
Abstract
A meta-analysis published in 2015 demonstrated a significant association between bullying victimization (BV) in school and workplace settings and the onset of post-traumatic stress disorder (PTSD) symptoms. However, a recent theoretical review showed that the consequences of BV are much more complex than the traditional PTSD criteria. The authors argue that two potential diagnoses ought to be considered in the context of BV: developmental trauma disorder (DTD) and complex post-traumatic stress disorder (CPTSD). This systematic review aims to synthesize the results regarding the relationship between BV and these two complex trauma symptoms. Following PRISMA guidelines, systematic searches were conducted in seven electronic databases in March 2024. We searched for Portuguese or English quantitative published studies, or unpublished quantitative master’s or doctoral theses. In total, 1056 studies were identified, and 12 were considered eligible. Ten were cross-sectional, and two were longitudinal. Five had youth samples, whereas seven had adult samples. Most studies presented a low risk of bias. No studies were found that aimed to assess the relationship between BV and DTD symptoms. In contrast, a significant positive relationship between BV and CPTSD symptoms in youth and adult populations was found. BV was particularly associated with CPTSD, but not with PTSD in both populations. Only one study found that BV was not a predictor of CPTSD status in a Danish adult population. The results reveal that BV might be associated with a more complex symptomatology. However, it is still not possible to assert the causal link between BV and DTD/CPTSD.
Keywords
Introduction
Bullying victimization (BV), defined by its intentionality, repetition, and the perceived power imbalance between aggressor and victim (Olweus, 1995), can occur through physical, verbal, relational, or cyber victimization (Juvonen & Graham, 2014; Olweus, 2012). It is associated with various physical and mental health issues, including depression, anxiety, irritability, fatigue, sleep problems, and difficulties with concentration (Guo et al., 2022; Halliday et al., 2021; Yang et al., 2024). Some authors emphasize that these problems, when combined, resemble the symptoms of post-traumatic stress disorder (PTSD), proposing a causal relationship between BV and PTSD (Kreiner et al., 2008; Tehrani, 2004). The only meta-analysis exploring this phenomenon in children and adults found a relationship between BV and PTSD, indicating that, on average, 57% of victims reported PTSD symptoms (Nielsen et al., 2015). Recent studies continue to demonstrate a significant relationship between BV and PTSD among young people (Chen & Elklit, 2018; Fernández-Aldana et al., 2024; Li et al., 2023) and adults (Andreou et al., 2021; Hyland et al., 2021).
As interpersonal violence, BV can be considered a potentially repeated traumatic event. However, according to the DSM-5, PTSD can only be diagnosed when symptoms are temporally and contextually linked to a traumatic event involving death, the threat of death, serious injury, or sexual violence (American Psychiatric Association, 2013). BV partly fulfills these criteria. In one hand, victims of bullying may evoke fear of dying depending on the circumstances and types of aggression used (Idsoe et al., 2021). However, BV constitutes systematic and prolonged exposure to interpersonal violence. Consequently, some authors conceptualize BV not as a type I trauma – the result of a single traumatic event (e.g., earthquake, car accident, attack by a violent dog), which is more closely linked to PTSD symptoms – but rather as a type II trauma – the result of repeated exposure to traumatic events (e.g., domestic violence), which are more commonly associated with complex symptomatology (Terr, 1991; Idsoe et al., 2021). This is consistent with the literature, given the relationship between BV and multiple mental health issues (Guo et al., 2022; Halliday et al., 2021; Iyer-Eimerbrink & Jensen-Campbell, 2019; Rasalingam et al., 2017; Tu et al., 2019; Sumter & Baumgartner, 2017; Yang et al., 2024).
A recent theoretical and conceptual review suggests that BV should be framed from a developmental perspective, with developmental trauma disorder (DTD) and complex post-traumatic stress disorder (CPTSD) better capturing the complexity of BV symptoms than traditional PTSD criteria (Idsoe et al., 2021). Regarding DTD, Herman (1992) originally proposed it as a diagnosis to capture the complex sequelae of chronic interpersonal trauma in children, particularly biopsychosocial dysregulation that can emerge after repeated and combined exposure to (a) interpersonal violence and (b) disruptions in attachment with a primary caregiver. However, DTD has not been formally recognized in either the DSM-5 or ICD-11; rather, it remains a proposed construct that has been used conceptually in trauma research and clinical discussions, with ongoing debate about its distinctiveness and diagnostic utility. Empirical studies have demonstrated that BV is related to each criterion of DTD (affective and physiological dysregulation, attentional and behavioral dysregulation, and self and relational dysregulation), indicating the potential complexity of symptoms presented by BV victims (Idsoe et al., 2021).
In contrast, CPTSD is a disorder formally included in the ICD-11, encompassing both PTSD symptoms and disturbances in self-organization (DSO). CPTSD emerges after prolonged and repeated exposure to extremely threatening interpersonal events from which the individual has difficulty escaping (Maercker et al., 2013). Clinical reports suggest that BV victims may fear for their lives, making it a subjectively extremely threatening experience that should not be assessed solely through traditional PTSD criteria (Idsoe et al., 2021).
These potential complex consequences, if proven empirically, can guide and improve future clinical practice when addressing victims of BV, but also establish preventive and interventive policies in school settings and in the workplace. Thus, Idsoe et al. (2021), through their theoretical and conceptual review, emphasize the need and urgency for future studies to further investigate the consequences of bullying exposure within frameworks like DTD and CPTSD.
Research Gap and Rationale for the Present Review
Despite consistent evidence linking BV to PTSD (e.g., Nielsen et al., 2015), there is a notable gap regarding its relationship with symptoms of complex trauma, such as DTD and CPTSD. Idsoe et al. (2021), in a theoretical and conceptual review, argued that DTD and CPTSD may better capture the multifaceted consequences of BV than traditional PTSD criteria. However, their review did not systematically synthesize empirical studies, leaving unanswered the extent to which BV is associated with DTD and CPTSD symptoms across developmental stages.
Since 2021, several new empirical studies have investigated BV in relation to complex trauma symptoms, but their findings remain fragmented. To date, no systematic review has integrated this emerging body of evidence. This lack of synthesis hampers the ability to confirm theoretical claims, delineate developmental patterns, and inform clinical and policy interventions.
The present systematic review addresses this gap by systematically evaluating empirical research on the associations between BV and symptoms of DTD and CPTSD in children, adolescents, and adults. By consolidating this evidence, the review seeks to provide a stronger empirical foundation for clinical practice and policy regarding the assessment and treatment of bullying victims.
Our systematic review aims to (a) verify the relationship between BV and DTD symptoms and (b) verify the relationship between BV and CPTSD symptoms in children, adolescents, and adult samples.
The objectives of this systematic review were defined from the research questions:
a) “What is the relationship between BV and DTD symptoms in children (individuals under the age of 10 years; World Health Organization, 2024), adolescents (individuals aged 10–19 years; World Health Organization, 2024) and adult populations (individuals aged 18 or more; United Nations, 1989)?”
b) “What is the relationship between BV and CPTSD symptoms in children, adolescents, and adult populations?”
Methods
Eligibility Criteria
The inclusion criteria were: (a) quantitative studies published in peer-reviewed journals; (b) unpublished master’s or doctoral theses that presented a quantitative method; (c) studies that focused on BV and symptoms of complex trauma (i.e., DTD and/or CPTSD); (d) studies written in English or Portuguese. Minimum sample sizes, population type, study design, or publication year were not stipulated.
The exclusion criteria were: (a) published or unpublished systematic reviews, meta-analysis, qualitative and mixed-method studies; (b) research reports, conference articles, opinion articles, posters, and chapters of books; (c) published quantitative studies that not assess BV or one of the symptoms of complex trauma (i.e., DTD, CPTSD); (d) studies with insufficient or unclear methodological or results reporting (e.g., absence of specification of variables measured, missing information about sample characteristics, or incomplete reporting of measures related to BV or complex trauma symptoms), which precluded assessment of eligibility or data extraction; and (e) articles not written in English or Portuguese.
Information Sources and Search Strategy
In March of 2024, relevant studies were identified by two reviewers (DM and PCS) through seven electronic databases: Web of Science/Medline, PubMed, Scopus, ERIC, PsycInfo, PsycARTICLES, and ScieLO. The search terms were equal in all databases. The search equation used was: (“Peer victim*” OR “Bully*” OR “Bullied” OR “Bullying Victimization” OR “Traditional Bullying” OR “School bullying” OR “School violence” OR “Peer Victimization” OR “Cyberbullying” OR “Cybervictim*” OR “Workplace Bullying” OR “Bullying at work” OR “Harass*” OR “Intimidation” OR “Mobbing”) AND (“Developmental Trauma Disorder” OR “DTD” OR “Developmental psychopathology” OR “Developmental Trauma” OR “Complex Trauma” OR “Interpersonal Trauma” OR “Complex Posttraumatic Stress Disorder” OR “Complex post-traumatic stress disorder” OR “Complex PTSD” OR “CPTSD” OR “C-PTSD” OR “Disorder of Extreme Stress Not Otherwise Specified” OR “DESNOS”) AND (“Child*” OR “Adolescen*” OR “Teen*” OR “Youth*” OR “Young people” OR “Young person*” OR “School student*” OR “Adult*”). Searches were also conducted on ProQuest Dissertations & Theses Global for the Inclusion of gray literature (i.e., master dissertations and doctoral theses). Database searches were supplemented by a bibliographic review of identified articles, as well as consultation with experts. There was no time interval restriction during the search strategy. However, we restricted the search strategy to English and Portuguese language.
After the first peer review, searches were reconducted in July 2025 and September 2025. New publications were not found.
Selection Process
Identified studies were imported into the Rayyan program, and the duplicates were removed. The titles and abstracts were independently screened by two reviewers (DM and PCS), who proceeded to include only potentially relevant studies. Full-text articles were then analyzed by these two reviewers to ensure that the inclusion criteria were fulfilled. All doubts were discussed between the two reviewers until a consensus was reached.
Data Collection Process
Data from the included studies were independently extracted by two reviewers (DM and PCS). For each study, we first identified the author(s) name(s), year of publication, and study design. Details about the sample size (N), country, and the main socio-demographic characteristics of the study samples were then collected (e.g., mean age). Subsequently, we identified the key dimensions (i.e., bullying victimization, DTD or CPTSD symptoms) and extracted how they were measured within each included study (e.g., self-report measures). Finally, we extracted the main results. Specifically, we extracted the correlations among the key measures. The results that showed statistical significance or null findings were extracted by the two reviewers. All disagreements between reviewers were solved after discussion and consensus. Description of main sample features, study design, and key results of the eligible studies are presented in Table 1.
Overview of Studies Included in the Systematic Review.
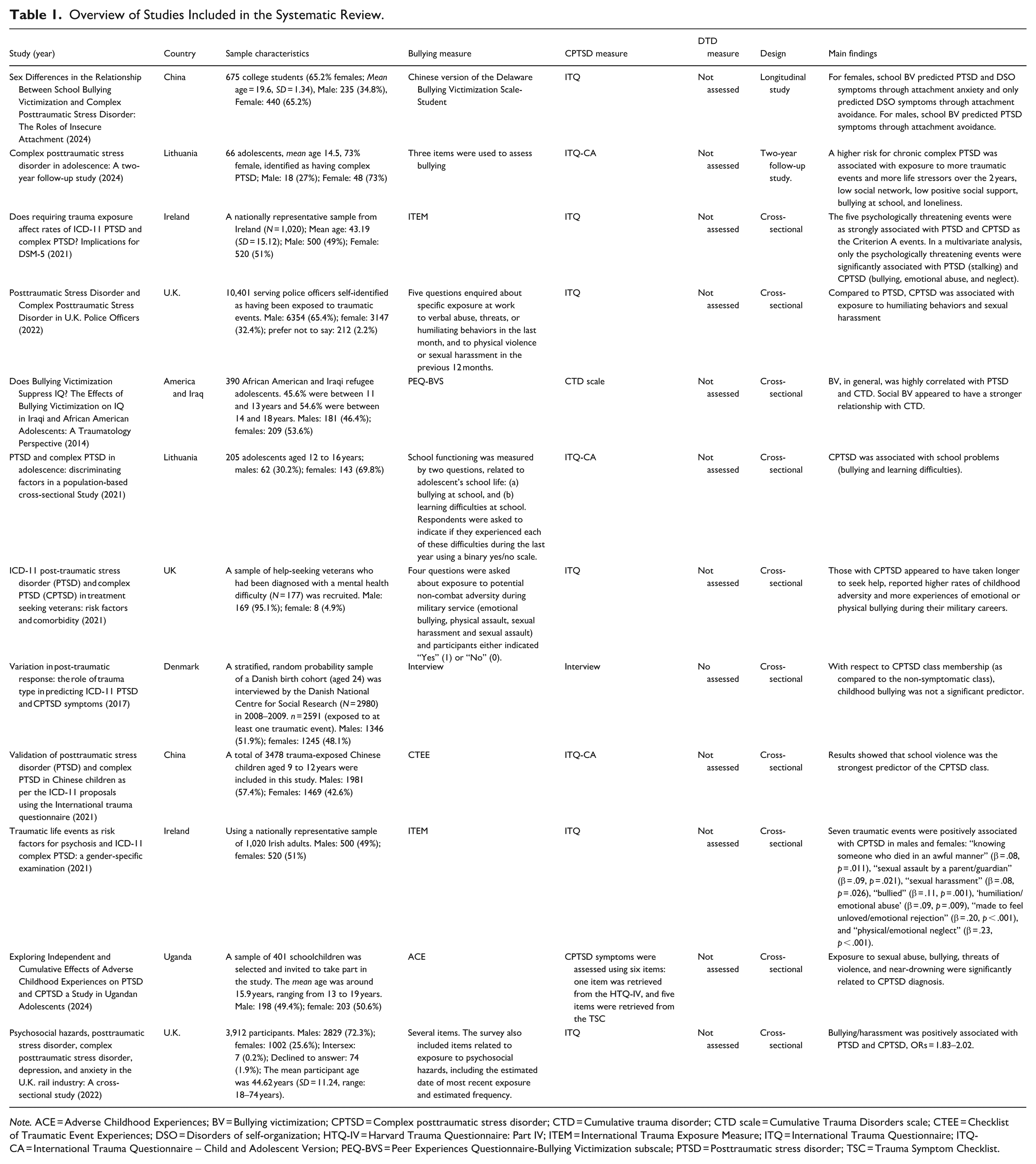
Note. ACE = Adverse Childhood Experiences; BV = Bullying victimization; CPTSD = Complex posttraumatic stress disorder; CTD = Cumulative trauma disorder; CTD scale = Cumulative Trauma Disorders scale; CTEE = Checklist of Traumatic Event Experiences; DSO = Disorders of self-organization; HTQ-IV = Harvard Trauma Questionnaire: Part IV; ITEM = International Trauma Exposure Measure; ITQ = International Trauma Questionnaire; ITQ-CA = International Trauma Questionnaire – Child and Adolescent Version; PEQ-BVS = Peer Experiences Questionnaire-Bullying Victimization subscale; PTSD = Posttraumatic stress disorder; TSC = Trauma Symptom Checklist.
Study Risk of Bias Assessment
The risk of bias in individual studies was independently conducted by two reviewers (AM and DM). We used the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies Checklist of 14 items (National Heart, Lung, and Blood Institute, 2016) for the assessment of cross-sectional and longitudinal quantitative studies. All items from the two checklists were utilized, and each study was independently assigned an overall quality rating (“Good,” “Fair,” or “Poor”) by the two reviewers (Tables 2 and 3). Studies rated as poor quality were considered to have a high risk of bias, whereas those rated as good quality were deemed to have a low risk of bias. Potential risk of bias may include selection bias, information bias, measurement bias, or confounding (National Heart, Lung, and Blood Institute, 2016). Quality ratings were not used to exclude studies but did serve to identify consistent weaknesses and risk of bias from eligible studies. Inter-rater agreement (or inter-rater reliability) was measured through Cohen’s Kappa coefficient (k), a robust statistic that measures the degree of agreement between two raters regarding the same qualitative (categorical) items, while considering chance agreement (McHugh, 2012). Cohen’s Kappa magnitude can range from −1 to +1, where ≤0 represents no agreement; 0.001 to 0.20 represents none to a slight agreement; 0.21 to 0.40 represents fair agreement; 0.41 to 0.60 represents moderate agreement; 0.61 to 0.80 represents substantial agreement; and 0.81 to 0.99 represents almost perfect agreement, and 1 represents perfect agreement (McHugh, 2012). Inter-rater agreement analysis was performed using the IBM SPSS, version 29 for Windows (United States, New York, IBM Corporation).
Risk of Bias Assessment of Included Cross-Sectional Studies.
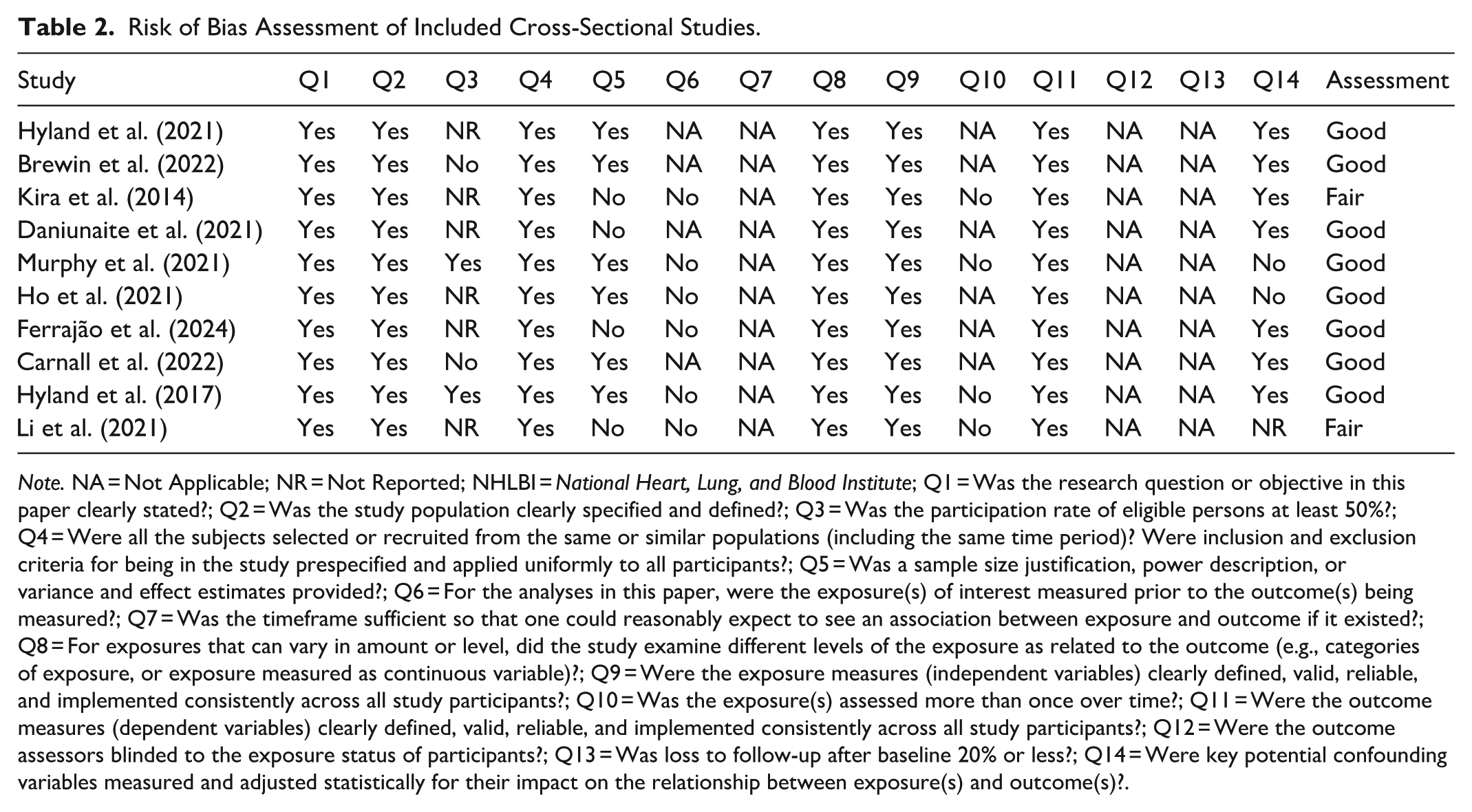
Note. NA = Not Applicable; NR = Not Reported; NHLBI = National Heart, Lung, and Blood Institute; Q1 = Was the research question or objective in this paper clearly stated?; Q2 = Was the study population clearly specified and defined?; Q3 = Was the participation rate of eligible persons at least 50%?; Q4 = Were all the subjects selected or recruited from the same or similar populations (including the same time period)? Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants?; Q5 = Was a sample size justification, power description, or variance and effect estimates provided?; Q6 = For the analyses in this paper, were the exposure(s) of interest measured prior to the outcome(s) being measured?; Q7 = Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed?; Q8 = For exposures that can vary in amount or level, did the study examine different levels of the exposure as related to the outcome (e.g., categories of exposure, or exposure measured as continuous variable)?; Q9 = Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants?; Q10 = Was the exposure(s) assessed more than once over time?; Q11 = Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants?; Q12 = Were the outcome assessors blinded to the exposure status of participants?; Q13 = Was loss to follow-up after baseline 20% or less?; Q14 = Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)?.
Risk of Bias Assessment of Included Longitudinal Studies.
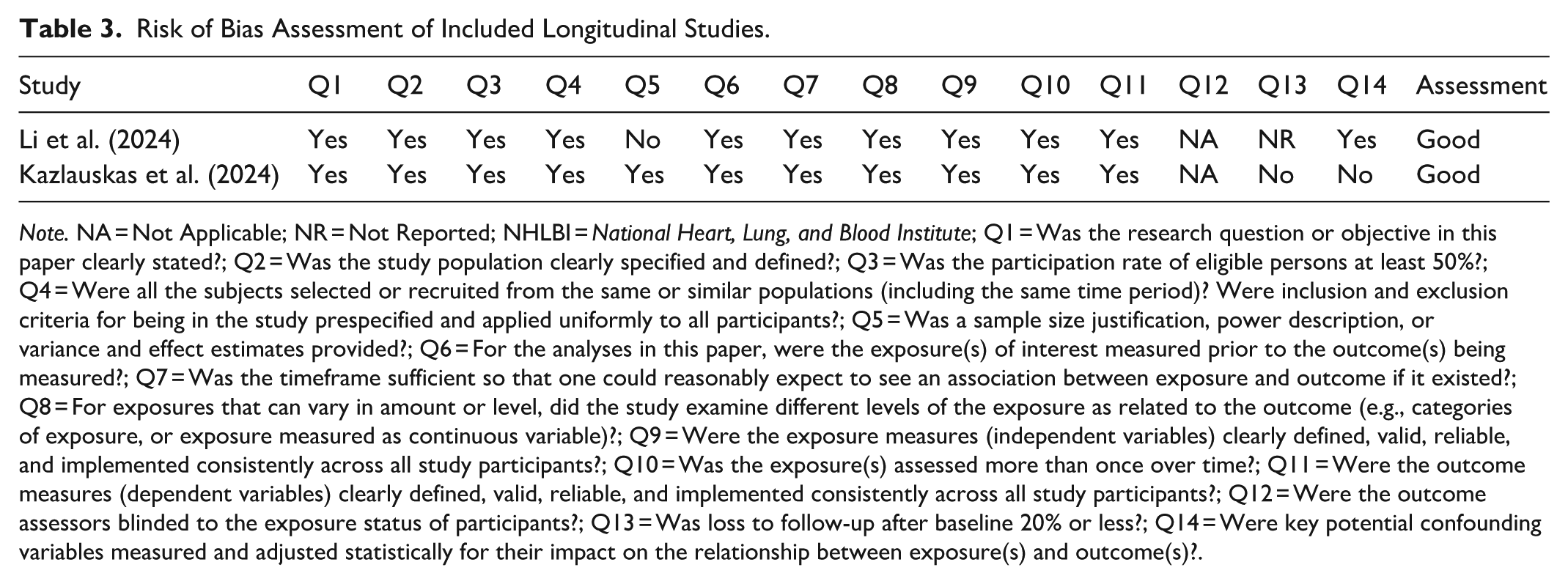
Note. NA = Not Applicable; NR = Not Reported; NHLBI = National Heart, Lung, and Blood Institute; Q1 = Was the research question or objective in this paper clearly stated?; Q2 = Was the study population clearly specified and defined?; Q3 = Was the participation rate of eligible persons at least 50%?; Q4 = Were all the subjects selected or recruited from the same or similar populations (including the same time period)? Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants?; Q5 = Was a sample size justification, power description, or variance and effect estimates provided?; Q6 = For the analyses in this paper, were the exposure(s) of interest measured prior to the outcome(s) being measured?; Q7 = Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed?; Q8 = For exposures that can vary in amount or level, did the study examine different levels of the exposure as related to the outcome (e.g., categories of exposure, or exposure measured as continuous variable)?; Q9 = Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants?; Q10 = Was the exposure(s) assessed more than once over time?; Q11 = Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants?; Q12 = Were the outcome assessors blinded to the exposure status of participants?; Q13 = Was loss to follow-up after baseline 20% or less?; Q14 = Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)?.
Effect Measures
Synthesis Methods
The included studies were reviewed using qualitative synthesis. Studies were categorized based on their primary focus and outcomes assessed: (a) BV only, (b) BV in relation to DTD symptoms, or (c) BV in relation to complex PTSD (CPTSD) symptoms. Within these categories, studies were further described according to sample characteristics, measures used, and study design. This structured categorization allowed for systematic comparison of key findings and ensured that categories were discrete and non-overlapping. Table 1 presents an overview of the extracted information for each included study, including country, sample characteristics, bullying and trauma measures, study design, and main findings.
A meta-analysis was not feasible due to substantial heterogeneity across studies. Specifically, the included studies varied in terms of bullying conceptualization (school, workplace, or lifetime), population characteristics (adolescents versus adults, community versus occupational samples), study design (cross-sectional versus longitudinal), and outcome measurement (e.g., ITQ, ITQ-CA, CTD scale, or non-standardized items). Furthermore, different self-report instruments were employed to assess BV, precluding the calculation of comparable effect sizes. Given these methodological discrepancies, a qualitative synthesis was judged to be the most appropriate approach.
Results
Study Selection
We initially identified 1051 studies through electronic database searching. After the duplicates were removed (n = 138), the titles and abstract were screened. After the Screening process, 860 studies were excluded. Of the fifty-three full-text articles assessed for eligibility, seven met the inclusion criteria. The main reasons for study exclusion were as follows: (a) did not assess BV (n = 3); (b) did not assess DTD or CPTSD (n = 38); presented a different study design (n = 3); or were not written in English or Portuguese (n = 2). References of the seven eligible studies were manually analyzed, resulting in two additional studies. Recent papers (that were not initially identified) that cited (seen in Google scholar) one or more of the nine included studies were also analyzed and resulted in three additional studies. References of these three studies were analyzed but did not result in additional studies. In total, 1056 studies were identified, of which 12 were considered eligible (Figure 1).
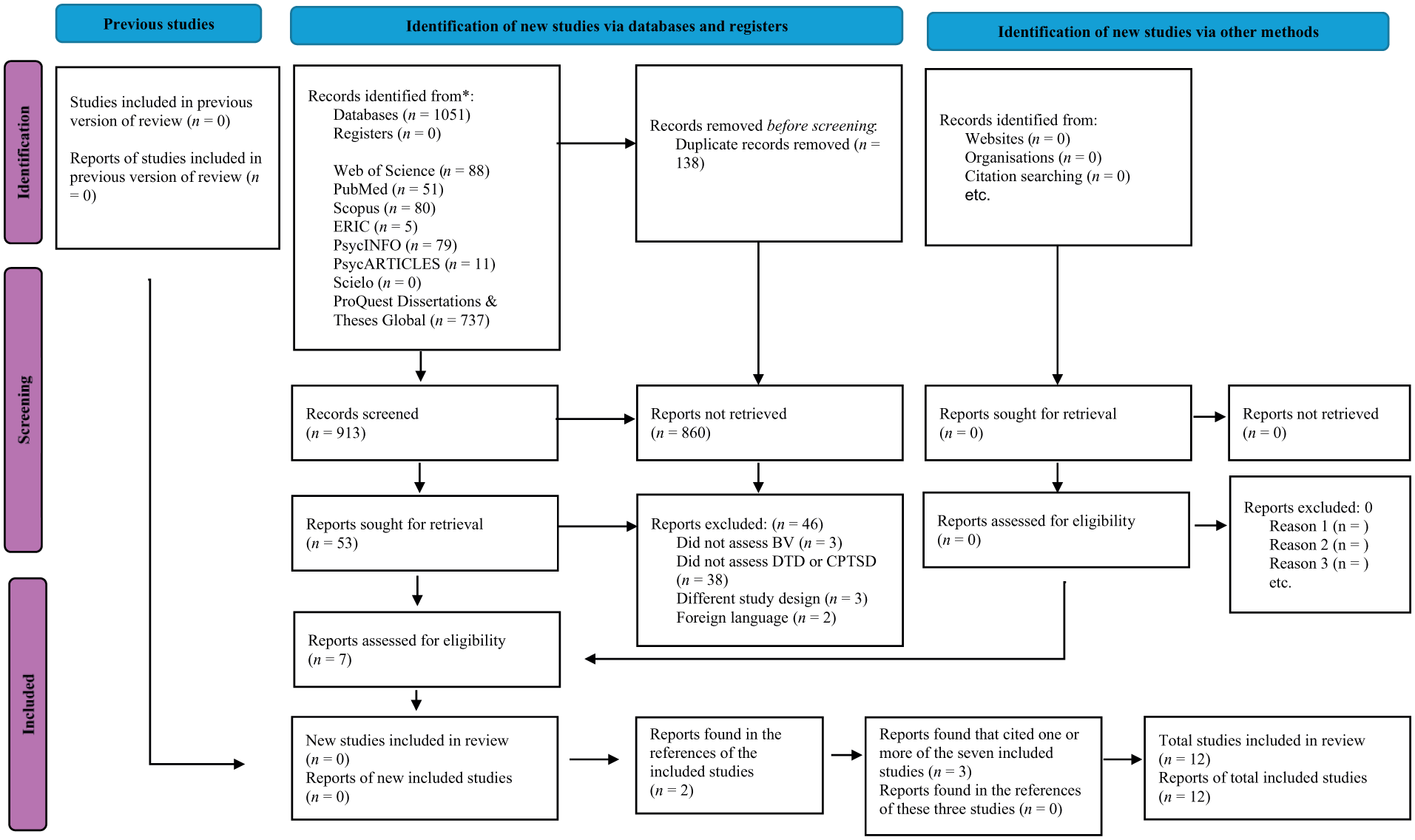
PRISMA 2020 flow diagram for updated systematic reviews, which included searches of databases, registers and other sources.
Study Characteristics
Year of publication: The included studies ranged between 2014 and 2024.
Country: The included studies include samples from China, Denmark, Iraq, Ireland, Lithuania, Uganda, UK, and USA.
Sample sizes and mean age: Regarding children and adolescents, the sample sizes varied between 66 (Kazlauskas et al., 2024) and 3478 (Li et al., 2021). The mean age was between 9 and 12 years old (Li et al., 2021) and 15.9 (Ferrajão et al., 2024). Regarding adults, the sample sizes varied between 177 (Murphy et al., 2021) and 10401 (Brewin et al., 2022). The mean age was between 19.6 (Li et al., 2024) and 44.62 (Carnall et al., 2022).
Design: All studies presented a cross-sectional design, except for two. Li et al. (2024) study presented a longitudinal design, and Kazlauskas et al. (2024) did a second wave of data collection.
Settings: All studies involving children and adolescents were conducted in educational settings (i.e., schools). Adult samples were recruited from various settings, including colleges (Li et al., 2024), Veterans’ associations (Murphy et al., 2021), police departments (Brewin et al., 2022), the National Centre for Social Research (Hyland et al., 2017), and the rail workforce (Carnall et al., 2022). Additionally, two studies had representative samples from a country – Ireland (Ho et al., 2021; Hyland et al., 2021).
Measures: Most studies used self-report measures to assess the key variables. However, one study employed an interview method to assess the participants (Hyland et al., 2017).
Bullying was assessed by different self-report measures, namely, the Chinese version of the Delaware Bullying Victimization Scale-Student (Li et al., 2024), the International Trauma Exposure Measure (Ho et al., 2021; Hyland et al., 2021), Peer Experiences Questionnaire-Bullying Victimization subscale (Kira et al., 2014), the Checklist of Traumatic Event Experiences (Li et al., 2021), and the Adverse Childhood Experiences (Ferrajão et al., 2024). This construct was also assessed by two (Daniunaite et al., 2021) or more questions (e.g., Brewin et al., 2022; Carnall et al., 2022; Kazlauskas et al., 2024; Murphy et al., 2021) created by authors.
CPTSD was mostly assessed by the International Trauma Questionnaire (ITQ; for adult samples), or the International Trauma Questionnaire – Child and Adolescent version (ITQ-CA). CPTSD was also evaluated by the Cumulative Trauma Disorders scale (CTD scale; Kira et al., 2014). Ferrajão et al. (2024) opted to use one item from the Harvard Trauma Questionnaire – IV (HTQ–IV) and five items from the Trauma Symptom Checklist to assess this construct.
Contrary to these authors, Hyland et al. (2017) did not use a specific measure. Instead, an algorithm-driven classification of ICD-11 PTSD was assigned if a participant endorsed all three symptoms, and two questions from the interview were used to assess the DSO symptom clusters.
No study assessed DTD symptoms.
Characteristics and main results are summarized in Table 1.
Risk of Bias of Included Studies
Quality appraisal of each criterion of the included studies is presented in detail in Tables 2 and 3. The main sources of bias were: (a) most studies presented a cross-sectional design thus preventing the determination of causality between variables; (b) few studies reported the participation rate (Hyland et al., 2017: Kazlauskas et al., 2024; Li et al., 2024; Murphy et al., 2021). This increases the risk of bias because if fewer than 50% of eligible subjects participated in the studies, then there is concern that the studies population may not adequately represent the target population; (c) five studies did not present any justification of sample size or statistical power, nor did they report effect size estimates (e.g., odds ratios, regression coefficients, mean differences, or confidence intervals) or measures of variance and precision (e.g., standard deviations, standard errors, or confidence intervals; Daniunaite et al., 2021; Ferrajão et al., 2024; Kira et al., 2014; Li et al., 2021, 2024). This increases the risk of bias because it is not clear whether the studies had enough participants to detect an association if one truly existed; (d) lack of representativeness in all studies due to convenience sampling, except the studies with Irish samples (Ho et al., 2021; Hyland et al., 2021); e) most studies relied only on self-report measures, and one study relied on an interview (Hyland et al., 2017), thus including possible reporting bias. There was great inter-rater agreement among the reviewers, κ = .82 (95% CI [0.75, 0.90]), p = .001, and doubts were discussed until a consensus was reached. A final overall quality rating for each study is presented in Tables 2 and 3.
Results of Individual Studies
Relationship Between BV and DTD Symptoms
We did not find any study that assessed the relationship between BV and DTD symptoms in children, adolescents, or adult samples.
Relationship Between BV and CPTSD Symptoms
Synthesis of Results
Children and Adolescents
Regarding the child and adolescent population, the five empirical studies indicated a significant positive relationship between BV and CPTSD symptoms. Specifically, this relationship was observed in four cross-sectional studies: one with a sample of African American and Iraqi refugee adolescents (Kira et al., 2014), another with a sample of Lithuanian adolescents (Daniunaite et al., 2021), a third with a sample of Ugandan adolescents (Ferrajão et al., 2024), and a final study with a sample of Chinese children (Li et al., 2021). Similarly, a longitudinal study with a sample of 66 adolescents indicated that negative life experiences (e.g., BV) were associated with a higher risk of presenting chronic CPTSD symptoms (Kazlauskas et al., 2024).
Adults
Regarding the adult population, overall, a significant positive relationship between BV (BV) and CPTSD symptoms was observed in five cross-sectional studies. Specifically, we found a significant positive relationship between lifetime exposure to bullying and CPTSD in two studies with representative samples of Irish adults (Ho et al., 2021; Hyland et al., 2021), as well as a positive relationship between workplace bullying and CPTSD in a sample of English police officers, a sample of English railway workers, and a sample of English veterans (Brewin et al., 2022; Carnall et al., 2022; Murphy et al., 2021).
The only longitudinal study identified with an adult sample also reported a similar finding. With a sample of 675 university students, Li et al. (2024) found that BV (i.e., school BV from primary school to college) was a significant predictor of the two CPTSD criteria (i.e., PTSD as defined by the ICD-11 and DSO) in female participants. However, BV was only a predictor of PTSD symptoms in male participants.
Contrary to the aforementioned studies, one cross-sectional study presented a different finding. In an adult Danish sample, Hyland et al. (2017) found no significant association between childhood bullying and CPTSD symptoms.
Discussion
The findings of this systematic review provide valuable insights into the relationship between BV and CPTSD symptoms across different age groups. Overall, the studies reviewed found a significant association between BV and CPTSD symptoms. Specifically, school-based bullying was positively and significantly related to CPTSD symptoms in children (Li et al., 2021), adolescents (Daniunaite et al., 2021; Ferrajão et al., 2024; Kira et al., 2014), and college students (Li et al., 2024). This finding was further supported by a 2-year follow-up study (Kazlauskas et al., 2024) reinforcing the stability of this relationship over time.
BV in the workplace was also related to CPTSD symptoms in adult samples, including police officers (Brewin et al., 2022), rail industry workers (Carnall et al., 2022), and veterans (Murphy et al., 2021). Moreover, BV was significantly associated with CPTSD symptoms in nationally representative samples of Irish adults (Ho et al., 2021; Hyland et al., 2021).
However, only one study showed that childhood bullying was not a significant predictor of CPTSD class membership in a stratified random probability sample of an adult Danish birth cohort (Hyland et al., 2017). Despite this contradictory result, the studies overall showed that BV was associated with CPTSD symptoms, regardless of the population being assessed.
PTSD symptoms or diagnosis were also related to BV (e.g., Hyland et al., 2021), as anticipated and previously demonstrated (see Nielsen et al., 2015). However, the studies reviewed in this systematic review revealed that BV was particularly associated with CPTSD compared to PTSD symptoms. For example, Daniunaite et al. (2021) underlined that BV at school was “particularly associated with CPTSD as opposed to PTSD status among traumatized adolescents” (p. 6). Similarly, BV was significantly associated with CPTSD diagnosis, but not with PTSD diagnosis in a sample of Ugandan adolescents (Ferrajão et al., 2024).
Among adult samples, Hyland et al. (2021) found that BV was associated with both PTSD and CPTSD in a bivariate association analysis. However, in a multivariate association analysis, BV was associated only with CPTSD in a nationally representative sample of Irish adults (Hyland et al., 2021). Similarly, among a sample of treatment-seeking veterans, Murphy et al. (2021) indicated that the participants who met the criteria for probable CPTSD were more likely to have experienced emotional bullying and physical assault in the military, compared to the veterans with probable PTSD or no PTSD.
These results are in accordance with the conclusion presented by Idsoe et al. (2021) that the symptoms associated with BV are more complex than those presented by PTSD. However, some caution is still needed regarding this topic. In their theoretical and conceptual review, Idsoe et al. (2021) argued that two potential diagnoses ought to be considered in the context of BV. One of these is CPTSD, which, as noted earlier, is consistently associated with BV, regardless of the population assessed. However, the other diagnosis that should be evaluated is DTD. To the best of our knowledge, no empirical study assessed the association between BV (at school, at work) and DTD symptoms or diagnosis. One possible explanation is the lack of self-report measure(s) that evaluate this construct. Overall, CPTSD was evaluated through the ITQ (for adults) and ITQ-CA (for children and adolescents), the most frequently used self-report measures that assess CPTSD. This method, despite its methodological limitations, may be the easiest to implement in most empirical and quantitative studies. In the case of DTD, there is one study that tested the psychometrics of a DTD semi-structured interview (DTD-SI) and the validity and structure of the DTD construct (Ford et al., 2018). However, this empirical study did not evaluate the potential association between BV and DTD, nor, to our knowledge, other studies. Another explanation is that some authors argue against the inclusion of DTD in DSM-5 or ICD-11. For example, Schmid et al. (2013) pointed out several conceptual and diagnostic concerns. First, they argued that DTD substantially overlaps with existing disorders, which could undermine rather than strengthen current diagnostic systems. Second, the model assumes that symptoms are uniquely attributable to complex trauma, even though many of these symptoms may also occur in individuals without such exposure. Third, some of the proposed symptoms are considered risk factors for future revictimization, raising questions about the assumption that trauma is the primary and unidirectional cause. Fourth, although DTD emphasizes developmental processes, it does not clearly differentiate between symptom manifestations in children versus adolescents. Finally, Schmid et al. (2013) cautioned that adopting DTD might inadvertently direct clinical interventions too narrowly toward trauma-related explanations, even when these may not fully account for the symptom presentation. On the other hand, other authors argue that DTD should be included in DSM (e.g., Van der Kolk, 2005). However, the arguments presented have relied primarily on theory rather than empirical evaluations of DTD symptom criteria. A systematic review synthesized and evaluated the existing empirical evidence for DTD (Morelli & Villodas, 2022). The authors concluded that DTD may be valid and reliable; may be distinct from other existing diagnostic constructs, and may have clinical utility. However, they caution that their findings are preliminary, and future research is still needed.
In their conceptual review, Idsoe et al. (2021) highlighted that several studies show that BV is, overall, associated with each criterion of DTD (i.e., affective, physiological, attentional, behavioral dysregulation, self and relational dysregulation); except, in specific criteria (e.g., in criterion D of DTD: D.1. “Intense Preoccupation with Safety of the Caregiver or Other Loved Ones (Including Precocious Caregiving) or Difficulty Tolerating Reunion with Them After Separation” where the authors could not find any studies that assessed BV with this specific criterion). Despite this significant association with different forms of dysregulation, it is not possible to determine if BV is associated with the DTD construct because there is no empirical study that tested this association. Therefore, we encourage future studies to test DTD in conjunction with BV in both youth and adult populations.
It is also not possible to determine with certainty whether BV leads (or causes) CPTSD. Our reviewed studies show a particular association between these variables. However, most studies presented a cross-sectional design, thus it is not possible to determine a causal relationship between BV and CPTSD. Thus, future studies should test this association through a longitudinal method.
Strengths and Limitations
To our knowledge, this is the first review that aimed to synthesize the breadth of knowledge available regarding the association between BV and complex trauma symptoms (i.e., DTD and/or CPTSD symptoms). This is the major strength of the present review. The inclusion of English and Portuguese language peer-reviewed journals, and the search of unpublished gray literature, regardless of year of publication and study design, reveals to be another possible strength of the current review, since prevents potential publication bias and efforts were made to capture all relevant articles through contact with subject matter experts and consulting references from the eligible studies. However, it is possible that articles may have been overlooked. Finally, the reviewed studies, overall, presented a good methodological quality, thus revealing to have a low risk of bias. However, some limitations should be considered: (a) most studies presented a cross-sectional-design, thus preventing the establishment of a casual relationship between BV and complex trauma symptoms (DTD or CPTSD); (b) the key findings from the current review may not be representative of all populations (e.g., children, adolescents; college students, adults), given that most included studies presented convenience sampling methods; and (c) all studies focused more on traditional bullying (physical, emotional, and relational bullying), than in cyberbullying. Although this review primarily included studies focusing on traditional forms of bullying, it is important to acknowledge that cyberbullying represents a pervasive and increasingly relevant form of BV. Online victimization may intensify the psychological consequences of bullying by extending exposure beyond physical environments and eliminating safe spaces for recovery (Kowalski et al., 2014). The constant accessibility of digital communication platforms can lead to sustained threat perception, social humiliation, and identity-related distress - factors that may exacerbate DSO, a hallmark of CPTSD (Idsoe et al., 2021). Moreover, the anonymity and permanence of online aggression can heighten feelings of helplessness and loss of control, potentially mirroring the mechanisms implicated in developmental trauma responses (Ford et al., 2018; Kowalski et al., 2014). Therefore, future research should systematically explore whether cyberbullying contributes to the onset or maintenance of CPTSD or DTD symptomatology.
Another limitation of this review is the language restriction. Only articles written in English or Portuguese were included, which may have led to the exclusion of relevant studies published in other languages, such as Spanish. This restriction was necessary to ensure accurate screening and data extraction by the review team, but future systematic reviews could expand the linguistic scope to capture research conducted in other cultural contexts.
Conclusion
Overall, the studies included in this review found a significant positive association between BV and CPTSD symptoms. Moreover, CPTSD was particularly associated with this violent interpersonal exposure in both school and workplace settings, compared to PTSD clinical status, across both youth and adult samples. This result supports the theory proposed by Idsoe et al. (2021), which argues that BV “is associated with a more complex sequelae than what is captured in traditional PTSD criteria” (p. 10).
However, some caution is still needed. The authors aforementioned argue that both DTD and CPTSD better capture the complexity of the symptoms associated with BV than PTSD, and that these consequences should be framed within a developmental perspective. Our included studies show a clear association between BV and CPTSD symptoms or status. However, most presented a cross-sectional design, thus it is not possible to assert that BV causes CPTSD. Moreover, no empirical cross-sectional or longitudinal study tested the association between BV and DTD symptoms. Given the early stage of research on this topic, we cannot conclusively state that BV is associated with more complex symptoms.
Therefore, we encourage future studies to test the association between BV (traditional bullying and cyberbullying) and complex trauma symptoms (DTD and CPTSD) for both youth and adult populations. Additionally, we recommend investigating the potential causal relationship between these variables using longitudinal designs.
Implications for Research and Practice
As argued by Idsoe et al. (2021), the most crucial implication regarding BV is that BV must be stopped, both in the school environment and in the workplace setting. In terms of intervention, several meta-analyses have shown that many school-based anti-bullying programs are effective in reducing bullying perpetration (BP) and BV (Gaffney et al., 2019; Gaffney et al., 2021) in children and adolescents. In contrast, empirical evidence regarding anti-bullying interventions in the workplace remains limited. For example, Gillen et al. (2017) found, after reviewing five studies, that organizational and individual anti-bullying interventions might prevent workplace bullying. However, the evidence was of very low quality, underscoring the need for more rigorous studies to determine the actual impact of these interventions. Another systematic review (Escartín, 2016) highlighted the importance of implementing anti-bullying policies within organizations. However, the mere existence of these policies revealed to be insufficient; their effectiveness largely depended on proper implementation and enforcement. For instance, a study involving 36 Human Resources professionals found that only one had a comprehensive anti-bullying policy that explicitly addressed bullying behaviors. The others either had indirect policies or none at all, indicating a gap between policy creation and practical application (Cowan, 2011). Contrarily, psychosocial factors may present positive results in reducing BV. For example, a positive organizational climate and supportive leadership have been associated with lower instances of bullying. Conversely, environments characterized by role conflict, ambiguity, and high stress levels may contribute to the occurrence of bullying behaviors (Escartín, 2016). Thus, the success of interventions can often be influenced by psychosocial factors such as organizational climate, leadership practices, and group dynamics. In sum, empirical evidence regarding the effectiveness of workplace bullying programs remains limited. Both organizational and individual-level strategies show some significant positive results, but their success is contingent upon factors such as proper implementation, organizational culture, and the presence of supportive leadership. Further high-quality research is necessary to identify the most effective approaches to prevent and mitigate workplace bullying (Table 4).
Implications for Practice, Police, and Research.
Note. Idsoe et al. (2021, p. 10).
A prior meta-analysis (Gaffney et al., 2019) shows that intervention programs are effective in reducing school BP by approximately 19–20% and school-BV by approximately 15–16%. These results reveal the effectiveness of intervention programs in reducing bullying. However, there are still young people and adults who suffer BV and its subsequent consequences. The complexity and severity of these consequences are probably related to the duration and intensity of the exposure (BV) and with several risk and protective factors that interact with BV (Idsoe et al., 2021).
Before the implication for practice, as aforementioned, more studies that assess the relation between BV and DTD/CPTSD are needed. If future high-quality studies show a positive association or casual relation between these variables, treatment of BV could be viewed within the conceptual framework of developmental interpersonal trauma, especially in children and adolescents. Idsoe et al. (2021) argue that treatments within this conceptual framework “should acknowledge the importance of a dysregulated stress-response system and problems related to emotion regulation” (p. 10). In terms of neurobiology, several studies have shown that BV, like child maltreatment, was associated with alterations (high or low levels of cortisol) in the hypothalamic-pituitary-adrenal (HPA) axis (Vaillancourt et al., 2011; Vaillancourt & Palamarchuk, 2021), and that sex was a potential moderator in the association between BV and cortisol secretion (Vaillancourt et al., 2008). Specifically, occasional exposure to bullying was associated with higher levels of cortisol for boys, while for girls it was associated with lower levels. This result may be due to the different perceptions and experiences in the social context. For example, in terms of social goals, males tend to value dominance more than females, while females tend to value inclusion more than do males. For girls, it may be possible that bullying from peers is perceived as more stressful than it is for boys, leading to lower levels of cortisol (Vaillancourt et al., 2008). This argument is in accordance with previous research that showed that hyposecretion of cortisol is the result of extreme or chronic stress while hypersecretion of cortisol is associated with less severe or acute stress (e.g., Pinto et al., 2016). In addition, fMRI studies also showed that socially excluded children and adolescents presented higher neural responses to social exclusion than controls (McIver et al., 2018; Will et al., 2016).
In terms of emotional regulation, as previously mentioned, BV was, overall, associated with each singular criterion of DTD: affective, physiological, attentional, behavioral, self, and relational dysregulation. Given these findings, Idsoe et al. (2021) recommend some clinical guidelines, especially for children:
a) “help children feel safe and support them in how to regulate their arousal”;
b) “change the environments from fear-inducing relationships with others into safe environments for healthy development”;
c) “a thorough mapping/assessment of the potential traumatic relationships the child has experienced be conducted (criteria A1 and A2 of DTD), along with the ongoing stressors they face, and the broad array of potential moderators present (e.g., age, gender, genetic vulnerabilities, and access to social support)”;
d) “the treatment should be tailored to the specific child” (p.10);
The authors also acknowledge the potential key role of educators and school staff in supporting bullied and traumatized children and give some key guidelines:
a) Educators can create trauma-sensitive environments and help traumatized children to feel safe and calm down. This will most likely lead to improvements in concentration, learning, and mental health;
b) Educators can try to identify potential triggers that children associate with bullying episodes from the past, which can lead to fear reactions;
c) Educators need to know when it is necessary to refer these children to a specialist.
Idsoe et al. (2021) conclude that anti-bullying interventions must be developed and employed at several tiers in order to be tailored according to severity, and that three-tier interventions are likely to be a good solution within schools: an universal tier for the majority of students; combined with a selected tier (with more intensive and comprehensive strategies) for students that report moderate problems after BV; and a indicated level for students that report high problems after BV. These interventions are, thus, tailored to the needs and characteristics of each child and target environmental factors.
With respect to adults, particularly in the context of workplace bullying (mobbing), the evidence base for effective interventions is less developed but nonetheless provides important practical insights. Systematic reviews indicate that both organizational- and individual-level strategies may reduce bullying, but their success depends heavily on contextual factors such as leadership practices, organizational culture, and the clarity of role expectations (Escartín, 2016; Gillen et al., 2017). Policies against bullying are necessary but insufficient unless they are explicitly formulated, implemented, and enforced (Cowan, 2011). In addition, psychosocial working conditions play a crucial role: environments characterized by supportive leadership and a positive organizational climate are associated with fewer bullying incidents, whereas high stress, role conflict, and ambiguity tend to increase risk (Escartín, 2016). Thus, in adult populations, interventions should combine structural measures (e.g., clear policies, reporting mechanisms, and training) with efforts to foster a supportive work environment. Such a dual focus may help to prevent bullying, mitigate its psychological consequences, and reduce the likelihood of chronic posttraumatic stress reactions, including symptoms of CPTSD.
Moreover, several authors have suggested that BV in adulthood may not occur in isolation but rather interact with earlier experiences of bullying or other interpersonal adversities (e.g., Brendgen & Poulin, 2018). Such continuity across developmental stages may contribute to cumulative trauma effects, reinforcing vulnerability to complex trauma symptomatology (Idsoe et al., 2021). This cumulative exposure framework aligns with developmental trauma theory, which posits that repeated or chronic victimization across the lifespan can disrupt affect regulation, self-concept, and relational functioning, which are core components of CPTSD (Ford et al., 2018; Herman, 1992). Therefore, when assessing adult victims of workplace bullying, it is important to consider prior histories of peer victimization as potential sensitizing experiences that may amplify posttraumatic responses.
In clinical settings, it is also important to mention that practitioners should conduct a differential assessment to distinguish between PTSD and CPTSD symptom presentations among individuals exposed to bullying. While both disorders share core posttraumatic features (i.e., re-experiencing, avoidance, and a persistent sense of threat) CPTSD additionally includes DSO (affective dysregulation, negative self-concept, and relational difficulties; Maercker et al., 2013). Recognizing this distinction is clinically relevant because it informs treatment planning and therapeutic focus. Interventions for PTSD primarily target fear-based symptoms through trauma-focused cognitive-behavioral methods, whereas CPTSD requires a broader, phase-oriented approach that integrates emotion regulation, identity reconstruction, and relational repair (Cloitre et al., 2012; Karatzias et al., 2019). Therefore, accurate assessment of CPTSD versus PTSD in bullying victims enables clinicians to tailor interventions more effectively and to prevent the potential under-treatment of complex trauma reactions.
In addition, future research should examine how the severity, frequency, and duration of BV, as well as individual characteristics such as personality traits and personal values, may shape the strength and nature of the association between BV and complex trauma symptoms.
It is also important to consider diversity factors, as gender, cultural, racial/ethnic, and socioeconomic differences may influence both the experience of BV and the manifestation of complex trauma symptoms. Future research should address these dimensions to better capture the variability in how bullying-related trauma develops and is expressed across different populations.
Major Priorities in this Field
To advance empirical understanding in this field, future research should prioritize three key directions. First, the development and validation of standardized, psychometrically sound self-report and clinician-administered instruments for assessing DTD are urgently needed, as the current absence of such tools hampers empirical testing of this construct (Ford et al., 2018; Morelli & Villodas, 2022). Second, cross-cultural comparative studies are essential to determine whether the associations between BV and complex trauma symptoms vary across sociocultural contexts, thereby enhancing the ecological validity and generalizability of findings. Third, longitudinal studies that explicitly examine causal mechanisms and developmental trajectories linking BV exposure to CPTSD and DTD symptoms are necessary to move beyond correlational evidence. Addressing these priorities will provide a stronger empirical foundation for theory, assessment, and intervention in bullying-related trauma research.
Footnotes
Author Note
This systematic review was registered in the “International Prospective Register of Systematic Reviews” (Prospero) in 2023 (CRD42023411244).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted at the Psychology Research Centre (CIPsi), School of Psychology, University of Minho, supported by the Foundation for Science and Technology (FCT) through the Portuguese State Budgets (Ref.: 2021.06671.BD) and (FCT; UID/01662: Psychology Research Centre (CIPsi)).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data,code,and other materials
This study is a systematic review and does not involve the collection of primary data. All data used in this review were obtained from publicly available sources, as cited in the manuscript. No additional data, code, or materials are available.