
Abstract
This review examines acute sexual assault response systems designed to meet survivors’ immediate medical, forensic, psychological, social, and legal needs following an assault. These systems operate at the intersection of health, justice, and psychosocial domains. By mapping service models and synthesising evidence on their structure and reported outcomes, the review highlights how current approaches address, or fail to address, holistic, survivor-centred care. The analysis aims to inform improvements in accessibility, quality, and responsiveness within acute sexual assault services. A scoping review was conducted following PRISMA-ScR guidelines. Systematic searches of MEDLINE, PsycINFO, and CINAHL (2000–2023) identified peer-reviewed studies describing and/or evaluating acute sexual assault responses for adults (≥18 years). Data were extracted on service components (e.g., medical, forensic, psychological, and advocacy), delivery models, and reported outcomes. Twenty-nine studies were included. Medical care (93%) and forensic examinations (79%) were most frequently described; psychological support (66%) and advocacy (28%) were less common. Only nine studies (31%) evaluated services, with psychological support most assessed (n = 7). Advocacy, though rarely reported, showed strong benefits (e.g., reduced secondary victimisation). Survivor experiences were underrepresented, and studies emphasised procedural compliance over trauma-informed outcomes. Acute sexual assault care remains dominated by medico-legal priorities, with limited evaluation of holistic models. The lack of outcome data, especially for psychological support and advocacy, signals a critical evidence gap. Future research should prioritise multi-site evaluations and survivor-defined outcomes to align services with survivors’ needs.
Introduction
Sexual assault is a pervasive public health and human rights issue with far-reaching consequences. The immediate aftermath of sexual assault represents a particularly critical period, often marked by acute psychological distress, physical trauma, and heightened social vulnerability for victim survivors (Dworkin et al., 2017; Rothbaum et al., 1992). During this time, individuals may encounter a complex network of service providers, including law enforcement, medical and nursing personnel, as well as mental health and social work professionals. The nature, timing, and coordination of these initial responses can significantly influence survivors’ psychological recovery, sense of safety, and engagement with ongoing care (Dworkin & Schumacher, 2018).
Despite the important role of crisis intervention, the systems and structures that underpin acute post-assault care remain heterogeneous and inconsistently evaluated across settings. Variations in service availability, institutional priorities and protocols, as well as interagency coordination, can lead to disparities in care and outcomes for survivors (Campbell, 2006). Moreover, while trauma-informed frameworks have garnered increasing attention (Quadara & Hunter, 2016), there remains a lack of synthesised evidence on how these principles are operationalised in acute response systems for adult sexual assault globally. In this context, “trauma-informed” refers to an approach that recognises the widespread impact of trauma and seeks to create services that prioritise safety, choice, collaboration, trust, and empowerment while actively working to avoid retraumatisation (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014). Applied to acute sexual assault response, trauma-informed care extends beyond individual practitioner behaviour to encompass system-wide practices, such as sensitive forensic protocols, informed-consent procedures, survivor-led decision-making, and cross-sector coordination among health, forensic, and psychosocial wellbeing services (New South Wales (NSW) Health, 2019; National Sexual Violence Resource Center, 2019).
This scoping review aims to systematically map and describe the existing systems, programmes, organisational structures, and support responses that address acute sexual assault in adults. It specifically seeks to identify the range, characteristics, and contextual variations of these responses as documented in the empirical literature, with an emphasis on how care is structured and delivered in the immediate post-assault period (Table 1).
Critical Findings of the Study.
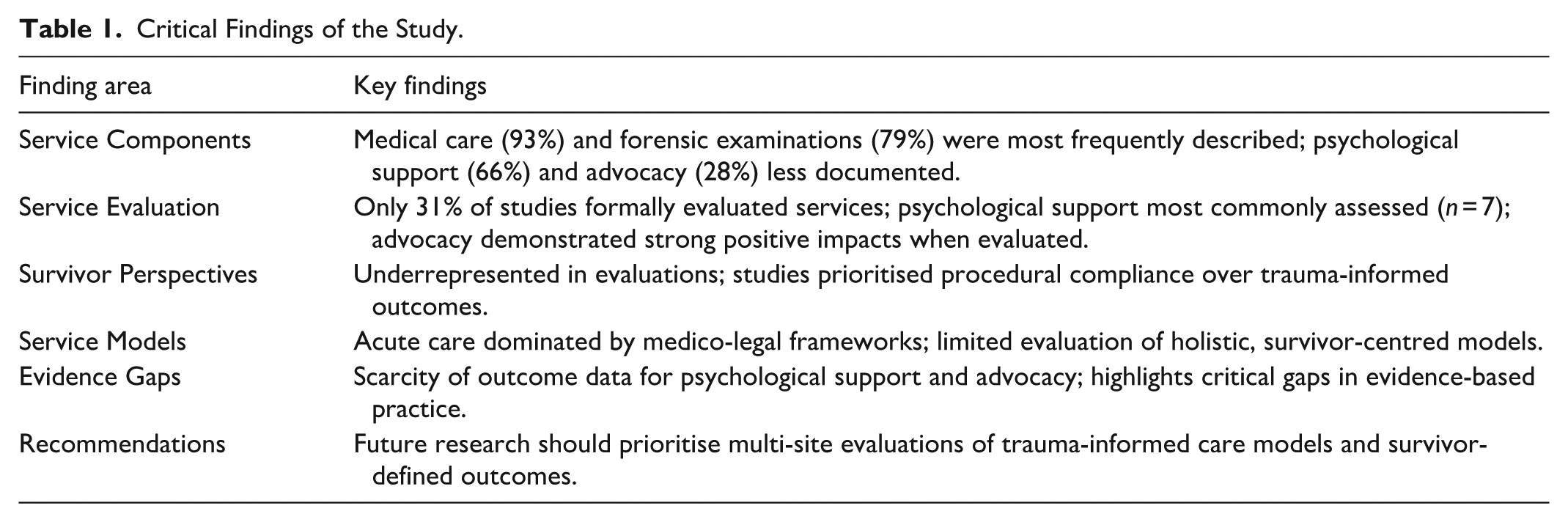
A secondary objective is to assess the extent to which outcomes or indicators of effectiveness are reported in the literature, and to synthesise available evidence regarding the impact of these interventions on the short and long-term wellbeing of victim survivors. Understanding how effectiveness is measured, and where gaps exist in evaluation, is essential to informing evidence-based improvements in service delivery.
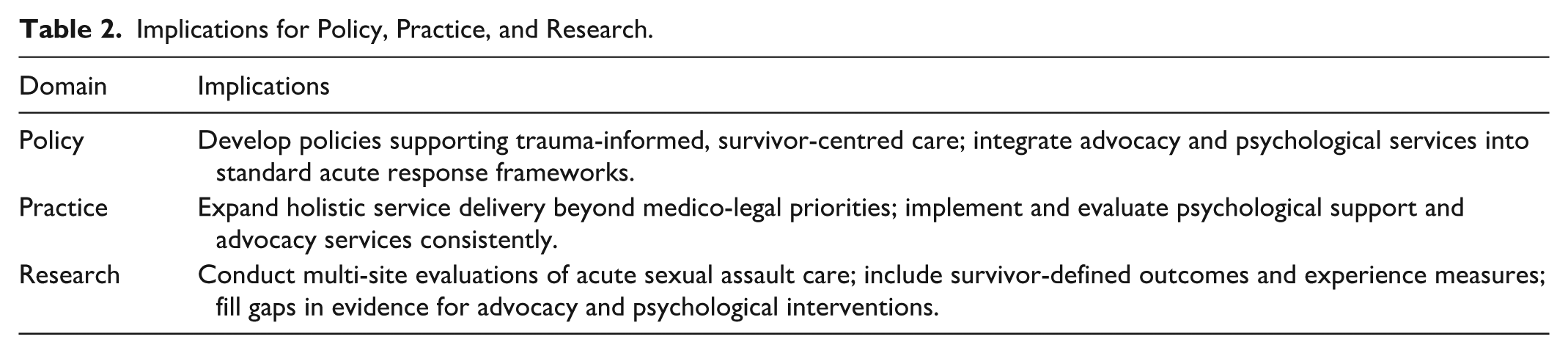
By consolidating existing findings, this review aims to identify common themes, address unmet needs, and highlight opportunities for service improvement and design (Table 2). The insights generated will contribute to ongoing efforts to improve the quality, accessibility, and responsiveness of acute responses for adult survivors of sexual assault.
Implications for Policy, Practice, and Research.
Methods
This review was conducted according to the framework proposed by the Joanna Briggs Institute (Tricco et al., 2018), building upon the previously established guidelines (Arksey & O’Malley, 2005). No protocol was registered or published for this scoping review.
Eligibility Criteria
This review included peer-reviewed sources that described systems, programmes, organisation responses, or support interventions addressing acute sexual assault in adults. In this review, “acute” was defined as care delivered within 72 hr following an assault, aligning with established timeframes for medical, forensic, and psychosocial intervention. However, several studies defined “acute” more broadly (up to 7 days). To capture the full range of service models, such studies were included when responses clearly encompassed the immediate post-assault period, even if care extended beyond 72 hr. Eligible studies focused on adults aged 18 years and over, were published in English, and provided a description and/or evaluation of a formal response mechanism to acute sexual assault. This encompassed both implemented services and descriptive papers that outlined coordinated approaches to acute care delivery.
Studies were excluded if they focused exclusively on responses occurring outside the acute timeframe; centred primarily on survivor or service provider experiences without describing a structured response; involved only children or adolescents under the age of 18; were not peer-reviewed; or were not published in English. Where services addressed both adult and child populations, studies were included if findings relevant to adult responses could be identified.
Information Sources and Search Strategy
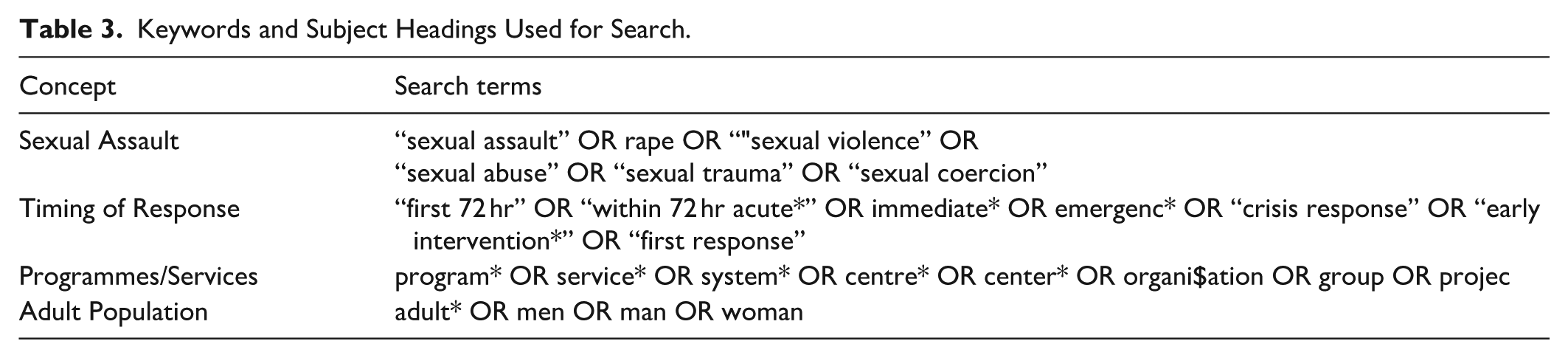
The literature search for this scoping review was conducted in March 2025 and aimed to identify relevant published studies. The following databases were searched from inception to March 2025: MEDLINE (via Ovid), PsycINFO (via Ovid), and CINAHL (via EBSCOhost). Although the initial search covered all available years, a post-hoc decision was made during the screening stage to restrict inclusion to studies published from January 2000 onward to ensure relevance to current practice. The keywords and subject headings used to search these databases are listed in Table 3.
Keywords and Subject Headings Used for Search.
Selection of Sources of Evidence
All identified sources were imported into Covidence (Veritas Health Innovations, 2025) for reference management and screening, and duplicate records were removed. Titles and abstracts were screened for relevance by two independent reviewers (A.S. and C.W). Full-text articles were subsequently assessed for eligibility against the inclusion criteria by the same authors. Discrepancies were resolved by discussion, with author C.W. (content expert) providing the final decision where consensus could not be reached.
Data Charting Process and Data Items
A data charting form, adapted from JBI Methodology for Scoping Reviews (The Joanna Briggs Institute, 2015) was developed in Microsoft Excel to systematically extract relevant information from each included study. The form was refined iteratively based on reviewer consensus. Data charting was conducted by author A.S. and verified by author C.W. (content expert) for accuracy and completeness. Key data items were grouped into the following categories:
Study characteristics: Study design and purpose, country, setting, and population.
Response characteristics: Description and/or name of the programme or system, and the core service components provided (e.g., advocacy, forensic examination, and medical care).
Evaluative elements: Whether outcomes were assessed, the type of outcomes reported, and key findings related to programme effectiveness or service delivery.
Demographic information (e.g., sample size and gender) was extracted only for studies that included direct data collection from survivors, staff, or service users. For descriptive papers focused on service structures or coordination processes rather than outcomes, demographic details were not extracted as they did not meaningfully contribute to the understanding of the model structure. After identifying the service components provided in each study, they were systematically coded into five categories to support synthesis and cross-study comparison. Each study could be coded for multiple service components to reflect the multidimensional nature of acute sexual assault response. These components reflected the core domains of acute post-assault care and were defined as follows:
Advocacy: The presence of a trained advocate or support worker (e.g., rape crisis advocate or SANE support staff) providing emotional, legal, or practical assistance to survivors during the acute care process.
Forensic Examination: The administration of a forensic medical exam, including evidence collection, documentation of injuries, and coordination with legal or law enforcement systems.
Medical Care: The provision of general (non-forensic) medical services, such as treatment of physical injuries, administration of emergency contraception, or pain management.
STI/HIV Management: Testing, prophylaxis, and treatment related to sexually transmitted infections, including HIV post-exposure prophylaxis and follow-up testing or referrals.
Psychological Support: Immediate psychosocial support provided by trained professionals to address acute emotional distress, such as crisis intervention, psychological first aid, or short-term mental health care, including referrals when appropriate.
These codes were applied across studies to guide the structured mapping and descriptive summary of findings, with particular attention to whether individual components were evaluated and what outcomes, if any, were associated with them. No critical appraisal was performed as the aim was to map the evidence rather than assess study quality.
Synthesis of Results
The synthesis involved two main processes: (a) mapping the frequency with which each service component (Advocacy, Forensic Examination, Medical Care, STI/HIV Management, Psychological Support) was described across studies; and (b) identifying which of these components were formally evaluated. Descriptive statistics were used to summarise the proportion of studies that described and/or evaluated each service component.
Given the heterogeneity across study designs, outcomes, and evaluative focus, a thematic synthesis was not conducted. Instead, findings from studies that included evaluative data were summarised using a narrative, study-by-study approach. Although some grouping occurred by service component, the synthesis was primarily structured at the level of individual studies to preserve the specificity of context, methodology, and outcomes reported in each source. This approach allowed for a descriptive overview of the types of components evaluated and the nature of findings associated with each, without drawing overarching thematic conclusions.
Results
Selection of Sources of Evidence
A total of 2,616 records were identified through searches of the three databases and imported into Covidence for screening. After the removal of 780 duplicate records, 1,836 titles and abstracts were screened for relevance. Of these, 95 full-text articles were assessed for eligibility. A further 66 articles were excluded following application of the inclusion criteria, leaving 29 studies for inclusion in the final review. The study selection process is presented in the PRISMA-ScR flow diagram (Figure 1).
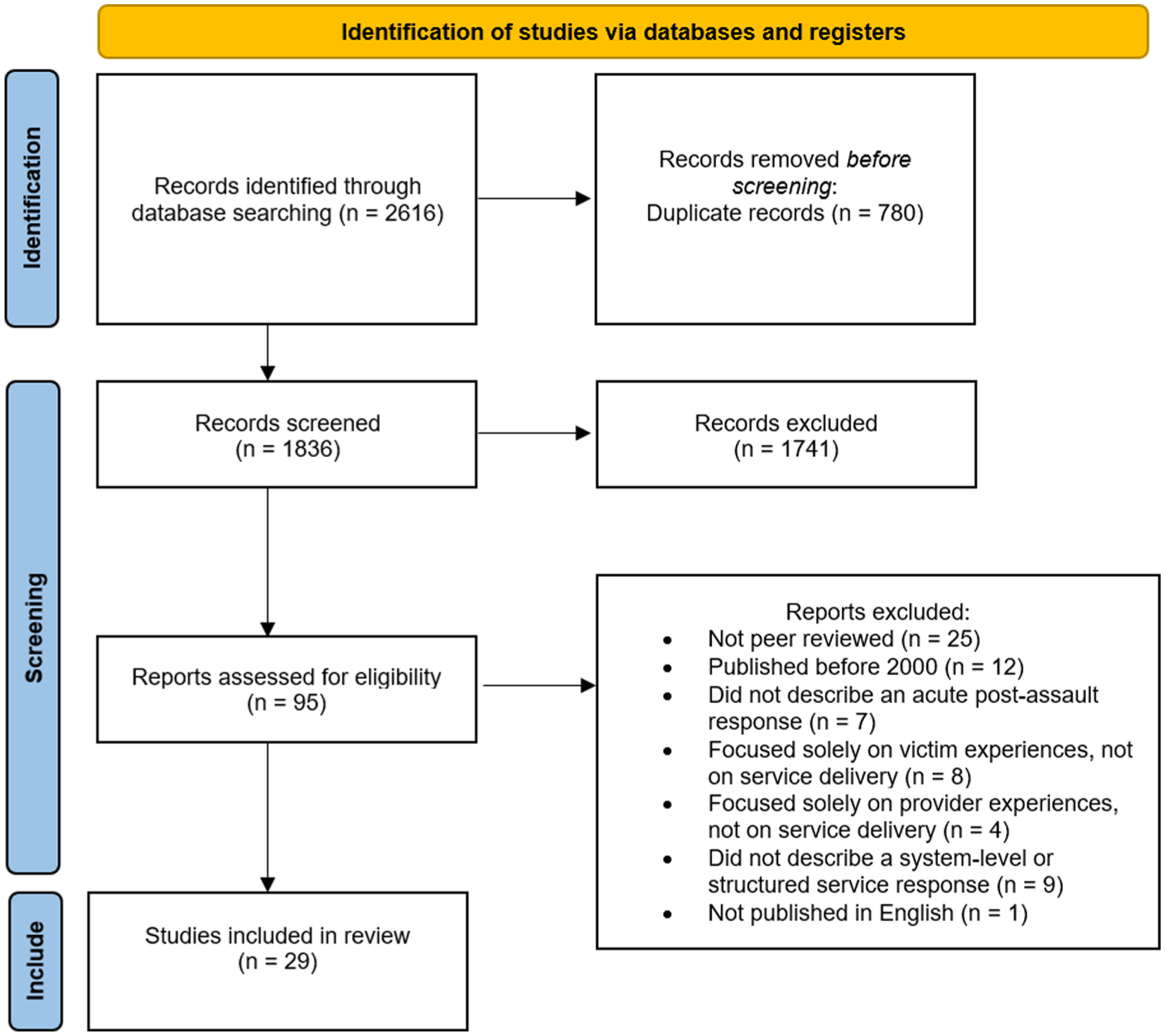
PRISMA 2020 flow diagram outlining the study selection process for the scoping review.
Characteristics of Sources of Evidence
This review included 29 studies conducted across a range of geographic locations. Most were based in high-income countries, with the largest number from the United States (n = 11; Campbell, 2006; Campbell et al., 2012; Chalmers et al., 2023; Darnell et al., 2015; Fehler-Cabral et al., 2011; Krause et al., 2014; Lewis et al., 2003; Patel et al., 2008; Patterson et al., 2006; Resnick et al., 2007; Walsh et al., 2019), followed by the United Kingdom (n = 4; Barron et al., 2023; Cowley et al., 2014; Kerr et al., 2003; Obeyesekera et al., 2007), and additional studies from Canada (Du Mont et al., 2009, 2014), Germany (Gilles et al., 2019; Peeters et al., 2019), and Norway (n = 2 each; Haugen et al., 2024, 2025). The remaining studies were conducted in Australia, Ireland, Spain, and several African countries (n = 8 in total; Debley & Malan, 2020; Inciarte et al., 2020; Kane et al., 2024; Kim et al., 2009; Krolikowski & Koyfman, 2012; Laima et al., 2021; Ranney et al., 2011; Stewart et al., 2025).
Of the studies included, 15 were conducted at a single hospital or centre (Campbell, 2006; Darnell et al., 2015; Debley & Malan, 2020; Du Mont et al., 2009; Fehler-Cabral et al., 2011; Gilles et al., 2019; Haugen et al., 2024, 2025; Kerr et al., 2003; Kim et al., 2009; Krause et al., 2014; Laima et al., 2021; Ranney et al., 2011; Stewart et al., 2025), 13 involved multi-site or national samples (Barron et al., 2023; Campbell et al., 2012; Chalmers et al., 2023; Cowley et al., 2014; Du Mont et al., 2014; Inciarte et al., 2020; Kane et al., 2024; Lewis et al., 2003; Obeyesekera et al., 2007; Patel et al., 2008; Patterson et al., 2006; Peeters et al., 2019; Walsh et al., 2019), and one was conceptual (Krolikowski & Koyfman, 2012). Most studies were set in hospital-based environments, particularly emergency departments (EDs; n = 16; Barron et al., 2023; Campbell, 2006; Chalmers et al., 2023; Darnell et al., 2015; Debley & Malan, 2020; Du Mont et al., 2014; Gilles et al., 2019; Inciarte et al., 2020; Krause et al., 2014; Krolikowski & Koyfman, 2012; Lewis et al., 2003; Patel et al., 2008; Patterson et al., 2006; Ranney et al., 2011; Stewart et al., 2025; Walsh et al., 2019). Others were conducted in sexual assault centres (n = 7; Du Mont et al., 2009; Haugen et al., 2024, 2025; Kane et al., 2024; Kerr et al., 2003; Obeyesekera et al., 2007; Peeters et al., 2019), rape crisis centres (n = 2; Campbell et al., 2012; Cowley et al., 2014), and various outpatient or community-based settings, including academic medical centres and outpatient hospitals (n = 4 combined; Fehler-Cabral et al., 2011; Kim et al., 2009; Laima et al., 2021; Resnick et al., 2007).
A range of study designs was represented, including cross-sectional surveys (n = 8; Barron et al., 2023; Chalmers et al., 2023; Darnell et al., 2015; Du Mont et al., 2014; Lewis et al., 2003; Patel et al., 2008; Stewart et al., 2025; Walsh et al., 2019), qualitative studies (n = 6; Cowley et al., 2014; Debley & Malan, 2020; Du Mont et al., 2014; Fehler-Cabral et al., 2011; Patterson et al., 2006; Peeters et al., 2019), retrospective audits or cohort designs (n = 9; Gilles et al., 2019; Inciarte et al., 2020; Kane et al., 2024; Kerr et al., 2003; Kim et al., 2009; Krause et al., 2014; Laima et al., 2021; Obeyesekera et al., 2007; Ranney et al., 2011), and quasi-experimental studies (n = 2; Campbell, 2006; Campbell et al., 2012). In addition, three randomised controlled trials (including pilot studies) were included (Haugen et al., 2024, 2025; Resnick et al., 2007). One discussion paper was retained due to its relevance to the design of acute response systems (Krolikowski & Koyfman, 2012).
Publication years ranged from 2003 to 2025, with the majority of the studies published in the past decade. While all studies described responses to sexual assault occurring within the acute timeframe (typically defined as within 72 hr), there was some variation in how this was operationalised, with a few studies extending the window to up to 1-week post-assault.
Results of Individual Sources of Evidence
The key characteristics and findings of each included study are summarised in Table 4, outlining their scope, demographic characteristics, response components described and evaluated, measurement methods, and evaluation focus.
Data Extraction Table: Summary of Results and Service Components.
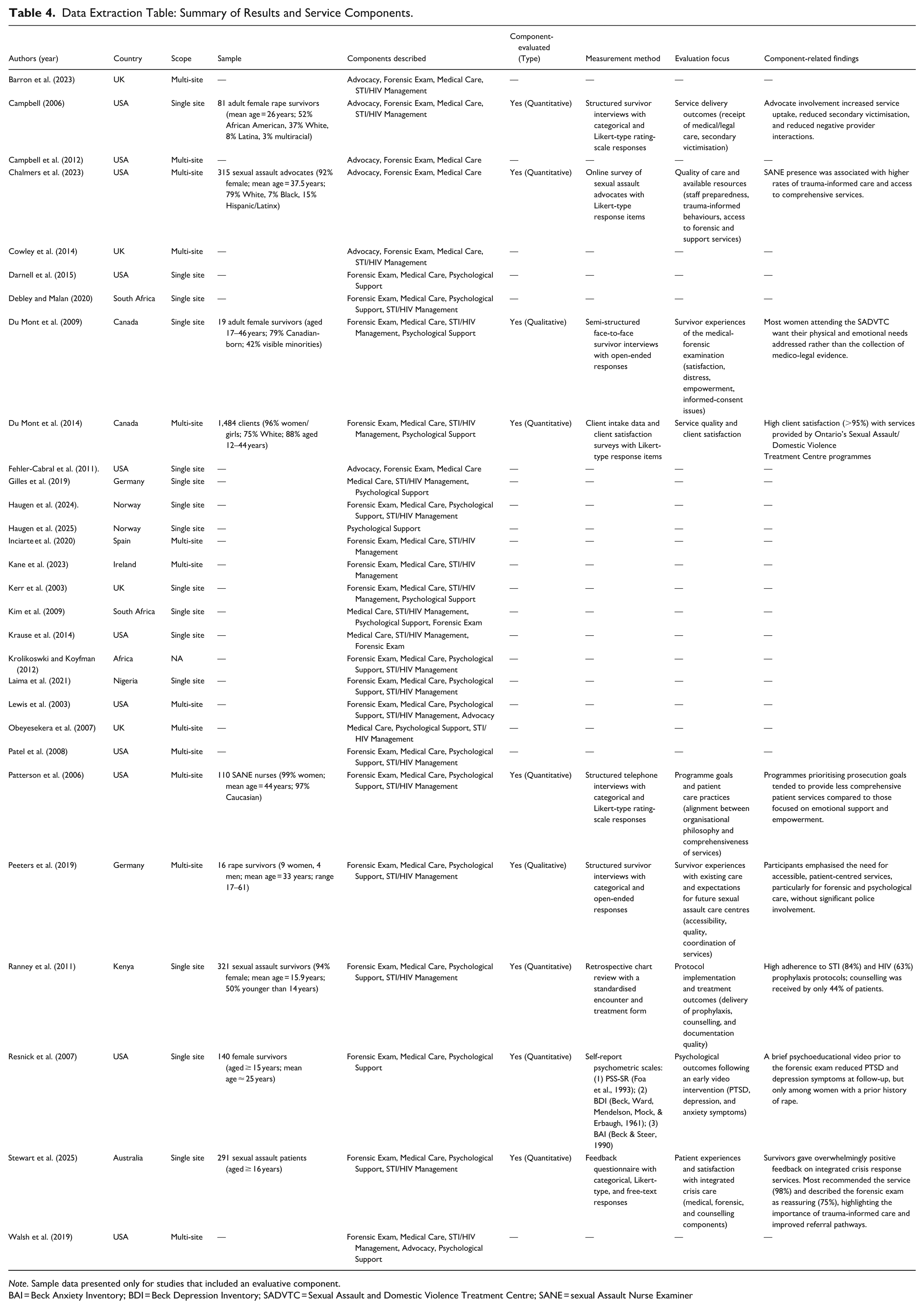
Note. Sample data presented only for studies that included an evaluative component.
BAI = Beck Anxiety Inventory; BDI = Beck Depression Inventory; SADVTC = Sexual Assault and Domestic Violence Treatment Centre; SANE = sexual Assault Nurse Examiner
Synthesis of Results
Frequency of Service Components
Across the 29 included studies, the most frequently described service components were medical care (n = 27, 93%) and forensic examination (n = 23, 79%), followed by STI/HIV management (n = 22, 76%). Psychological support was reported in 19 studies (66%). Advocacy was the least frequently described component, present in only eight studies (28%). It is possible that advocacy or support services were provided in practice but not explicitly described in publications; only studies that clearly identified a distinct advocate or support worker were coded as including advocacy.
Evaluation of Service Components
Of the 29 studies, only nine (31%) formally evaluated any aspect of service delivery. Psychological support was the most frequently evaluated component (n = 7; Du Mont et al., 2009, 2014; Patterson et al., 2006; Peeters et al., 2019; Ranney et al., 2011; Resnick et al., 2007; Stewart et al., 2025), followed by forensic examination (Du Mont et al., 2009, 2014; Patterson et al., 2006; Peeters et al., 2019; Stewart et al., 2025), medical care (Du Mont et al., 2009, 2014; Patterson et al., 2006; Peeters et al., 2019; Stewart et al., 2025), and STI/HIV management (Du Mont et al., 2009, 2014; Patterson et al., 2006; Ranney et al., 2011; Stewart et al., 2025; n = 5 each). Advocacy, though infrequently described, was evaluated in two of the eight studies that reported it (Campbell, 2006; Chalmers et al., 2023). The information is summarised in Table 5 below.
Frequency of Service Components Described and Evaluated (N = 29 Studies).
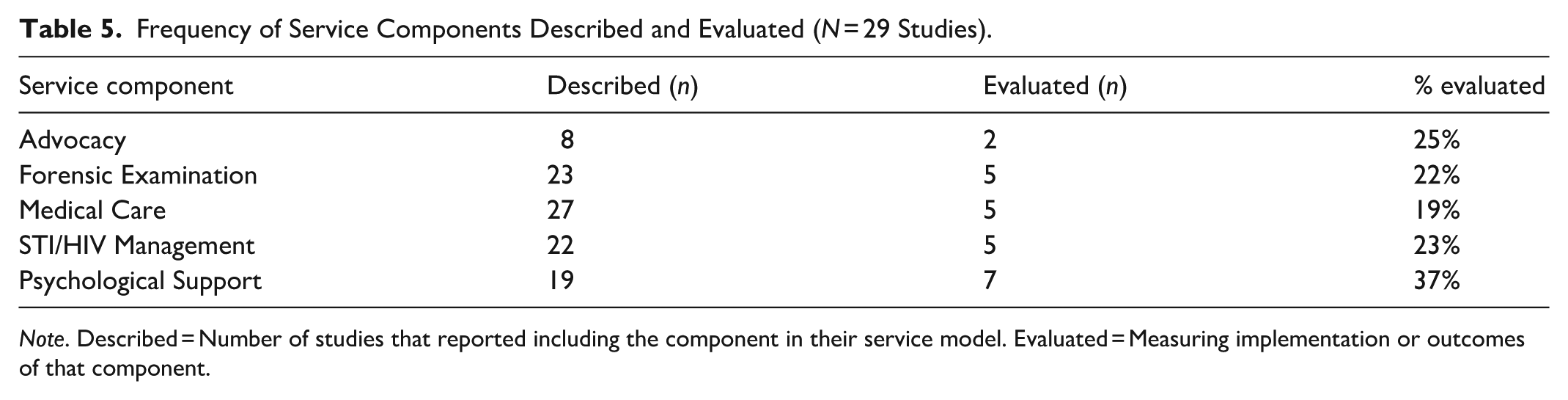
Note. Described = Number of studies that reported including the component in their service model. Evaluated = Measuring implementation or outcomes of that component.
Evaluation methods varied across studies. Survivor experiences were assessed through structured or semi-structured interviews (Campbell, 2006; Du Mont et al., 2009; Peeters et al., 2019) and self-report surveys and/or psychometric scales (Resnick et al., 2007; Stewart et al., 2025). Staff perspectives were captured through telephone or online surveys (Chalmers et al., 2023; Patterson et al., 2006), while service audits and chart reviewers were used to assess procedural adherence and documentation quality (Du Mont et al., 2014; Ranney et al., 2011).
Findings from Evaluative Studies
Nine studies formally evaluated one or more components of acute sexual assault response (medical care, forensic examination, STI/HIV management, psychological support, and advocacy). Campbell et al. (2006) demonstrated that the presence of an advocate increased service uptake, reduced secondary victimisation, and improved provider interactions. Similarly, Chalmers et al. (2023) reported that advocacy through SANEs was associated with higher rates of trauma-informed and comprehensive care. Survivor interviews in Du Mont et al. (2009) and Peeters et al. (2019) highlighted the importance of emotional and psychological support, even within procedural components such as the forensic medical examination. Programmes that prioritised prosecution goals were found to offer less comprehensive care compared to those oriented toward empowerment and survivor wellbeing (Patterson et al., 2006).
Together, these studies highlight the importance of including psychological support and advocacy in the immediate response to sexual assault. However, these elements were evaluated less consistently than medical or forensic care, indicating that their specific impact on survivor outcomes remains insufficiently examined.
Du Mont et al. (2014) and Stewart et al. (2025) reported high levels of satisfaction across multiple service components, including forensic examination, medical care, STI/HIV management, and psychological support, in ED settings in Canada and Australia, respectively. In contrast, Ranney et al. (2011) evaluated a hospital-based service in Kenya. They reported high provision rates of prophylaxis but low uptake of counselling, despite its inclusion in the service protocol. This variation highlights both the importance of psychological care and potential barriers to its uptake in different contexts. Notably, Resnick et al. (2007) found that a brief psychoeducational video shown prior to the forensic exam reduced PTSD and depression symptoms at follow-up, indicating that even low-resource psychological interventions can have measurable impacts during the acute phase.
The included studies overwhelmingly described medical care (93%) and forensic examinations (79%) as core components of acute sexual assault responses across diverse settings. However, only five studies (17%) formally evaluated these elements, and those that did focused primarily on clinical protocol adherence rather than survivor-centred outcomes. Du Mont et al. (2014) and Stewart et al. (2025) conducted quantitative evaluations of medical and forensic services in EDs, reporting high levels of procedural compliance. However, they provided limited insight into how these procedures affected survivor recovery. Notably, studies that included survivor perspectives, such as Du Mont et al. (2009) and Peeters et al. (2019), found that forensic examinations were more tolerable when psychological support was available. These findings highlight the importance of trauma-informed care (SAMHSA, 2014 ) in minimising the risk of overwhelming distress and even retraumatisation during essential medical-legal interventions.
Discussion
Across the 29 included studies, the most frequently described service components were medical care and forensic examination, followed by STI/HIV management. Psychological support was reported in 19 studies, while advocacy was the least frequently described component, present in only eight studies. Only nine formally evaluated any aspect of service delivery. As such, the findings of this scoping review indicate an emphasis on medico-legal priorities within acute sexual assault responses, despite increasing endorsement of more holistic, trauma-informed models (Quadara & Hunter, 2016). More recent studies increasingly reflected this shift towards trauma-informed and integrated care (Haugen et al., 2024, 2025; Peeters et al., 2019) compared to earlier work that focused primarily on establishing medico-legal infrastructure (Kerr et al., 2003; Lewis et al., 2003). When such components were evaluated, they were associated with better engagement, reduced psychological distress, and improved experiences of care (Campbell et al., 2006; Chalmers et al., 2023; Resnick et al., 2007).
Gaps Between Delivery and Experience
Despite their centrality in service delivery, medical and forensic procedures are rarely examined from the survivor’s point of view, which may reflect a persistent institutional focus on evidence collection and prosecutorial goals. Although these forensically focused aims are vitally important, they risk compromising the therapeutic needs of survivors when not balanced with appropriate support. In many studies, service effectiveness was defined by procedural compliance rather than by outcomes that matter to survivors themselves, such as emotional safety, autonomy, and respect (Du Mont et al., 2009; Peeters et al., 2019). Although protocols for forensic evidence collection and prophylactic STI/HIV treatment are well established, it remains unclear whether these procedures are experienced by survivors as supportive or intrusive. Qualitative studies have shown that, in the absence of emotional support, survivors may experience forensic examinations as distressing or even retraumatising (Du Mont et al., 2009), suggesting that procedural adherence alone is an insufficient marker of quality care. This emphasis on procedural care reflects the reality that most acute responses occur in hospital and emergency settings, where medical and forensic imperatives naturally dominate. However, this context does not diminish the importance of survivor-centred and emotionally supportive approaches within these environments.
In contrast to the emphasis on procedural care, psychological and advocacy services were described less consistently across models and varied in their implementation and evaluation. Although psychological support was the most frequently evaluated component, the evaluation differed widely in scope, ranging from survivor interviews (Du Mont et al., 2009; Peeters et al., 2019) and satisfaction surveys (Stewart et al., 2025) to one psychometric trial (Resnick et al., 2007). In addition, psychological care was examined secondarily within a medical-forensic framework rather than a distinct focus. Where psychological support was examined, positive effects such as lower rates of post-traumatic stress and depression symptoms were evident (Resnick et al., 2007). Nonetheless, these interventions were not consistently embedded in care models and often appeared to be treated as supplementary rather than integral to survivor recovery. Similarly, while advocacy was rarely the focus of evaluation, studies that included it, such as Campbell et al. (2006), documented significant benefits, including improved coordination of care and reduced secondary victimisation. Collectively, these findings reinforce the importance of advocacy and psychological support, but also highlight the need for greater consistency and intentional integration of trauma-informed principles within acute services (Choi et al., 2024).
An emerging nuance in the literature relates to the timing and nature of psychological care. While structured counselling may not always be appropriate immediately post-assault, survivors consistently expressed the need for emotional support and clear information during this acute phase (Du Mont et al., 2009; Peeters et al., 2019). In this context, psychological support typically involved brief, on-scene measures such as validation, reassurance, clear and trauma-informed explanation of procedures, and safety planning rather than structured therapy sessions. Across the seven studies, this support was consistently described as informal and immediate, aimed at reducing distress and promoting a sense of safety rather than delivering therapeutic interventions. Formal counselling or psychotherapy was generally deferred to later stages, once acute medical and forensic needs were addressed and survivors were stabilised. This distinction emphasises the importance of differentiating between crisis-oriented psychosocial care and longer-term therapeutic engagement, both of which play complementary roles in recovery.
The methodological limitations of the existing evidence base constrain our understanding of effective practice. Study designs varied substantially, ranging from qualitative case studies (Du Mont et al., 2009) to national surveys (Stewart et al., 2025), yielding inconsistent measures and perspectives that complicate cross-study comparison. Evaluations were often shaped by local contextual factors such as staffing, organisational culture, and resource availability, which restrict the transferability of findings to other settings. These gaps limit progress towards developing evidence-based, survivor-centred standards of care.
The findings illustrate the inherent complexity of post-assault care. Each domain brings distinct priorities and procedural requirements, such as the urgency of forensic evidence collection within narrow timeframes, medical stabilisation, and the need for emotional support, that can compete or overlap in practice. These systemic tensions shape not only service delivery but also evaluation frameworks, which can privilege procedural compliance over survivor-centred outcomes. Addressing these challenges requires integrated models that reconcile medico-legal imperatives with trauma-informed principles, ensuring that care is both technically robust and responsive to survivor wellbeing.
Implications for Research and Practice
While evidence remains limited, this review suggests that acute response integrated medical, forensic, psychological, and advocacy components within a trauma-informed framework are associated with better engagement, lower distress, and more positive survivor experiences (Campbell, 2006; Chalmers et al., 2023; Du Mont et al., 2009; Patterson et al., 2006; Peeters et al., 2019). Models that include emotional support and advocacy alongside procedural care appear to closely align with survivor-centred standards, although implementation requires further evaluation across various service contexts. Future research could prioritise comparative evaluations of service models to determine which components and delivery approaches best support survivor recovery. Particular attention should be given to how psychological support and advocacy are integrated, given their demonstrated contributions to positive outcomes.
Addressing current methodological gaps will require research that examines not only whether care is delivered according to protocol, but also how survivors experience and respond to different approaches. That is, centring survivor perspectives is critical to bridge the disconnect between procedural compliance and trauma-informed care. This may include mixed-methods research that captures both implementation fidelity and survivor-centred outcomes. Research could also explore how medico-legal procedures can be delivered in ways that uphold survivor wellbeing, for example, by assessing whether specialised forensic examiners improve both evidentiary quality and survivor experience compared to generalist providers.
Conclusion
This review highlights gaps between recommended best practices and how acute sexual assault responses are currently delivered and evaluated. While medical and forensic care are widely prioritised and procedurally standardised, psychological support and advocacy, despite their clear benefits, remain inconsistently implemented and under-evaluated. As a result, survivor-centred elements are often peripheral rather than central to post-assault care.
To achieve evidence-informed care, future research must evaluate not only what services are delivered, but how they are experienced. Integrated, trauma-informed service models that embed advocacy and psychological support as core components, not optional components, are urgently needed. Rebalancing priorities to centre survivor wellbeing alongside medico-legal imperatives will be essential to closing the gap between service delivery and survivor needs.
Footnotes
Author Contributions
Andy Sitoh: methodology; screening; data extraction and synthesis (primary); original draft preparation.
Caroline Whitehouse: conceptualisation, screening; data extraction and synthesis (review and verification); draft preparation; supervision; editing and administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.