
Abstract
Many individuals who have experienced behaviors that legally qualify as rape do not “acknowledge” them (or label them) as such. Although the prevalence of and barriers surrounding rape acknowledgment have been substantially researched, its associations with victims’ recovery remain less understood. This systematic review aims to (a) critically assess the methodology used to study the associations between rape acknowledgment and mental health outcomes; (b) explore how rape acknowledgment is associated with mental health outcomes; and (c) identify variables that may influence or explain these associations (e.g., moderators, mediators, and confounders). Three electronic databases (PsycNet, PubMed, and Scopus) were systematically screened following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Peer-reviewed studies written in English and published between 1985 and May 2023 were included if they met the following criteria: (a) employed a quantitative design; (b) assessed rape acknowledgment; (c) assessed psychological distress or post-traumatic stress disorder (PTSD) symptoms; (d) involved adult participants; and (e) presented original data. A total of 26 studies met the inclusion criteria. The included studies primarily focused on the experiences of White undergraduate cisgender women. In most studies, unacknowledged victims reported lower or similar levels of psychological distress or PTSD symptoms compared to acknowledged victims. In some cases, a significant association between rape acknowledgment and psychological distress or PTSD symptoms became nonsignificant after accounting for other variables. Although rape acknowledgment is crucial from a societal standpoint, these findings challenge the assumption that acknowledging a nonconsensual sexual experience as rape inherently facilitates recovery. Instead, rape characteristics and meaning attributions may play a more significant role.
Introduction
Approximately 1 in 4 women and 1 in 26 men in the United States report a lifetime history of attempted or completed rape (i.e., nonconsensual penetrative sexual acts; Basile et al., 2022). Trans and gender-expansive individuals are understudied but tend to report similar or even higher rates of rape compared to cisgender women (Steele et al., 2024; Stotzer, 2009). Although recent social movements have played a pivotal role in raising awareness about this issue (Maier, 2023), many individuals who report experiencing sexual acts that fit the operational definition of rape do not label them as such (Pugh et al., 2024; Wilson & Miller, 2016). Instead, they often use other labels to describe their experiences, such as “a lack of communication,” “a mistake,” or “a bad sexual experience” (Peterson & Muehlenhard, 2011). This phenomenon was first documented by Koss (1985). In her pioneering study, Koss sought to validate a new questionnaire—the Sexual Experiences Survey (SES)—to measure nonconsensual sexual experiences among female college students using behaviorally specific descriptions of sexual acts instead of legal terms, such as “rape,” whose definitions may vary across jurisdictions and be unknown to the general population. The last item of this questionnaire, which was initially intended to assess content validity, directly asked participants if they had ever been raped. Koss inadvertently discovered that 57% of women who reported experiencing a behavior that legally qualified as rape did not label it as such, hence the term “unacknowledged victims.”
Notably, consistent with Koss’s (1985) early work and much of the subsequent published scholarship on this topic, we use the term “victims” in this review to describe individuals who have experienced a nonconsensual sexual experience that meets legal or research definitions of rape. We recognize that this choice of terminology is inherently imperfect, as it does not reflect the perspectives or preferences of those involved. However, it was adopted for consistency with other studies in the field.
In a more recent meta-analysis, Wilson and Miller (2016) corroborated Koss’s early findings by revealing that up to 60% of women who experienced rape do not acknowledge that they have been raped. Although most studies focus on college women, emerging data suggest even higher rates of unacknowledged rape among men and lower rates among trans and gender-expansive people. These differences may be partially explained by men’s greater tendency to adhere to pervasive rape myths compared to women, whereas trans and gender-expansive individuals may be less likely to endorse such beliefs (Anderson et al., 2021; Pugh et al., 2024; Reed et al., 2020).
According to Peterson and Muehlenhard (2011), whether an individual (specifically, a woman, in their study) labels a nonconsensual sexual experience as rape or not depends on how closely the incident aligns with their preconceived notions of rape (e.g., whether the perpetrator fits their image of a rapist, whether they perceive the incident as “forceful” enough to be rape), alongside the perceived consequences of using that label (e.g., feeling more traumatized or obligated to report it to the police). Thus, several barriers may prevent an individual who has experienced a nonconsensual sexual experience from acknowledging it as rape (see Rousseau et al., 2020, for a metasynthesis of qualitative studies on rape acknowledgment barriers in women).
Existing research has provided insights into the prevalence and barriers surrounding rape acknowledgment, but its associations with victims’ recovery remain ambiguous. Although rarely explicitly stated, it is generally assumed that acknowledging rape is beneficial for recovery and failure to do so is often seen as a sign of denial or self-blame among victims. Indeed, even the term “unacknowledged rape” suggests that the individual is in denial about the true nature of their experience. However, it is essential to recognize that acknowledging rape can carry significant risks due to societal stigma, including potential negative impacts on one’s sense of self (e.g., feeling ashamed, powerless or like a “social failure”), interpersonal relationships (e.g., jeopardizing friendships or romantic relationships), and broader life goals (e.g., compromising academic and career opportunities; Khan et al., 2018). If left unaddressed, these negative impacts may also well contribute to adverse mental health outcomes for acknowledged victims.
In an earlier review of the literature, H. L. Littleton et al. (2007) identified inconsistent findings regarding the associations between rape acknowledgment and mental health outcomes, with some studies suggesting that unacknowledged victims experience higher or lower levels of psychological distress than acknowledged victims, and others indicating similar levels across both groups. More recently, H. Littleton et al. (2025) have published an updated overview of the literature on rape acknowledgment since 2006, including its associations with a broad range of post-assault outcomes. The authors conducted two analyses specifically examining mental health outcomes and reported no clear pattern of association between rape acknowledgment and general psychological distress, and a pattern of greater post-traumatic stress disorder (PTSD) symptoms among acknowledged than unacknowledged victims.
Compared to prior literature reviews, the present review offers a more comprehensive synthesis of all relevant quantitative studies published since 1985 that have examined the associations between rape acknowledgment and psychological distress or PTSD symptoms. It focuses on critically evaluating the methodologies used to assess these associations and on identifying key variables (e.g., moderators, mediators, and confounders) that may influence or explain them. Our review aims to clarify for whom, in which contexts, and through what mechanisms, rape acknowledgment is associated with mental health outcomes.
Objectives
This systematic review aims to (a) critically assess the methodology used to investigate the associations between rape acknowledgment and mental health outcomes; (b) explore how rape acknowledgment is associated with mental health outcomes; and (c) identify variables that may influence or explain these associations (e.g., moderators, mediators, and confounders). Specifically, this review focuses on psychological distress, depression, anxiety, and PTSD, as these are among the most studied mental health outcomes of rape (Dworkin et al., 2017).
Method
Eligibility Criteria
This review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Page et al., 2021) guidelines. To be included, studies had to meet the following criteria: (a) use a quantitative design (quantitative portions of mixed methods studies were retained); (b) include a measure of rape acknowledgment; (c) include a measure of psychological distress, anxiety, depression, or PTSD symptoms; (d) involve adult participants (≥ 18 years); and (e) present original data. Only peer-reviewed studies published since 1985 (the year of Koss’s first study of rape acknowledgment) and written in English were screened for eligibility. Studies that focused on sexual harassment (n = 12) or childhood sexual abuse acknowledgment (n = 1), as well as those that failed to distinguish between childhood and adolescent/adulthood rape acknowledgment (since the age of 14; n = 5), were excluded from the review.
When multiple studies relied on overlapping samples, the Standard Quality Assessment Criteria from the Alberta Heritage Foundation for Medical Research (AHFMR; Kmet et al., 2004; described below) was employed to evaluate the quality of each study, and then, the study with the highest quality rating was selected for inclusion. One duplicate study was excluded based on this criterion. Three studies by Wilson & Scarpa (2017) and Wilson et al. (2017, 2018) and two studies by H. Littleton and Henderson (2009) and H. Littleton et al. (2009) were retained despite relying on overlapping samples, as they addressed distinct research questions and were included in separate sections of the manuscript.
Search Strategy
Three electronic databases (PsycNet, PubMed, and Scopus) were searched for peer-reviewed journal articles published from 1985 to May 20, 2023. The following keywords were used to identify all relevant studies: (“rape” OR “sexual* assault*” OR “sexual violence” OR “sexual victim*” OR “nonconsensual sex*” OR “unwanted sex*” OR “sexual* coerc*” OR “forced sex*”) AND (“label*” OR “acknowledg*” OR “hidden” OR “unacknowledg*”). Additionally, reference lists of relevant reviews (e.g., H. L. Littleton et al., 2007; Wilson & Miller, 2016) were examined to ensure a comprehensive assessment of all suitable studies.
Selection Process, Data Extraction, and Quality Assessment
VT (principal investigator) conducted the initial screening of titles and abstracts and the eligibility assessment. NF (last author) and LB (second author) independently evaluated a randomly assigned subset of reports comprising a third of the total and verified the exclusions. VT performed data extraction, with LB cross-checking for accuracy. Any disagreements or discrepancies were resolved through discussion. In cases where consensus could not be reached, ZP (third author) was consulted.
An Excel spreadsheet was created to extract relevant information from the included reports. The Standard Quality Assessment Criteria from the AHFMR (Kmet et al., 2004; see Appendix A for more details) was used to identify key limitations and sources of bias across studies, as well as assess the internal and external validity of our findings. This quality assessment served as a foundation for our critical analysis of the research methods. AL (fourth author) conducted the initial quality assessment. VT independently evaluated a randomly selected subset of reports, comprising one-third of the total, and then cross-checked the entire assessment. Based on the total score, the quality of included studies was categorized as follows: “strong” (>80%; n = 7), “good” (70%–80%; n = 9), “adequate” (50%–70%; n = 6), and “limited” (<50%; n = 4). The assessment focused specifically on the evidence relevant to this review. Some studies received lower scores because rape acknowledgment was examined only as a covariate rather than as a primary variable (e.g., Bhuptani & Messman, 2021; McConnell et al., 2020). As such, these scores should be interpreted within the context of this review’s specific objectives and do not reflect the overall quality of the studies.
Results
Research Methods and Populations of Focus
Study Selection
The search strategy yielded a total of 2,357 reports from the databases, supplemented by five reports from the reference search. Initial screening led to the identification of 210 reports for further review. All full-text reports were retrieved and assessed for eligibility. Upon thorough assessment, 184 studies were excluded from the review, whereas 26 met the inclusion criteria. Detailed reasons for exclusion can be found in Figure 1.
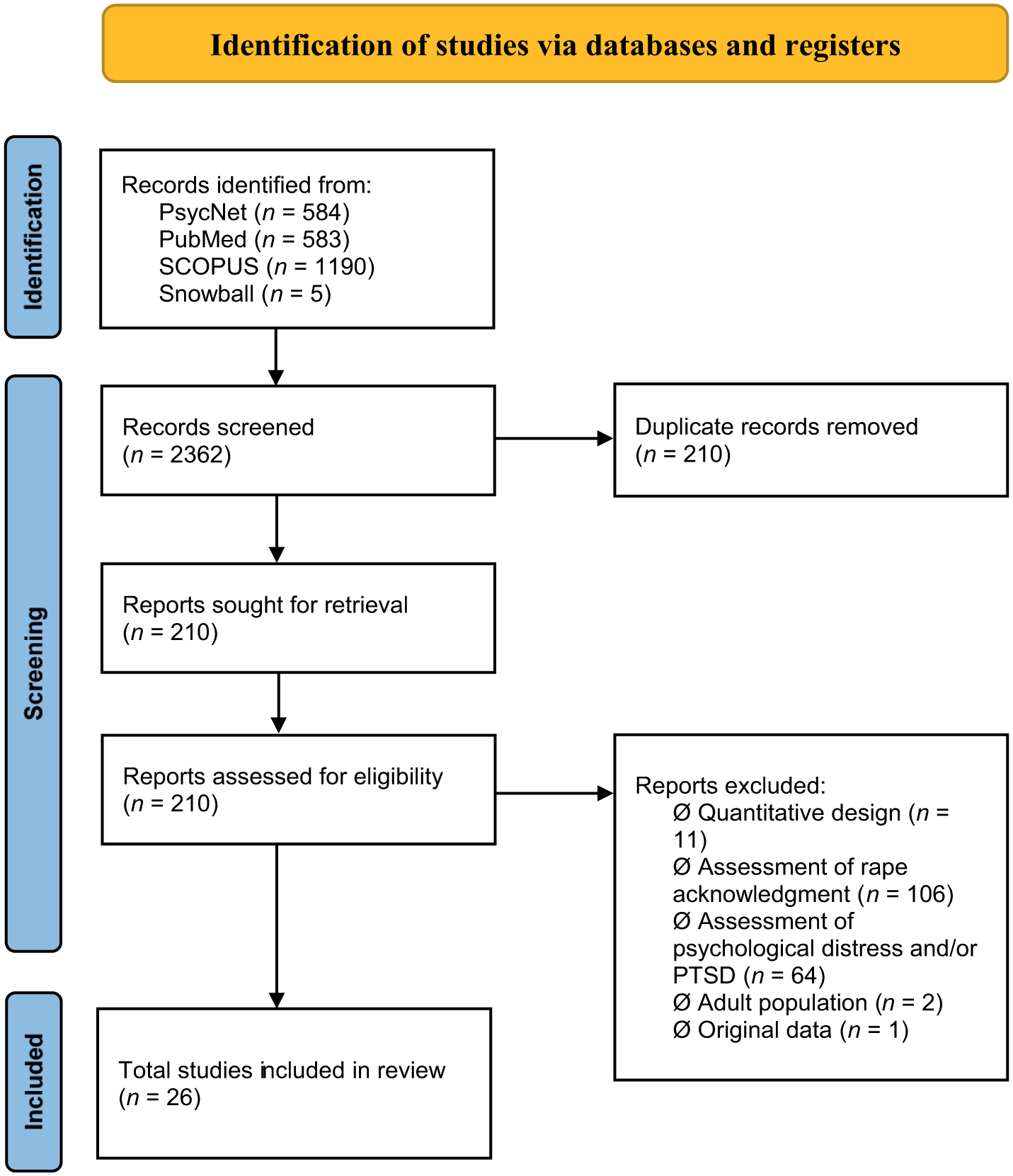
PRISMA flow diagram.
Study Characteristics
All studies were conducted within the United States. Most studies were cross-sectional, with only two relying on longitudinal methods (Maryn & Dover, 2021; McMullin & White, 2006), which limits our ability to draw conclusions about the directionality of the associations between rape acknowledgment and mental health outcomes. Sample sizes varied considerably, ranging from 69 to 1,395 participants. Some studies compared nonvictims to both unacknowledged and acknowledged victims (n = 9), whereas others focused on a subsample of participants who had experienced rape to compare unacknowledged and acknowledged victims (n = 17). Notably, several studies had a relatively small sample size for the acknowledged victim subgroup and did not report power analyses or estimates of variability, raising concerns about the reliability of group comparisons.
Regarding sociodemographic characteristics, most studies focused on women exclusively (n = 23), mainly undergraduate/college women (n = 19). Four studies focused on specific populations, including nonbinary individuals (Anderson et al., 2021), men from the community (Artime et al., 2014), sexual minority women (Blayney et al., 2018), or Latinx students (Maryn & Dover, 2021). White participants were overrepresented in most studies (between 51% and 94% of the samples). Only 10 studies provided information on participants’ sexual orientation. Most of their samples consisted predominantly of heterosexual individuals (between 73% and 95%). Thus, the current body of research remains limited to a fairly homogenous group of people (i.e., White undergraduate cisgender women), which restricts the generalizability of findings. Additional details regarding study characteristics can be found in Table 1.
Characteristics and Results of Included Studies.
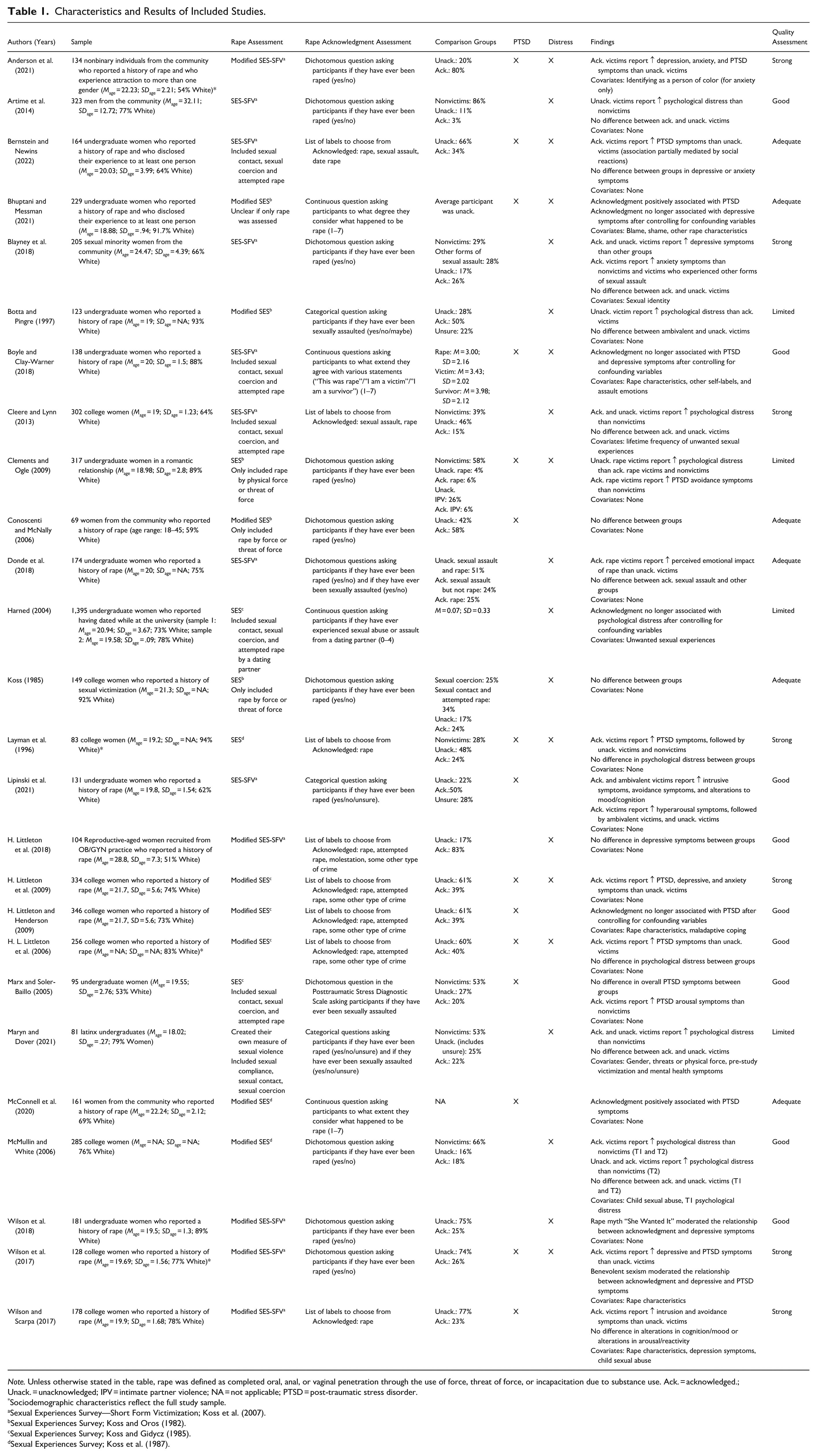
Note. Unless otherwise stated in the table, rape was defined as completed oral, anal, or vaginal penetration through the use of force, threat of force, or incapacitation due to substance use. Ack. = acknowledged.; Unack. = unacknowledged; IPV = intimate partner violence; NA = not applicable; PTSD = post-traumatic stress disorder.
Sociodemographic characteristics reflect the full study sample.
Sexual Experiences Survey—Short Form Victimization; Koss et al. (2007).
Sexual Experiences Survey; Koss and Oros (1982).
Sexual Experiences Survey; Koss and Gidycz (1985).
Sexual Experiences Survey; Koss et al. (1987).
Assessment of Rape Acknowledgment
The conceptualization of rape varied substantially across studies. In most studies, rape was operationalized using the legal definition from the SES, which includes completed oral, anal, or vaginal penetration through the use of force, threat of force, or incapacitation due to substance use (n = 16). However, many authors modified the original items, and thus, definitions may not be exactly equivalent across studies. Three studies defined rape more narrowly, only including oral, anal, or vaginal penetration by force or threat of force (Clements & Ogle, 2009; Conoscenti & McNally, 2006; Koss, 1985), whereas six studies defined it more broadly, also including instances of attempted rape, unwanted sexual contact, and/or sexual coercion (Bernstein & Newins, 2022; Boyle & Clay-Warner, 2018; Cleere & Lynn, 2013; Harned, 2004; Marx & Soler-Baillo, 2005; Maryn & Dover, 2021).
There was also considerable variation in how rape acknowledgment was measured across studies. Although no universally validated measure exists for this concept, most studies used the single item from the SES, “Have you ever been raped?” (yes/no), to assess rape acknowledgment. Following the SES structure, this item was typically positioned at the end of a series of behaviorally specific descriptions of nonconsensual sexual experiences, including rape.
To distinguish between unacknowledged and acknowledged victims, researchers typically compared participants’ responses to the behaviorally specific descriptions of rape with their answers to the acknowledgment question. Those who endorsed at least one behaviorally specific rape item and answered “yes” to the acknowledgment question were categorized as acknowledged victims. Conversely, those who endorsed at least one behaviorally specific rape item but answered “no” to the acknowledgment question were categorized as unacknowledged victims. Notably, in this method, researchers cannot be certain that the experience endorsed in the behaviorally specific item is the same experience that the participant labels as rape; in other words, the acknowledgment question is not tied to a specific incident of nonconsensual sex. Moreover, this binary framework oversimplifies what is likely a nuanced and dynamic process.
Some authors used a rape acknowledgment measure that allowed for more variability and flexibility in response choices. For instance, in four studies, researchers replaced the binary response option with a continuous scale, enabling participants to provide a more nuanced response (Bhuptani & Messman, 2021; Boyle & Clay-Warner, 2018; Harned, 2004; McConnell et al., 2020). In others, researchers added an “unsure” response option to capture participants’ ambivalence (Botta & Pingre, 1997; Lipinski et al., 2021; Maryn & Dover, 2021). Additionally, in eight studies, multiple potential labels were proposed for participants to choose from, such as “serious miscommunication,” “sexual assault,” “a crime other than sexual assault or rape,” “hook-up,” “bad sex,” “not sure,” and “other” (with the option to add another label). However, there was variability among researchers in how they interpreted and classified some labels. For example, although some researchers considered participants who labeled their experience as “some other type of crime” as acknowledged victims (H. Littleton & Henderson, 2009; H. Littleton et al., 2009, 2018; H. L. Littleton et al., 2006), others classified them as unacknowledged (Bernstein & Newins, 2022; Cleere & Lynn, 2013; Layman et al., 1996; Wilson & Scarpa, 2017).
Researchers who considered other types of nonconsensual sexual experiences (e.g., attempted rape, unwanted sexual contact, and sexual coercion) generally adapted their definition of an “acknowledged victim” by including participants who labeled their experience as “sexual assault,” “date rape,” “sexual abuse from a dating partner,” “attempted rape,” or “molestation.” However, some authors, arguably, misclassified participants as unacknowledged victims by including nonconsensual sexual experiences that do not legally qualify as rape (e.g., sexual coercion) in the rape acknowledgment measure. In sum, the lack of consensus in operationalizing rape and rape acknowledgment introduces substantial heterogeneity across studies, which directly impacts the comparability of findings across studies. Additional information on rape and rape acknowledgment measures can be found in Table 1.
Assessment of Mental Health Outcomes
Most authors used validated scales to assess mental health outcomes; however, some employed non-validated single-item measures (Donde et al., 2018; Koss, 1985) or custom scales (Botta & Pingre, 1997). Studies focusing on depression, anxiety, or psychological distress were grouped into a single section in this review, as these conditions often overlap, and many studies did not differentiate between them. Studies on PTSD were analyzed separately due to its distinct classification as a trauma-related clinical disorder.
Associations Between Rape Acknowledgment and Mental Health Outcomes
Psychological Distress
Twenty studies focused on the association between rape acknowledgment and psychological distress, including depression and anxiety. Of these, ten found no significant difference in psychological distress between acknowledged and unacknowledged victims (Artime et al., 2014; Bernstein & Newins, 2022; Blayney et al., 2018; Cleere & Lynn, 2013; Koss, 1985; H. Littleton et al., 2018; H. L. Littleton et al., 2006; Layman et al., 1996; Maryn & Dover, 2021; McMullin & White, 2006). Conversely, seven studies found that acknowledged victims experienced higher levels of psychological distress compared to unacknowledged victims (Anderson et al., 2021; Bhuptani & Messman, 2021; Boyle & Clay-Warner, 2018; Donde et al., 2018; H. Littleton et al., 2009; Harned, 2004; Wilson et al., 2017). Five out of eight studies that included a nonvictim comparison group found that both acknowledged and unacknowledged victims exhibited higher levels of psychological distress compared to nonvictims (Blayney et al., 2018; Cleere & Lynn, 2013; Harned, 2004; Maryn & Dover, 2021; McMullin & White, 2006).
Only three studies found that unacknowledged victims reported higher levels of psychological distress than acknowledged victims and/or nonvictims (Artime et al., 2014; Botta & Pingre, 1997; Clements & Ogle, 2009), whereas one found no significant differences in psychological distress between nonvictims and either acknowledged or unacknowledged victims (Layman et al., 1996). These results are discussed below.
Layman et al. (1996) observed that unacknowledged, acknowledged, and nonvictims reported comparable levels of psychological distress. The authors suggested that this similarity may result from a natural fading of immediate post-rape symptoms for many victims. However, it is worth noting that 15% of unacknowledged victims in this study believed that they had experienced “a crime other than rape,” meaning that even though they did not use the label “rape,” they did recognize the experience as victimization. This could have contributed to the absence of discernible differences in reported levels of psychological distress between acknowledged and unacknowledged victims.
Artime et al. (2014) examined the association between rape acknowledgment and psychological distress among male participants. They found that unacknowledged victims experienced higher levels of psychological distress compared to nonvictims. Interestingly, acknowledged victims had a higher overall score of psychological distress (M = 45.60; SD = 41.81) than both nonvictims (M = 25.80; SD = 22.94) and unacknowledged victims (M = 38.50; SD = 29.30). However, the difference between the nonvictim and unacknowledged groups was the only one that reached statistical significance, which may be attributable to the small sample size of acknowledged victims (n = 11).
Botta and Pingre (1997) compared victims who were “unsure” if they had ever been raped (i.e., ambivalent victims) to unacknowledged and acknowledged victims on psychological distress. They found that acknowledged victims reported less psychological distress than unacknowledged or ambivalent victims, but no significant difference emerged between ambivalent victims and unacknowledged victims. However, it is important to note that the authors did not use a validated measure of psychological distress. Instead, participants were asked to assess the extent to which emotional problems interfered with their work and social activities and the frequency of various positive and negative feelings experienced over the last two months.
Finally, Clements and Ogle (2009) are the only ones to have found that unacknowledged victims generally reported higher levels of psychological distress compared to both nonvictims and acknowledged victims. Unlike other studies, the researchers compared mental health outcomes across five groups: acknowledged rape victims (n = 18), unacknowledged rape victims (n = 14), acknowledged intimate partner violence victims (n = 19), unacknowledged intimate partner violence victims (n = 81), and nonvictims (n = 185). Although this study is often cited to support the hypothesis that unacknowledged victims report more psychological distress than acknowledged victims, the relatively small sample sizes and unique composition of its groups warrant cautious interpretation.
Post-Traumatic Stress Disorder
Fifteen studies focused on the association between rape acknowledgment and PTSD. Of these, eight found that acknowledged victims experienced more PTSD symptoms compared to unacknowledged victims (Anderson et al., 2021; Bernstein & Newins, 2022; Boyle & Clay-Warner, 2018; H. Littleton et al., 2009; H. L. Littleton et al., 2006; Layman et al., 1996; Lipinski et al., 2021; Wilson et al., 2017). This trend persisted even when researchers utilized a continuous measure of rape acknowledgment (Bhuptani & Messman, 2021; McConnell et al., 2020). No study found that unacknowledged victims exhibited more PTSD symptoms than acknowledged victims, and only four studies suggested no discernible difference in overall PTSD symptoms between these two groups (Clements & Ogle, 2009; Conoscenti & McNally, 2006; H. Littleton & Henderson, 2009; Marx & Soler-Baillo, 2005).
Six studies examined the associations between rape acknowledgment and specific clusters of PTSD symptoms. However, it is not possible to draw definitive conclusions from these studies due to variations in the PTSD clusters assessed, which often corresponded to different versions of the Diagnostic and Statistical Manual of Mental Disorders (DSM). Nonetheless, two studies found positive associations between rape acknowledgment and all clusters of PTSD symptoms (intrusive symptoms, avoidance, and hyperarousal; Layman et al., 1996; McConnell et al., 2020), whereas four studies indicated variations based on specific clusters. These results are outlined below.
Clements and Ogle (2009) found no significant difference in intrusive symptoms between acknowledged, unacknowledged, and nonvictims, but acknowledged victims reported more avoidance symptoms compared to nonvictims. Wilson and Scarpa (2017) observed that acknowledged victims reported higher levels of intrusive and avoidance symptoms compared to unacknowledged victims, with no significant difference between the two groups in alterations in cognition and mood or in arousal and reactivity. Lipinski et al. (2021) compared unacknowledged, ambivalent, and acknowledged victims and found that the latter two groups reported comparable levels of intrusive symptoms, avoidance symptoms, and alterations in cognition and mood, all of which were higher than those reported by unacknowledged victims. As for alterations in arousal and reactivity, acknowledged victims exhibited significantly higher symptoms than ambivalent victims, who, in turn, exhibited significantly higher symptoms than unacknowledged victims. Finally, Marx and Soler-Baillo (2005) found that acknowledged victims reported greater alterations in arousal and reactivity than unacknowledged victims; however, no differences were observed in intrusive or avoidance symptoms, nor in overall severity scores.
Moderators, Mediators, and Confounding Variables
Only 10 studies accounted for covariates in their analyses. These variables ranged from sociodemographic and baseline characteristics to child sexual abuse history, mental health issues, and rape-related characteristics. Notably, Wilson and Scarpa (2017) found that acknowledged victims reported higher levels of intrusive and avoidance symptoms than unacknowledged victims, even after controlling for rape characteristics and severity of child sexual abuse. In contrast, other researchers observed that the associations between acknowledgment and mental health outcomes became nonsignificant when rape characteristics were controlled for, suggesting that they might act as confounding factors (Bhuptani & Messman, 2021; Boyle & Clay-Warner, 2018; H. Littleton & Henderson, 2009; Harned, 2004). These findings are further discussed below.
Bhuptani and Messman (2021) found that rape acknowledgment was positively correlated with both PTSD and depressive symptoms among victims who disclosed their experience to at least one person. However, after controlling for rape characteristics (resistance, freeze response, and injury/pain) and post-assault experiences (blame and shame), only the association with PTSD remained significant. Interestingly, rape acknowledgment was also linked to higher levels of rape-related shame, which, in turn, was correlated with heightened PTSD symptoms. This indirect path, however, was not formally tested because it fell outside the scope of the study.
Boyle and Clay-Warner (2018) investigated how women labeled their most recent nonconsensual sexual experience (“this was rape”) and themselves (“I am a victim”/“I am a survivor”) using continuous scales. Bivariate correlations showed that all labels were positively associated with PTSD and depressive symptoms, except for “survivor,” which was not related to depressive symptoms. However, in multivariate analyses, the label “rape” was no longer associated with PTSD and depressive symptoms after controlling for self-labels, rape characteristics, and assault-related emotions. Instead, self-identifying as a victim was positively associated with PTSD symptoms, whereas identifying as a survivor was negatively associated with depressive symptoms. These findings suggest that self-identification may have a stronger association with mental health outcomes than labeling the experience as rape.
Harned (2004) examined whether psychological distress among undergraduate women was predominantly influenced by the frequency and types of nonconsensual sexual experiences (behaviorally specific items), their self-assessment of having experienced “sexual abuse or assault” (labeling item), or both. They found that psychological distress was directly associated with the frequency and types of nonconsensual sexual experiences and that labeling did not mediate this relationship. These findings suggest that psychological distress is more related to the nature of the experience than to the label used to describe it. However, an important limitation of this study is that a score of 0 on the labeling question could indicate either non-victimization or lack of acknowledgment, conflating two fundamentally different experiences.
Finally, H. Littleton and Henderson (2009) found that rape acknowledgment was no longer associated with PTSD symptoms after accounting for rape characteristics (perpetrator’s force and victim’s resistance) and maladaptive coping strategies (wishful thinking, social withdrawal, and self-criticism). Their model suggested that more violent assault predicted greater use of maladaptive coping strategies, which, in turn, was associated with higher levels of PTSD symptoms. Although rape acknowledgment was associated with more violent assaults, it did not significantly mediate the relationship between rape characteristics and PTSD symptoms. The authors concluded that differences in PTSD symptoms were better explained by assault severity and coping strategies than by rape acknowledgment.
Only three studies focused on mediating (n = 1) or moderating variables (n = 2) that might explain or qualify the associations between rape acknowledgment and psychological distress or PTSD symptoms. Bernstein and Newins (2022) tested a mediation model to examine whether social reactions explained the association between rape acknowledgment and mental health outcomes among undergraduate women who disclosed their nonconsensual sexual experience to at least one person. Their analyses revealed that acknowledged victims reported more turning against responses (e.g., stigmatization, infantilization, and blaming) and more positive social responses (e.g., emotional support and tangible aid) than unacknowledged victims. Both types of responses were associated with higher levels of PTSD symptoms, although no significant indirect effects emerged for anxiety and depression. The authors hypothesized that acknowledged victims may experience more severe assaults, leading to greater disclosure, and both more positive and negative responses from disclosure recipients. Their findings thus underscore the potential role of stigmatizing responses and rape characteristics in shaping the association between rape acknowledgment and PTSD symptoms.
Wilson et al. (2017, 2018) explored how sexism and rape myth acceptance may moderate the associations between rape acknowledgment and mental health outcomes. In their 2017 study, they found that benevolent sexism (i.e., inclination to offer protection and affection toward women in traditional and restricted roles), but not hostile sexism (i.e., blatant animosity toward women), moderated these associations. Specifically, acknowledged victims with low levels of benevolent sexism reported the highest levels of depressive and PTSD symptoms, followed by acknowledged and unacknowledged victims with high levels of benevolent sexism, and unacknowledged victims with low levels of benevolent sexism. Thus, acknowledgment was associated with greater distress only when benevolent sexism was low. The authors postulated that women who reject notions of inferiority to men, including stereotypes of fragility or dependence, may experience heightened self-blame following rape, thus intensifying depression and PTSD symptoms. In their 2018 study, they found that, although overall acceptance of rape myths did not significantly moderate the association between rape acknowledgment and depressive symptoms, a significant interaction emerged for the “she wanted it” rape myth (PTSD was not included in this study). Among those who more strongly accepted this specific myth, acknowledged victims reported more depression than unacknowledged victims. Importantly, among seven different rape myths tested, only this one moderated the association between acknowledgment and depression, suggesting limited support for the moderating role of rape myths. Taken together, these two studies suggest that the associations between rape acknowledgment and mental health outcomes may depend somewhat on the meaning attributed to the experience, particularly in terms of self-blame.
Discussion
Acknowledging a nonconsensual experience as rape can serve as a significant turning point for victims to begin their healing process, notably by helping them gain deeper insight into the impact of the assault, reframe their perceived role in it, process distressing memories, and reclaim a sense of hope and agency (Draucker et al., 2009; Sinko et al., 2022). Yet, quantitative studies examining the associations between rape acknowledgment and mental health outcomes have yielded mixed findings. We aimed to gain a clearer understanding of these discrepancies by critically evaluating the existing literature on the associations between rape acknowledgment and psychological distress and PTSD symptoms.
Although rape acknowledgment is often viewed by practitioners as inherently beneficial to recovery, the findings from this review challenge this widespread assumption. Indeed, most studies found that acknowledged victims reported equivalent or higher levels of psychological distress and higher PTSD symptoms compared to unacknowledged victims. However, interpreting these findings as evidence that acknowledgment is harmful or that unacknowledged victims do not experience substantial distress would be both reductive and misleading. In fact, our review also revealed that unacknowledged victims generally reported higher levels of psychological distress than individuals who have not experienced rape, with some evidence suggesting that approximately 60% of them experience depressive or PTSD symptoms likely meeting diagnostic criteria (Littleton & Henderson, 2009; Littleton et al., 2018). Taken together, these findings suggest that rape acknowledgment may be distressing, healing, or both, depending on the individual and the circumstances under which it occurs. This points to a more important question: For whom, in what contexts, and through what mechanisms does rape acknowledgment relate to mental health outcomes? Unfortunately, the existing research does not yet provide clear answers to those questions, though some broad patterns are beginning to emerge. Indeed, there is some evidence suggesting that the associations between rape acknowledgment and mental health outcomes may be more accurately attributed to the characteristics of the assault itself and the meaning attached to it than the label used to describe it. These patterns are discussed below (see Table 2 for a summary of critical findings).
Critical Findings.
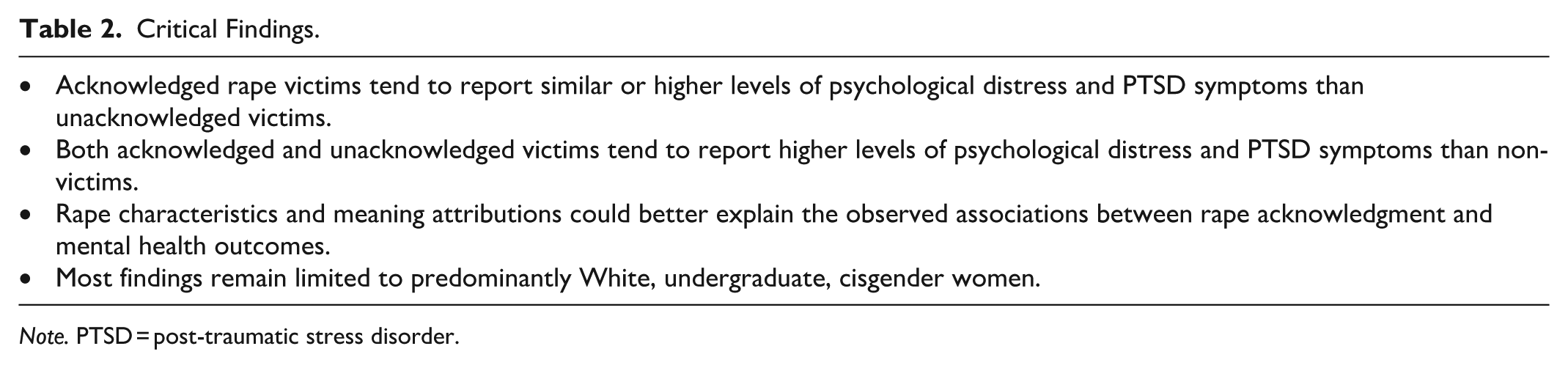
Note. PTSD = post-traumatic stress disorder.
Many of the reviewed studies conducted analyses comparing unacknowledged and acknowledged victims on rape characteristics and found that stereotypical rape characteristics (i.e., higher degree of perpetrator-inflicted force, physical injury, and victim resistance) were associated with increased likelihood of acknowledgment (e.g., Cleere & Lynn, 2013; Donde et al., 2018; H. Littleton et al., 2018; Lipinski et al., 2021) and with higher levels of psychological distress and PTSD symptoms (Bhuptani et al., 2021; McConnell et al., 2020). These results mirror those of a metasynthesis of qualitative studies, which found that women are less likely to label an experience as rape when it does not match with their preconceived notions of what constitutes rape (Rousseau et al., 2020). A major limitation of the current literature is that relatively few studies included these variables as covariates in multivariate analyses. Among those that did, findings often showed that the associations between acknowledgment and mental health outcomes diminished or disappeared once assault characteristics were included (Bhuptani & Messman, 2021; Boyle & Clay-Warner, 2018; H. Littleton & Henderson, 2009; Harned, 2004). This suggests that, it may not be acknowledgment per se that predicts psychological distress and PTSD symptoms, but rather the characteristics of the assault itself.
Research investigating the meaning behind the label of rape remains limited. However, internalized stigma (self-blame and shame) and experienced stigma (negative social reactions upon disclosure) frequently emerge as key variables for understanding the associations between rape acknowledgment and mental health outcomes. These findings suggest that acknowledgment may be indirectly associated with psychological distress and PTSD symptoms through the stigma that often comes with labeling an experience as rape. Although the evidence is limited, some studies reported that rape-related shame and self-blame were positively associated with both acknowledgment and mental health outcomes (e.g., Bhuptani & Messman, 2021; Boyle & Clay-Warner, 2018). From this perspective, rape acknowledgment may be linked to heightened psychological distress and PTSD symptoms, not because labeling is intrinsically harmful, but because it exposes victims to stigmatizing beliefs and reactions. This interpretation has important clinical implications, as one cannot change what happened to them, but we can change both individually and collectively the stigma surrounding rape. Interventions that promote adaptive meaning-making and reduce rape stigma may, therefore, be key in supporting victims’ recovery, regardless of how they label their experience. Of note, stigma, particularly self-blame, may also act as a barrier to rape acknowledgment. A metasynthesis of qualitative studies (Rousseau et al., 2020) found that women who felt like the assault could have been prevented, or that they were partially responsible for it, were less likely to acknowledge their experience as rape.
To conclude, it is essential to contextualize these results within the scope of the reviewed studies. Most of the existing research has focused on predominantly White, heterosexual, college-age, cisgender women in the United States, which significantly limits the generalizability of our findings. In general, this demographic not only has greater access to sexual assault prevention programs and services but also forms the primary target audience for which these initiatives were initially developed (Harris & Linder, 2023). As a result, acknowledgment may carry different meanings and implications across diverse populations. Emerging evidence suggests that trans and gender-expansive individuals may be more likely than women to label a nonconsensual experience as rape, whereas men may be less likely to do so (Anderson et al., 2021; Pugh et al., 2024; Reed et al., 2020). Likewise, bisexual women appear more likely to acknowledge a nonconsensual experience as rape than lesbian women (Blayney et al., 2018). These differences could reflect variations in the acceptance of rape myths, which tend to be more strongly endorsed by men and less so by queer, trans, and gender-expansive people (Anderson et al., 2021; Pugh et al., 2024; Reed et al., 2020). More broadly, there appears to be a general trend in which greater vulnerability to sexual violence is associated with a higher likelihood of acknowledgment (Blayney et al., 2018). Still, most studies with underrepresented groups remain primarily descriptive, underscoring the need for further research to explore the role of rape acknowledgment on the mental health of men, marginalized groups, and individuals from different sociodemographic backgrounds.
Limitations of the Current Review
The findings of this systematic review should be interpreted in light of several limitations. To begin, we only considered peer-reviewed studies for inclusion, which may have introduced publication bias, as studies with significant results are more likely to get published. In addition, we focused exclusively on psychological distress (including anxiety and depression) and PTSD symptoms, thereby overlooking other potential detrimental outcomes that may be associated with rape acknowledgment (e.g., substance use, sexual revictimization, and somatic symptoms). Finally, due to substantial methodological differences across the included studies, we decided not to conduct a meta-analysis. Instead, we focused on documenting how differences in design, sampling, and measurement may have influenced the results. Although this decision limits our ability to calculate overall effect sizes, we think it allows for a more nuanced understanding of the current scientific literature.
Implications for Practice, Policy, and Future Research
Multiple recommendations for practitioners, policymakers, and researchers can be derived from this systematic review (see Table 3 for a summary).
Implications of the Review for Practice, Policy, and Research.
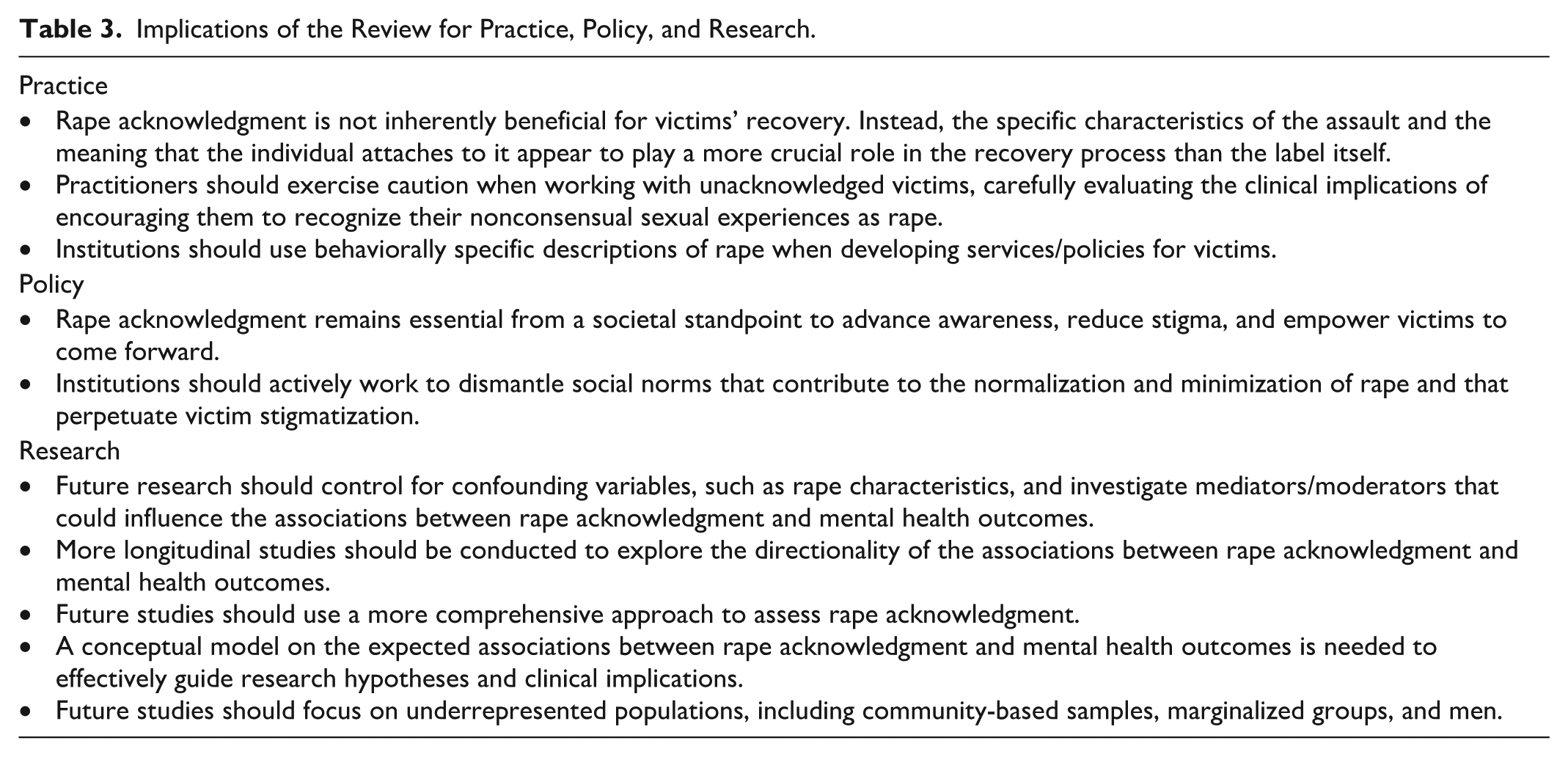
Practice
This review suggests that rape acknowledgment is not necessarily linked to better mental health outcomes. Practitioners should, therefore, carefully reconsider the prevailing notion that unacknowledged victims benefit from being encouraged to label their nonconsensual sexual experiences as rape. Although labeling may help some individuals feel less guilty, make sense of their experience, and feel entitled to support and treatment, for others, it may make them feel vulnerable, frightened, and out of control (Peterson & Muehlenhard, 2011). Even if well-intentioned, encouraging an individual to adopt a specific label may inadvertently undermine their sense of agency and replicate the power dynamics of the original assault, potentially leading to retraumatization. Practitioners working with individuals who experienced rape should instead recognize the inherent tensions involved in rape acknowledgment by respecting their preferred label and allowing space for them to explore any conflicting responses at their own pace. These considerations are equally important for those who would choose not to label their experience at all.
The findings from this review also suggest that the characteristics of the assault itself and the meaning attributed to it may play a significant role in explaining the associations between rape acknowledgment and mental health outcomes. Given that there is still a stigma attached to rape in our society, which often manifests itself as shame and self-blame among victims (Kennedy & Prock, 2018), interventions aimed at resolving the identity disruption caused by labeling an experience as rape could be particularly relevant to address the psychological distress and PTSD symptoms associated with rape acknowledgment. This could be achieved by either making the assault less central or salient to the individual’s identity or by reframing the harmful emotional and cognitive content attached to it (Quinn & Earnshaw, 2013). To this end, institutions dedicated to supporting victims should use behaviorally specific descriptions of rape when developing services instead of stigmatized labels like “rape,” as many victims may not readily identify their experience as rape but could still benefit from these services.
Policy
Although the individual-level clinical implications of rape acknowledgment remain somewhat ambiguous, its societal relevance is clear. Research has shown that acknowledged victims are more inclined to disclose their assault, seek medical or psychosocial services, and pursue legal action against their perpetrator compared to unacknowledged victims (e.g., Botta & Pingree, 1997; Cleere & Lynn, 2013; H. L. Littleton et al., 2006). Thus, when victims acknowledge rape, it often results in greater disclosure, which is beneficial for advancing societal awareness, reducing stigma, and empowering other victims to come forward. Importantly, rape acknowledgment does not occur in a vacuum; if society and communities fail to recognize sexual violence as a systemic issue, individuals may, in turn, struggle to label their nonconsensual sexual experience as rape. Indeed, most barriers, risks, and adverse outcomes related to rape acknowledgment seem to be tied, in one way or an other, to a broader societal context that stigmatizes victims. Institutions should, therefore, actively work to dismantle social norms that contribute to the normalization and minimization of rape and that perpetuate victim stigmatization (Kennedy & Prock, 2018).
Finally, the high levels of psychological distress among both acknowledged and unacknowledged victims emphasize that attention to recovery after assault always needs to be coupled with a conversation about doing more to prevent sexual violence. More than four decades into the widespread public recognition of sexual violence as a social problem on college campuses in the United States, prevention efforts have yet to meaningfully reduce victimization rates (Koss et al., 2022), despite these being the settings that have received the most attention.
Future Research
This review highlights several research gaps that need to be tackled in future studies to better understand the associations between rape acknowledgment and mental health outcomes. To begin, many studies did not have clear hypotheses regarding the expected associations. To inform future empirical research, a theoretical framework is needed to clarify the circumstances under which acknowledging rape might either exacerbate or alleviate psychological distress and PTSD symptoms. Similarly, researchers should move beyond bivariate analyses and instead adopt multivariate approaches that consider contextual and individual factors likely to influence these associations, such as gender and sexual identity, rape characteristics, relationship to the assailant, and location of the assault. For instance, even within campus settings, levels of institutional commitment and cultural support for people who have experienced sexual violence can vary substantially, underscoring the importance of examining environmental factors across diverse educational contexts.
Moreover, most studies that examined the associations between rape acknowledgment and mental health outcomes have been cross-sectional. Although these studies offer valuable insights, they may not fully capture the evolving nature of rape acknowledgment and its associations with mental health. Healing from sexual violence has been described as a dialectical process marked by conflicting responses during which individuals may feel compelled to acknowledge the assault by confronting its impact on their self-perception, while simultaneously striving to preserve their identity by minimizing its significance and rejecting the labels of “victim” or “survivor” (Draucker et al., 2009). This internal tension may contribute to fluctuations in both rape acknowledgment and mental health symptoms over time. For instance, individuals who acknowledge their assault as rape may initially experience an exacerbation of psychological distress and PTSD symptoms as they work through restoring a sense of self. However, these reactions may evolve as they engage in more meaning-making, potentially leading to long-term improvements in mental health. Although rape acknowledgment is often treated as a predictor of mental health, it is also plausible that individuals experiencing higher symptom levels may be more likely to label their experience as rape. Indeed, qualitative research suggests that some women may come to label their nonconsensual experience as rape as a result of the negative consequences it had on them (Rousseau et al., 2020). Individuals who experience more negative outcomes may also be more likely to seek social or professional support, which could, in turn, lead them to redefine their nonconsensual sexual experiences as rape as a result of being exposed to educational information and others’ perspectives. Thus, more longitudinal research is needed to clarify the directionality of these associations.
Additionally, much of the quantitative research conducted to date has categorized individuals based on whether they acknowledge their nonconsensual experience as rape or not. However, findings from many studies suggest that these simplistic categories do not adequately reflect victims’ experiences. Indeed, some women report a shift in the way they label their nonconsensual sexual experience over time (Peterson & Muehlenhard, 2011), whereas others express ambivalence regarding how to label their experience (Johnstone, 2016). Researchers would thus benefit from using a more nuanced approach to assessing rape acknowledgment, such as offering multiple labeling options (including write-in responses or the option to refrain from labeling altogether) and using continuous rating scales to capture ambivalence.
Finally, the findings from this systematic review remain circumscribed to a predominantly White, cisgender undergraduate women population, which significantly limits the external validity of the conclusions. There is a pressing need to examine how rape acknowledgment relates to the mental health of men, sexual and gender-expansive individuals, and other marginalized groups who are disproportionately targeted by perpetrators (e.g., sex workers, immigrants, and people with disabilities). Nearly two decades ago, H. L. Littleton et al. (2007) cautioned that we would not be able to fully understand the consequences of unacknowledged rape until it was studied in more diverse populations. Unfortunately, limited progress has been made in this direction. Although studies involving underrepresented groups are beginning to emerge, they remain few and largely descriptive. Future research must move beyond descriptive approaches to explore the unique meanings and implications of acknowledgment within these groups.
Conclusion
Previous studies have found conflicting results regarding the role of rape acknowledgment in victims’ recovery. This systematic review aimed to clarify these discrepancies by critically examining the existing literature on the associations between rape acknowledgment and mental health outcomes. The findings indicated that unacknowledged rape was generally associated with either lower or comparable levels of psychological distress and lower PTSD symptoms than acknowledged rape. However, these findings should not be interpreted as meaning that acknowledgment is harmful or inconsequential, as some studies suggest that rape characteristics and meaning attribution may play an important role in shaping these associations. Taken together, this systematic review challenges the idea that acknowledging a nonconsensual sexual experience as rape inherently benefits recovery and emphasizes the need for a robust conceptual framework to gain a better understanding of the circumstances under which acknowledgment may mitigate or exacerbate psychological distress and PTSD symptoms.
Footnotes
Appendix
Quality Assessment Criteria.
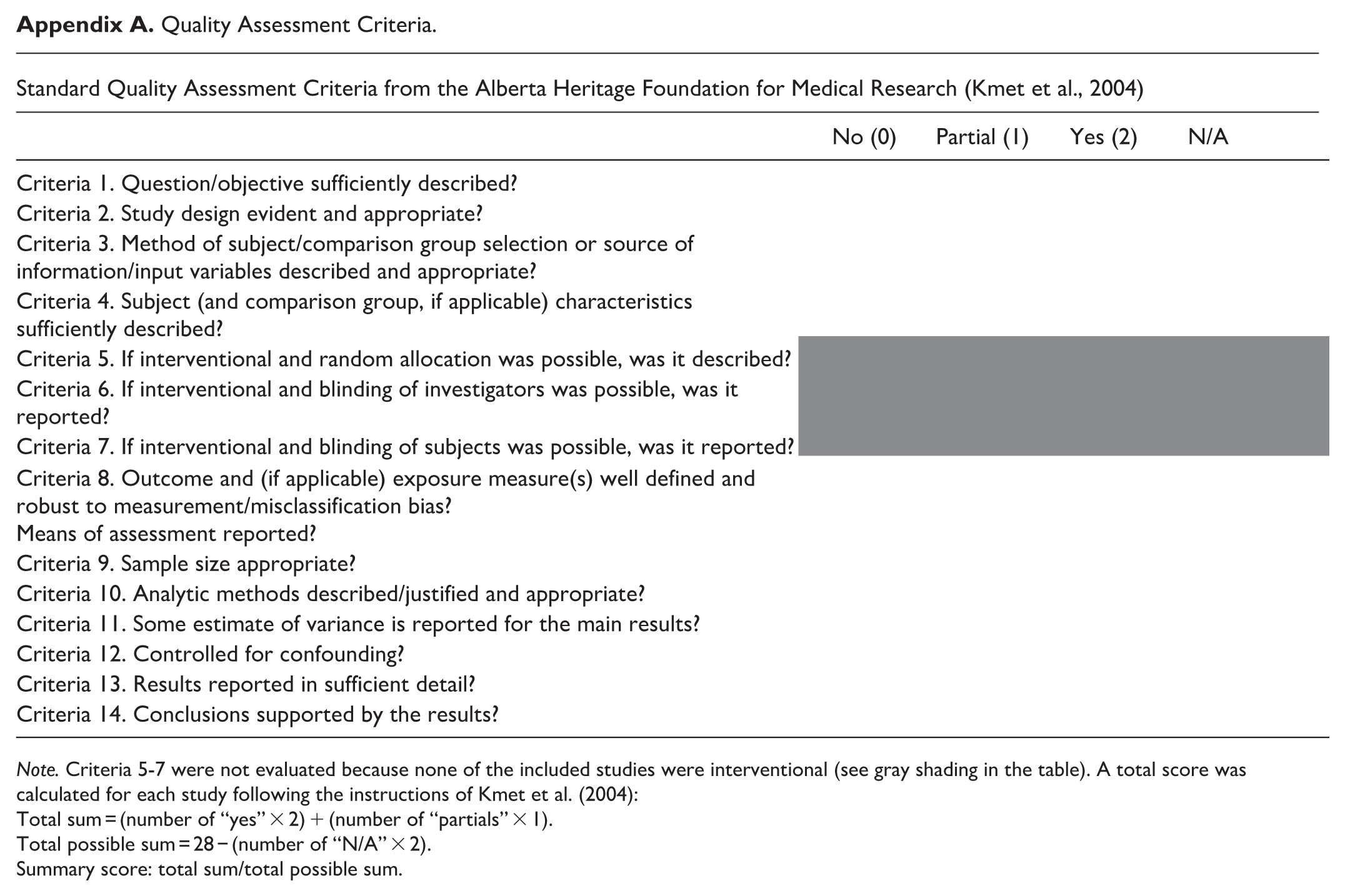
| Standard Quality Assessment Criteria from the Alberta Heritage Foundation for Medical Research (Kmet et al., 2004) | ||||
|---|---|---|---|---|
| No (0) | Partial (1) | Yes (2) | N/A | |
| Criteria 1. Question/objective sufficiently described? | ||||
| Criteria 2. Study design evident and appropriate? | ||||
| Criteria 3. Method of subject/comparison group selection or source of information/input variables described and appropriate? | ||||
| Criteria 4. Subject (and comparison group, if applicable) characteristics sufficiently described? | ||||
| Criteria 5. If interventional and random allocation was possible, was it described? | ||||
| Criteria 6. If interventional and blinding of investigators was possible, was it reported? | ||||
| Criteria 7. If interventional and blinding of subjects was possible, was it reported? | ||||
| Criteria 8. Outcome and (if applicable) exposure measure(s) well defined and robust to measurement/misclassification bias? |
||||
| Criteria 9. Sample size appropriate? | ||||
| Criteria 10. Analytic methods described/justified and appropriate? | ||||
| Criteria 11. Some estimate of variance is reported for the main results? | ||||
| Criteria 12. Controlled for confounding? | ||||
| Criteria 13. Results reported in sufficient detail? | ||||
| Criteria 14. Conclusions supported by the results? | ||||
Note. Criteria 5-7 were not evaluated because none of the included studies were interventional (see gray shading in the table). A total score was calculated for each study following the instructions of Kmet et al. (2004):
Total sum = (number of “yes” × 2) + (number of “partials” × 1).
Total possible sum = 28 − (number of “N/A” × 2).
Summary score: total sum/total possible sum.
Funding
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.