that maladaptive consistency-related attributions, characterised by the belief that traumatic events result from stable and global causes, contribute to the persistence and severity of trauma-related symptoms, including PTSD, and create barriers to effective recovery. However, this association should be interpreted with caution as only one study examined this relationship in a specific context (military context) with limited variability in gender and ethnicity among its participants.
Negative Attributional Style
The results of one study (Elwood, Mott, et al., 2009) could not be analysed using our attribution classification because the negative attribution style assessed in the study did not clearly fit into any of our three categories. This is because, rather than focusing on specific aspects of causality, control, or consistency, the study examined a broader, more general negative attribution style of negative life events (characterised by a tendency to associate negative events with personal worthlessness and to predict further negative outcomes). In the study by Elwood, Mott, et al. (2009), negative attributional style was not found to independently predict PTSD symptom clusters over time, nor did it significantly interact with negative life events in predicting these symptoms over time. Negative attributional style thus appears to play a limited role in predicting PTSD symptoms over time. However, the relationship between negative attributional style and PTSD development over time may require a longer time frame to manifest, as the lack of association in this study could also be due to the short 3-month follow-up period (Elwood, Mott, et al., 2009).
Discussion
This systematic review examined the role of causal attributions in the maintenance and recovery of trauma-related symptoms, specifically post-traumatic stress disorder (PTSD). The primary aim was to consolidate existing evidence on how causal attributions of traumatic events influence PTSD symptoms. We hypothesised that locus-related attributions (including Weiner’s dimension of locus, external locus of control, and self-blame), control-related attributions (Weiner’s dimension of controllability and learned helplessness), and consistency-related attributions (Weiner’s dimensions of globality and stability) contribute to chronic PTSD and hinder recovery. Our results show that maladaptive attributions – whether related to locus, control, or consistency – play a significant role in the exacerbation of PTSD symptoms and the impairment of recovery. An external locus of control with another person, as well as internal characterological self-blame, appeared to be maladaptive. In addition, both low levels of experienced control and control options that were not (sufficiently) exercised, and high levels of perceived consistency, seemed to be maladaptive. This integrated analysis highlights the complex role of attributions in trauma-related symptom severity and recovery.
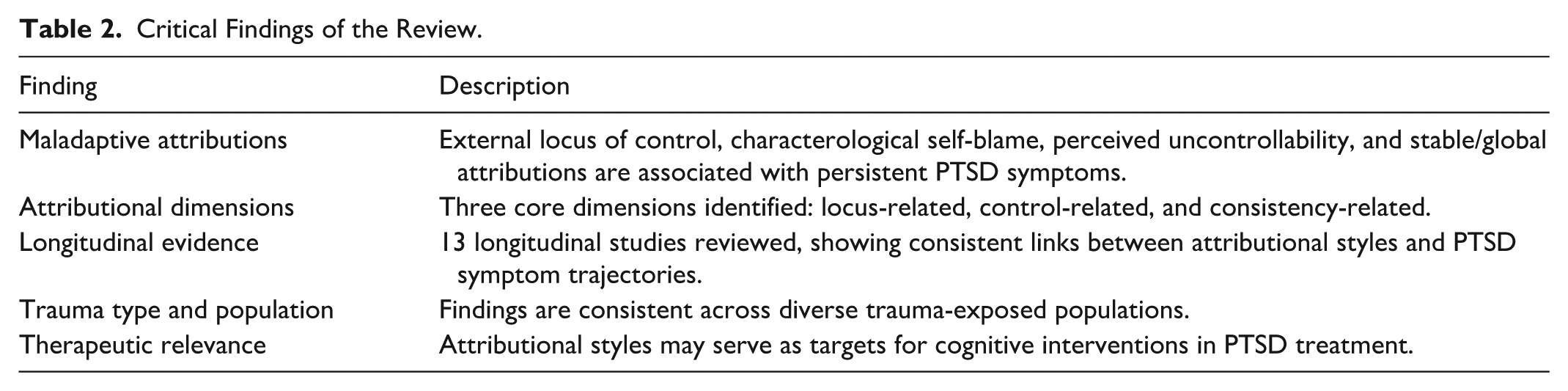
To better understand how these cognitive patterns may influence recovery, it is important to consider the psychological mechanisms through which they operate. Characterological self-blame appears particularly detrimental, as it can evoke negative emotions such as shame and guilt. These emotions can deepen the impact of trauma and hinder therapeutic engagement. By contrast, behavioural self-blame, which focuses on specific actions rather than the self’s core identity, can foster a sense of agency and facilitate recovery. External attributions, particularly when the trauma is caused by another person, can intensify feelings of injustice and unpredictability, potentially reinforcing feelings of helplessness. Similarly, stable and global attributions may contribute to feelings of hopelessness by framing the trauma as permanent and pervasive. An overview of the critical findings across attributional dimensions and their associations with PTSD symptom trajectories is presented in Table 2.
Critical Findings of the Review.
Our findings are consistent with previous research (e.g. Massad & Hulsey, 2006) suggesting that attributional dimensions play a critical role in the maintenance of trauma-related symptoms. For instance, individuals who blame themselves for their trauma (locus-related attribution) (e.g. Seah & Berle, 2022), perceive the trauma as unchangeable (consistency-related attribution) (e.g. Gray et al., 2003; Reiland et al., 2014; Zinzow & Jackson, 2009), and believe it signifies a broader sense of helplessness (control-related attribution) (e.g. Hancock & Bryant, 2018; Salcioglu et al., 2017) are more likely to experience enduring PTSD symptoms. These findings provide valuable insights into the cognitive mechanisms underpinning PTSD, shedding light on why some individuals develop chronic trauma-related symptoms, including PTSD.
Considerations in Understanding the Role of Attributions in PTSD
A consideration in understanding the relationship between causal attributions and PTSD is the perceived controllability and changeability of, and responsibility for, traumatic experiences. These perceptions significantly shape an individual’s cognitive and emotional response to trauma, influencing the severity and persistence of symptoms and the trajectory of recovery (Carlson & Dalenberg, 2000). When individuals perceive their trauma as uncontrollable and unchangeable, they may experience a profound sense of hopelessness (Levi et al., 2012). This belief can lead to a cycle of emotional and behavioural stagnation in which the person feels powerless to change their circumstances or reduce their distress (Collins & Cutcliffe, 2003). In such cases, recovery efforts are hampered by a lack of motivation or belief in the possibility of improvement. For individuals who experience high levels of perceived loss of control or unchangeability, these perceptions can exacerbate PTSD symptoms and hinder recovery by fostering hopelessness and stagnation.
Similarly, perceptions of responsibility for the trauma are central to how individuals process their experiences and develop coping strategies (Delahanty et al., 1997). Self-blame, a common attribution among people with PTSD, can take several forms, each with different implications for the symptom severity of trauma-related symptoms, including PTSD. Characterological self-blame, in which individuals blame their inherent characteristics or perceived faults for the traumatic event taking place, is particularly damaging. This form of attribution reinforces feelings of shame, worthlessness, and inadequacy, often leading to chronic PTSD symptoms and an increased risk of comorbid conditions such as depression. On the other hand, behavioural self-blame for the traumatic event taking place, which involves attributing the trauma being (partly) due to one’s specific actions or choices, can provide a sense of agency and promote learning from past experiences, potentially aiding recovery when combined with self-compassion (Janoff-Bulman, 1979). For individuals who experience high levels of responsibility, the way they attribute responsibility for the trauma has a significant impact on their PTSD symptoms and recovery.
A noteworthy finding in our review is that a human cause for traumatic events negatively affects the course of PTSD symptoms (e.g. Palgi et al., 2020), presumably due to a perceived loss of control. When someone else takes control, the individual loses their own sense of control and feels powerless to change the situation. This perceived lack of control significantly increases the negative impact on PTSD symptoms. Combined with intentional harm, this can lead to complex emotional reactions that further impede recovery and prolong distress (Frazier, 2003).
Towards a More Thorough Understanding of Attributions in PTSD
In this review, we present a theoretical reclassification of attributions, specifically in the context of causal attributions of traumatic events, to provide a more thorough understanding of their role in PTSD symptomatology. The complexity of the relationship between attributions of traumatic events and PTSD necessitates this theoretical reclassification, as the impact of attributions varies depending on factors such as the type of attribution, the nature of the trauma, and individual characteristics. For example, the same type of attribution – internal or external – may have very different effects depending on whether it focuses on personal characteristics (such as self-blame) or external circumstances (such as victimisation by another person), or whether it is perceived as a stable or changeable factor. This reclassification transcends the simplistic internal–external dichotomy by considering who is blamed, for what, and when.
The proposed reclassification into attributions related to locus of control and consistency was informed by a synthesis of the reviewed studies. Although the original studies employed different attributional frameworks, such as Weiner’s dimensions, locus of control theory, and trauma-specific constructs, we identified conceptual categories that extend beyond the classic Weiner dimensions. The attributional constructs were then grouped into broader thematic categories based on their theoretical function and their empirical association with PTSD symptom trajectories. This ensured coherence and consistency across the reclassification.
The review highlights the need to further refine the theoretical reclassification by including subcategories. Specifically, within the main category of locus, we recommend distinguishing between causes that are natural and those that are human-induced for external locus. Therefore, the subcategory intentionality (‘unintentional’ vs. ‘intentional’) is added. For internal locus, the subcategory responsibility (‘behavioural responsibility’ vs. ‘characterological responsibility’) is added to distinguish between self-blame related to one’s own actions and self-blame related to one’s own characteristics. Furthermore, within the main category of control during the traumatic event, the subcategory applied control (‘exercised control’ vs. ‘control not exercised’) for controllability is included to distinguish between situations where control was exercised and those where the individual perceives that they failed to exercise control that they did have. With this refined reclassification, we can more accurately determine which factors are critical for the development of PTSD symptoms over time, while providing a more thorough understanding of the factors that underpin the attribution process of traumatic experiences. Figure 2 provides a schematic overview of the refined reclassification of causal attributions of traumatic events as proposed in the current review.
In light of a more thorough understanding of causal attributions of traumatic events, we also propose a more nuanced interpretation of the dichotomies, in which attributions are conceived more as independent and can be complementary rather than mutually exclusive. That is, rather than viewing attributions strictly as internal or external, we recognise that individuals may hold both types of attributions simultaneously, to varying degrees. For example, a person may attribute a traumatic event partly to their own actions (internal attribution) and partly to external circumstances or other people (external attribution). This interpretation of attributions recognises the complexity of human cognition by allowing conceptually opposite attributions to co-exist within an individual. It may also allow for a more accurate understanding of how people interpret and respond to traumatic events. Rather than viewing attributions as opposite poles on a single continuum, we should recognise each dimension as existing in their own right. This allows us to better appreciate the interplay between different types of attributions and how they collectively influence psychological outcomes.
In summary, we propose a refined reclassification for understanding causal attributions of traumatic events, emphasising their complexity and role in PTSD. This refined reclassification may advance attribution theory within trauma psychology by offering a more refined understanding of how attributions shape the psychological processes involved in recovery from trauma-related symptoms, including PTSD.
Limitations
Several methodological limitations were identified that may have influenced the findings. Firstly, no longitudinal studies examined how attributional styles affect the long-term effectiveness of trauma-focused treatments. Moreover, the role of causal attributions in shaping treatment outcomes remains unclear. Similarly, only one study addressed learned helplessness longitudinally, highlighting a significant knowledge gap regarding its impact on PTSD symptom trajectories.
Secondly, the included studies showed considerable heterogeneity in terms of the types of trauma and the populations studied. Most studies focused on sexual assault or motor vehicle accidents, with limited representation of other trauma types, such as combat, natural disasters, and childhood abuse. The samples were predominantly female and White, which limits the generalisability of the results to more diverse populations.
Thirdly, most studies relied on self-developed, unvalidated measures of both attributions and PTSD symptoms. Only one study used a validated attribution instrument (ASQ), and PTSD was typically assessed via self-report rather than structured clinical interviews. Furthermore, many studies employed outdated diagnostic criteria (DSM-III or DSM-IV), small sample sizes, and short or inconsistent follow-up periods ranging from one week to twenty years, often with only one or two measurement points. These factors limit the comparability and validity of the findings, hindering conclusions about long-term symptom trajectories.
Finally, while this review adhered to PRISMA guidelines, the majority of the screening and data extraction was conducted by a single reviewer, which may have introduced selection bias. Excluding non-English and non-Dutch studies may have limited the scope further. Despite an initial pool of over 1,500 records, only 13 studies met the inclusion criteria. This suggests that either the search strategy was rather broad, or the inclusion criteria were rather restrictive. Furthermore, the methodological quality of the included studies was limited in several ways, including inadequate control for confounders and difficulties in ensuring group comparability.
These limitations highlight the need for future longitudinal research that uses validated instruments, has consistent follow-up intervals, and includes more diverse trauma populations, in order to clarify how attributional processes shape PTSD development and recovery.
Clinical Implications
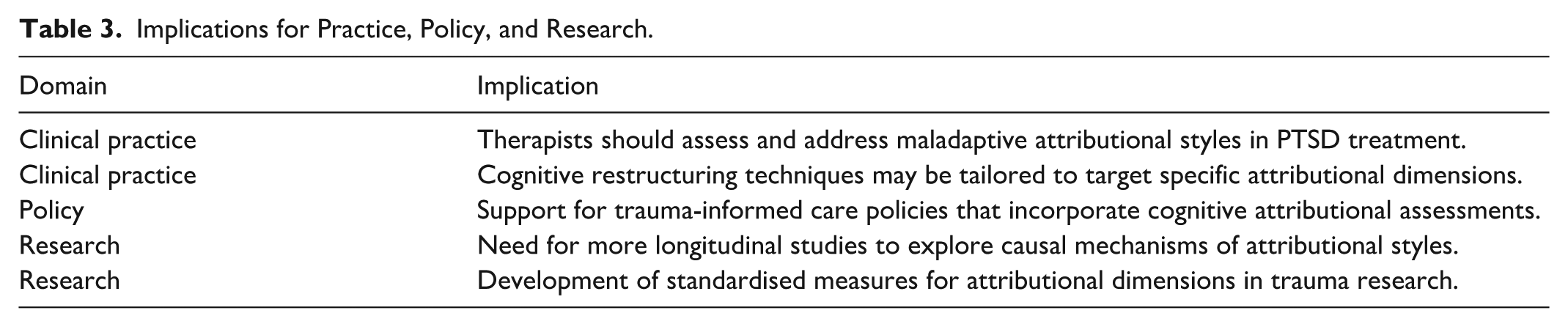
This review emphasises the clinical importance of attributional styles in the development and maintenance of PTSD symptoms. Maladaptive attributions, such as interpreting trauma as being caused by uncontrollable, external, stable or global factors, are consistently linked to prolonged distress and may undermine the efficacy of treatment. Such attributions can exacerbate feelings of helplessness (Brown & Siegel, 1988; Reiland, 2017) and encourage avoidance behaviours (Carlson & Dalenberg, 2000). In addition, locus-related attributions, including self-blame or blaming external forces, can intensify emotional distress and impede therapeutic progress (Ullman, 1997). While such attributional styles pose challenges, they also present clinical opportunities: identifying and modifying these attributions can promote psychological growth and improve treatment outcomes (Massad & Hulsey, 2006). Future research should examine how shifts in attributional patterns influence recovery trajectories across diverse populations, thereby informing targeted interventions and advancing our understanding of PTSD mechanisms. Table 3 summarises the practical, policy-related, and research implications derived from the findings of this review.
Implications for Practice, Policy, and Research.
Future Research Directions
Future research should aim to address existing gaps by conducting longitudinal studies that investigate the role of attributions in PTSD symptom trajectories and treatment outcomes. For example, it would be beneficial to examine how the nuanced view of locus attributions that we propose (independency approach) is helpful in better understanding how causal attributions of traumatic events influence PTSD symptoms and recovery. Specifically, it would allow us to investigate whether an individual who attributes a traumatic event partly to their own actions and partly to external circumstances or other people recovers more effectively and reports fewer PTSD symptoms following trauma-focused treatment than an individual who attributes a traumatic event entirely to their own actions or entirely to external circumstances or other people. The independency approach suggests that individuals can perceive the causes of their trauma as a combination of personal actions and external factors. This approach may allow for a more balanced understanding of the event, potentially leading to better coping strategies and more effective recovery. On the other hand, the opposite poles on a continuum approach assume that the trauma is attributed to either purely internal factors (e.g. self-blame) or purely external factors (e.g. blaming others or circumstances). If therapists approach clients’ attributions for trauma from this perspective, this may limit an individual’s ability to engage in a nuanced understanding of their traumatic experience, which could hinder emotional processing and integration, and may result in less effective recovery and more persistent PTSD symptoms. By exploring this potentially valuable new independency approach to locus attributions, researchers can gain insights into how unique elements in understanding and explaining traumatic events affect the effectiveness of trauma-focused treatment. This knowledge could help tailor therapeutic approaches to better support individuals based on their attributional styles, ultimately improving treatment outcomes and reducing PTSD symptoms.
Lastly, researchers should investigate how attributional styles interact with treatment modalities in order to develop more tailored approaches for individuals with specific cognitive profiles, particularly in the context of trauma-related symptoms, including PTSD. Such research could pave the way for more personalised, effective PTSD treatments that focus on attributional patterns and their role in trauma recovery.
Conclusion
The systematic review highlights the significant influence of causal attributions in the maintenance and recovery of trauma-related symptoms, particularly PTSD. By reclassifying the classic dimensions of causal attribution proposed by Weiner (1986) and integrating other attributional tendencies, the review offers a more thorough understanding of how individuals perceive and interpret traumatic events. This refined reclassification into locus, control, and consistency attributions and their subcategories clarifies the complex relation between different types of attributions and their impact on PTSD symptomatology. The findings suggest that maladaptive attributions, whether locus-related, control-related, or consistency-related, contribute significantly to the persistence and severity of trauma-related symptoms, including PTSD. The suggestion that different attributions within one attribution type (i.e. locus) may operate independently rather than only attribution at one position along the locus continuum is possible provides a more comprehensive perspective. Recognising that individuals may hold both internal and external locus attributions simultaneously allows for a more accurate understanding of how people interpret and respond to traumatic events, particularly in the context of PTSD. This independency approach acknowledges the complexity of human cognition. By integrating these findings, the review advances attribution theory within trauma psychology and offers valuable implications for future research and clinical practice. Targeted therapeutic interventions that address maladaptive attributional styles may have the potential to improve treatment effectiveness and, ultimately, recovery outcomes for individuals with trauma-related symptoms, including PTSD.
Footnotes
Acknowledgements
The author(s) would like to express their sincere gratitude to Dr. Monique A.M. Zeegers and Laura N. Alders of Radboud University for their invaluable contributions to this review. Their insightful feedback greatly enhanced the quality of this study. We are very grateful for their support and collaboration throughout the project.
Ethical Considerations
This study is a systematic review of previously published research and did not involve the collection of new data from human participants. Therefore, this review did not require ethical approval. All the included studies were peer-reviewed and are assumed to have obtained appropriate ethical approval with the standards and guidelines of their respective institutions.
Consent to Participate
As this study is based exclusively on previously published research and did not involve direct interaction with human participants, obtaining informed consent was not applicable. It is assumed that the original studies included in the review secured informed consent from participants in line with institutional and ethical requirements.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This study is a systematic review and does not involve the generation of new data. All the data analysed in this review were extracted from previously published studies, which are cited in the reference list. The datasets supporting the conclusions of this article are available in the original publications.
Statement on Identifying Information
This manuscript does not contain any identifying information related to the authors, their institutions, funders, or approval committees that could compromise anonymity during the peer-review process.