
Abstract
Adverse childhood experiences (ACEs) are significant risk factors affecting neurobiological, emotional, and behavioural development across the lifespan. While extensively studied, the interplay between ACEs and individual characteristics such as temperament remains underexplored. This scoping review systematically mapped evidence on the relationship between ACEs, temperament dimensions, and developmental outcomes. Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews guidelines, searches were conducted in PubMed, Scopus, Web of Science, and EBSCOhost. Studies published between 1998 and 2025 in English, Portuguese, or Spanish, including those involving children and adolescents up to 18 years old, were eligible. From 1,505 records, 19 studies met the inclusion criteria, totalling 22.375 participants, mostly from the United States and using longitudinal designs. Findings indicate that temperamental traits, particularly inhibitory control, emotional reactivity, and negative affectivity, are implicated in the association between ACEs and outcomes such as externalizing behaviours, anxiety, executive functioning deficits, attention-deficit/hyperactivity disorder symptoms, and personality disorder features, with existing studies examining these traits as potential mediators or moderators. Most studies applied diathesis-stress models, with limited use of differential susceptibility theory (DST), which considers “for-better-and-for-worse” effects depending on environmental quality. This gap limits understanding of developmental plasticity and individual differences in susceptibility. Future research should adopt longitudinal, culturally diverse, DST-aligned designs, examining temperament as both vulnerability and plasticity markers to enhance understanding and guide interventions for children exposed to early adversity.
Introduction
Childhood and adolescence are widely recognized as critical developmental periods in which early experiences exert a lasting influence on psychological and relational functioning. Increasing evidence suggests that development is shaped by a continuum of environmental experiences, encompassing both adverse and positive exposures. Research on positive childhood experiences indicates that supportive and nurturing early environments are associated with better mental health, lower levels of anxiety and depression, and greater psychological resilience, even among individuals exposed to adversity (Bethell et al., 2019; Kocatürk & Çiçek, 2023; Şanli et al., 2024). These findings highlight the foundational role of early-life contexts in shaping developmental trajectories. Within this broader framework, adverse childhood experiences (ACEs) have been identified as particularly potent risk factors due to their cumulative and often chronic nature, and have therefore been the primary focus of research examining pathways to maladaptive developmental outcomes.
ACEs affect a substantial proportion of the population worldwide. Global estimates suggest that more than half of adults have experienced at least one ACE during childhood (World Health Organization, 2020), while data from the United States indicate that up to 61% of adults report exposure to at least one ACE (Centers for Disease Control and Prevention, 2016). Recognized as a major public health concern, ACEs are strongly associated with a wide range of negative developmental, psychological, and health outcomes across the lifespan. ACEs refer to a broad range of stressful, potentially harmful, and traumatic experiences during childhood, often within the family setting, such as parental separation or divorce, domestic violence, and various forms of abuse or neglect—emotional, physical, or sexual (Dong et al., 2004; Felitti et al., 1998). However, recent research has broadened this definition, acknowledging that adversity can also stem from outside the home. Experiences such as community violence, bullying, racial or ethnic discrimination, persistent poverty, housing insecurity, and forced migration or refugee status are now recognized as equally impactful forms of childhood adversity (Folayan et al., 2023; Lee et al., 2017). This expanded perspective highlights the complex and multidimensional nature of ACEs, recognizing that adverse experiences embedded in diverse social and structural contexts can have a profound impact on developmental trajectories. Although not all adverse experiences are necessarily traumatic, many ACEs do involve exposure to events that may be experienced as traumatic, depending on their severity, duration, the child’s developmental stage, and the presence of protective relationships. Thus, trauma refers to the psychological and emotional response to events that pose actual or perceived threats to a child’s physical or emotional safety, such as abuse, serious harm, or exposure to violence, and typically elicits intense reactions of fear, helplessness, or horror (Carlson & Dalenberg, 2000; Dalenberg et al., 2017).
When ACEs occur in early developmental periods, they may disrupt core processes involved in emotional regulation, interpersonal trust, and cognitive functioning, potentially compromising a child’s capacity to navigate future challenges and relationships (Sciaraffa et al., 2018; Sege & Harper Browne, 2017). On a neurobiological level, the ACEs have been shown to affect brain areas responsible for emotional regulation, stress response, and decision-making, including the amygdala, hippocampus, and prefrontal cortex (Herzog & Schmahl, 2018; Weems et al., 2021). According to the neurobiological model, prolonged exposure to high-stress environments can lead to a heightened activation of the amygdala, which controls the fight-or-flight response, while simultaneously reducing the regulatory control of the prefrontal cortex (Ryznar et al., 2025). This imbalance can result in increased emotional reactivity, difficulties with impulse control, and a tendency to perceive social interactions as threatening, often affecting different areas of one’s temperament (Dollar et al., 2023; Sanson et al., 2004). At a mechanistic level, early adversity has been shown to impact multiple neural and physiological systems that support emotional regulation and temperament. Specifically, exposure to stress in early life is associated with alterations in the hypothalamic-pituitary-adrenal axis, leading to dysregulated stress responses that may persist across development (Gunnar & Quevedo, 2007; McLaughlin et al., 2014). Concurrently, children exposed to adversity often exhibit heightened amygdala reactivity to emotional stimuli, reflecting increased sensitivity to threat (Tottenham, 2009). These changes are frequently accompanied by delayed maturation and altered connectivity of prefrontal regulatory networks, which are critical for top-down control of emotion (Gee et al., 2013). Together, these neurobiological adaptations contribute to stable patterns of emotional reactivity and self-regulation, shaping temperament traits that can influence behaviour and risk for psychopathology throughout life.
The cumulative ACE theory highlights that ACEs are not isolated but build up over time, intensifying their impact on development and health outcomes (Hakamata et al., 2022). Research demonstrates that the accumulation of ACEs increases the risk of poor mental health, physical health challenges, and social difficulties, creating a “dose–response” relationship between the number of ACEs and the severity of outcomes (Tan & Mao, 2023). This compounding effect emphasizes the importance of addressing multiple adversities rather than focusing solely on individual events (Hakamata et al., 2022).
These ACEs can lead to different negative outcomes throughout an individual’s life, affecting mental health and relationships that may persist into adulthood (Daines et al., 2021). For example, children who undergo stressful or traumatic experiences may grow up struggling to trust others and showing higher levels of impulsivity. (Shain et al., 2022). From the cumulative ACEs perspective, these challenges also interact with neurobiological changes, creating a feedback loop where early difficulties compound vulnerabilities, increasing susceptibility to psychopathological symptoms like anxiety, depression, or aggression in adulthood (Hawes & Allen, 2023; Kobrinsky & Siedlecki, 2023). Recognizing the impact of early adversity and the neurobiological changes it may bring is essential, not only to understand these individuals’ difficulties but also to inform interventions for people who undergo these experiences (Ellis et al., 2022). Early adversity can lead to neurobiological alterations that, when combined with an individual’s inherent biological susceptibility, increase the risk for negative developmental outcomes (Ellis et al., 2022; Hakamata et al., 2022). Temperament may serve as a behavioural indicator of this susceptibility, with certain profiles being more prone to manifestations such as heightened anxiety, aggression, or emotional dysregulation (Blader et al., 2025; Carmassi et al., 2022).
Temperament
Previous studies have tested the link between ACE and outcomes using linear dose-response models (Anda et al., 2020; Briggs et al., 2021). However, recent evidence has suggested that the effects of cumulative adversity on the developing child may not be linear (Tan & Mao, 2023; Wilson-Genderson et al., 2022), considering certain classes of ACE may interact synergistically with the environment to significantly increase the overall risk beyond the simple accumulation of ACE (Briggs et al., 2021; Lanier et al., 2018). Differential susceptibility theory (DST; Belsky, 1997; Belsky & Pluess, 2009) proposes that individuals differ in their biologically based sensitivity to environmental influences. Unlike diathesis stress models, which emphasize vulnerability only under adverse conditions, DST argues that the same traits that increase risk in negative environments can also enhance developmental benefits in supportive contexts, a “for-better-and-for-worse” pattern.
Empirical work supports DST across temperament, genetic, and physiological domains. Highly reactive or low effortful control children exhibit more behavioural problems under harsh parenting but also show greater social, emotional, and cognitive gains when exposed to warm and structured caregiving (Kiff et al., 2011; Pluess & Belsky, 2013; Slagt et al., 2017). Genetic sensitivity markers (e.g., DRD4-7R, 5-HTTLPR) and neurobiological indicators such as heightened cortisol or autonomic reactivity (Boyce & Ellis, 2005) show similar patterns, predicting both heightened vulnerability and enhanced responsivity to supportive environments. For instance, studies have shown that children carrying the DRD4-7R allele are more susceptible to both negative and positive parenting practices (Bakermans-Kranenburg & Van Ijzendoorn, 2011), and that autonomic reactivity moderates children’s behavioural adaptation in both supportive and adverse contexts (Obradović et al., 2010).
Despite this evidence, most ACE, temperament studies continue to adopt diathesis stress frameworks, focusing solely on adverse environments.
Temperament is a key factor in studying environmental sensitivity (Pluess et al., 2023). Temperament refers to biologically based individual differences in emotionality, activity levels, and sociability, characteristics that emerge early in life and exhibit moderate stability over time. Genetic influences shape these temperamental characteristics and form the foundation for later personality development (Rothbart et al., 2011).
From a developmental psychopathology perspective, developmental outcomes are understood to emerge from dynamic and transactional interactions between individual characteristics and environmental contexts across time (Hawes & Allen, 2023). This framework emphasizes that risk and adaptation are not solely determined by exposure to adverse experiences, but rather by how such experiences interact with biologically and psychologically based individual differences throughout development. Accordingly, the impact of early adversity is shaped by timing, chronicity, and the presence of moderating individual factors, which together influence developmental trajectories across childhood and adolescence.
Within this framework, temperament can be conceptualized as a biologically based, individual-level marker of vulnerability and/or plasticity that shapes children’s sensitivity to environmental influences (Hartman & Belsky, 2016). From a differential susceptibility perspective, temperamental traits associated with heightened reactivity or reduced self-regulation may amplify risk in adverse contexts while also conferring increased responsiveness to supportive or enriched environments (Belsky & Pluess, 2009). Accordingly, ACEs are conceptualized as salient environmental stressors, whereas temperament represents a core individual characteristic that may influence both the magnitude and direction of developmental outcomes, either by intensifying maladaptive pathways or by modifying individual responses to adversity (Ellis et al., 2022).
Similarly, C. Robert Cloninger proposed a psychobiological model of temperament, identifying central dimensions such as novelty seeking, harm avoidance, reward dependence, and persistence. Cloninger’s model emphasizes the genetic and neurobiological bases of these characteristics, suggesting that temperament is strongly linked to the structure and function of the nervous system, thus reflecting the complex interaction between biological and behavioural aspects (Cloninger, 2008; Cloninger et al., 1993). Other authors have also contributed to the definition of temperament. Derryberry and Rothbart broadened the understanding of temperament by specifying the concepts of reactivity and self-regulation as central elements in its formation (Lamb & Brown, 2013). For Buss and Plomin (1984), temperament is something determined in the first years of life, with a strong hereditary nature, suggesting that temperamental bases can be traced from the earliest stages of development (Plomin & Dunn, 2013). Currently, the most widely accepted definition of temperament is that it is about individual differences that emerge early in life and tend to remain relatively constant throughout life, with evidence suggesting a persistence of certain temperamental characteristics (Wilson & Olino, 2021). These temperamental characteristics play a fundamental role in shaping personality, influencing both adaptive and maladaptive behaviours throughout the life cycle (Pekdoğan & Kanak, 2022). These perspectives illustrate the multifaceted nature of temperament, which encompasses the biological, psychological, and behavioural dimensions.
As previously discussed, theories such as differential susceptibility and biological sensitivity to context suggest that temperament influences individuals’ sensitivity to environmental influences, shaping their responses to both adversity and supportive conditions. Empirical research on ACEs further reinforces this perspective, showing that early adversity interacts with temperament to influence developmental and psychological outcomes, either intensifying risks or fostering resilience.
Despite this strong theoretical and empirical foundation, there is currently no scoping review that systematically maps the relationship between temperament, adversity, and outcomes. Given the importance of understanding these interactions, a comprehensive synthesis of existing research is necessary to clarify the nature, direction, and mechanisms underlying the relationship between ACE and temperament across developmental stages. This scoping review aims to map and synthesize the existing scientific evidence on the relationship between ACEs and temperament, and its associations with developmental outcomes.
Methods
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (Tricco et al., 2018). The final search was completed on January 31, 2025. The review was not prospectively registered, as its primary aim was to provide an exploratory mapping of an emerging and heterogeneous body of literature, consistent with the methodological objectives of scoping reviews.
Search Strategy
A scoping review was conducted to map evidence on the relationship between ACEs and/or traumatic events, temperament dimensions, and associated outcomes. Searches were performed in PubMed, Scopus, Web of Science, and EBSCOhost-hosted databases, complemented by manual screening of reference lists to minimize publication bias. Search terms were constructed using Boolean operators (“AND,” “OR”) and limited to studies in English, Portuguese, or Spanish. The complete list of terms is available in Appendix A.
Study Selection
Inclusion criteria comprised studies that: (a) assessed ACEs and/or trauma; (b) involved participants <18 years or provided separate analyses for this group; (c) examined temperament dimensions; (d) were peer-reviewed; and (e) published between 1998 (the seminal ACE study; Felitti et al., 1998) and 2025. For studies with pregnant women, only those linking maternal adversity to postnatal child temperament were included. Additionally, to ensure methodological rigor and comparability across studies, we included only studies that employed psychometrically validated or widely used assessment instruments developed to measure for at least one of the following domains: ACE exposure, temperament, or developmental/mental health outcomes. Examples of accepted validated measures included the Childhood Trauma Questionnaire (CTQ), the ACEs Questionnaire, the Child Behavior Checklist (CBCL), validated temperament scales (e.g., the EAS, IBQ-R, CBQ), and other instruments with established psychometric support.
Studies in which temperament-like constructs were derived from administrative or risk/needs assessment tools (e.g., probation or recidivism risk instruments) rather than from validated temperament or personality measures were excluded, even when such constructs were labelled as “effortful control” or “negative emotionality.” Studies that assessed ACEs or temperament using non-validated, ad hoc items or unclear measurement procedures were also excluded. Moreover, studies were eligible if the operationalization of ACEs was clearly defined (e.g., maltreatment, household dysfunction, community violence), regardless of whether cumulative indices or single-domain measures were used, provided that measurement quality met minimum methodological standards. Eligible study designs included longitudinal, cross-sectional, and prospective cohort studies.
Exclusion criteria covered studies not addressing the research variables, lacking empirical data, or published in other languages. Studies using inadequate designs were excluded, such as case reports or studies providing insufficient methodological detail (e.g., unclear measurement procedures, undefined operationalization of ACEs or temperament, or analytic strategies that did not allow examination of associations between adversity, temperament, and outcomes). Duplicates were removed.
Screening of titles and abstracts, followed by full-text screening, was conducted according to Cochrane Collaboration recommendations (Cumpston et al., 2022) using Rayyan (Ouzzani et al., 2016). Two reviewers independently screened titles, abstracts, and full texts; discrepancies were resolved by discussion. Interrater agreement coefficients (e.g., Cohen’s κ) were not calculated as disagreements between reviewers were resolved through discussion until consensus was reached.
Data Collection Process
Data were extracted through a standardized form. A total of 1,505 records were identified; after duplicate removal, 253 underwent screening. Of these, 234 full texts were excluded for reasons including: no assessment of ACE–temperament relationship (n = 112), non-empirical publications (n = 34), contextual/theoretical only (n = 19), inadequate populations (n = 10), irrelevant or unreported outcomes (n = 24), inadequate designs (n = 14), insufficient relational assessment (n = 8), language restrictions (n = 8), and duplicate entry (n = 1; Figure 1). To ensure consistency and accuracy, the data extraction form was pilot-tested prior to use.
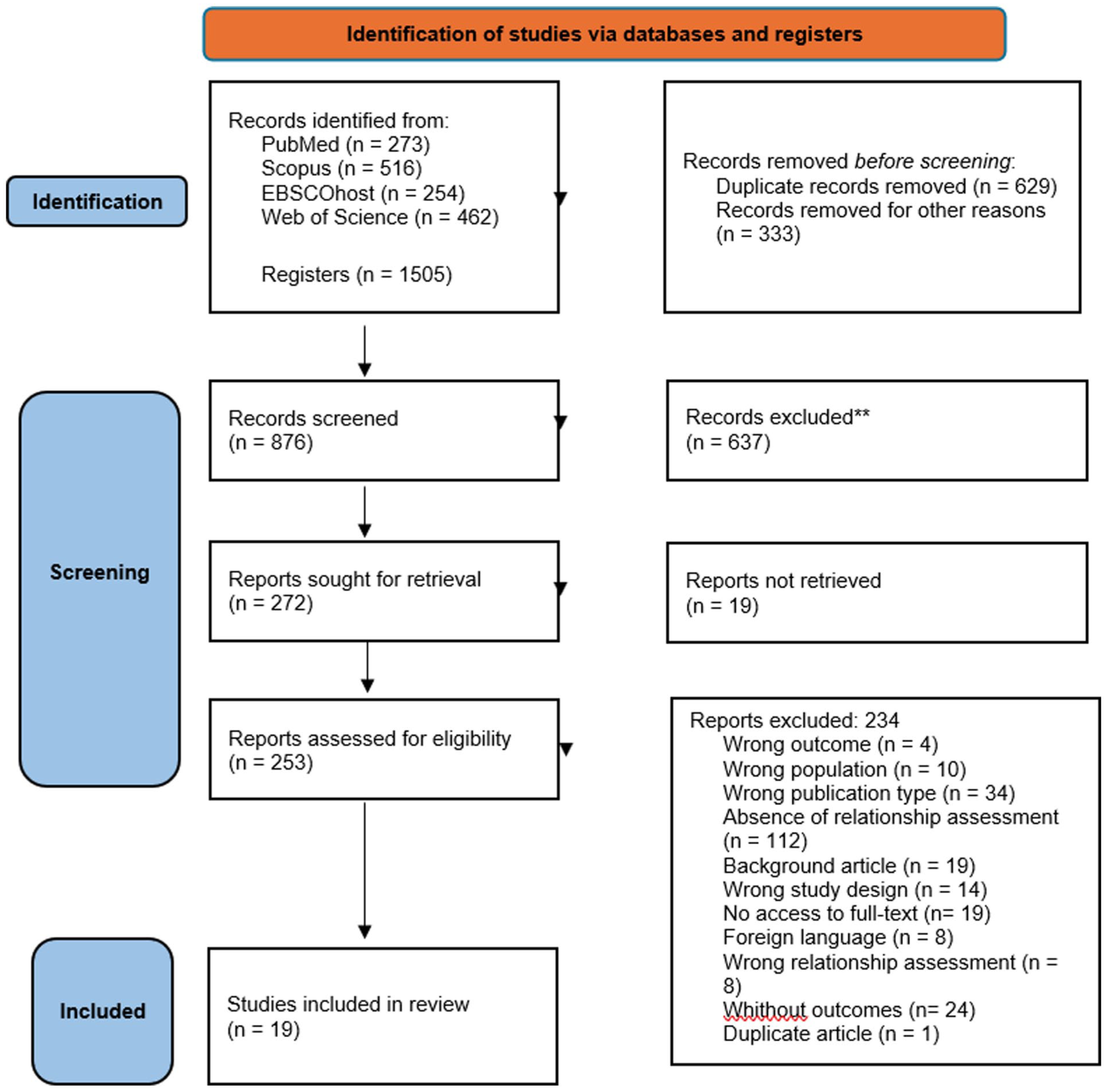
Flowchart of the screening process (following PRISMA).
Results
Study Characteristics
The extracted data included study characteristics (e.g., author, year, location, sample size), population details (e.g., age, gender), methods used to assess adversity/trauma and temperament, and key findings or outcomes (as listed in Table 1).
Characteristics of Included Studies.
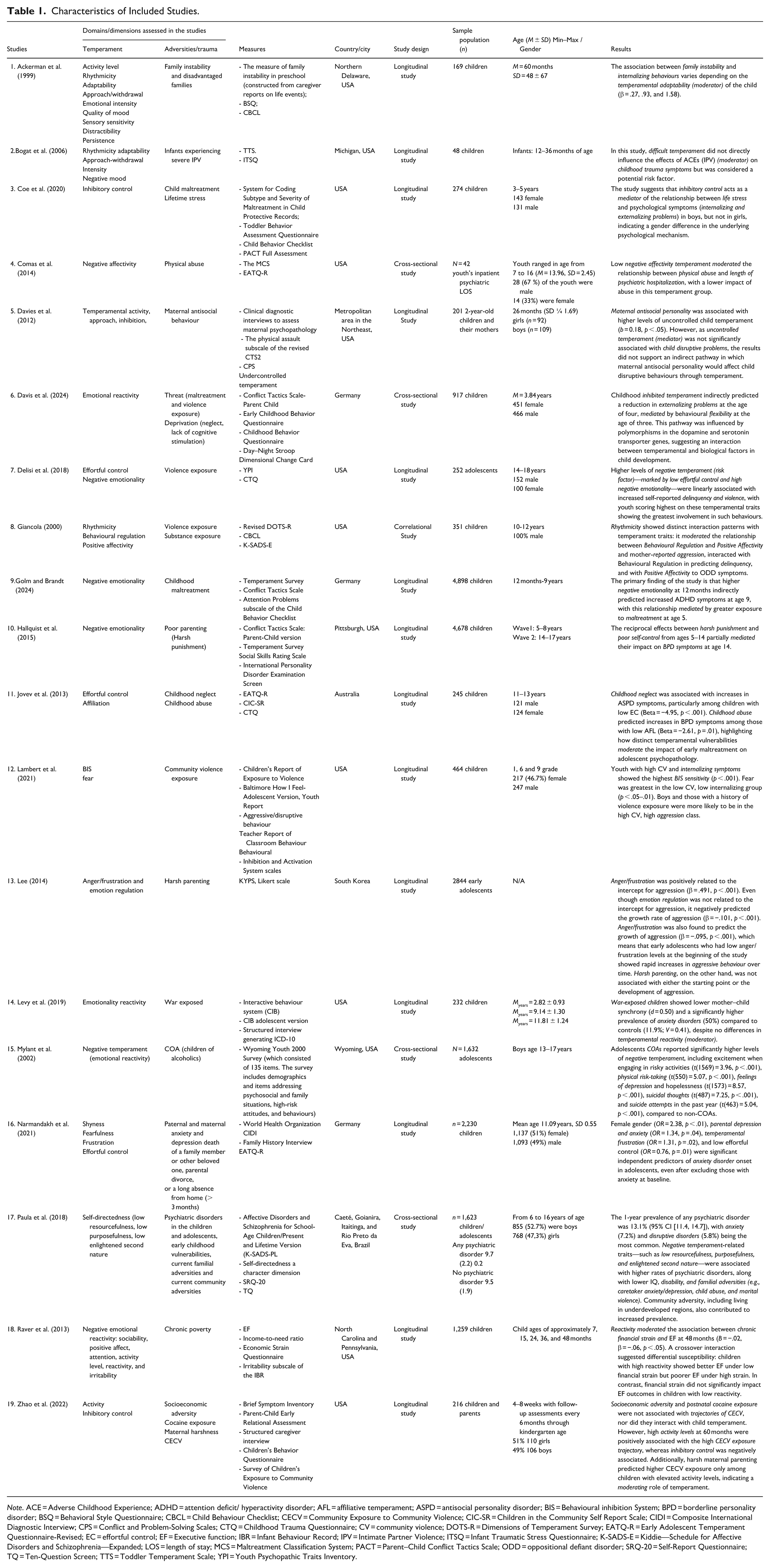
Note. ACE = Adverse Childhood Experience; ADHD = attention deficit/ hyperactivity disorder; AFL = affiliative temperament; ASPD = antisocial personality disorder; BIS = Behavioural inhibition System; BPD = borderline personality disorder; BSQ = Behavioral Style Questionnaire; CBCL = Child Behaviour Checklist; CECV = Community Exposure to Community Violence; CIC-SR = Children in the Community Self Report Scale; CIDI = Composite International Diagnostic Interview; CPS = Conflict and Problem-Solving Scales; CTQ = Childhood Trauma Questionnaire; CV = community violence; DOTS-R = Dimensions of Temperament Survey; EATQ-R = Early Adolescent Temperament Questionnaire-Revised; EC = effortful control; EF = Executive function; IBR = Infant Behaviour Record; IPV = Intimate Partner Violence; ITSQ = Infant Traumatic Stress Questionnaire; K-SADS-E = Kiddie—Schedule for Affective Disorders and Schizophrenia—Expanded; LOS = length of stay; MCS = Maltreatment Classification System; PACT = Parent–Child Conflict Tactics Scale; ODD = oppositional defiant disorder; SRQ-20 = Self-Report Questionnaire; TQ = Ten-Question Screen; TTS = Toddler Temperament Scale; YPI = Youth Psychopathic Traits Inventory.
Study Design
Following the typology proposed by Montero and León (2007), most studies used longitudinal designs (n = 14), while five employed cross-sectional designs.
Measures
The included studies employed a wide range of validated instruments to assess child temperament, exposure to adversity or trauma, family context, and related outcomes.
Adversity and Trauma
Adversity was assessed using standardized self-report and caregiver-report tools, including the CTQ, Children’s Report of Exposure to Violence, Infant Traumatic Stress Questionnaire, and the Survey of Children’s Exposure to Community Violence. Maltreatment and family violence were measured through instruments such as the Conflict Tactics Scale (including parent–child versions), the Maltreatment Classification System, and coding systems based on child protection records. Broader family context was evaluated using caregiver-reported life events, the Economic Strain Questionnaire, Income-to-Need Ratio, the Wyoming Youth 2000 Survey, and the Family History Interview. Maternal psychopathology was assessed with structured diagnostic interviews and screening instruments (e.g., Brief Symptom Inventory, SRQ-20, Composite International Diagnostic Interview [CIDI], IPDE).
Temperament
Temperament was measured with validated parent- and self-report questionnaires, including the Behavioral Style Questionnaire, Toddler Temperament Scale, Early Childhood Behavior Questionnaire, Childhood Behavior Questionnaire, Revised Dimensions of Temperament Survey, Emotionality, Activity, and Sociability Survey, and the Early Adolescent Temperament Questionnaire-Revised. Complementary tools assessed behavioural and emotional regulation, such as the CBCL, Teacher Report of Classroom Behavior, Youth Psychopathic Traits Inventory, and executive function tasks (e.g., Day–Night Stroop, Dimensional Change Card Sort, LAB-TAB).
Child Outcomes
Outcomes were primarily assessed using the CBCL, complemented by performance-based executive function tasks and structured diagnostic interviews (e.g., Developmental and Well-being Assessment, Composite International Diagnostic Interview). Parent- and teacher-report measures increased ecological validity. These instruments enabled a comprehensive assessment of behavioural, emotional, cognitive, and clinical dimensions.
Setting
The 19 studies were published between 1998 and 2025, predominantly in the United States (n = 13, 68.4%), with additional studies from Germany (n = 3, 15.7%), and one each from Australia, South Korea, and Brazil (n = 1, 5.3% each).
Participants
A total of 22,375 participants were included across the studies in this scoping review. Of these, 3,156 (14.1%) were girls (reported in 10 studies) and 5,291 (23.6%) were boys (reported in 11 studies). In seven studies, participant sex was not specified, accounting for 13,928 individuals (62.3%). Most studies (n = 12; 63.2%) included only children, while three studies (15.8%) focused exclusively on adolescents. In addition, two studies (10.5%) included both children and adolescents, and two studies (10.5%) included parents–child. The age of participants at the time of assessment ranged from 7 months to 18 years.
Interaction Between ACEs and Temperament: Empirical Findings and Associated Outcomes
This scoping review identified 43 empirical studies examining the relationship between ACEs and temperament. Although 43 empirical studies were initially identified that examined the relationship between adversity/trauma and temperament dimensions, only 19 studies that also examined related outcomes were included in the final selection for this scoping review.
Across the included studies, a range of developmental and psychopathological outcomes were identified in relation to, and in some cases appearing to result from, the interaction between ACEs and temperament. Externalizing problems (n = 5) were the most frequently reported, including aggressive behaviours (Ackerman et al., 1999; Coe et al., 2020; Davis et al., 2024), oppositional defiant symptoms (Giancola, 2000), conduct or disruptive behaviour problems (Davies et al., 2012). Internalizing problems (n = 1) were also noted, with a study reporting an association with Anxiety (Levy et al., 2019).
Personality disorders were explored in three studies (n = 3), with findings indicating elevated symptoms and traits associated with borderline personality disorder (BPD) (Hallquist et al., 2015; Jovev et al., 2013) and antisocial personality disorder (Jovev et al., 2013) in individuals with specific temperamental vulnerabilities. Additional outcomes included attention-deficit/hyperactivity disorder (ADHD) (n = 1; Golm & Brandt, 2024), executive functioning (EF) deficits (n = 1; Raver et al., 2013), length of psychiatric hospitalization (n = 1; Comas et al., 2014), and trauma-related symptoms (n = 1; Bogat et al., 2006). One study (Zhao et al., 2022) specifically addressed exposure to community violence, highlighting its association with community-level adversity and temperament. This study was included in the review because the authors conceptualized exposure to community violence not merely as a risk factor, but as an outcome in itself, reflecting the child’s psychological or behavioural response to adverse environmental conditions. Across all studies included in this review, the interaction between specific temperamental traits and ACEs has been shown to significantly influence developmental trajectories, either by amplifying vulnerability or by mitigating the psychological and behavioural impacts of adversity. This dynamic interplay constitutes the central focus of the present analysis and is addressed through the following review question:
How have studies examined the role of temperament and adverse childhood experiences (ACEs) in predicting developmental and mental health outcomes in children and adolescents, particularly in terms of interaction and indirect effects:
Descriptive or Unspecified Effects (n = 6): This category includes studies in which no formal tests of mediation, moderation, or interaction between ACEs and temperament were conducted, or in which the analytic roles of these variables were unclear and primarily descriptive or correlational. In these studies, both ACEs and temperamental traits were considered predictors in additive models, but without examining potential interactive or indirect effects (DeLisi et al., 2018; Lambert et al., 2021; Lee, 2014; Mylant et al., 2002; Narmandakh et al., 2021; Paula et al., 2018).
Temperament as a Mediator or Moderator (n = 13): This group encompasses studies that explicitly tested temperament as either a mediator, explaining the pathway from ACEs to outcomes, or as a moderator, modifying the strength or direction of the relationship between adversity and developmental/mental health outcomes. Findings across these studies illustrate a variety of roles for temperamental dimensions: Self-regulation domain: Inhibitory control was the most frequently studied dimension. Two studies identified it as a mediator (Coe et al., 2020; Davis et al., 2024), while two others identified it as a moderator (Jovev et al., 2013; Zhao et al., 2022), underscoring its central role in shaping developmental trajectories in the context of early adversity.
Reactivity and affective traits: Three studies examined reactivity (Levy et al., 2019; Raver et al., 2013) as a moderator, specifically, one study analysed negative affectivity as a moderator (Comas et al., 2014), while another identified negative emotionality as a mediator (Golm & Brandt, 2024); Other temperament dimensions: Adaptability (Ackerman et al., 1999) and Rhythmicity (Giancola, 2000) were each examined in one study as moderators. One study (Davies et al., 2012) conceptualized temperament as a global construct and tested its moderating effect on the relationship between ACEs and outcomes. Finally, one study (Hallquist et al., 2015) identified partial mediation by poor self-control in the relationship between harsh parenting and BPD symptoms. We identify a study (Bogat et al., 2006) that uniquely examined ACEs as a moderator, specifically evaluating how severe exposure to intimate partner violence in infancy moderated the effects of temperament on childhood PTSD symptoms.
Taken together, the reviewed studies demonstrate a range of methodological approaches to examining the interplay between temperament and ACEs in predicting developmental and mental health outcomes. While some studies remain descriptive or correlational, a growing number have employed more sophisticated models to test indirect and interactive effects, particularly highlighting the roles of self-regulation, reactivity, and affective traits. Inhibitory control emerged as a frequently studied temperamental dimension, highlighting its relevance in both mediating and moderating developmental pathways. Notably, one study uniquely examined ACEs as a moderator, specifically assessing how severe exposure to intimate partner violence in infancy moderated the effects of temperament on childhood trauma symptoms. These findings emphasize the role of temperament not only as an individual trait but also as an interactive mechanism through which early adversity influences developmental outcomes.
Discussion
This scoping review underscores the multifaceted and context-sensitive role of temperament in shaping developmental and mental health outcomes among children and adolescents exposed to ACEs. From a total of 43 initially identified studies, 19 met the inclusion criteria of also examining developmental or psychopathological outcomes, thereby enabling a focused analysis of temperament as a mediating or moderating factor in the ACEs-outcomes pathway.
The majority of studies were conducted in the United States (n = 13), with additional contributions from Germany, Australia, South Korea, and Brazil, reflecting a somewhat limited yet diverse international perspective. Over two-thirds of studies were conducted in the United States, potentially limiting cross-cultural generalizability. For instance, the association between high reactivity and externalizing problems may differ in collectivistic cultures where emotional expression is regulated differently (Chen et al., 2015).
Across these 19 studies, 22.375 participants were included, ranging in age from 7 months to 18 years. However, considerable heterogeneity in sample reporting, particularly regarding sex and age, was noted, with seven studies not reporting participants’ sex (62.3%) and a predominance of child rather than adolescent samples. For example, 14.1% of participants lacked sex/gender data, and only 23.6% were males in the studies that differentiated gender. This limited evidence obscures potential sex differences in susceptibility, critical given evidence that boys show stronger ACE effects on externalizing behaviours (Davis et al., 2024), while girls may have increased internalize outcomes (Levy et al., 2019). The predominance of child samples (13 of 19 studies), with limited adolescent representation (three studies), reveals key age-related patterns: Studies like Raver et al. (2013) on EF deficits examined preschoolers (3–5 years), aligning with DST emphasis on sensitive periods for self-regulation development (Belsky & Pluess, 2009). However, the lack of adolescent data (e.g., puberty’s role in moderating temperament-ACEs links) represents a critical gap. Bogat et al. (2006) showed IPV exposure amplifies temperamental irritability, supporting DST’s premise that susceptibility emerges early (Pluess, 2015). However, since the study did not test whether these same irritable infants would benefit most from enriched caregiving, its findings provide only partial support for DST. While early temperamental traits like irritability mark vulnerability in adversity (Belsky & Pluess, 2009), their role as plasticity markers hinges on future research that manipulates environmental quality, including the presence of enriched or supportive contexts.
Of the 19 studies, 13 adopted analytical models testing temperament as a mediator or moderator between ACEs and developmental outcomes. This growing body of literature has moved beyond descriptive correlations, aligning with theoretical frameworks that recognize the transactional and dynamic nature of child development, consistent with the conceptual framework of DST (Belsky & Pluess, 2009). In the mediation models, Inhibitory control, a core self-regulatory function, emerged as a prominent mediator. For example, Golm and Brandt (2024) found that low effortful control accounted for 28% of the variance in the relationship between neglect and ADHD symptoms (β = 0.32, p < .01), suggesting a neurocognitive mechanism through which early adversity is translated into behavioural dysfunction. Other studies similarly implicated negative emotionality and poor self-control as mediators (Coe et al., 2020; Davis et al., 2024; Hallquist et al., 2015). However, despite theoretical predictions from DST, none of the studies tested whether these same vulnerable traits confer enhanced benefits in enriched or therapeutic environments.
Concerning moderation models, eight studies examined temperament as a moderator, highlighting its conditional influence on the impact of ACEs. Traits such as high emotional reactivity (Zhao et al., 2022), low adaptability (Ackerman et al., 1999), and negative affectivity (Comas et al., 2014) intensified associations between environmental stressors and maladaptive outcomes. These patterns suggest that temperament can amplify or attenuate the effects of adversity, depending on context, a principle core to DST.
Importantly, some findings align partially with DST’s premise of heightened sensitivity to environmental inputs. For instance, Zhao et al. (2022) found that high activity levels at 60 months were positively associated with a high exposure trajectory to community violence, while inhibitory control was negatively associated. Moreover, harsh maternal parenting predicted higher exposure to community violence only among children with elevated activity levels, suggesting a moderating role of temperament. However, no studies directly demonstrated classic “for-better-and-for-worse” effects, in which the same temperament traits confer both increased vulnerability in adverse contexts and enhanced adaptation in supportive ones. As such, much of the current evidence continues to reflect a diathesis-stress orientation, rather than true differential susceptibility (Stoltz et al., 2017).
Moreover, a striking limitation in the broader literature is the limited attention given to temperament as a moderating or mediating factor in the relationship between ACEs and developmental outcomes. Despite the vast number of studies investigating how ACEs influence development, only 13 explicitly tested models in which individual differences in temperament shaped these associations. This reveals a conceptual gap: much of the literature fails to account for individual differences in susceptibility, thereby overlooking central principles of DST.
Additionally, only one study tested ACEs as a moderator, a particularly surprising finding, given that from a conceptual standpoint, it is more coherent to treat temperament as the individual-level variable and ACEs as the contextual factor that moderates or mediates its effect. Beyond the limited number of studies that tested such interactions, only one adopted an analytical approach that explicitly aligned with the theoretical logic of DST. This underscores not only a methodological gap but a broader disconnect between empirical research and the theoretical models that emphasize the dynamic interplay between individual traits and environmental contexts.
Regarding the results of interest and their relationship with the temperament-ACEs interaction: The explored outcomes spanned a range of psychological and behavioural domains, with externalizing problems most frequently reported (n = 5), including aggression, conduct problems, and oppositional defiant symptoms. Internalizing outcomes were less commonly studied, though anxiety (Levy et al., 2019) and trauma-related symptoms (Bogat et al., 2006) were observed. Additionally, the interaction between temperament and ACEs was implicated in symptoms of personality disorders, particularly borderline and antisocial personality characteristics (Hallquist et al., 2015; Jovev et al., 2013), as well as ADHD, executive function deficits, and psychiatric hospitalization duration. The reviewed studies demonstrated distinct temperament-based pathways to externalizing behaviours, with important implications for DST. However, the absence of "for better" tests in these studies represents a significant limitation, we cannot determine whether these same reactive children might have shown superior outcomes in particularly supportive environments, as predicted by DST’s plasticity hypothesis (Belsky & Pluess, 2009).
Zhao et al. (2022) is notable for conceptualizing exposure to community violence not just as a risk factor but as an outcome reflecting children’s psychological and behavioural responses to adversity. This view expands traditional adversity models by showing exposure as a developmental outcome influenced by both context and temperament (Armstrong-Carter & Telzer, 2022; Jean-Thorn et al., 2023).
Their findings align with the ecological-transactional model (Cicchetti & Lynch, 1993), demonstrating how temperament traits like activity level and inhibitory control moderate the effects of harsh maternal parenting on violence exposure trajectories (Belsky & Pluess, 2009). Framing exposure as an outcome highlights children’s active role in shaping adversity experiences, consistent with DST (Belsky, 1997).
This dynamic perspective suggests interventions should address both environmental risks and individual resilience (Masten, 2021). Overall, Zhao et al. (2022) advance a nuanced understanding of adversity as an intertwined process of exposure and response, warranting further research on these bidirectional dynamics.
An alternative pathway emerged through mediation analyses, where low inhibitory control explained 25% to 30% of the association between ACEs and aggressive behaviours across multiple studies (Coe et al., 2020). This neurocognitive mechanism suggests that interventions targeting effortful control might mitigate externalizing outcomes for children exposed to adversity. From a DST perspective, these findings raise important questions about whether inhibitory control functions as a general vulnerability factor or a true plasticity marker that would also enhance responsiveness to positive environmental influences (Obradović, 2016).
The most compelling evidence for biological susceptibility emerged from studies of personality disorder risk, particularly Hallquist et al. (2015) longitudinal examination of BPD pathways. Their finding that poor self-control mediated 28% of the association between harsh parenting and later BPD symptoms, with additional moderation by 5-HTTLPR genotype, provides strong support for DST’s emphasis on gene-environment-temperament interplay. The German sample’s demonstration that serotonin-related genetic variants moderated environmental sensitivity replicates core DST findings reported by Davis et al. (2024) while extending them to personality pathology outcomes. Notably, this study’s design captured both the “for worse” (vulnerability to harsh parenting) and “for better” (responsivity to supportive environments) aspects of susceptibility, offering a more complete test of DST than most other reviewed studies. These outcome-specific pathways collectively suggest that temperament traits may operate differently across psychopathology domains, with reactivity showing particularly strong links to externalizing behaviours, negative affectivity to internalizing problems, and effortful control deficits to personality pathology. This pattern underscores the importance of moving beyond generic “difficult temperament” constructs to examine how specific temperamental dimensions interact with particular types of environmental experiences to shape divergent developmental outcomes (Hinshaw & Lee, 2003; McCauley et al., 2001).
The single identified study examining internalizing outcomes (Levy et al., 2019) found that negative affectivity significantly predicted anxiety symptoms, specifically in high-ACEs contexts (β = .39). While this conditional effect aligns with DST’s environmental sensitivity framework, the exclusive focus on adverse environments leaves open critical questions about the potential “bright side” of this temperamental trait. The study’s cross-sectional design and failure to examine positive environmental moderators (e.g., parental warmth, social support) represent missed opportunities to fully test DST predictions. Future research should investigate whether children high in negative affectivity might demonstrate particularly strong benefits from supportive interventions, as suggested by recent DST-informed work on anxiety prevention suggested by recent DST-informed work on anxiety prevention (Pluess et al., 2018).
Conclusion and Future Directions
This scoping review aimed to identify studies that highlight the significant role of temperament as both a mediator and moderator in the relationship between ACEs and developmental outcomes. Overall, the existing literature provides important insights into specific mechanisms linking ACEs, temperament, and early developmental outcomes. However, key limitations constrain current understanding, particularly regarding the developmental timing and duration of ACE exposure assessed in the included studies. Because most samples consisted of children and relied on a single or limited number of assessments of adversity, the available evidence primarily reflects proximal outcomes of early ACEs rather than the cumulative burden of adversity accrued by age 18. As a result, these studies do not encompass later-emerging adversities (e.g., peer victimization, dating violence, community-level risks) or developmental periods in which new ACEs and mental health problems are especially likely to occur.
Although many of the included studies adopted longitudinal designs with respect to developmental and mental health outcomes, ACE exposure was most often assessed at a single time point, either early in development or retrospectively. Consequently, even within longitudinal frameworks, adversity was typically operationalized as a static or proximal exposure, limiting the ability to model the accumulation, timing, and evolution of ACEs across childhood and adolescence. These child-based designs are therefore well suited to identifying early associations and temporal ordering, but are less capable of capturing cumulative exposure, developmental change, and long-term trajectories of psychopathology and adaptation. This limits current knowledge about ACE–temperament interplay to early and middle childhood and may lead to underestimation of both total ACE load and long-term developmental trajectories of psychopathology and adaptation.
To address these gaps, future research should prioritize longitudinal designs with repeated assessments of ACEs, temperament, and outcomes across multiple developmental periods, ideally from early childhood through adolescence and, where possible, into adulthood. Such designs would allow researchers to examine how cumulative and time-varying ACE exposure interacts with relatively stable temperamental traits, to test whether certain developmental windows (e.g., puberty) represent sensitive periods for ACE–temperament effects, and to identify how early vulnerabilities or plasticity markers unfold into later functioning. Multi-wave, prospective cohorts with diverse samples are therefore essential to refine inferences drawn from the predominantly child-based literature with limited repeated assessment of ACE exposure reviewed here.
A further limitation concerns the way adversity was operationalized across the included studies. Although the ACE framework is conceptually cumulative (Anda et al., 2020), most studies examined only a single ACE type or a narrow subset of exposures. While single-exposure approaches offer valuable insights into specific mechanisms, they do not reflect the broader accumulation of risk that defines ACEs and may underestimate the overall adversity burden (Briggs et al., 2021). Consequently, associations between temperament and adversity should be interpreted cautiously, as effects may differ when multiple ACEs co-occur. Evidence from cumulative-risk research shows that combined adversities often exert stronger and qualitatively distinct influences on developmental outcomes compared to isolated exposure types (Lanier et al., 2018). To advance the field, future studies should employ comprehensive cumulative ACE measures that capture the number and co-occurrence of adversity types, ideally within longitudinal, multi-informant designs capable of modelling diverse adversity patterns over time.
Selection bias emerged from the exclusion of studies examining only direct ACE–temperament links, potentially overlooking whether temperament reflects an outcome of adversity or a pre-existing vulnerability. Additionally, possible publication bias and the predominance of Western-based samples limit the generalizability and developmental insight of findings. Longitudinal studies spanning adolescence remain scarce, and resilience-promoting traits such as sociability or adaptability are underexplored.
While evidence supports temperament’s role in shaping susceptibility to adversity, the existing literature rarely tests the full theoretical implications of this susceptibility. In particular, no study examined whether the same temperamental traits that confer vulnerability in adverse contexts also predict enhanced outcomes in supportive or enriched environments, a central tenet of DST.
Consistent with this gap, out of a vast number of studies on ACEs, only 13 explicitly tested models in which temperament moderated or mediated developmental outcomes. Even more concerning, only one study tested ACEs as a moderator, despite ACEs conceptually representing the environmental context and temperament of the individual-level trait. This pattern highlights a misalignment between commonly used analytic models and foundational developmental theories. Moreover, only one study explicitly applied a DST framework, and none systematically examined “for-better-and-for-worse” effects, limiting progress in both theory testing and application.
Taken together, these limitations do not undermine the contribution of the existing literature but instead delineate clear priorities for future research. Future studies should explicitly test “for-better-and-for-worse” interactions using DST-aligned statistical models that incorporate both adverse and supportive environments. Greater attention to age- and sex-specific pathways, particularly during adolescence, is warranted. Studies must also disaggregate temperament into its core dimensions to map their specific links to distinct psychopathological outcomes. Additionally, biologically informed, longitudinal designs integrating genetic, temperamental, and environmental variables are essential to advancing a mechanistic understanding of developmental plasticity and individual differences in susceptibility. Crucially, the limited use of interactional models to date and their inconsistent conceptual alignment with DST have constrained progress in both theory and application. Clinical implications, such as interventions targeting inhibitory control or emotional regulation, remain speculative without direct experimental validation, reinforcing the need for translational designs that bridge basic research and intervention science.
Supplemental Material
sj-docx-1-tva-10.1177_15248380261429500 – Supplemental material for Temperament and Adversity in Childhood and Adolescence: A Scoping Review of Influences on Developmental Outcomes
Supplemental material, sj-docx-1-tva-10.1177_15248380261429500 for Temperament and Adversity in Childhood and Adolescence: A Scoping Review of Influences on Developmental Outcomes by Laura Silva, Maria Vieira de Castro, Beatriz Alves, Tânia Gonçalves, Ângela Maia and Ricardo J. Pinto in Trauma, Violence, & Abuse
Footnotes
Author Contributions
L.S. and M.V.C. contributed to the conception and design of the work. L.S. and M.V.C. contributed to the design of the search strategy. B.A. and T.G. contributed to the acquisition of data. B.A. and T.G. contributed to the extraction and analysis of data. L.S., M.V.C., A.M., and R.P. contributed to the contextualization and interpretation of data. A.M. and R.P. contributed to drafting and revision. All authors have approved the final version.
Funding
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in this published article and its supplementary information files.
Pre-Registration Statement
This study was not preregistered.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.