
Abstract
Sexual objectification of women is common and may expose them to events (e.g., interpersonal violence) that confer high risk for posttraumatic stress disorder (PTSD), and/or lead to self-objectification. This systematic review examines the relationships between self-objectification and trauma exposure, posttraumatic stress symptoms, and PTSD, identifying the measures used to assess self-objectification. Scopus, PsycINFO, Web of Science, OVID Medline, and CINAHL were searched through 23 January 2025. Peer-reviewed articles that measured self-objectification and assessed relationships between self-objectification and trauma exposure, posttraumatic stress symptoms, and/or PTSD were included. Thirteen articles with 5,035 participants met inclusion criteria; most recruited women exclusively. Quality was assessed using the Mixed Methods Appraisal Tool. Evidence was synthesized narratively. No articles evaluated interventions. Five measures were used to assess two conceptualizations of self-objectification: bodily self-objectification (e.g., body shame, body surveillance) and self-dehumanization. Associations varied with the conceptualization and measurement of self-objectification. Body shame was positively associated with trauma exposure and symptoms, including dissociation, while associations between body surveillance, trauma exposure, and trauma symptoms were inconsistent. Self-dehumanization was positively associated with trauma exposure. Overall, findings suggest a relationship between exposure to traumatic events and self-objectification. Further research is needed to clarify the influence of self-objectification on trauma symptomatology. Given the impact of violence, self-objectification, and PTSD on women, research that informs clinical practice is needed, along with policy-based actions that enhance women’s safety and wellbeing, particularly in the age of artificial intelligence.
Violence against women is prevalent globally, with an estimated one in three women experiencing lifetime violence (World Health Organization, 2021). Women are subjected to violence through systems that reinforce gender-based oppression, such as sexualization and objectification of women and girls that is ubiquitous in Western societies (Fredrickson & Roberts, 1997; Pecini et al., 2023). Women may be literally (e.g., treated as less-than-human objects; Beech et al., 2020; Nussbaum, 1999) and/or sexually (e.g., reduced to sexual parts/functions; Bartky, 1990; Fredrickson & Roberts, 1997) objectified. Interdependent systems of violence and sexual objectification manifest in events ranging from sexual harassment and intimidation to sexual assault (Fredrickson & Roberts, 1997; Kozee et al., 2007), all of which may have deleterious impacts on women’s mental health and wellbeing.
Sexual violence disproportionately impacts women (i.e., cisgender and trans women), and people socially perceived as women, even those who may not identify as such (e.g., non-binary people; Australian Bureau of Statistics [ABS], 2023; Callander et al., 2019; Kearl, 2018). Australian data from trans and gender diverse people indicates that sexual violence and coercion are more common among people assigned female at birth, compared to those assigned male 1 (Callander et al., 2019). Further, one in five women in Australia have experienced lifetime sexual violence compared to one in 16 men (ABS, 2023). Likewise, 81% of women in the United States (US) report experiencing sexual harassment and/or assault in their lifetime compared to 43% of men (Kearl, 2018). These data illustrate that gendered violence is potentially underpinned by sexual objectification, the consequences of which are borne predominantly by women and people perceived as women.
Posttraumatic Stress as a Result of Violence Against Women
Experiencing violence is associated with poor mental health outcomes (e.g., psychological distress, depression, anxiety, posttraumatic stress; Fernández-Fillol et al., 2021; Townsend et al., 2022). Sexual violence survivors experience higher rates of posttraumatic stress disorder (PTSD) than survivors of other interpersonal and non-interpersonal traumas (Kimerling et al., 2018; Liu et al., 2017; Tolin & Foa, 2006). PTSD may develop following exposure to a traumatic event that involves actual or threatened death, serious injury, or sexual violence, as defined by Criterion A of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR; American Psychiatric Association [APA], 2022). To be diagnosed with PTSD, a person must have experienced a Criterion A event, along with symptoms of intrusion (e.g., dissociation), avoidance (e.g., repression of memories), negative alterations in cognition and mood (e.g., fear, shame), and alterations in arousal and reactivity (e.g., hypervigilance). These disturbances must cause marked distress and/or functional impairment (APA, 2022). Although exposure to violence may be classified as a Criterion A event and confer risk for PTSD, non-Criterion A events may also have adverse consequences, including posttraumatic stress symptoms (Anders et al., 2011; Wamser & Richardson, 2024).
PTSD is also associated with emotion dysregulation and shame (Mirabile et al., 2024), suicidal thoughts and behavior (Krysinska & Lester, 2010), and other mental and physical health problems (e.g., cardiovascular conditions; Sareen, 2014). Shame has been identified in pathways to PTSD symptoms for people who have experienced interpersonal traumas, such as sexual assault (Mirabile et al., 2024; Seah & Berle, 2023). Even when the threshold for PTSD is not met, adverse outcomes (e.g., suicidal ideation) have been documented (Marshall et al., 2001; McLaughlin et al., 2015). Indeed, non-Criterion A events, such as discrimination and prejudice (e.g., racial discrimination; Wamser & Richardson, 2024), are also associated with PTSD symptoms (Anders et al., 2011). This points to the need to explore how exposure to sexual objectification, which may range from insidious oppression to direct violence (Holland et al., 2017; Kozee et al., 2007), influences trauma symptoms among women.
Women are more likely than men to experience traumatic events associated with PTSD (e.g., sexual and intimate partner violence; Kimerling et al., 2018; Tolin & Foa, 2006). Findings from a global survey (N = 34,676; Liu et al., 2017) indicated the prevalence of PTSD was highest for those who reported experiencing rape (17.4%), kidnapping (11.3%), and other sexual assault (11.0%); all traumas to which women are more likely to be exposed (Kimerling et al., 2018). These gendered patterns of trauma exposure increase women’s risk of developing PTSD compared to men. It is important to understand what factors exacerbate the risk of these traumas, the pathways from these events to psychological outcomes, and ways in which women can be supported to recover following these events.
Sexual and Self-Objectification as Gendered Risks for Trauma Symptomatology
Objectification is a form of psychological oppression that attacks personhood and reduces an individual to an instrument for others’ use, effectively dehumanizing them (Bartky, 1990; Nussbaum, 1999). According to the American Psychological Association (2007) Task Force on the Sexualization of Girls, sexualization occurs when a person’s value is based on their sexual appeal/behavior, when they are held to a standard that equates physical attractiveness with being sexy, when “sexuality is inappropriately imposed” (p. 1), and/or when they are sexually objectified (i.e., “made into a thing for others’ sexual use, rather than seen as a person”; p. 1). In other words, sexual objectification occurs when a person’s sexual parts/functions are treated as representing them (Bartky, 1990; Fredrickson & Roberts, 1997). Objectification, sexualization, and sexual objectification have been used interchangeably to explain these experiences, which has confused the literature, as these concepts are distinct (Beech et al., 2020; Grower & Ward, 2021). Objectification Theory (Fredrickson & Roberts, 1997) offers a way to explore the relationship between gender-linked exposure to potentially traumatic experiences (e.g., sexual violence) and posttraumatic stress symptoms.
Objectification Theory suggests women are routinely subjected to sexual objectification wherein their bodies are evaluated, and taken as objects for others’ use (e.g., sexual object for male gaze; Holland et al., 2017; Tiggemann & Williams, 2012). This is posited to result in self-objectification, whereby women internalize an observers’ perspective of themselves (e.g., view themselves as an object of sexual desire; Fredrickson & Roberts, 1997). Directly experiencing and witnessing sexually objectifying behavior (e.g., catcalling, groping) has been positively associated with self-objectification among women (Holland et al., 2017; Koval et al., 2019). Interpersonal sexual objectification is a form of violence that ranges from harassment and leering to sexual assault. Illustrating the ubiquity of sexual objectification, women in an Australian study (N = 81) reported being targeted by a sexually objectifying event approximately once every 2 days and witnessing objectification 1.35 times per day (Holland et al., 2017). Although less common than experiencing an objectifying gaze or catcalling, more severe forms of interpersonal sexual objectification (e.g., groping, sexual gestures) were reported to occur weekly (Holland et al., 2017). Regardless of whether sexually objectifying experiences are classified as traumatic events according to the DSM-5-TR (APA, 2022), they may be distressing and have negative psychological consequences.
Negative consequences of sexual objectification are theorized to occur via self-objectification (Fredrickson & Roberts, 1997), which may manifest as habitual monitoring of one’s body and how it appears (i.e., body surveillance; McKinley & Hyde, 1996). This may result in shame when one’s appearance does not conform to sociocultural standards (i.e., body shame; Daniels et al., 2020; McKinley & Hyde, 1996; Tiggemann, 2011). Focusing on observable bodily features is thought to lead to valuing appearance over functionality and agency, thereby contributing to viewing self as object (Fredrickson & Roberts, 1997; Lindner & Tantleff-Dunn, 2017). Indeed, Beech et al. (2020) posited that objectification can be conceptualized literally (e.g., treated as less-than-human object) and sexually (e.g., catcalled). There may be variation in the intrapersonal process of internalizing these perspectives (i.e., self-objectification). That is, self-objectification, too, can be conceptualized in multiple ways (e.g., self-dehumanization, sexual or bodily self-objectification).
Several measures are used to assess self-objectification (e.g., body shame, body surveillance; McKinley & Hyde, 1996). Even so, the conceptualization and measurement of self-objectification has been a persistent challenge (Calogero, 2011; Lindner & Tantleff-Dunn, 2017). Existing measures tap into different constructs that may “exact different consequences” (Grower & Ward, 2021, p. 69), such as cognitive, affective, or behavioral components of self-objectification. For example, self-objectification has often been operationalized as body surveillance, which, in turn, has predicted body shame. However, surveillance alone does not adequately capture the experience of internalizing an observer’s perspective, potentially overlooking ways of seeing the self as an object that extend beyond monitoring physical appearance (Calogero, 2011). For example, sexually objectifying encounters may result in women self-objectifying by monitoring their appearance and seeing themselves as less than human; however, these processes may not always occur simultaneously (Pecini et al., 2023). Research is needed to clarify how self-objectification is conceptualized and operationalized in the existing literature to understand the nature of what is being assessed and relationships among relevant outcomes, including mental health.
Research has found that self-objectification is associated with negative consequences that put women at increased risk for mental health disorders (see Jones & Griffiths, 2015; Tiggemann, 2011; Tiggemann & Williams, 2012). Indeed, self-objectification has been positively associated with body shame, appearance anxiety, and vigilance about bodily harm. These have been linked with eating disorders, depression, and sexual dysfunction (e.g., Calogero et al., 2021; Davidson & Gervais, 2015; Fredrickson & Roberts, 1997; Jones & Griffiths, 2015; Tiggemann & Williams, 2012). For example, in a momentary ecological assessment study with 268 women in Australia and the US, habitual self-objectification was found to predict increases in negative emotions, such as shame and guilt (Koval et al., 2019). Relatedly, it has been proposed that self-dehumanization, which can be considered an aspect of self-objectification, has negative consequences for women (e.g., tolerance of sexual harassment; Galdi & Guizzo, 2020; Pecini et al., 2023).
Self-objectification has also been positively associated with women’s exposure to violence in cross-sectional research (Davidson & Gervais, 2015; Jonnson et al., 2018). In a study of 1,005 female (70.8%) and male (29.2%) university students in Canada, self-objectification was positively associated with psychological, physical, and sexual victimization among females, but not males (Jonnson et al., 2018), suggesting there is something unique about women’s experiences of violence and self-objectification. Moreover, self-objectification explained the association between intimate partner violence and body shame in a study of 503 US undergraduate women (Davidson & Gervais, 2015). These findings indicate the potential for self-objectification to explain some of the psychological consequences associated with women’s experiences of violence.
Women at the Intersection
Research exploring the relationships between interpersonal sexual objectification, self-objectification, and posttraumatic stress has not attended fully to intersectionality. Most studies have recruited women who are cisgender, white, and attending university (see Calogero et al., 2021; Daniels et al., 2020) This limits generalizability and precludes consideration of the unique ways women experience overlapping systems of power. Intersectionality considers ways identities (e.g., ethnicity, sexuality) intersect to expose people to overlapping forms of marginalization within systems of power (Crenshaw, 1989). These intersections increase certain women’s risk of experiencing violence, feeling unsafe, vigilance to threats, as well as mental health difficulties (Watson et al., 2015).
Violence, objectification, self-objectification, and PTSD are known to be associated with poor mental health (Jones & Griffiths, 2015; Koval et al., 2019; Krysinska & Lester, 2010; Sareen, 2014; Tiggemann & Williams, 2012; Townsend et al., 2022), but scant attention has been devoted to how these issues intersect. Examining how these experiences overlap will enhance understanding of the etiology of PTSD symptoms and help clarify how objectification and self-objectification contribute to PTSD.
The Present Study
The aim of this systematic review was to synthesize the literature on the associations between trauma exposure, self-objectification, and posttraumatic stress symptoms. Four research questions were posed:
What is the relationship between trauma exposure and self-objectification?
What is the relationship between self-objectification and posttraumatic stress symptoms?
How is self-objectification measured in studies that examine trauma exposure and posttraumatic stress?
What interventions have aimed to reduce self-objectification among trauma survivors?
Method
The method and results for this study are reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines (PRISMA; Page et al., 2021). The review protocol was registered with Prospero (CRD42024547127).
Search Strategy
On 16 May 2024, Scopus, PsycINFO, Web of Science, OVID Medline, and CINAHL databases were searched for publications that investigated self-objectification and trauma. For comprehensiveness, searches were re-run twice (final search conducted on 23 January 2025). The search strategy was developed in consultation with an expert librarian (Supplemental Table 1). Records were extracted to EndNote 21 where duplicates were removed. Records were exported to Rayyan (Ouzzani et al., 2016). Title and abstract screening and full-text review were conducted separately by two researchers (ES, LR). During title and abstract screening, 14 discrepancies were resolved by a third researcher (JLM); during full-text review, one discrepancy was resolved by the same researcher.
Selection Criteria
Articles that (a) were published in a peer-reviewed journal; (b) were published between 1997 and January 2025; (c) included a measure of self-objectification; (d) reported on PTSD symptoms and/or diagnosis; and (e) examined the relationship between self-objectification and trauma exposure, PTSD symptoms and/or PTSD diagnosis were included. Articles published from 1997 onwards were included, as this was the year Objectification Theory was first published (Fredrickson & Roberts, 1997). Publications were excluded if they were (a) book chapters, (b) review articles or meta-analyses, (c) theses or dissertations, (d) perspective-type articles (e.g., commentaries, editorials), or (e) not available in English.
Data Extraction and Synthesis
Key details of included articles were extracted into a Microsoft Excel database. Variables included author(s); publication year; sample size and characteristics (e.g., age, gender); country where the study was conducted; measure(s) used to assess self-objectification, objectification, trauma exposure, and posttraumatic stress symptoms/disorder; associations between constructs of interest; and main findings. Heterogeneity of measures precluded meta-analysis. Results were synthesized narratively.
Quality Assessment
Two reviewers (ES, LR) independently assessed risk of bias using the Mixed Methods Appraisal Tool (MMAT; Hong et al., 2018). Discrepancies were discussed among the research team until agreement was reached. Authors of the MMAT do not recommend an overall score calculation: therefore, commentary on bias is presented.
Results
Database searches on 16 May 2024 retrieved 2,062 articles (530 duplicates); 1,532 titles and abstracts were screened. Thirteen articles (10 unique studies; 5,035 2 participants) met inclusion criteria, including two articles identified in subsequent searches (see Figure 1).
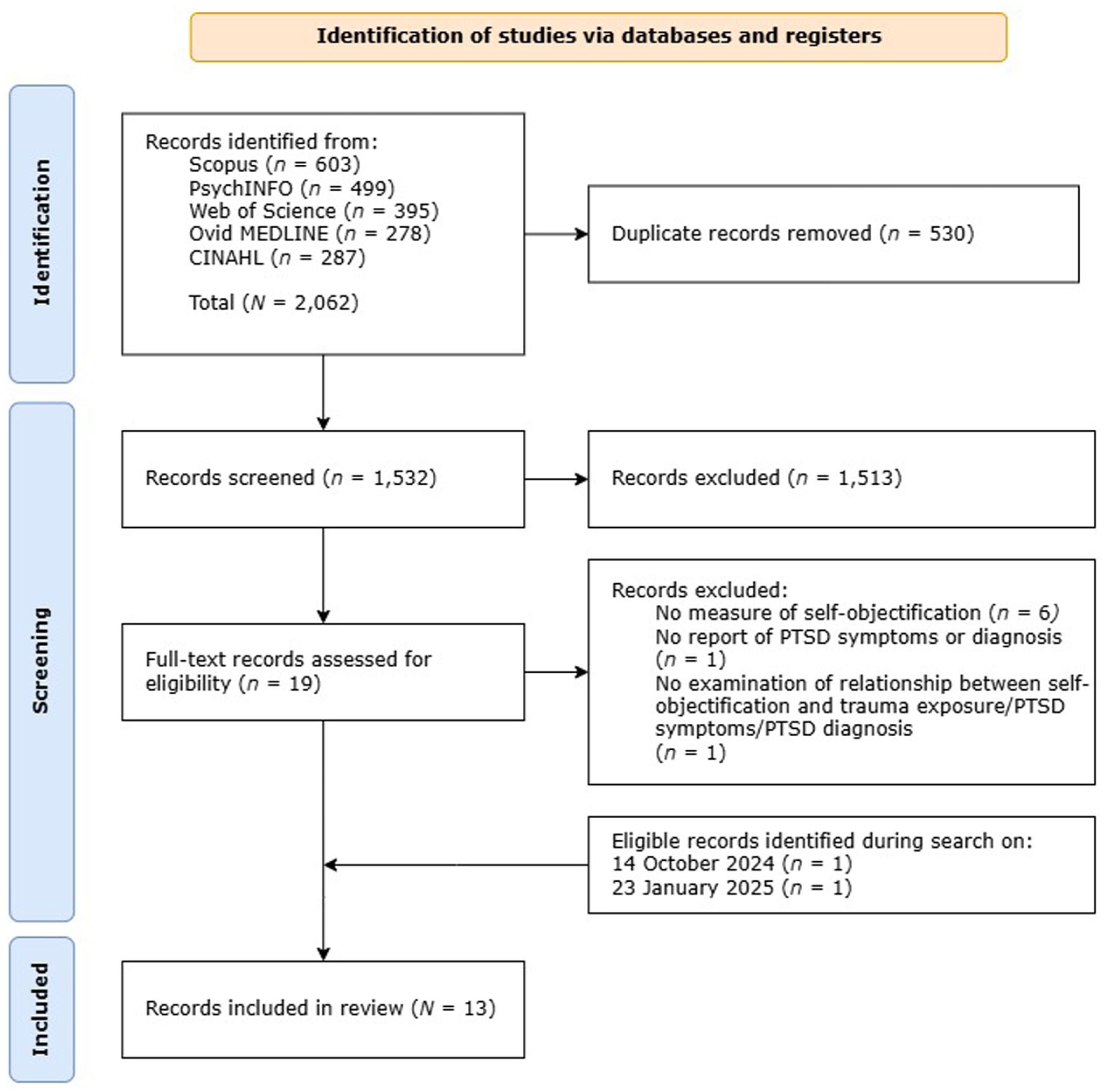
PRISMA flow diagram.
Study Characteristics
Articles were published from 2013 to 2024 and recruited adults (18–73 years; Table 1). Data were collected in the US (n = 7; Erchull et al., 2013; Hayes & Lease, 2023; Miles-McLean et al., 2015; Millen et al., 2019; Szymanski et al., 2024; Watson et al., 2013; Weaver et al., 2020) or Israel (n = 6; Ginzburg et al., 2024; Talmon & Ginzburg, 2016, 2017, 2018, 2019a; 2019b). Ten articles recruited women/female participants; three had mixed-gender samples (Talmon & Ginzburg, 2016, 2018, 2019b). Three studies (five articles) recruited college students (Talmon & Ginzburg, 2016, 2017, 2018, 2019b; Watson et al., 2013), one of which recruited ethnically diverse women (Watson et al., 2013). Six studies recruited women with histories of trauma and/or marginalization: sex trafficked vs not (Hayes & Lease, 2023), with/without sexual trauma history (Miles-McLean et al., 2015), pregnant/postpartum women (Ginzburg et al., 2024; Talmon & Ginzburg, 2019a), intimate partner violence survivors (Weaver et al., 2020), and in mental health/correctional settings (Millen et al., 2019).
Characteristics of Included Studies (N = 13).
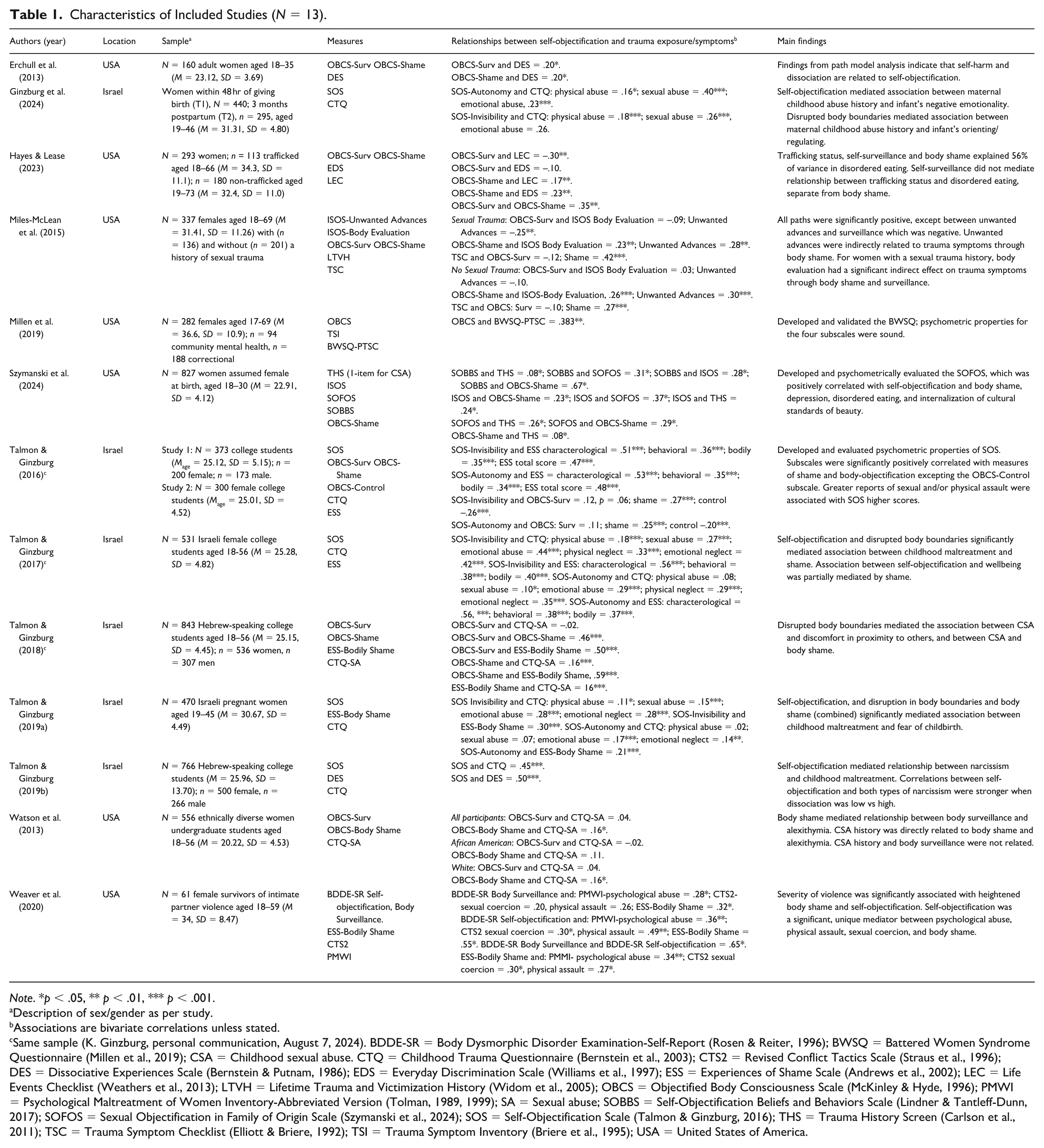
Note. *p < .05, ** p < .01, *** p < .001.
Description of sex/gender as per study.
Associations are bivariate correlations unless stated.
Same sample (K. Ginzburg, personal communication, August 7, 2024). BDDE-SR = Body Dysmorphic Disorder Examination-Self-Report (Rosen & Reiter, 1996); BWSQ = Battered Women Syndrome Questionnaire (Millen et al., 2019); CSA = Childhood sexual abuse. CTQ = Childhood Trauma Questionnaire (Bernstein et al., 2003); CTS2 = Revised Conflict Tactics Scale (Straus et al., 1996); DES = Dissociative Experiences Scale (Bernstein & Putnam, 1986); EDS = Everyday Discrimination Scale (Williams et al., 1997); ESS = Experiences of Shame Scale (Andrews et al., 2002); LEC = Life Events Checklist (Weathers et al., 2013); LTVH = Lifetime Trauma and Victimization History (Widom et al., 2005); OBCS = Objectified Body Consciousness Scale (McKinley & Hyde, 1996); PMWI = Psychological Maltreatment of Women Inventory-Abbreviated Version (Tolman, 1989, 1999); SA = Sexual abuse; SOBBS = Self-Objectification Beliefs and Behaviors Scale (Lindner & Tantleff-Dunn, 2017); SOFOS = Sexual Objectification in Family of Origin Scale (Szymanski et al., 2024); SOS = Self-Objectification Scale (Talmon & Ginzburg, 2016); THS = Trauma History Screen (Carlson et al., 2011); TSC = Trauma Symptom Checklist (Elliott & Briere, 1992); TSI = Trauma Symptom Inventory (Briere et al., 1995); USA = United States of America.
Twelve articles were cross-sectional; one article was longitudinal (Ginzburg et al., 2024). Ten articles tested theoretical models to identify whether the relationship between an independent variable (e.g., childhood maltreatment) and an outcome (e.g., trauma symptoms) was affected by a facet of self-objectification (e.g., body shame) alone or in combination with other variables (Erchull et al., 2013; Ginzburg et al., 2024; Hayes & Lease, 2023; Miles-McLean et al., 2015; Talmon & Ginzburg, 2017, 2018, 2019a, 2019b; Watson et al., 2013; Weaver et al., 2020). Body shame was frequently measured due to being a common aspect of self-objectification (i.e., Objectified Body Consciousness Scale [OBCS]; McKinley & Hyde, 1996). However, other facets of shame (e.g., characterological, behavioral) were also measured alongside self-objectification and trauma. Three studies developed measures: the Self-Objectification Scale (SOS; Talmon & Ginzburg, 2016), the Sexual Objectification in Family of Origin Scale (SOFOS; Szymanski et al., 2024), and the Battered Woman Syndrome Questionnaire (Millen et al., 2019). No articles reported evaluated interventions.
Self-Objectification Measures
Self-objectification was assessed using five measures (Supplemental Table 2): OBCS (McKinley & Hyde, 1996), Body Dysmorphic Disorder Examination Self-Report (BDDE-SR; Rosen & Reiter, 1996), Experiences of Shame Scale (ESS; Andrews et al., 2002), Self-Objectification Beliefs and Behaviors Scale (SOBBS; Lindner & Tantleff-Dunn, 2017), and SOS (Talmon & Ginzburg, 2016). Most studies administered measures informed by Objectification Theory (Fredrickson & Roberts, 1997) that focus on body-related facets of self-objectification, such as body surveillance and/or body shame (i.e., BDDE-SR, ESS, OBCS), that are theorized to occur as a result of acculturation to sexual objectification. Relatedly, Szymanski et al. (2024) used the SOBBS, which assesses the degree to which women both internalize an observer’s perspective and see their body as representing the self (Lindner & Tantleff-Dunn, 2017). Several studies used the SOS (Talmon & Ginzburg, 2016), a measure of self-objectification that focuses on self-dehumanization or the extent to which individuals lose subjectivity and see themselves as an instrument to satisfy others’ needs.
Eight articles administered the OBCS, which has three subscales (McKinley & Hyde, 1996). One used only the Body Shame subscale (Szymanski et al., 2024); five used the Body Surveillance and Body Shame subscales (Erchull et al., 2013; Hayes & Lease, 2023; Miles-McLean et al., 2015; Talmon & Ginzburg, 2018; Watson et al., 2013); and two also used the third subscale, Appearance Control Beliefs (Millen et al., 2019; Talmon & Ginzburg, 2016). Three studies (Talmon & Ginzburg, 2018, 2019a; Weaver et al., 2020) administered the ESS Bodily Shame subscale (Andrews et al., 2002). Weaver et al. (2020) used 5 of 28 BDDE-SR (Rosen & Reiter, 1996) items to measure self-objectification and body surveillance. Four studies (five articles; Ginzburg et al., 2024; Talmon & Ginzburg, 2016, 2017, 2019a, 2019b) used the SOS to measure self-objectification as a construct with two unique factors: invisibility and lack of autonomy.
Measures of Trauma Exposure and Posttraumatic Stress Symptoms
Eleven articles examined trauma exposure, specifically interpersonal trauma (e.g., sexual violence, childhood abuse). Seven articles (Ginzburg et al., 2024; Talmon & Ginzburg, 2016, 2017, 2018, 2019a, 2019b; Watson et al., 2013) used the Childhood Trauma Questionnaire (CTQ; Bernstein et al., 2003); two reported the Sexual Abuse subscale only (Talmon & Ginzburg, 2018; Watson et al., 2013). Miles-McLean et al. (2015) used the Lifetime Trauma and Victimization History (Widom et al., 2005) to screen for sexual assault history, along with the Interpersonal Sexual Objectification Scale (ISOS; Kozee et al., 2007). Szymanski et al. (2024) used the ISOS and a single Trauma History Screen (THS) item (Carlson et al., 2011) to assess childhood sexual abuse. Weaver et al. (2020) used the Revised Conflict Tactics Scale (Straus et al., 1996) and Psychological Maltreatment of Women Inventory (Tolman, 1989, 1999) to assess history of intimate partner violence. Hayes and Lease (2023) used the Everyday Discrimination Scale (Williams et al., 1997) and Life Events Checklist (LEC-5; Weathers et al., 2013). Four studies administered trauma symptom measures: Erchull et al. (2013) and Talmon and Ginzburg (2019b) used the Dissociative Experiences Scale (DES; Bernstein & Putnam, 1986), Miles-McLean et al. (2015) used the Trauma Symptom Checklist (TSC-40; Elliott & Briere, 1992), and Millen et al. (2019) used the Trauma Symptom Inventory (Briere et al., 1995). No studies reported PTSD diagnosis.
Relationships Between Self-Objectification and Posttraumatic Stress
Relationship Between Self-Objectification and Trauma Exposure
Ten articles reported relationships between trauma exposure and self-objectification; findings varied across articles. While some evidence suggested trauma exposure was negatively associated with body surveillance, it was largely positively associated with aspects of self-objectification, particularly body shame (see Table 2). Miles-McLean et al. (2015) found that among women with and without a sexual trauma history, sexually objectifying experiences (i.e., ISOS Body Evaluation and Unwanted Sexual Advances subscales) were significantly positively associated with body shame (OBCS). Among those with a sexual trauma history, scores on the ISOS Unwanted Sexual Advances and OBCS Body Surveillance subscales were significantly negatively associated. No significant relationship was found between the ISOS Body Evaluation and OBCS Body Surveillance subscales in either group (Miles-McLean et al., 2015). Szymanski et al. (2024) found that childhood sexual abuse was significantly positively associated with both self-objectification (SOBBS) and body shame (OBCS). The same study found significant positive associations between interpersonal sexual objectification (ISOS) and childhood sexual abuse (THS), self-objectification (SOBBS), and body shame (OBSC). In Hayes and Lease’s (2023) study, trauma exposure (LEC-5; Weathers et al., 2013) was significantly positively associated with body shame and significantly negatively associated with body surveillance (OBCS; McKinley & Hyde, 1996).
Summary of Key Findings in Relation to Research Questions.
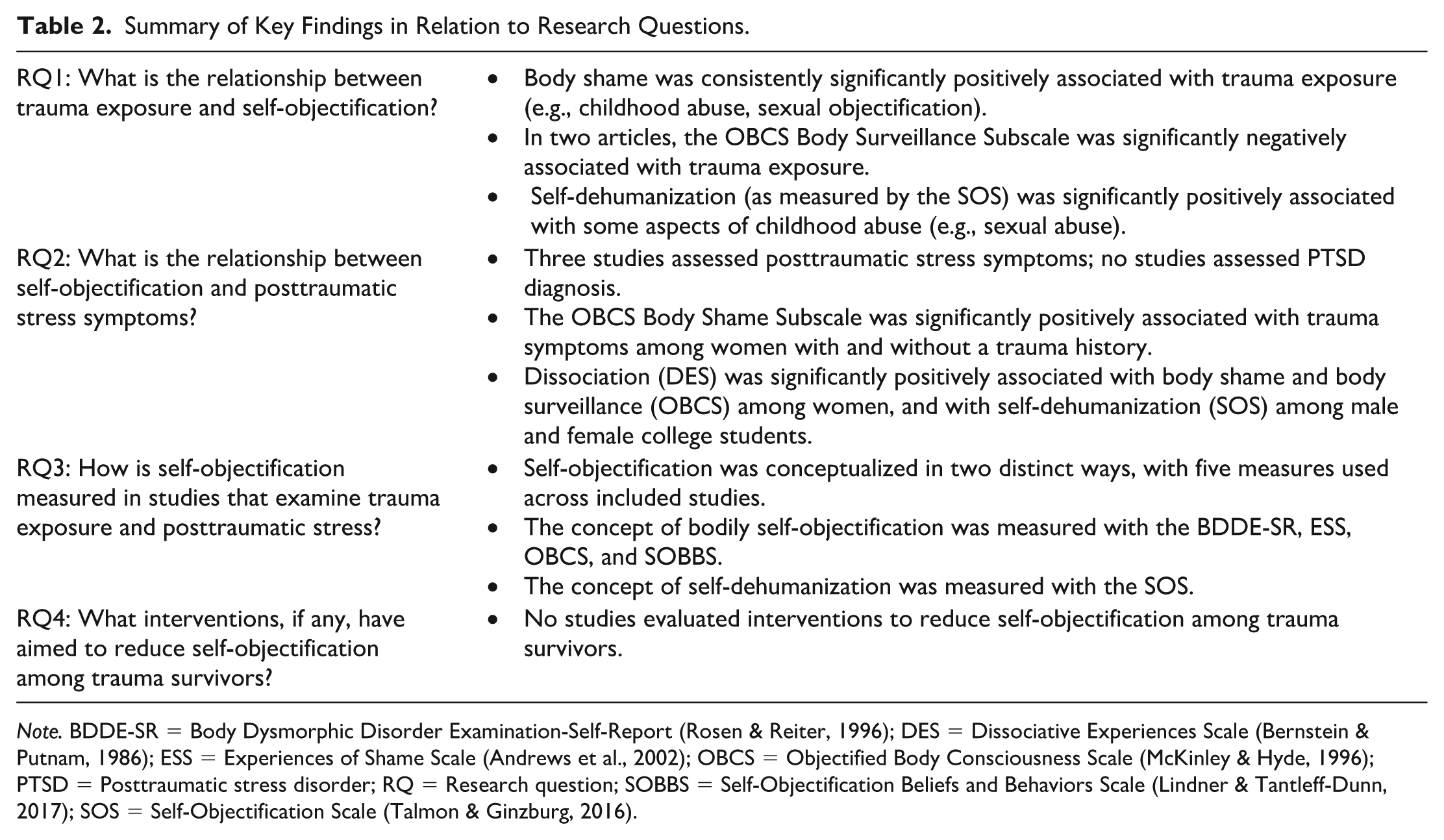
Note. BDDE-SR = Body Dysmorphic Disorder Examination-Self-Report (Rosen & Reiter, 1996); DES = Dissociative Experiences Scale (Bernstein & Putnam, 1986); ESS = Experiences of Shame Scale (Andrews et al., 2002); OBCS = Objectified Body Consciousness Scale (McKinley & Hyde, 1996); PTSD = Posttraumatic stress disorder; RQ = Research question; SOBBS = Self-Objectification Beliefs and Behaviors Scale (Lindner & Tantleff-Dunn, 2017); SOS = Self-Objectification Scale (Talmon & Ginzburg, 2016).
In a US study, childhood sexual abuse was significantly positively associated with body shame (OBCS) among White women, but not African American women (Watson et al., 2013). Among college men and women, childhood sexual abuse was significantly positively associated with body shame, as per the OBCS and ESS (Talmon & Ginzburg, 2018). In five articles (Ginzburg et al., 2024; Talmon & Ginzburg, 2016, 2017, 2019a, 2019b), relationships between the SOS and childhood trauma (CTQ) were examined among college students and pregnant/postpartum women. The SOS Invisibility subscale was significantly positively associated with emotional abuse (Ginzburg et al., 2024; Talmon & Ginzburg, 2017, 2019a), emotional neglect (Talmon & Ginzburg, 2017, 2019a), sexual abuse and physical abuse (Ginzburg et al., 2024), and physical neglect (Talmon & Ginzburg, 2017). The SOS Lack of Autonomy subscale was significantly positively related to emotional abuse (Ginzburg et al., 2024; Talmon & Ginzburg, 2017, 2019a), emotional neglect (Talmon & Ginzburg, 2017, 2019a), sexual abuse (Ginzburg et al., 2024; Talmon & Ginzburg, 2017), physical abuse (Ginzburg et al., 2024), and physical neglect (Talmon & Ginzburg, 2017).
Relationships between Self-Objectification and Posttraumatic Stress Symptoms
Three articles reported relationships between self-objectification and trauma symptoms. The OBCS Body Shame subscale was significantly positively correlated with trauma symptoms (TSC) amongst women with and without a history of sexual trauma (Miles-McLean et al., 2015). The OBCS Body Surveillance subscale was not significantly associated with trauma symptoms in either cohort (Miles-McLean et al., 2015). Dissociative experiences (DES) were significantly positively associated with both Body Surveillance and Body Shame subscales in adult women (OBCS; Erchull et al., 2013), and with self-objectification (SOS) among male and female college students (Talmon & Ginzburg, 2019b).
Pathways Between Trauma Exposure, Self-Objectification, and PTSD Symptoms
In a study on disordered eating among sex trafficking survivors, body shame (OBCS) trafficking status, and self-surveillance explained 56% of the variance in disordered eating, though self-surveillance alone did not mediate this relationship (Hayes & Lease, 2023). Among women with a sexual trauma history, sexual objectification in the form of body evaluation (ISOS) was indirectly and positively related to trauma symptoms (TSC) via body shame and surveillance (OBCS; Miles-McLean et al., 2015). Among women with and without a trauma history, unwanted sexual advances (ISOS) were indirectly and positively related to trauma symptoms via body shame (OBCS; Miles-McLean et al., 2015). Weaver et al. (2020) found self-objectification (BDDE-SR) mediated a positive relationship between intimate partner violence (i.e., psychological abuse, physical assault, sexual coercion) and body shame (ESS); the indirect effect of self-objectification best explained the total effect.
Childhood maltreatment had a significant indirect effect on narcissism through self-objectification (SOS), with associations between self-objectification and narcissism observed to be stronger when dissociation was low (Talmon & Ginzburg, 2019b). Among postpartum women, self-objectification (SOS) at baseline had a significant indirect effect on the positive association between maternal history of child abuse and infant negative emotionality at 3 months (Ginzburg et al., 2024). Self-objectification (SOS) and disrupted body boundaries (Sense of Body Boundaries Survey; Krzewska & Dolińska-Zygmunt, 2013) significantly mediated the positive association between childhood maltreatment and shame (Talmon & Ginzburg, 2017), with self-objectification (SOS) and the combination of disrupted body boundaries and body shame (ESS) also significantly mediating the positive relationship between childhood maltreatment and fear of childbirth (Talmon & Ginzburg, 2019a). Finally, Erchull et al. (2013) found internalization of objectifying media messages was significantly and positively associated with dissociation through body surveillance (OBCS).
MMAT Quality Assessment
Statistical analyses used to answer relevant research questions in each article were clearly stated and justified. Appropriate sampling strategies relevant to target populations and appropriate measures to assess constructs of interest (i.e., valid and reliable measures; Hong et al., 2018) were used in 10 of 13 articles. Where this was not the case, measures were either not validated for the sample or information about the reliability of language translations was not provided. Samples reported in most articles were questionable in their representativeness (Supplemental Table 3). Further, risk of non-response bias was greater than low for one article and uncertain for seven articles. This uncertainty was largely due to insufficient reporting on response rates, missing data, and management of missing data.
Discussion
The aim of this systematic review was to synthesize the literature on associations between self-objectification and trauma exposure, posttraumatic stress symptoms, and PTSD diagnosis, and to identify measures used to assess self-objectification. The 13 included articles were published between 2013 and 2024, indicating this is a nascent area within Objectification Theory research (Fredrickson & Roberts, 1997). Relationships between self-objectification and trauma exposure, and self-objectification and posttraumatic stress symptoms, were inconsistent. This was likely influenced by self-objectification measures and their respective subscale content relating differently to trauma exposure and trauma symptoms. Although mixed, the findings demonstrate an interplay between trauma exposure, objectification, and self-objectification, thereby contributing to the growing body of literature in this area and pointing to future research, practice, and policy considerations (Table 3).
Summary of Implications.
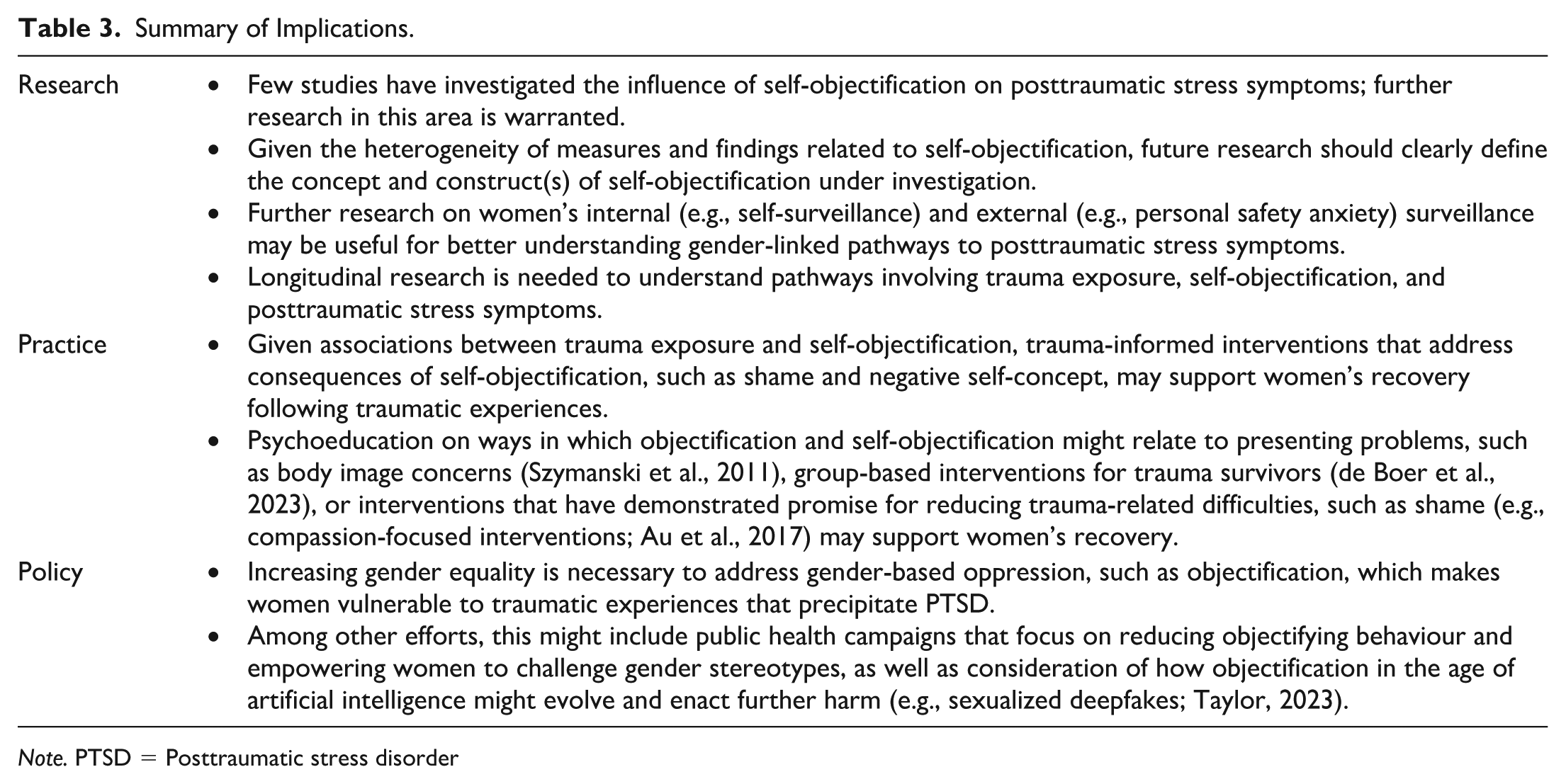
Note. PTSD = Posttraumatic stress disorder
Measuring Self-Objectification
Measures used in included studies were underpinned by two distinct self-objectification conceptualizations, one focusing on appearance-related concerns that arise in sexually objectifying environments (i.e., bodily self-objectification) and one focusing on self-dehumanization. Studies on self-dehumanization recruited college students (Talmon & Ginzburg, 2016, 2017, 2019b) or pregnant/postpartum women (Ginzburg et al., 2024; Talmon & Ginzburg, 2019a) and administered the SOS, which assesses “a process of self-dehumanization” (Talmon & Ginzburg, 2016, p. 54) not focused solely on an individual’s perception of their body or assumptions about a sexually objectifying environment (e.g., “Sometimes I feel invisible”, “I don’t let anyone treat me disrespectfully”). Findings from studies that used the SOS link childhood trauma and self-dehumanization, extending the literature on self-objectification by providing evidence that the impacts of being treated as less than human extend beyond sexual objectification (Ginzburg et al., 2024; Talmon & Ginzburg., 2016, 2017, 2019a, 2019b). The SOS is thus useful for understanding how traumatic experiences wherein a person treats another as a thing (e.g., less-than-human, location for violence) may affect self-concept and mental health, including views about self and autonomy (Talmon & Ginzburg, 2016).
Articles reporting on bodily self-objectification used measures focused on the consequences of internalizing sexual objectification due to living in cultures that view women’s bodies as sexual objects (Calogero, 2011). Although administered in only one study (Szymanski et al., 2024), the SOBBS captures the degree to which an observer’s perspective is taken when thinking about the body and to which the body is seen as representative of the self (Lindner & Tantleff-Dunn, 2017). The SOBBS factors measure concepts distinct from body surveillance, whereby the OBCS Body Surveillance subscale may be used in addition to the SOBBS when the intention is to assess habitual self-monitoring (Lindner & Tantleff-Dunn, 2017). In this way, the SOBBS addresses some limitations of using body surveillance as the sole measure of self-objectification (see Calogero et al., 2011). Despite progression in measurement of self-objectification (i.e., SOBBS), most articles assessed body-related aspects of self-objectification using OBCS subscales exclusively and found variation in their respective relationships to trauma exposure and symptoms. It is possible that inconsistent findings are related to the specific content of subscales. Arguably, the OBCS Body Shame Subscale assesses more affective responses (e.g., “I feel like I must be a bad person when I don’t look as good as I could”), while the OBCS Body Surveillance Subscale captures cognitive and behavioral processes, such as how frequently someone attends to their appearance and whether they think of their body more in terms of how it looks or how it feels (e.g., “I think about how I look many times a day”; McKinley & Hyde, 1996).
The Relationship Between Self-Objectification and Posttraumatic Stress
Relationships between self-objectification and trauma exposure/symptoms diverged depending on the self-objectification measure(s) and subscale(s) administered. Similarly, a systematic review on motherhood and objectification (Beech et al., 2020) reported that findings were influenced by measure choice; all purported to evaluate self-objectification but assessed “different concepts of the same construct” (p. 534). While other relationships were mixed, we observed a consistent positive relationship between trauma exposure and body shame. This may reflect the affective impact of objectification (or other traumas) and highlight potential links between self-objectification and trauma-related outcomes, such as shame.
Our findings suggest adverse outcomes related to trauma exposure occur, in part, via body shame (Erchull et al., 2013; Hayes & Lease, 2023; Miles-McLean et al., 2015). In one study, the positive relationship between unwanted sexual advances and trauma symptoms was mediated by body shame (Miles-McLean et al., 2015). Sexualized violence may lead to self-objectification and “attunement” (p. 894) to appearance that intensifies self-conscious emotions (e.g., shame), thereby worsening mental health (Koval et al., 2019). The affectively laden content of body shame subscales may therefore explain the positive relationship with trauma outcomes. Indeed, shame has been associated with self-objectification (Daniels et al., 2020; Koval et al., 2019), interpersonal trauma (e.g., intimate partner violence), and PTSD symptoms (Mirabile et al., 2024; Seah & Berle, 2022, 2023).
It is possible that during the process of self-objectification, individuals begin to see themselves as flawed (e.g., when appearance transgresses sociocultural norms) and apply global negative self-evaluations (e.g., “I am a bad person”; Mirabile et al., 2024) or begin to feel excluded or even invisible (e.g., Talmon & Ginzburg, 2017, 2019a, 2019b). Again, it is possible that the affective content in subscales relating to shame and invisibility explain their association with trauma exposure. Interestingly, despite childhood sexual abuse being significantly positively associated with body shame amongst White women, this was not the case amongst African American women (Watson et al., 2013), suggesting demographic variables may also explain differential findings relating to trauma and self-objectification.
Given that persistent negative emotional states and beliefs about the self (e.g., shame) are characteristic of PTSD (APA, 2022), further exploration of the influence of trait and state self-objectification on shame could illuminate paths between these variables and PTSD symptoms. This might provide evidence for the direction of relationships and identify potential intervention targets, however, consideration to demographic characteristics will be essential to broadening understanding. While the absence of interventions is conspicuous, findings from this systematic review indicate that clinical interventions that address self-concept and shame may reduce self-objectification following trauma exposure. Such interventions could include psychoeducation on how external and internal objectification might relate to presenting problems (Szymanski et al., 2011); group-based interventions for women trauma survivors (de Boer et al., 2023); and/or promising interventions for reducing trauma-related difficulties, such as shame (e.g., compassion-focused interventions; Au et al., 2017). Further research evaluating interventions targeting self-objectification and assessing the impact on trauma symptoms are needed.
In comparison to body shame, associations between body surveillance and trauma exposure/symptoms were mixed. This may be related to the content of the subscales assessing body surveillance, which represent cognitive and behavioral aspects of self-objectification. Reflecting on the negative relationship between trauma exposure and body surveillance, Miles-McLean et al. (2015) proposed that experiencing sexual objectification makes women more vigilant to environmental threats to personal safety, rather than to monitoring how their bodies appear. Eye-tracking technology has been used to evaluate what male and female participants were looking at when imagining walking around college campuses (Chaney et al., 2023). Female participants tended to focus on areas where danger may be present, particularly at night, and where risk of entrapment was high, suggesting they concentrate on identifying safety threats. In contrast, males tended to focus on the most direct route through the environment.
Women’s attentional focus has been explored in the context of Objectification Theory. Calogero et al. (2021) found that sexual and self-objectification were positively associated with safety anxiety, as measured by the Personal Safety Anxiety and Vigilance Scale. Personal safety anxiety was directly associated with women’s restricted freedom of movement and mediated the relationship from sexual and self-objectification to restricted freedom of movement. This provides support for the notion that women focus on external threats, rather than their appearance. Collectively, these findings suggest that, in addition to the subscale tapping into more cognitive/behavioral responses, vigilance to personal safety could partially explain mixed findings on the relationship between trauma exposure and/or symptoms and the body surveillance component of self-objectification.
Given the ubiquity of violence against women, it is unsurprising that women monitor safety threats, rather than appearance, when moving through the world (Calogero et al., 2021; Miles-McLean et al., 2015; World Health Organization, 2021). Safety vigilance may manifest more similarly to PTSD symptoms than body monitoring, particularly when avoiding stimuli associated with a traumatic event (e.g., place where one was harassed), such as by restricting movement (Calogero et al., 2021). Further investigation of women’s experiences of personal safety anxiety and PTSD symptoms could offer insights on gender-linked pathways to PTSD. Indeed, future research might explore an Objectification Theory model that includes personal safety anxiety and vigilance and posttraumatic stress. It remains to be seen whether internal (e.g., self-surveillance) or external (e.g., personal safety anxiety) surveillance focus depends on environment. For example, it is unknown whether differences in the focus of surveillance (e.g., self, environment) arise when in an objectifying public milieu, compared to a sexual encounter, where a person might be expected to focus on their body to a greater degree.
Limitations
Included studies had to report a relationship between self-objectification and trauma exposure/symptoms/diagnosis. This may have excluded articles that reported on potentially traumatic experiences without labelling them as a trauma. Only one study (Miles-McLean et al., 2015) reported relationships between self-objectification and trauma symptoms beyond dissociation, limiting conclusions about the influence of self-objectification on the spectrum of trauma symptoms. Further, few studies and heterogeneous measures limited the extent to which synthesis was possible. Recent research has highlighted that lack of consistent, clear definitions for objectification and synonymous use of terms obfuscate findings (Beech et al., 2020; Pecini et al., 2023). Future research should clearly define the concept and construct of self-objectification, so the relationship between self-objectification and posttraumatic stress symptoms can be elucidated and the impacts of self-objection better understood.
Participants in the included studies were relatively homogenous; most included white, college-aged women. Although several studies recruited minoritized groups (e.g., women with sexual trauma histories, African American women), research dedicated to exploring experiences of objectification, self-objectification, and posttraumatic stress among diverse cohorts (e.g., men and gender diverse folx, racialized women) with intersecting identities is needed, particularly given the high rates of violence against marginalized people. Without data on intersectionality, certain cohorts will continue to be misunderstood and marginalized, which will maintain health inequities. Further, most studies were cross-sectional and tested models informed by Objectification Theory (Fredrickson & Roberts, 1997), which proposes that sexual objectification is an antecedent to self-objectification and sets the stage for adverse psychological outcomes. Without temporal data, conclusions about the causal chain of events, directionality of relationships, and stability over time cannot be ascertained.
Conclusion
We found inconsistent relationships between trauma exposure and self-objectification, and self-objectification and posttraumatic stress symptoms. The five measures used in included studies were informed by distinct but related conceptualizations of self-objectification, potentially explaining the varied findings. However, a consistent positive relationship between body shame and trauma exposure/symptoms was identified in studies that assessed body shame as part of self-objectification, which may be due to the affective content of body shame subscales. Findings highlight the need to clarify relationships between objectification (sexual or otherwise) that exposes women to violence, and subsequently impacts their mental health, such as self-objectification and shame. Only three studies assessed the relationship between self-objectification and trauma symptoms (Erchull et al., 2013; Miles-McLean et al., 2015; Talmon & Ginzburg, 2019b), two of which focused on dissociation. This highlights the need for future research to explore the influence of self-objectification on the full range of trauma symptoms. Investigating the role sexual and self-objectification play in posttraumatic stress symptoms may identify opportunities and actions that could enhance women’s wellbeing at the individual (e.g., clinical intervention) and systemic level (e.g., policymaking). Addressing systems of gender-based oppression (e.g., objectification) that perpetuate violence against women may reduce exposure to events that make them vulnerable to PTSD, along with the negative consequences of self-objectification. Given that violence against women is prevalent worldwide and ever-evolving in the age of artificial intelligence (e.g., deepfake pornography; Taylor, 2023), women’s rights are increasingly under attack. There is a pressing need for research that informs individual- and policy-level interventions to enhance women’s safety and wellbeing and to prevent harm.
Supplemental Material
sj-pdf-1-tva-10.1177_15248380251395098 – Supplemental material for Objects of Trauma: A Systematic Review of Self-Objectification and Posttraumatic Stress
Supplemental material, sj-pdf-1-tva-10.1177_15248380251395098 for Objects of Trauma: A Systematic Review of Self-Objectification and Posttraumatic Stress by Elena Slodecki, Simone Buzwell, Lucca Randazzo and Jessica L. Mackelprang in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
We thank Ms Annette Steere, Library Liaison Team Leader, at Swinburne University of Technology for her assistance in developing the systematic review search strategy. We also thank Dr. Sharon Grant, Prof. Kay Cook, and Dr. Jessica Sharp for their constructive feedback on an early draft of this manuscript.
Author Note
Lucca Randazzo’s current affiliation is the Turner Institute for Brain and Mental Health, School of Psychological Sciences, Monash University, Melbourne, Australia.
Ethical Considerations
Ethical approval not required.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Australian Government Research Training Program (RTP) Scholarship awarded to Elena Slodecki.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article, as no new data were created or analyzed in this study. Search strategies can be viewed in the supplemental materials.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.