
Abstract
People with traumatic experiences of migration, sexual violence (SV), and/or intimate partner violence (IPV) are at heightened risk of mental health problems such as post-traumatic stress disorder (PTSD). Group-based psychosocial interventions may offer value, fostering social support and normalisation. However, the complexity of addressing migration trauma and SV and/or IPV trauma warrants careful consideration. This review aimed to identify group-based psychosocial interventions developed for or tested with women who have experienced migration and SV and/or IPV. Studies of any design and setting were eligible, provided interventions were delivered in a group format or were known to have been delivered in a group format in other contexts. Populations under 15 years were excluded. A systematic search was conducted on April 19, 2023 across five databases: ASSIA, CINAHL, PsycINFO, PubMed, and Scopus. Two authors independently screened titles and abstracts. A wider team conducted full-text screening and extracted data on intervention details, context, and publication information. Seventeen papers met the criteria, covering 13 interventions. These included arts-based, therapeutic, and skills-focused approaches. Around half were designed specifically for women with migration and SV/IPV experiences, while the rest were established psychosocial programmes applied to this group. Tailored interventions often combined relaxation and strength-based techniques to support emotional regulation, safety, and empowerment. Hesitancy to join groups was frequently reported, suggesting that combining group with individual support may be beneficial. Implementing interventions for migrants with experiences of SV and/or IPV requires sensitivity to context and a holistic approach to recovery.
Introduction
Violence against women is widely acknowledged as a serious public health issue and a violation of human rights. Among its various forms, sexual violence (SV) and intimate partner violence (IPV) are two prevalent and deeply harmful manifestations, posing substantial physical, psychological, and social consequences for those affected. SV refers to any non-consensual sexual act or activity that involves coercion, force, or the use of threats. It encompasses a broad range of behaviours, including sexual assault, rape, unwanted sexual touching, harassment, and any form of sexual coercion (World Health Organization, 2024). IPV involves any pattern of abusive behaviour used by one partner in an intimate relationship to exert power and control over the other partner. This can manifest in various forms, including sexual coercion, physical violence, emotional or psychological abuse, and controlling behaviours (Wong et al., 2018).
Theoretical models of the causes of IPV and other forms of violence against women suggest that an interplay of individual, situational and socio-cultural factors influence an individual’s risk of experiencing violence (Heise, 1998; Kelly, 2011). Gender and gender norms are understood as key factors, and while it is challenging to ascertain true rates of IPV, there is evidence to suggest that differences in the distribution of IPV exposure exist related to gender identity and sexual orientation, with women reporting greater prevalence, as well as more severe and more frequent exposure than men (Fanslow et al., 2023), and heterosexual men reporting lower levels of SV compared to women, nonbinary + youth, and gay and bisexual men (Löfström-Bredell et al., 2025). Further, factors understood to increase the risk of experiencing violence include a personal history of experiencing multiple interpersonal traumas, such as child abuse, women’s unemployment and economic dependency on the partner, and social inequities and marginalisation related to, for example, racism, poverty and disability (Heise, 1998; Kelly, 2011). As migration can lead to an accumulation of such risk factors, women who have migrated are often hypothesised as being particularly at risk of experiencing SV and IPV. This is supported by studies demonstrating a higher prevalence of IPV victimisation among migrant women compared to women born in the host country (Almeida et al, 2017; Hicks et al, 2021). However, the evidence base is inconclusive: systematic reviews have found highly heterogeneous prevalence rates of IPV victimisation among migrant women, with estimations varying depending on country of origin, type of violence measured, and what measure was used, and the possibilities to draw conclusions complicated by issues such as small sample sizes (Gonçalves & Matos, 2016; Morrison et al., 2023). For this paper, ‘migration’ refers specifically to forced or involuntary migration, including displacement due to conflict, persecution, or other circumstances associated with traumatic experiences. We focus on women who have experienced such forced migration, as their psychosocial needs and exposure to trauma differ from those of voluntary or economic migrants (Freedman, 2016).
Mental Health and Experiences of Sexual Violence, IPV, and Migration
Sexual assault is associated with an increased likelihood of developing various psychiatric disorders, including substance use disorders, mood disorders, and post-traumatic stress disorder (PTSD; Dworkin et al., 2017). Similarly, survivors of IPV have an increased prevalence of mental health problems such as PTSD, depression and suicide, as well as a significantly increased risk of chronic pain, including pelvic pain, back pain and headaches (Campbell, 2002). Moreover, IPV and SV are known to impact relationships, trust, and social connections. The recovery process often involves re-establishing a sense of self and rebuilding connections with the broader community, which plays a crucial role in healing (Sinko & Saint Arnault, 2019; Sinko et al., 2021).
Research on the association between combinations of traumatic experiences and mental health outcomes has demonstrated that both type of and combination of traumatic experiences are associated with mental health outcomes; with experiences of sexual violence and of multiple types of traumas being associated with an increased odds of mental health problems (Yapp et al., 2023). Thus, women who have experienced both forced migration and SV and/or IPV are likely to be at risk of experiencing complex psychiatric needs. Research indicates that around two‑thirds of asylum seekers and victims of trafficking meet criteria for Complex PTSD (CPTSD; Jowett et al., 2021), which includes the classic PTSD symptoms of re‑experiencing, avoidance, current sense of threat, plus disturbances in self-organisation, including affective dysregulation, negative self‑concept, and relational difficulties. CPTSD is also common among women who have survived IPV, with around two-fifths meeting the criteria (Fernández-Fillol et al., 2021). Research specifically examining the combination of forced migration and SV and/or IPV in relation to CPTSD is lacking. However, the cumulative, and for some, ongoing trauma is likely linked to CPTSD, which is suggestive of the need for interventions that address emotional regulation and resilience.
Support for Experiences of Sexual Violence and IPV
In a systematic review of early intervention after experiencing sexual assault, Dworkin and Schumacher (2018) found mixed effects on the likelihood of developing PTSD. Informal support (e.g. telling friends or family) and formal therapy show varied results, with some studies indicating no impact and others suggesting benefits. In one case, there was a report of potential harm depending on trauma history; women without a rape history reported elevated PTSD and depression symptoms after a video intervention designed to reduce PTSD (Resnick et al., 2007). Early interactions with the criminal justice and healthcare systems also yield mixed findings, though positive perceptions of these interactions were linked to lower post-traumatic stress (Dworkin & Schumacher, 2018).
A systematic review of psychological therapies for women who experience IPV reported evidence of reduced depression and a positive impact on anxiety (Hameed et al., 2020). However, it remains unclear whether the therapeutic interventions adequately address women’s ongoing needs for safety, support, and comprehensive healing from complex trauma (Hameed et al., 2020). The authors concluded there is a pressing need for more interventions centred on trauma-focused approaches, and rigorous trials with consistent outcomes and comparable follow-up time points are essential, as much of the available research could not be synthesised (Hameed et al., 2020). In a further review, focused on counselling interventions, Craven et al. (2023) report on the value of group interventions for IPV victims, both independently and in conjunction with individual counselling. They discuss how the connection with others can promote self-esteem, and participants can learn from one another.
A meta-analysis of a broader range of IPV interventions, including both psychological therapies as well as social work support such as advocacy services, telephone social support, and safety planning aid, showed promising improvements in anxiety, depression, safety, violence prevention, health, self-esteem, social support, and stress management, though findings on self-efficacy and quality of life were mixed (Karakurt et al., 2022). Empowerment was found to be particularly important in addressing depression and PTSD, highlighting the need for interventions that address co-morbid issues and foster long-term recovery.
While these reviews aid our understanding of how interventions can support women who have experienced SV and/or IPV, specific reviews of interventions for subgroups in society are essential to understanding how interventions for SV and IPV are experienced by different demographic groups, as well as by groups who have experienced multiple traumas. People with traumatic experiences of migration, SV and/or IPV can be in a particularly vulnerable situation in terms of access to adequate services. Seeking care can be hampered by difficulties with trust due to interpersonal traumas; a lack of knowledge regarding your rights and navigation in the host society; fear relating to deportation (your own, or the perpetrator’s) or to other agencies finding out about your difficulties, as well as; a limited or non-functioning use of interpreters in the required services (Jolof & Rocca, 2023). The survivor of IPV might be dependent on the perpetrator – financially, socially, relating to language, civic orientation or even residence permit, if the case concerns family reunification. Qualitative research by Voolma (2018) showed that undocumented women in Sweden face major barriers in accessing support, including the lack of financial aid for shelter accommodation. Even when women are formally eligible for services, they often lack awareness of their rights, struggle to prove eligibility, or fear approaching authorities. Survivors described how threats of deportation were used by abusers as a form of control, reinforcing dependence and silencing help-seeking. The fear of return was compounded by having no means of survival as a single woman, concerns for their children’s safety, and fear of facing violence (including lethal) from family and community members due to negative cultural norms about divorce. If migrant survivors do seek care, they might face various challenges: health professionals in Europe have reported lacking clarity on the entitlement and eligibility of different migrants to receive mental healthcare, administrative issues when providing care to undocumented migrants, variability in access and quality of interpreters, and reluctance to provide counselling to migrants experiencing uncertain and unsafe socioeconomic conditions (Peñuela-O’Brien et al., 2023). Furthermore, challenges in cross-service collaboration have been described as particularly relevant when providing care to patients with a migrant background, due to the frequent need for multiple services. In addition, emotional responses to migrant patients have been found among healthcare professionals, including both positive responses, such as admiration for resilience and taking on an advocacy role, and hostile, untrusting responses, such as querying whether migrants exaggerated their mental health symptoms to remain in the host country. Moreover, some clinicians describe experiencing vicarious traumatisation.
In the context of mental health care, it is also important to recognise that an individual’s understanding of illness and their help‑seeking behaviour will be influenced by the medical paradigms in their countries of origin. In many cultures, physical symptoms, often somatic presentations such as pain or fatigue, are socially acceptable ways to express distress, whereas psychological or psychiatric attributions are stigmatised. For example, Turkish‑born women in Sweden frequently conceptualised suffering in terms of bodily symptoms and rejected psychiatric explanations (Bäärnhielm & Ekblad, 2000). Healthcare professionals’ lack of knowledge about what indicates psychopathology for different patients, and what constitutes a socially acceptable response, can lead to misunderstandings (Peñuela-O’Brien et al., 2023), and healthcare professionals have described avoiding culturally based assumptions in assessment and taking an open, patient-led approach in medical encounters as crucial for avoiding misunderstandings (Peñuela-O’Brien et al., 2023; Wylie et al., 2018).
Responding to the complex issues that women who have experienced both forced migration and SV and/or IPV might face places high demands on customisable interventions and collaboration between relevant service providers. We sought interventions that have been specifically designed for these circumstances or examples of existing psychosocial interventions that have been used with the target group, and that would lend themselves to group delivery. By this, we mean the intervention was delivered as a group intervention or was known to have previously been delivered in a group format. We did not seek to answer a specific question about the interventions but rather to establish the scope of available psychosocial interventions; therefore, a scoping review was chosen over a systematic review. The purpose of the review was to inform intervention delivery within specialist services in Sweden. By evaluating interventions for various subgroups, we can ensure they are effective, equitable, and address each population’s unique needs and vulnerabilities, ultimately leading to more comprehensive and inclusive solutions.
Objective
This review aimed to identify psychosocial interventions tested with or developed for migrant women with experience of sexual violence and/or IPV. The interventions could have been delivered in any geographic or service context but need to have been delivered in a group format, either previously or in the identified literature.
Method
We decided to use a scoping review methodology to examine the extant literature on psychosocial interventions for migrant women with experiences of SV and/or IPV. To guide our scoping review, we followed the framework developed by Arksey and O’Malley (2005). This framework involves five stages: (1) identifying the research question(s); (2) identifying relevant studies; (3) selecting articles; (4) charting the data; and (5) collating, summarising, and reporting the results.
Stage 1. Identifying the Research Question(s)
We involved knowledge users to set and refine our research questions. For our review, knowledge users included psychologists and managerial personnel from the Swedish Red Cross and the National Knowledge Centre for Men’s Violence Against Women (NCK) and four women who have been engaged as public contributors in a broader programme of research on gender-based violence (GBV) among refugees. Regular meetings were held as part of the wider programme of research, in which it was identified that the involved organisations needed to extend the reach of their services. The Swedish Red Cross had formerly focused service attention on experiences of trauma related to war and torture, whereas the NCK clinics served women with experience of SV and IPV. A service provision gap was identified for women with dual experiences. The public contributors in the team advised that the user group would value a group-based service, as becoming aware that others had similar experiences of violence could alleviate shame, building social networks and finding peers was regarded as important for recovery, and learning was seen as easier and more enjoyable in a group where you could exchange thoughts and opinions with others. Their recommendation, based on experiential knowledge, aligns with previous research pointing to the potential of promoting social support and normalisation through group delivery of psychosocial interventions for migrants (Abo-Rass et al., 2025; Due et al., 2024). It is further supported by a qualitative meta-synthesis on healing and recovery from GBV, which identified connecting with others as an important construct of the healing process, with research suggesting meeting others with similar experiences to be beneficial (Sinko et al., 2021). It was recognised by the knowledge users that while specific interventions may have been developed for the dual experience of migration and SV and/or IPV, it could be the case that existing interventions have been used with the target group and that both were of interest. Thus, the resulting research questions were: (i) Which existing psychosocial interventions that have been delivered in a group format have been used with migrant women with experiences of sexual violence and IPV? And (ii) Are there psychosocial interventions that have been designed specifically for women with experiences of migration and SV and/or IPV and delivered in a group format?
Stage 2. Identifying Relevant Studies
A systematic literature search was conducted by a trained librarian on 19 April 2023 using five databases: ASSIA, CINAHL, PsycINFO, PubMed, and Scopus. These databases were chosen for their disciplinary breadth, including health, social sciences, and interdisciplinary research, to capture peer-reviewed studies spanning mental health, public health, and social support interventions. The review intentionally focused on peer-reviewed publications indexed in electronic databases and did not include additional search methods such as hand-searching journals, conference proceedings, or organisational networks. This decision was made to ensure the inclusion of rigorously reviewed evidence and to maintain the feasibility and reproducibility of the search. The search terms for each database are provided as Supplemental Material. The search was designed to detect records with English titles and abstracts; however, papers in any language were included in the review. The search was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009). Only publications with female participants were included. Only publications from 2015 onwards were included to focus on recent advancements while excluding earlier works deemed less relevant to current practice. The year 2015 was selected as the starting point for the review because it represents a pivotal shift in the context of migration, gender-based vulnerabilities, and humanitarian response. The large-scale influx of asylum seekers in Europe during 2015 to 2016 brought new challenges for migrant women (Freedman, 2016). This period also saw the publication of updated international guidelines, such as the 2015 IASC Guidelines for Integrating GBV Interventions in Humanitarian Action (Ward et al., 2015), reflecting contemporary approaches to psychosocial support. By limiting our review to studies published from 2015 onwards, we ensured that the included interventions were relevant to current lived realities of people on the move, policy frameworks, and best practices for addressing the needs of migrant women.
Stage 3. Selecting Articles
We sought literature on psychosocial interventions for SV and/or IPV for migrant women. ‘Psychosocial interventions for SV and/or IPV’ were defined as interpersonal or informational activities, techniques, or strategies offered to survivors of SV and/or IPV to improve mental health and well-being. We were interested in psychosocial interventions that can be offered in a group format. Thus, we included interventions that were delivered in a group format in the identified literature or were known to have been delivered in a group format in other contexts. The aim of the intervention should be to improve mental health and well-being; it could also target social and environmental factors connected to mental health and well-being. We sought interventions that were suitable for adults and thus literature describing populations only under the age of 15 years was excluded. The age of 15 was selected because in Sweden, where the review was conducted, individuals from this age are legally able to provide informed consent for participation in psychosocial interventions. Literature describing interventions specifically targeting men was excluded. There was no restriction on the type of study design eligible for inclusion. For literature reviews, the included papers were screened for eligibility. No other reference tracking took place. There was no restriction on the context; studies in clinical or community settings conducted in low, middle or high-income countries were included.
Step 4. Charting the Data
Two authors (APA and GW) independently screened records for articles that could be excluded based on title and abstract. The initial screening process was blinded. Thereafter, decisions were revealed, and disagreements between individual judgements were resolved through discussion. All review decisions were recorded using the software system Rayyan. If exclusion could not be judged based on the abstract alone, the records proceeded to the next round in which a broader team, including a trainee psychologist (APA, GW, and EH), conducted a full paper review of the remaining records. APA and GW extracted data from the selected records into a data extraction form. Data fields included: intervention name; intervention details; setting (location, context, format); and publication information (author, date, methodology, number of participants). The search was designed to detect records with English titles and abstracts. If the record appeared to meet eligibility criteria but the full paper was in another language, the research team translated the document using an online machine translation service to perform the full paper review.
Step 5. Collating, Summarising, and Reporting the Results
An overview table of all the included records was constructed and ordered by intervention name (Table 1). A written summary of the interventions was organised according to the research questions. In other words, existing interventions that had been used with the target group were described first, followed by a summary of psychosocial interventions that had been designed specifically for experiences of migration and SV and/or IPV.
Overview of Included Publications, Organised by Intervention.
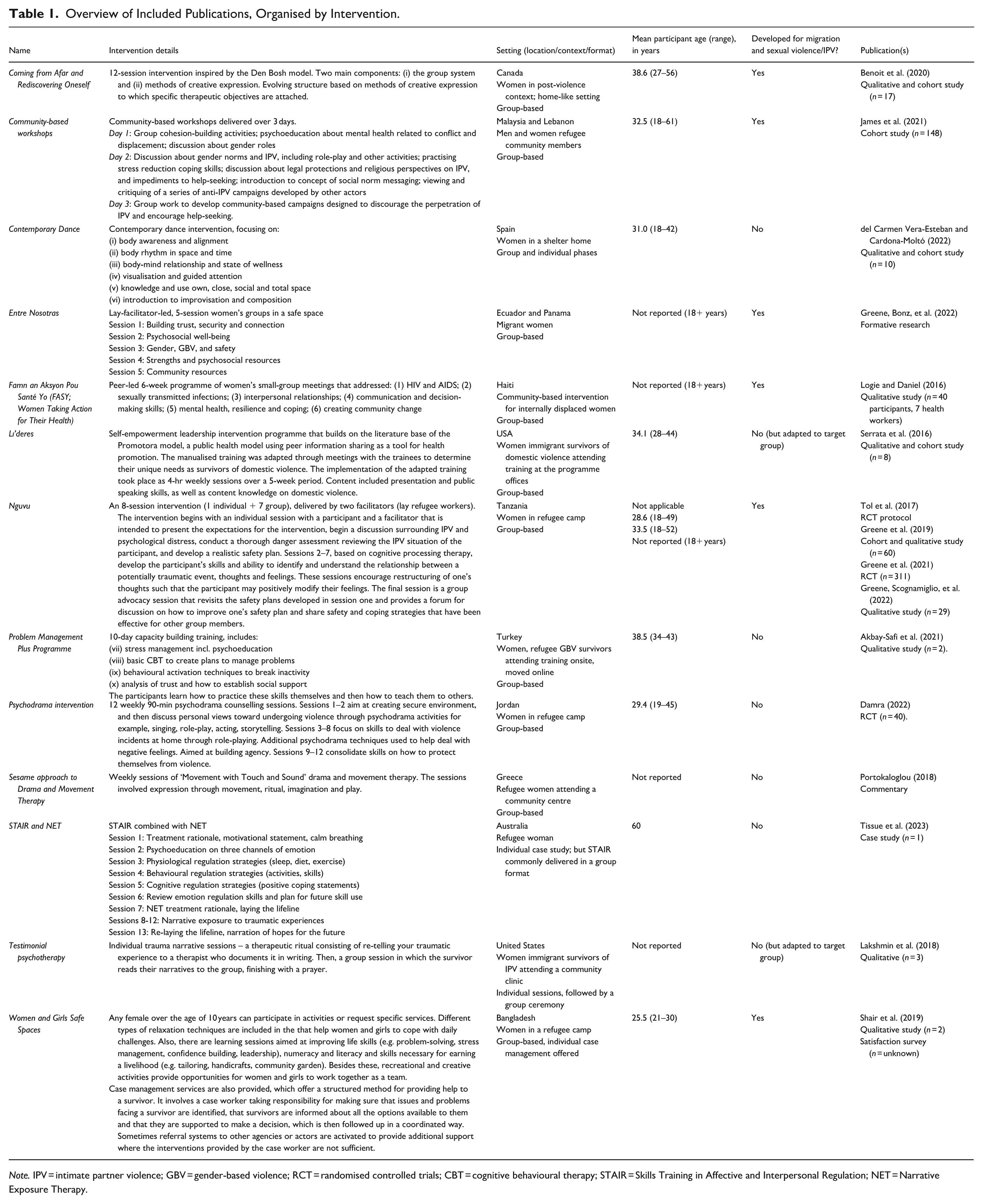
Note. IPV = intimate partner violence; GBV = gender-based violence; RCT = randomised controlled trials; CBT = cognitive behavioural therapy; STAIR = Skills Training in Affective and Interpersonal Regulation; NET = Narrative Exposure Therapy.
Results
The literature search yielded 1,573 records (Figure 1). Of these, 595 were identified as duplicates and removed. The titles and abstracts were screened for the remaining 978 records, with 853 deemed irrelevant and excluded at this stage. Full manuscripts were sought for 125 records; however, it was not possible to retrieve 33 of these. Of the 92 full manuscripts that were reviewed, 16 met the inclusion criteria, reporting on 13 interventions (Table 1). These comprised 1 commentary, 1 case study, 1 protocol paper, 1 formative research paper, 7 qualitative evaluations, 5 cohort studies, and 2 randomised controlled trials (RCTs). Some papers included both qualitative and quantitative studies, hence why the number of study formats exceeds the number of records. The main reasons for exclusion were: the paper did not describe a defined intervention, the focus was not on migration and SV and/or IPV survivors, the intervention was not focused on mental health and well-being, or the intervention had an individual (rather than group-based) delivery format. One paper was excluded because it described an intervention targeting men. Of the 13 interventions, around half were existing psychosocial interventions used with the target group and half had been designed for experiences of migration and sexual violence and/or IPV.
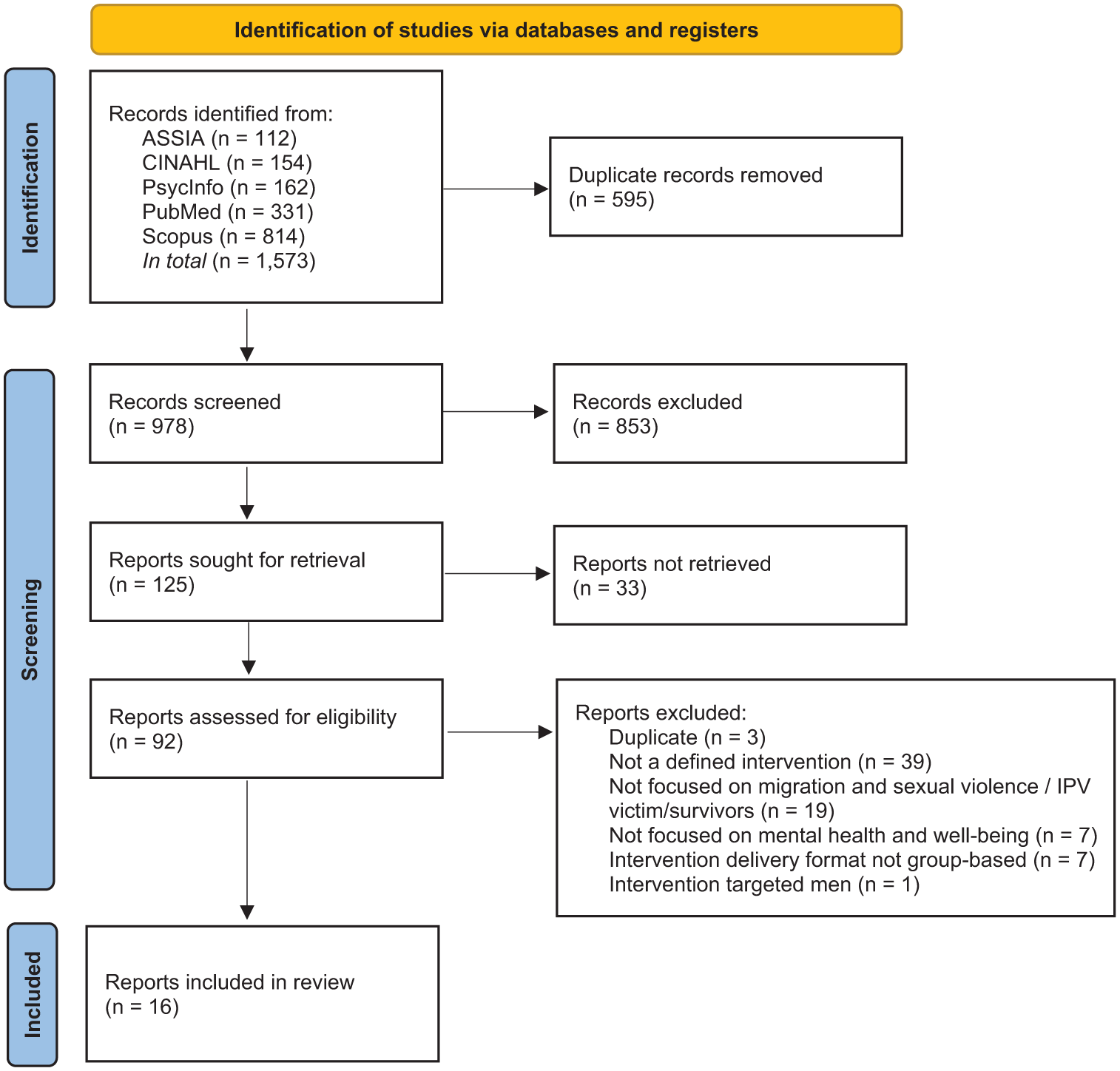
PRISMA flowchart.
Existing Psychosocial Interventions Used With the Target Group
The existing interventions that had been used with the target group encompassed arts-based interventions (Damra, 2022; del Carmen Vera-Esteban & Cardona-Moltó, 2022; Portokaloglou, 2018), therapeutic interventions (Akbay-Safi et al., 2021; Lakshmin et al., 2018), and skills training (Serrata et al., 2016; Tissue et al., 2023). The arts-based interventions covered dance/movement (del Carmen Vera-Esteban & Cardona-Moltó, 2022; Portokaloglou, 2018) and drama (Damra, 2022; Portokaloglou, 2018). The therapeutic interventions included a cognitive behavioural therapy (CBT)-based intervention (Akbay-Safi et al., 2021), testimonial psychotherapy (Lakshmin et al., 2018), and narrative exposure therapy (Tissue et al., 2023). While Akbay-Safi et al. (2021) did not report the use of an intervention with the target group, their paper was included in the scoping review as it described preparatory work for applying an existing intervention with the target group; refugee GBV survivors were trained in how to deliver a CBT-based intervention. The skills-based interventions targeted emotion regulation and interpersonal relationship skills (Tissue et al., 2023), as well as empowerment and leadership skills (Serrata et al., 2016).
Arts-Based Interventions
The collection of papers on arts-based interventions consisted of a case study, a mixed-method pre-post evaluation, and a RCT. The case study described the ‘Sesame approach’ (Portokaloglou, 2018), which used movement, touch, and sound to facilitate psychological healing for GBV survivors. Based on their observations, the authors described improvements in the psychological well-being of the survivors, symbolised by the metaphor of a tree growing new roots after trauma. The pre-post evaluation (N = 10; del Carmen Vera-Esteban & Cardona-Moltó, 2022), which involved both interviews and surveys before and after the 12-week programme, conveyed improvements in self-reported emotional management, self-concept, assertiveness, and overall well-being among GBV survivors living in a shelter in Alicante who attended a contemporary dance intervention. The small-scale RCT (N = 40; Damra, 2022) showed that Syrian refugee women living in a refugee camp in Jordan who attended group psychodrama, consisting of 12 weekly 90-min psychodrama counselling sessions, reported significantly reduced domestic violence and improved self-reported Quality of Life (QoL) directly after the intervention, with the exception of environmental QoL. All of the arts-based interventions were tested in a group format.
Therapeutic Interventions
The therapeutic interventions were included a field report (Akbay-Safi et al., 2021) and a case report (Lakshmin et al., 2018). The field report described a group intervention in educating survivors of GBV by running a supervised psychological support programme, named ‘Problem Management Plus’ (PM+), with other survivors of GBV. PM+ consists of five sessions of skills training and is based on basic CBT. The small-scale qualitative evaluation (N = 2) of the educational intervention indicated a positive impact on the women’s personal lives as well as on their ability to support other survivors. The case report outlined the intervention of Testimonial Psychotherapy (Lakshmin et al., 2018), a humanistic approach where three migrated female survivors of IPV were invited to share their trauma narratives. In one to three individual sessions, the narratives were written down, framed by resilience and thereafter shared in a group context in a ceremonial procedure, to support community reintegration and spiritual coping. A qualitative account from one of the participating women highlighted that sharing your narrative in a group context had been painful yet rewarding as it facilitated sense-making of traumatic experiences and lessened feelings of shame and loneliness.
Skills Training
Two papers described skills-based training, one case study on the implementation of Skills Training in Affective and Interpersonal Regulation for refugees and asylum-seekers (STAIR-R) followed by NET (Tissue et al., 2023), and the other through an evaluation of a leadership development programme named ‘Líderes’ (Serrata et al., 2016). ‘Líderes’ is described as a part of a peer-based approach with an adapted manualised programme for leadership training with survivors of DV. The study embedded a mixed-methods design (N = 8) with quantitative data as the primary data type, where single-subject analyses found gains concerning the participant’s self-empowerment relating to leadership competency. The case study (Tissue et al., 2023) described the implementation of STAIR-R, a treatment that targets skill-training of interpersonal and emotional regulation, followed by trauma-focused exposure therapy according to NET. The case study followed a total of 13 individual sessions with a refugee woman with war-related trauma and post-migration stressors, who made improvements in PTSD symptoms and functional gains. Adjustments in the treatment and the phase-based approach were discussed as suitable interventions for patients with ongoing post-migration stressors and limited literacy skills. The intervention was included in the review since STAIR can be delivered in a group format (Moreland & Weiss, 2023).
Psychosocial Interventions Designed for Experiences of Migration and SV and/or IPV
The identified interventions specifically designed for women with experiences of migration and sexual violence/IPV tended to employ a combination of strategies, and were often part of broader programmes that encompassed a variety of services and approaches. Among these, only ‘FASY’ (Logie & Daniel, 2016) adopted a focused approach, solely offering psychoeducation. However, psychoeducation emerged as a common element, featured in the majority of interventions (‘Coming from Afar and Rediscovering Oneself’; ‘Community-based workshops’; ‘Entre Nosotras’; and ‘FASY’). Relaxation techniques and associated activities, such as stress management and yoga, were also widely integrated across interventions (‘Coming from Afar and Rediscovering Oneself’; ‘Community-based workshops’; ‘Entre Nosotras’; ‘Women and Girls Safe Spaces’), while creative activities, though present, were less frequently utilised (‘Coming from Afar and Rediscovering Oneself’; ‘Community-based workshops’; ‘Women and Girls Safe Spaces’). Similarly, therapeutic trauma-processing methods were relatively rare, appearing in two interventions. ‘Coming from Afar and Rediscovering Oneself’ (Benoit et al., 2020) is described as a condensed version of the Den Bosch Phase-Oriented Trauma Treatment and ‘Nguvu’ (Tol et al., 2017) utilises cognitive processing therapy. Skills training was included in only two interventions: ‘Entre Nosotras’ (Greene, Bonz, et al., 2022) focused on problem-solving skills, while ‘Women and Girls Safe Spaces’ (Shair et al., 2019) provided a broader range of life skills.
Coming From Afar and Rediscovering Oneself
‘Coming from Afar and Rediscovering Oneself’ (Benoit et al., 2020) is a 12-session, group-based therapeutic intervention based mainly on creative expression modalities. The intervention, delivered by social workers or psychologists, is held in a community setting. It is centred on a ‘life line’ that spans the past, present, and future. Through creative expression, psychoeducation, and relaxation techniques, participants are supported in integrating traumatic experiences into their life history and re-establishing their identity. A mixed-method evaluation incorporating individual interviews, observation notes, and pre-post self-report questionnaires (N = 17) indicated positive impact, with participants reporting sleeping better, feeling calmer, stronger, and more integrated in society, as well as improved psychological health and fewer symptoms of PTSD (Benoit et al., 2020).
Community-Based Workshop
‘Community-based workshops’ (James et al., 2021) were implemented in Malaysia and Lebanon with the aim of reducing IPV and encouraging help-seeking. The workshops were hosted in easily accessible and non-stigmatising settings, and participants received meals and a stipend to compensate for travel and missed work. The first workshop focused on psychoeducation, the second involved practical activities such as role-play and practising coping skills, and the third focused on developing community-based campaign posters to discourage IPV and encourage help-seeking. Discussion was encouraged in all workshops. A pre–post evaluation (N = 148) indicated reduced acceptability of violence and rigid gender norms, and improvements in mental health, functioning, coping, and self-efficacy following workshop participation. Workshop participation was also associated with increased help-seeking intent, for both mental health and IPV (victims and perpetrators). James et al. (2021) also tested the campaign posters among the broader community in both Malaysia (N = 240) and Lebanon (N = 260), with women reporting lower acceptability of IPV in the areas where the posters were distributed.
Entre Nosotras
Greene, Bonz, et al. (2022) report on the co-design of ‘Entre Nosotras’ through a three-phase process that included needs assessments through community member interviews and mock intervention sessions. Through this formative research, they identified the relevance placed on the social dimension of psychosocial well-being, with the participants prioritising IPV, xenophobia, discrimination, limited livelihood opportunities and challenges meeting basic needs as the most salient mental health and psychosocial problems, and describing emotional distress as influenced by such social, cultural and contextual challenges rather than an isolated problem. As a result, the five-session intervention ‘Entre Nosotras’ was developed to include information on available services and strategies for developing protection pathways in the community, coping and stress management skills, and content related to mobilising social support and learning how to support each other, such as role play. The mock sessions revealed a preference for an in-person format as it was experienced to facilitate sharing with peers and connection with the activities, a need for childcare during the sessions, having a pair of facilitators when possible, and, in some sites, a preference for women from within the community as facilitators. Furthermore, participants preferred sessions to be concluded with strength-based, interactive activities rather than stress management activities, which were noted to lead to strong emotional responses.
FASY
While ‘FASY’ (Logie & Daniel, 2016) is described as targeting HIV prevention, IPV is discussed in the 6-week group intervention, which was implemented with internally displaced women in post-earthquake Haiti. Focus group discussions with participating women (N = 40) revealed that ‘FASY’ promoted intrapersonal, interpersonal, relational, and collective agency (Logie & Daniel, 2016). Women described gaining knowledge on how to protect themselves and how this improved their self-confidence. Their fear of speaking up for themselves with partners lessened. They gained social support from the group and described the value of hearing others’ experiences. Participation in the intervention led to a reduced acceptance of IPV, as well as a strengthened endorsement of women’s rights more generally.
Nguvu
‘Nguvu’ (Greene et al., 2019; Tol et al., 2017) is described as a psychological and advocacy intervention. It was developed to be delivered in a refugee camp in Tanzania, with the intervention name meaning ‘Strength’ in the local language of Kiswahili. The intervention begins with information on IPV, danger assessment, and construction of safety and emergency plans. The sessions then move on to cognitive processing techniques, with a specific focus on safety, trust, power, control, and the impact of distressing events. The intervention concludes with an advocacy session, which includes a review of the safety plan and sharing of coping strategies among group members. In a randomised controlled trial of Nguvu (N = 311; Greene et al., 2021), the women who participated in the intervention reported improvements in depression, anxiety and post-traumatic stress compared to women who received care as usual. A qualitative evaluation of Nguvu involving participating women (N = 10), facilitators (N = 10), a clinical supervisor (N = 1), a project coordinator (N = 1), implementing agency representatives (N = 3), and Community Advisory Board Members (N = 4; Greene, Scognamiglio, et al., 2022) revealed that the intervention met participant needs. Nguvu was considered acceptable, including group discussions on sensitive topics, with confidentiality highly valued, enhancing feelings of safety and acceptance. Training non-specialist refugee workers was considered feasible with supervision. Facilitators noted challenges like limited infrastructure, competing priorities, and population mobility. The intervention was perceived to increase awareness of violence-mental health links, reduce self-blame, and build well-being skills.
Women and Girls Safe Spaces
‘Women and Girls Safe Spaces’ (WGSS; Shair et al., 2019) is described in a brief case study, reporting on individual interviews with two women on their experiences of WGSS and a satisfaction survey with an unknown number of respondents. The two women expressed that participating in WGSS had contributed to their recovery, indicating that the combination of individual contact with a personal caseworker and participation in group activities with other women had been beneficial for them. Both women reported feeling more at ease in contact with other people in the community, and mentioned that strategies such as relaxation techniques and prayer had provided comfort. The survey was reported to show a particular appreciation among respondents for case workers’ support in contacts with other actors, including speedy referrals and accompanying clients to services, with the main source of dissatisfaction being the absence of formal legal systems and security services and the length of the processes.
Discussion
This review aimed to identify psychosocial interventions developed for or tested with migrants with experience of sexual violence and/or IPV. In total, 13 interventions were identified. These included arts-based, therapeutic, and skills-based interventions. Half had been designed for experiences of migration and sexual violence and/or IPV, and half were existing psychosocial interventions used with the target group.
Implications of the Group Format
Findings across various studies (Fernandes & Aiello, 2018; Lakshmin et al., 2018; Logie & Daniel, 2016; Shair et al., 2019) highlighted initial hesitation in joining a group intervention or disclosing experiences in a group setting, demonstrating the need to recognise the difficulty of entering a group setting for people who have experienced interpersonal violence. This indicates that group intervention may need to be coupled with individual intervention, which was the case in some papers (Fernandes & Aiello, 2018; Lakshmin et al., 2018; Shair et al., 2019).
At the same time, the studies did show that group participation was perceived to be helpful for recovery through, for example, contributing to increased trust and comfort in contact with others (Fernandes & Aiello, 2018; Logie & Daniel, 2016; Shair et al., 2019) making sense of traumatic experiences (Fernandes & Aiello, 2018; Lakshmin et al., 2018) and reducing shame (Fernandes & Aiello, 2018; Lakshmin et al., 2018). This aligns with broader literature that shows rebuilding connections within the community can support the recovery process (Sinko & Saint Arnault, 2019; Sinko et al., 2021). In some cases, the group format held practical value too; for instance, Women and Girls Safe Spaces (Shair et al., 2019) facilitated skill-based group exercises focused on working together as a team.
The complexity of joining a group setting is acknowledged in some interventions by interviewing potential participants before joining the group to assess suitability, for example, ‘Coming from Afar and Rediscovering Oneself’ (Benoit et al., 2020), and the incorporation of group rules, for example, ‘Coming from Afar and Rediscovering Oneself’ (Benoit et al., 2020), ‘Entre Nosotras’ (Greene, Bonz, et al., 2022) and ‘Nguvu’ (Greene et al., 2019; Tol et al., 2017).
An interesting aspect to consider is the maintenance of social support that can come from group interventions. This is addressed in the Entre Nosotras intervention (Greene, Bonz, et al., 2022) by the development of an action plan to maintain contact with other participants to facilitate social support. This approach aligns with evidence that refugees resettled in high-income countries experience high levels of isolation and loneliness, particularly women who are experiencing mental health issues (Nguyen et al., 2024).
The Potential for Creative Approaches to Foster Inclusivity
The arts-based approaches identified in the review (Damra, 2022; del Carmen Vera-Esteban & Cardona-Moltó, 2022; Portokaloglou, 2018) were described as offering a particular form of inclusivity by relying on expression through movement, emotion, and creativity, rather than linguistic discourse. One could make the case that such approaches are particularly relevant for individuals from diverse linguistic backgrounds or with varying language abilities, such as migrant and refugee populations, allowing them to connect and express themselves despite language barriers, fostering a sense of belonging and shared experience. Previous research points to the potential importance of physical activity for trauma-affected populations; a recent Swedish RCT demonstrated significant increases in well-being and decreases in symptoms of PTSD, depression and anxiety among refugees participating in a trauma-informed physical activity intervention (Nilsson, 2024). Furthermore, a review of scientific literature on the use of creative therapies with refugees reports positive outcomes (Kolah, 2023), yet identifies a need for more research that specifically focuses on the impact of creative therapies on linguistic barriers when working with refugees.
The Combination of Various Components Among Targeted Interventions
Interventions developed specifically for migrant women with experiences of SV and/or IPV often combined multiple components, with relaxation techniques such as breathing exercises or grounding methods being particularly common. Extant literature on psychological treatment for complex PTSD suggests that relaxation techniques can serve an important function in promoting emotional regulation and providing a sense of stability, which is often necessary before engaging in deeper therapeutic work (Darby et al., 2023). In this way, relaxation practices support participants’ ability to ‘endure’ and stay present during emotionally demanding sessions.
Findings from mock sessions of the Entre Nosotras intervention (Greene, Bonz, et al., 2022) also highlighted participants’ preference for ending sessions with strength-based exercises. These exercises, which focus on personal resilience, positive identity, and coping skills, reportedly helped to foster a sense of empowerment and closure. Together, these practices underscore the importance of pacing, emotional safety, and reinforcing strengths in intervention design for this population.
Participatory Intervention Design
Interestingly, several of the interventions developed specifically for migrant women with experiences of SV and/or IPV incorporated elements of participatory design. After a qualitative needs assessment, Greene, Bonz et al. (2022) conducted participatory workshops to develop Entre Nosotras. Community members were asked to consider how an intervention could improve outcomes for women. Their ideas were documented and distilled into key mechanisms, which were then mapped onto the theories of change of existing interventions to identify and assemble a series of interventional components. Finally, mock sessions were held, and feedback was gathered to refine the intervention. Similarly, interventions were selected and adapted to develop Nguvu (Greene et al., 2019; Tol et al., 2017), which was done in collaboration with a community advisory board.
Taking a different approach, James et al. (2021) integrated participatory action into their community-based workshop intervention. In the third and final workshop, the participants co-designed IPV campaign posters, which were then tested with the wider community. The review only identified formative research on Entre Nosotras (Greene, Bonz et al., 2022); however, positive impact was reported for Nguvu (Greene et al., 2019, 2022, Greene, Scognamiglio, et al., 2021) and the campaign posters designed as part of the community-based workshops (James et al., 2021). These positive results are consistent with the wider literature on participatory research (Cargo & Mercer, 2008), which describes how the process can enhance the relevance and responsiveness of studies to community needs, fostering ownership, empowerment, and capacity building through active engagement. It is argued that participatory research minimises disruption to local contexts, improves credibility, and links participants to needed resources. Additionally, it is considered to increase the cultural relevance of interventions, inform policy and practice, and boost participation rates. Sustained partnerships can further enhance funding opportunities, cross-sector collaboration, and integration across community and government levels.
Peer Delivery
Another interesting design element seen in a couple of the interventions was peer delivery. Internally displaced women were hired and trained to deliver ‘FASY’ (Logie & Daniel, 2016), and refugee GBV survivors were trained to deliver the ‘PM+ Programme’ (Akbay-Safi et al., 2021). While valuable insights were gained through the qualitative exploration of ‘FASY’, which indicated a positive impact on participating women’s agency (Logie & Daniel, 2016), an impact evaluation of the ‘PM+ Programme’ was not conducted as the COVID-19 pandemic prevented the intervention from being implemented. However, the broader literature on peer delivery indicates that group peer support is a promising interventional method for immigrants and refugees, with improvements in social support and emotional well-being reported (Abo-Rass et al., 2025). Yet, the overall evidence base for these interventions remains in the early stages of development (Abo-Rass et al., 2025), and the complexity of supporting migrants who have experienced SV and/or IPV must be held in mind, as well as the potential stress placed upon the peers delivering the interventions.
Quality of Evidence
While the inclusion of RCTs and cohort studies reflects the presence of higher-quality evidence for assessing causal relationships and outcomes, the overall body of literature was primarily composed of qualitative, descriptive and case example studies. These methodologies provide valuable insights into context, processes, and participant perspectives, enriching our understanding of the interventions. The limited number of experimental and longitudinal studies means that the evidence base may be less equipped to support generalisable conclusions or definitive assessments of intervention effectiveness. A further constraint was that some of the papers lacked methodological details, such as sampling strategy, sample size, and analysis methods, which impaired the possibility of assessing the scientific quality and interpreting the presented findings.
The Importance of Clinical Feasibility and Sociocultural Context
When selecting psychosocial interventions for individuals with experiences of migration, sexual violence, and IPV, feasibility is a critical consideration. Barriers such as limited access to services, safety concerns, ongoing risk of abuse, and the need for coordinated responses require careful evaluation of intervention approaches. Lower-intensity interventions that demand less training and supervision may support broader implementation but should not compromise safety or effectiveness. Clear protocols for identifying violence, assessing risk, and coordinating with relevant services are essential to support clinicians and ensure appropriate care. While trauma-focused treatments, such as those involving exposure to traumatic memories, have demonstrated efficacy for PTSD among refugees (McLean et al., 2022; Thompson et al., 2018; Turrini et al., 2019), the evidence is less compelling among female survivors of IPV (Karakurt et al., 2022), and there is some evidence to suggest that trauma-focused treatment leads to higher dropout rates compared with other psychological therapies (Lewis et al., 2020). In many cases, stabilisation-focused approaches, such as emotion regulation skills or empowerment-based CBT, may be more feasible.
It is important to acknowledge, as Greene, Bonz, et al. (2022) do in their paper, that interventional support for migrant women who have experienced violence should take into consideration the sociocultural context. Expectations embedded in some IPV-focused interventions, such as encouraging women to leave abusive relationships, may not be appropriate for all contexts, particularly where cultural norms or migration-related dependency constrain such decisions (Voolma, 2018). Additionally, using PTSD diagnoses as entry criteria for psychosocial support may be inappropriate. Standard PTSD diagnostic frameworks, developed largely in Western settings, may inadequately capture the intersecting and cumulative trauma of SV and/or IPV, and forced migration, highlighting the need for more contextually sensitive approaches (Silove et al., 2017). Practical barriers such as language, literacy, childcare responsibilities, and transportation must also be considered to ensure equitable access (Due et al., 2024). Here, the value of cross-sector collaborations should be noted. Individuals who have experienced forced migration and SV and/or IPV often face multiple, overlapping challenges that require comprehensive and holistic care (Jolof et al., 2024; Robinson et al., 2025).
Among the papers included in this review, Greene, Bonz, et al. (2022) emphasise the need to address practical issues such as employment and livelihoods, meeting basic needs, and support for children and families, as well as mental health support, social and interpersonal problems, and legal concerns. By integrating social support services with mental health interventions, cross-sector collaborations can provide both the practical resources (such as housing, legal aid, and social support) and psychological care needed for healing and recovery. Such an approach can support victim-survivors in receiving tailored, multi-faceted care that addresses both immediate needs and long-term mental health outcomes, fostering resilience and empowerment. We know from the extant literature that this integrated approach can support improved safety and mental health (Karakurt et al., 2022). Accordingly, the Entre Nosotras intervention (Greene, Bonz, et al., 2022) encompasses information on available community resources. Taking a slightly different approach, WGSS (Shair et al., 2019) includes the development of skills necessary for creating a livelihood, for example, tailoring and handicrafts.
Beyond these examples, the included papers do not explicitly describe how the interventions had been designed to address the key challenges faced by migrant women who have experienced SV and/or IPV identified in the broader literature, such as difficulties in seeking care, lack of knowledge about rights and services, fear of deportation, language barriers, or dependency on the perpetrator (Jolof & Rocca, 2023). This lack of detail limits our understanding of how such interventions operate within the complex realities of migrant women’s lives, and of how the interventions have handled the challenges that could come with cross-sector collaborations. Future research should therefore prioritise documenting how interventions are designed and implemented to overcome these intersecting barriers to access, safety, and empowerment.
Methodological Discussion
The involvement of a trained librarian in the review ensured a comprehensive and systematic search strategy, minimising the risk of missing key literature. The inclusion of multiple reviewers enhanced the rigour and reliability of the study, promoting diverse perspectives and reducing potential bias. Furthermore, the blinded review process employed in the initial stage added an additional layer of objectivity, ensuring that study selection was based purely on content relevance rather than reviewer expectations or preconceived notions. These measures collectively improved the credibility and thoroughness of the review.
A further strength was the involvement of public contributors in shaping the review. While patient and public involvement (PPI) in systematic reviews appears to have increased, it remains at a low level (Zhou et al., 2024). Guidance on how to incorporate PPI into systematic reviews has been published (Pollock et al., 2021) and makes the case that PPI is important to ensure that reviews are relevant and meaningful to people affected by a health condition, as well as to the people using the reviews to inform health policy or practice. There is also some evidence to suggest that reviews that have incorporated PPI have a higher potential for broad dissemination (Zhou et al., 2024). Yet, to be involved across all the phases of a literature review places a high demand on public contributors. In line with good PPI practice (Liabo et al., 2020), we employed a proportional involvement approach. The public contributors helped to shape the formulation of the research questions, ensuring that the review addressed service gaps identified by both professionals and those with lived experience. While a clinician was involved in the review process, the public contributors were not involved in the literature searching phase, as the authors perceived this technical task to have a limited scope for meaningful input. Rather, they were re-engaged once the articles had been selected to give input on the identified interventions.
The review has several methodological limitations that should be acknowledged. Despite our comprehensive search strategy, it is possible that evidence on group-based interventions for SV and/or IPV survivors may have been missed, particularly studies not explicitly labelled as targeting migrants. Some interventions designed for broader populations of SV and/or IPV survivors may have included migrant participants or involved culturally relevant approaches that could be beneficial for migrant communities. These missed studies could have provided valuable insights into effective strategies for addressing the unique needs of migrant SV and/or IPV survivors, especially in group-based settings that foster social support and community-building. While full papers in other languages were not excluded, the search was designed to detect records with English titles and abstracts. This may have led to language bias and the exclusion of relevant evidence published in other languages. Moreover, the search was limited to selected electronic databases and did not include hand-searching of journals, conference proceedings, or organisational websites, which may have restricted the breadth of evidence captured. The quality and design of included studies were heterogeneous, with variations in study populations, settings, and intervention types, which limits the ability to draw definitive conclusions or directly compare outcomes. Finally, the review focused on women who experienced forced migration, and findings may not be generalisable to men or to migrants experiencing voluntary migration. Despite these limitations, the review provides a comprehensive overview of contemporary psychosocial interventions targeting a highly vulnerable population and highlights gaps in the current evidence base.
Conclusions
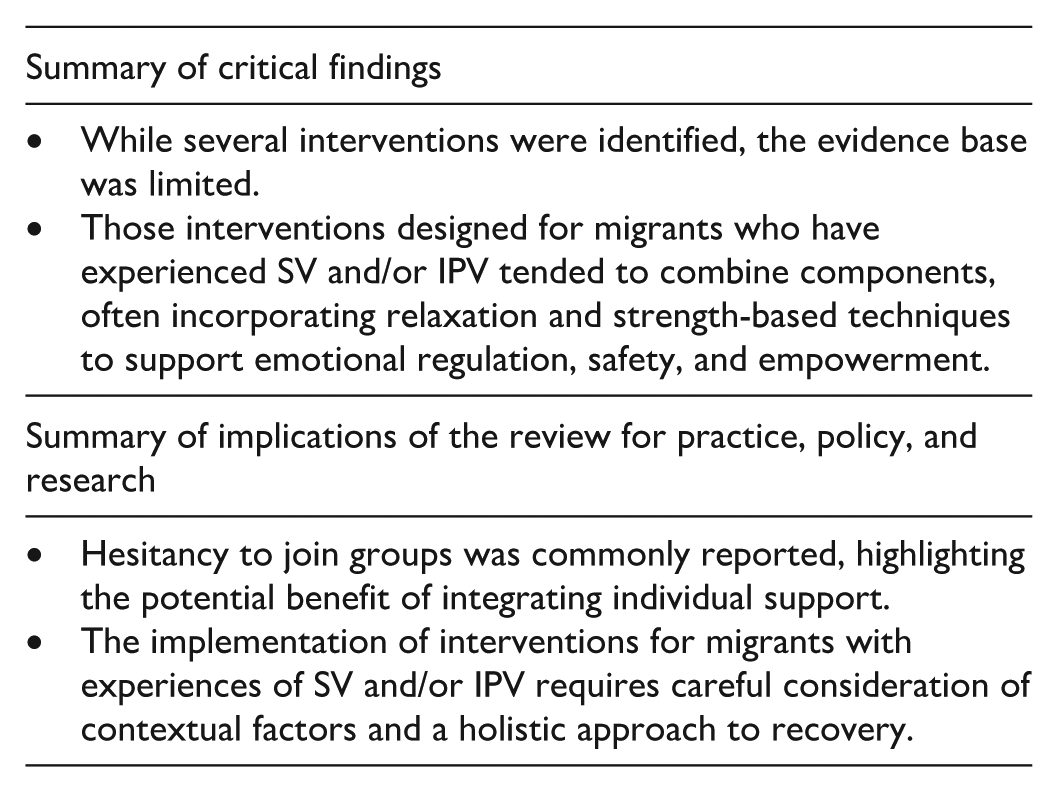
This scoping review mapped the current evidence on psychosocial interventions for migrant women who have experienced SV and/or IPV. While several interventions were identified, the overall evidence base was limited and highly heterogeneous in terms of intervention type, delivery mode, duration, and measured outcomes. Interventions designed specifically for migrant women who have experienced SV and/or IPV tended to combine components. They often incorporated relaxation and strength-based techniques to support emotional regulation, safety, and empowerment. Hesitancy to join groups was commonly reported, highlighting the potential benefit of integrating individual support.
Importantly, there is a lack of rigorous evaluation studies, standardised outcome measures, and long-term follow-up data, limiting conclusions about effectiveness. Given these limitations, a systematic review is not yet feasible; the current evidence base is too sparse and heterogeneous to allow robust synthesis of intervention effects. However, as more high-quality studies become available, a systematic review could provide critical guidance on effective strategies and best practices for supporting this vulnerable population.
Although limited by language, database selection, and heterogeneity among included studies, this review presents an important overview. The predominance of interventions targeting women, combined with the scarcity of high-quality evidence, underscores the ongoing need for rigorous research and highlights key areas for improving intervention design, delivery, and evaluation to meet the psychosocial needs of migrant women affected by SV and IPV. The implementation of interventions for migrants with experiences of SV and/or IPV requires careful consideration of contextual factors and a holistic approach to recovery.
Supplemental Material
sj-pdf-1-tva-10.1177_15248380261423882 – Supplemental material for A Scoping Review of Psychosocial Interventions for Migrant Women With Experiences of Sexual Violence and/or Intimate Partner Violence
Supplemental material, sj-pdf-1-tva-10.1177_15248380261423882 for A Scoping Review of Psychosocial Interventions for Migrant Women With Experiences of Sexual Violence and/or Intimate Partner Violence by Anna Pérez-Aronsson, Elisa Hagby, Frida Johansson Metso and Georgina Warner in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
The authors would like to thank the group of knowledge users who helped shape the aim and research questions for this systematic review, with special thanks to Heba Alanbari, Iman Alsalamah, Miras Ghannoum, Zozan Abu Mohammad, Johanna Belachew, and Tove Filén. We also extend our thanks to the university librarian, Malin Barkelind, at Uppsala University Library, for conducting the systematic review of databases.
Author Contributions
APA and GW led the public involvement process through which this scoping review was conceptualised. FJM and EH are clinicians who participated in the conceptualisation. APA and GW conducted the screening of references, with EH contributing to the later stages of the review process. GW led the original writing, with contributions from APA and EH. APA and GW revised the manuscript, supported by FJM. All authors read and approved the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Centre of Women’s Mental Health during the Reproductive Lifespan (WOMHER) at Uppsala University, and an applied welfare planning grant from the Swedish Research Council for Health, Working Life and Welfare (ref. 2022-01342).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The records identified and screened during the review were managed in Rayyan. All data extracted and analysed are included in this article. Additional information can be made available from the corresponding author on reasonable request.*
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.