
Abstract
People living with dementia face a disproportionately high risk of abuse and neglect, yet safeguarding responses remain underexplored, particularly within the context of English legal and care systems. This realist review investigates how safeguarding practices for people with dementia operate in England, examining what works, for whom, in what circumstances, and why. Drawing on 44 studies published between 2014 and 2024, supplemented by extensive stakeholder engagement with individuals with lived experience, carers, practitioners, and community representatives, the review synthesizes evidence through Context–Mechanism–Outcome configurations. Five core domains emerged: stakeholder roles, conceptualization of abuse and neglect, safeguarding processes and diversity, safeguarding law and policy, and partnership working. Findings reveal that effective safeguarding depends not only on statutory frameworks like the Care Act 2014 and Mental Capacity Act 2005, but also on professional judgement, relational dynamics, and inter-agency collaboration. Significant barriers include inconsistent training, conceptual ambiguity, cultural stigma, and systemic under-resourcing. Importantly, safeguarding outcomes improves in environments where legal literacy, trust, and communication are strong, and services are culturally competent and person-centered. The review highlights the need for integrated, rights-based approaches and greater inclusivity in safeguarding systems to better protect diverse populations of people living with dementia.
Keywords
Introduction
People living with dementia are more likely to experience abuse or neglect than older adults without dementia, with prevalence estimates ranging from 27% to over 50% globally (Fang & Yan, 2018). Such abuse may take a variety of forms and can take place in the community or care homes. Dementia is “a collective name for progressive degenerative brain syndromes which affect memory, thinking, behaviour and emotion, which affects a person’s ability to perform normal daily activities” (Dementia Alliance International, 2021). In this paper, we adopt the position that dementia constitutes a disability, implying that individuals with dementia should be provided with support that maximizes autonomy and facilitates the pursuit of meaningful lives (Shakespeare et al., 2019). Research within community setting has highlighted several types of abuse against people living with dementia, including chronic verbal aggression, physical abuse, and neglect by family carers (Cooney et al., 2006; Cooper et al., 2009; Gimeno et al., 2021; Yan & Kwok, 2011). A systematic review of abusive episodes among home-dwelling persons with dementia reported a pooled prevalence of 15.7% for elder abuse, a statistic believed to underrepresent the actual prevalence given the challenges in detecting abuse in this population (Steinsheim et al., 2022). Other studies have identified concerns about the financial abuse of people living with dementia by family members or strangers (Fraga Dominguez et al., 2022; Rogers et al., 2023; Samsi et al., 2014). Research within care homes has identified abusive behaviors by paid carers toward people living with dementia, including verbal threats, the use of unlawful restraints, avoiding residents with difficult behavior and not giving enough time for feeding (Cooper et al., 2013; Moore, 2016).
In England, where this review is focused, the government has sought to tackle adult abuse and neglect through multi-agency safeguarding procedures. The Care and Support Statutory Guidance defines safeguarding as “protecting an adult’s right to live in safety, free from abuse and neglect” (Department of Health & Social Care, 2022). The first significant policy was No Secrets: Guidance on Developing and Implementing Policies to Protect Vulnerable Adults (Department of Health, 2000). This document set out the first national strategy; providing guidance to social services departments (which were named as the lead agency), National Health Service (NHS) trusts, health authorities, and the police. Whilst multi-agency was central to the policy, research indicated several problems. High-level strategic partnerships between agencies did not always translate into local collaboration, and safeguarding adults’ boards did not engage well with NHS safeguarding boards (Braye et al., 2012). There was a perception among local authority managers and health staff that the issue of adult abuse was not sufficiently prioritized within the NHS (Manthorpe et al., 2010; McCreadie et al., 2008), and cultural differences in the assessment and management of risk existed between agencies (McCreadie et al., 2008). A government consultation also reported joint working as “patchy” with some partners being unwilling to “come to the table” (Department of Health, 2008, p. 5).
No Secrets was superseded by the Care Act 2014, which put adult safeguarding on a statutory footing for the first time. Section 42 stipulates where an adult has care and support needs, is at risk of abuse or neglect, and cannot protect themselves, the local authority must make necessary enquiries to decide on protective action. Local authorities were given the lead responsibility for adult safeguarding with Section 43 of the Act stating that local authorities should establish a Safeguarding Adults Board. Safeguarding Adults Boards should help and protect adults at risk of abuse in their area and should coordinate such work across partner agencies. Schedule 2 of the Care Act lists the local authority, the integrated care board, and the Chief Officer of Police for the area as the key core members of the Safeguarding Adults Board, although local authorities may appoint representatives from other agencies, following consultation with other core members. While efforts have been made to strengthen multi-agency working, through the Care Act 2014, little is known about how social care and health professionals have conceptualized or responded to the abuse and neglect of people living with dementia since the legislation was introduced.
Although there is a growing body of research examining the abuse and neglect of people living with dementia, few studies have synthesized this evidence through a comprehensive review. Existing literature reviews tend to focus narrowly on specific types of abuse (e.g., financial or caregiver abuse) or are limited to particular settings, such as care homes (Fang & Yan, 2018; Wei et al., 2024). Moreover, most systematic reviews emphasize prevalence or risk factors, offering limited insight into the mechanisms and contextual factors that shape professional safeguarding responses. To date, there are no realist reviews that explore how safeguarding for people with dementia operates across different contexts in England, or how professionals interpret and apply safeguarding law in practice.
Methods
Patient, Public, and Professional Involvement
The review was informed by the involvement of three stakeholder groups with lived and professional expertise in safeguarding. One group functioned as the formal study advisory group, while the other two were community-based. Collectively, these groups included people living with dementia (n = 18), family carers (n = 9) with safeguarding experience (n = 4), professional caregivers (n = 2), health and social care practitioners (n = 3), a retired police officer, representatives from advocacy organizations (n = 1), a professional identifying as deaf, another as partially sighted, and four members of ethnic minority communities.
Engagement with these groups occurred at regular intervals throughout the study. The community groups were consulted on five separate occasions (between April 2023 and February 2024), and the advisory group met quarterly (between August 2022 and March 2024). Their contributions were integral to shaping the review process, particularly in refining program theories, interpreting Context–Mechanism–Outcome (CMO) configurations, and offering critical reflections on the conceptualization of abuse, the safeguarding process, legal interpretation, and partnership working. They expanded the review findings by drawing on their own experiences, offering critical reflections that contextualized the CMOs within diverse cultural, social, and community settings.
Their insights highlighted critical gaps within the existing literature, particularly concerning the limited representation of people living with dementia and their family carers, the under exploration of cultural and ethnic diversity, and the structural barriers that hinder access to safeguarding systems for minority populations. Their contributions extended beyond critique, providing illustrative examples of effective safeguarding in practice, where positive outcomes were attributed to the coherent alignment of legal frameworks, statutory responsibilities, and community-led initiatives. By embedding these diverse perspectives into the analytical process, stakeholder engagement not only enriched the conceptual depth of the emerging program theories but also ensured that the review remained closely aligned with the realities of those most affected by safeguarding interventions.
Realist Review Design and Process
Given the complexity of safeguarding practices for people living with dementia, a realist synthesis approach was adopted to explore what works, for whom, in what circumstances, and why (Wong et al., 2013)). This methodology is particularly well-suited to examining complex systems interventions involving multiple actors, systems, and contextual influences. Unlike traditional systematic reviews, which focus primarily on effectiveness and generalizability, or scoping reviews that map broad topic areas, realist synthesis aims to uncover the underlying mechanisms that generate outcomes and how specific contexts shape these mechanisms (Pawson, 2006). It provides a valuable framework for examining complex issues such as multi-agency collaboration, professional reasoning, legal interpretation, and safeguarding responses. In keeping with realist methodology (Jagosh, 2019; Jagosh et al., 2012; Wong et al., 2013), data were analyzed using CMO configurations to explain how safeguarding processes operate under different conditions. Mechanisms were further disaggregated into Mechanism (Resource), the intervention or structural input intended to produce change (e.g., training, policy, legislation) and Mechanism (Response), the cognitive, emotional, or behavioral reaction triggered in participants by the resource, which ultimately influences outcomes. Context (C) is defined as the social, organizational, political, and demographic conditions in which safeguarding occurs, including geography, workforce capacity, and characteristics of individuals at risk (e.g., age, ethnicity, disability). While the Outcome (O) is understood as the intended or observed results of the activities, as reported in the literature or identified through stakeholder consultation.
This review was conducted in five key stages as detailed below (Pawson, 2006). The review period was extended to incorporate literature published up to February 2024, ensuring that recent developments in policy and practice were captured. Additional iterative searches were undertaken during this period to account for emerging themes and gaps identified in earlier stages of synthesis. These changes were necessary to ensure the relevance of the review findings in a rapidly evolving area of adult safeguarding.
Scoping and Theory Development
The review questions were refined through collaborative discussions with the research team, Patient and Public Involvement and Engagement (PPIE) group members, and professionals. These resulted in the development of concepts aligned with the core research questions:
a) What are the roles and responsibilities of key stakeholders in identifying, managing, and reducing safeguarding risks?
b) How does partnership working function, how effective is it, what are its pathways and mechanisms, and for whom does it work?
c) How do health and social care professionals conceptualize abuse and neglect, and how do they interpret and apply safeguarding law?
An exploratory scoping phase combined preliminary literature searches with stakeholder consultation to support the development of initial theories. This early work identified recurring concepts related to risk, protection, decision-making, and professional practice, particularly in relation to legal frameworks such as the Care Act 2014 and the Mental Capacity Act 2005. These insights helped shape the focus and theoretical direction of the review.
Search Strategy and Iterative Searching
An initial background familiarization search was conducted to identify appropriate databases and develop relevant search terms related to safeguarding for people living with dementia. Consultations with a specialist librarian helped refine both the terminology and the scope of the search strategy, ensuring alignment with the review’s conceptual focus. A systematic and iterative search was performed using a combination of Mesh terms and text words: “Dementia” AND “Safeguarding” OR “Abuse” OR “Neglect” (Supplemental file 3). The following databases were screened: ASSIA, CINAHL, Web of Science, PsycINFO, and Google Scholar (utilizing Publish and Perish software). Moreover, expert referencing was also utilized to identify any additional relevant literature that the research team was aware of (Figure 1). Searches were initially carried out in March 2022 and updated in February 2024 to include the most recent evidence. Studies were eligible for inclusion if they were published between 2014 and 2023, written in English, conducted in England, and focused on dementia and safeguarding, including related themes of abuse and neglect. Eligible sources included primary research and policy briefs that contributed to an understanding of context, mechanism, or outcome (CMO) in safeguarding processes and supported program theory development. Studies were excluded if they were published before 2014; conducted outside of England (including Wales, Scotland, Northern Ireland, or other international contexts); not available in full text; not written in English; or focused on dementia without clear relevance to safeguarding. Documents exclusively addressing training without broader engagement with safeguarding practices in the context of dementia were also excluded. A detailed overview of the search process is provided in the PRISMA flow diagram (Figure 1).
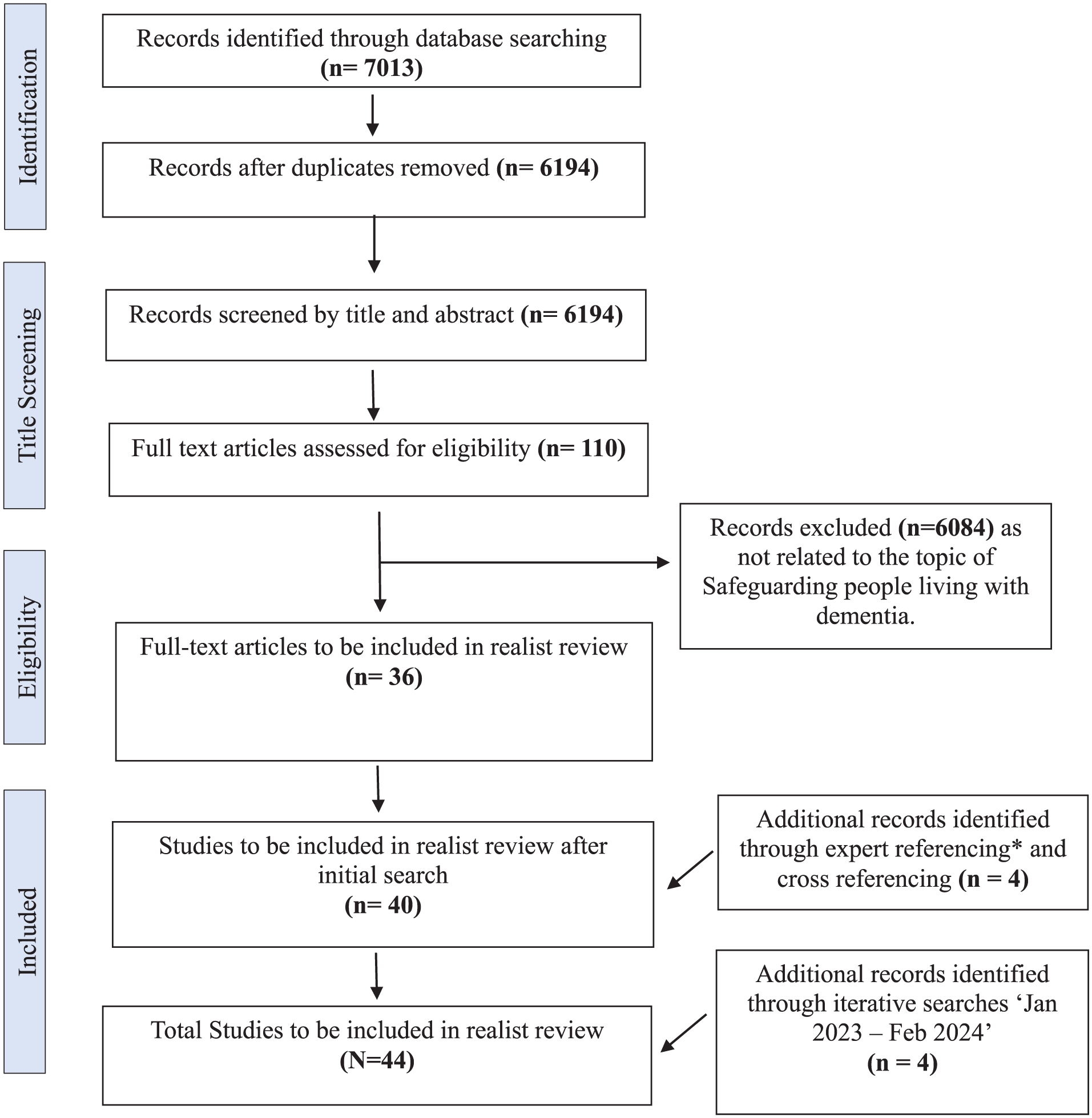
PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) flow diagram.
Selection and Evidence Appraisal
Articles were initially screened and organized by KS using Rayyan and EndNote, with RL advising on the organization of sources for theory development, and JD contributing to final appraisal decisions to ensure interpretive rigor. Each source was appraised using realist-informed criteria of relevance, rigor, and richness (Supplemental file 1) (Pawson, 2006), with inclusion determined by its contribution to explaining the core concepts in theory-building rather than adherence to traditional evidence hierarchies (Wong et al., 2013). Relevance was judged by the degree to which a study addressed safeguarding for people living with dementia and contributed to understanding one or more elements of a CMO (Context, Mechanism, Outcome). Rigor refers to the credibility and transparency of the data presented in the article, rather than the methodological quality of the study design. This aligns with RAMESES guidance, which discourages the use of rigid checklists for methodological appraisal in realist reviews (Wong et al., 2013). Richness assessed the explanatory depth of each source (Dada et al., 2023), whether it offered insight into how and why safeguarding practices were effective or limited within particular contexts, and whether it supported or challenged emerging theories. A wide range of literature types was included, qualitative studies, reviews, policy documents, and professional commentaries, to reflect the multidisciplinary and context-sensitive nature of safeguarding in dementia care.
Data Extraction
To ensure consistency in data interpretation, three researchers (KS, RL, and JD) initially extracted CMOs from four randomly selected articles. Each researcher worked independently, after which a consensus meeting was held to harmonize coding approaches and develop a shared analytic framework. This process was further validated in consultation with a realist review expert, who provided methodological guidance and confirmed alignment with best practices in realist synthesis. Following this calibration exercise, one researcher (KS) conducted the primary extraction of CMOs from the remaining articles, with regular oversight and input from the other two researchers (RL, JD) to ensure fidelity to the agreed framework. Extracted data focused on the interaction between contextual factors, mechanisms (disaggregated into resource and response), and safeguarding outcomes. A realist-informed extraction matrix was used to capture the following key elements:
Contextual features (e.g., policy environment, organizational setting, demographic variables)
Mechanism–Resource (e.g., training, legal mandates, professional frameworks)
Mechanism–Response (e.g., trust, resistance, compliance, confidence)
Outcomes (e.g., abuse identification, access to support, safeguarding failures or successes)
Stakeholder roles and inter-agency pathways
Consideration of diversity, including protected characteristics and intersecting vulnerabilities.
Synthesis
The analysis focused on identifying patterns in how mechanisms operate in specific contexts to produce particular outcomes. Extracted CMOs were coded and organized using NVivo (v12), with matrix queries developed around concept-based themes to support comparison and pattern identification across studies and PPIE consultations (Supplemental files 1 and 2). Through iterative analysis, CMOs were refined and grouped into five overarching theory domains: stakeholders and roles; conceptualization of abuse and neglect; safeguarding process and diversity; safeguarding law and policy; partnership working. Theories were constructed through cross-study synthesis and triangulated with insights gathered from stakeholder consultations. These were articulated using “if–then” statements, capturing how safeguarding outcomes emerge from the interaction between mechanisms and contexts. This process allowed for theory refinement grounded in both empirical data and experiential knowledge, ensuring that findings were explanatory and applicable across settings. Summaries of the key findings and illustrative CMOs from the included articles are presented in Supplemental files 1 and 2.
Findings
A total of 44 published articles were included (Figure 1), of which 4 were obtained through iterative searches. Among these, 19 were research articles (qualitative n = 11, mixed methods n = 7, RCT n = 1, quantitative n = 1), 5 book chapters, 3 service evaluations, 3 systematic reviews, and 14 other articles (opinion/editorial/clinical intelligence/legal update/CQC analysis/reports). The main characteristics of the included articles are detailed in Supplemental file 1. The findings describe how the safeguarding process, as stipulated in the Care Act 2014 works for people living with dementia in England and the contexts in which it applies. An initial scoping of the literature and discussion with PPIE groups and professionals helped to identify broad conceptual categories for theory development. These categories include stakeholders and their roles (n = 17), conceptualizing terms, process, and person-centered approach (n = 11), understanding of safeguarding law (n = 12), and partnership working (n = 13). A total of 12 articles discussed various aspects of diversity, including migrant representation (n = 1), socioeconomic status (n = 3), sexual identity (n = 2), ethnic backgrounds (n = 4), and protected characteristics (disabilities) (n = 2) in dementia care.
The study team alongside PPIE groups and professionals developed and refined the initial program theories using “If-Then” statements that resulted in 48 CMOs (contexts, mechanisms resource, mechanism response, and outcomes configurations) (Supplemental files 1 and 2). A narrative summary of the CMOs is discussed under the categories of stakeholder roles, conceptualization, safeguarding process and diversity, safeguarding law and policy, and partnership working.
Stakeholders and Their Roles in Safeguarding:
The findings highlight that safeguarding in the context of dementia is a complex and multifaceted process, influenced by the progressive nature of the condition, cognitive decline, care settings, and the roles and responsibilities of both family members and professionals. Several key contextual factors influence safeguarding effectiveness, including the vulnerability of both people living with dementia and care staff, challenges in professional boundaries, risks associated with refusals of care, institutional cultures within care homes, and systemic gaps in training and policy implementation (Supplemental files 1 and 2) (Abrams et al., 2019; Backhouse et al., 2018; Backhouse, 2021; Backhouse et al., 2021, 2022; Baird et al., 2023; Baker, 2017; Benbow & Kingston, 2017; Car et al., 2017; Carter, 2015; Cooper et al., 2016; Cooper & Livingston, 2020; Dalphinis, 2016; Dixon, 2023; Dixon et al., 2020, 2022; Gibson et al., 2016; Hopkinson et al., 2021; Manthorpe & Martineau, 2016; Marsland et al., 2015; Mileski et al., 2019; Moore, 2019, 2020; Peate, 2016; Penhale, 2014; Soilemezi et al., 2023; Sorinmade et al., 2021; Stevens et al., 2021; Tingle, 2014; White & Alton, 2022; Wood, 2019). These contexts create tensions between protection, autonomy, and the ability to identify risks, often requiring a balance between safeguarding interventions and the rights of people living with dementia.
Effective safeguarding requires the coordinated efforts of multiple stakeholders across the health, social care, legal, and financial sectors (CMO10 in Supplemental file 2). The findings highlight the critical roles of social workers, police, advocates, healthcare professionals, and other agencies in safeguarding people living with dementia. Data indicate that social workers provide leadership, supervision, and advocacy, including capacity and best interest assessments (Dixon et al., 2020, 2022; Harding, 2017), while police respond to emergencies and criminal cases (Dixon et al., 2020; Harding, 2017; Lee et al., 2019; Manthorpe & Martineau, 2016). Advocacy, such as through Independent Mental Capacity Advocates (IMCAs), Independent Domestic Violence Advisors (IDVAs), Lasting Power of Attorney (LPA) and court appointed deputies ensure that the views of people living with dementia are represented (Baker, 2017; Dixon et al., 2022; McGarry et al., 2014; Morgan & Andrews, 2016; Samsi et al., 2014). The government also has a role in publicizing the value of LPAs to prevent and criminalize financial abuse (Samsi et al., 2014).
Healthcare Professionals
Healthcare professionals play a significant role in safeguarding due to their frequent contact with people living with dementia. Regular health assessments provide opportunities to detect signs of abuse or neglect or health deterioration that might otherwise go unnoticed, especially in socially isolated individuals. However, gaps in safeguarding and dementia training often limit HCP’s ability to recognize and report concerns effectively. Training programs on behavioral indicators, legal responsibilities, and safeguarding processes can enhance professional awareness and integrate safeguarding into clinical care. This, in turn, can improve the reporting of safeguarding concerns, leading to appropriate interventions that enhance the safety and protection of people living with dementia (CMOs 1, 2 in Supplemental file 2) (Backhouse, 2021; Benbow & Kingston, 2017; Marsland et al., 2015; Rogers et al., 2023; Stevens et al., 2021; Tingle, 2014; White & Alton, 2022; Wood, 2019). When routine health checks are neglected, PLWD (Person (s) Living With Dementia) and their families may perceive this as institutional neglect (CMOs 3 in Supplemental file 2). Inconsistencies in conducting routine health checks further exacerbate the risk of neglect. National guidelines (NICE, 2018) emphasize the importance of regular health reviews, yet their implementation remains inconsistent due to resource constraints and systemic factors. When these checks are neglected, emerging health issues may go unnoticed, increasing the risk of harm and leading to perceptions of institutional neglect. Conversely, when conducted consistently, they facilitate early intervention, ensuring that people living with dementia receive timely support and reducing the likelihood of safeguarding failures. However, achieving this requires a shift toward proactive safeguarding, with clearer accountability structures, enhanced workforce training, and stronger integration of safeguarding measures within healthcare practice.
Advocacy
Advocacy is essential in safeguarding decisions, particularly to empower and represent people living with dementia. As dementia progresses, people living with dementia may experience difficulties in decision-making and consenting to safeguarding measures. The appointed advocates (IMCA/IDVA/LPA/Deputy) have an important role in supporting people living with dementia during safeguarding proceedings by ensuring that their voices are heard, and their rights are upheld. When advocates are present, there is a higher likelihood that safeguarding interventions are more person-centered, respectful, and aligned with individual’s preferences, ultimately leading to better safeguarding outcomes (CMO 4,5 in Supplemental file 2) (Baker, 2017; Dixon et al., 2020, 2022; Morgan & Andrews, 2016; PPIE). The voluntary sector, including charities and community organizations, support safeguarding by providing advocacy, outreach, and specialized services for people living with dementia. Voluntary organizations play a key role in detecting financial abuse, particularly among isolated, however, limited collaboration with statutory safeguarding services limits their impact (Samsi et al., 2014). Moreover, gaps in service provision mean older survivors of domestic violence often struggle to access support, as safeguarding policies are frequently geared toward younger populations (McGarry et al., 2014).
Care Staff
Care home staff play a crucial role in safeguarding people living with dementia, yet professional boundaries, training, institutional culture, and ethical dilemmas related to care provision shape their ability to do so effectively. Both residents and care staff are vulnerable to abuse, making professional boundaries essential for safeguarding. However, a rigid approach to boundaries may conflict with the need for person-centered care, requiring flexibility to ensure both protection and dignity (Abrams et al., 2019). The issue of refusals of care further complicates safeguarding, as people living with dementia who decline assistance may be at risk of forced care or neglect. The Mental Capacity Act (MCA, 2005) provides a legal framework for managing such situations, but inconsistent implementation and limited training often lead to inappropriate interventions (Backhouse, 2021; Backhouse et al., 2022).
Dementia-related changes in behaviors, such as distress, aggression, or “wandering,” pose risks to both people living with dementia and care staff, sometimes resulting in restrictive practices like physical restraints or sedation. While statutory frameworks such as Deprivation of Liberty Safeguards (DoLS) and Care Quality Commission (CQC) guidance emphasize proportionate, least-restrictive interventions, staff often experience conflicts in balancing human rights with safety concerns (Backhouse et al., 2018). The cultural environment within care homes also impacts safeguarding practices, with staff often fearing repercussions for whistleblowing. Although safeguarding training is essential, its effectiveness is limited if staff concerns are not addressed (Mileski et al., 2019; Moore, 2020). Additionally, the shift toward positive risk-taking, which promotes autonomy while managing risks, presents challenges in care settings where risk aversion remains dominant (Backhouse et al., 2021). Strengthening safeguarding requires not only improved training but also institutional changes that support open communication, clear reporting mechanisms, and a balanced approach to protection and autonomy (CMO 6 and 7 in Supplemental file 2).
Social Workers, Police, and Social Care
Social workers, social care staff, and police play distinct yet interconnected roles in safeguarding people living with dementia, particularly in responding to abuse, neglect, and financial exploitation. Social workers are central to safeguarding processes, conducting Section 42 inquiries under the Care Act (2014) and ensuring that safeguarding interventions align with legal and ethical frameworks (Dixon, 2023). However, their decision-making is influenced by both legislation and personal values, leading to inconsistencies in whether a case is treated as a safeguarding issue or a care need (Dixon et al., 2022). Social workers also face challenges in balancing positive risk-taking with protection, as the Convention on the Rights of Persons with Disabilities (CRPD) and MCA (2005) emphasize autonomy, yet professionals often struggle to apply these principles in practice (Dixon et al., 2020) (CMO 8 in Supplemental file 2).
The police play a key role in investigating abuse, particularly in cases of physical, sexual, and financial exploitation of people living with dementia (Lee et al., 2019). However, underreporting remains a significant challenge, as safeguarding adult reviews (SARs) suggest that professionals, including social workers and police, sometimes fail to recognize signs of abuse or act on concerns (Manthorpe & Martineau, 2016). Communication barriers between agencies further limit the effectiveness of safeguarding responses, with multi-agency safeguarding hubs and Safeguarding Adult Boards (SABs) struggling to ensure coordinated efforts (Harding, 2017). Financial abuse is often hidden within family dynamics, and police involvement is limited by difficulties in gathering evidence and securing prosecutions (Dalley et al., 2017) (CMO 9 in Supplemental file 2). Social care staff, including homecare workers, play a critical frontline role in safeguarding, as they often provide direct care to people living with dementia. However, a lack of resources and insufficient safeguarding training can result in poor identification and reporting of abuse (Carter, 2015). Social care staff also face significant workplace pressures, such as high caseloads and limited time to engage meaningfully with people living with dementia, which can lead to neglect (Car et al., 2017). Moreover, safeguarding within home care settings is particularly complex due to financial abuse risks and the hidden nature of mistreatment within families, making early intervention difficult (Dalley et al., 2017) (CMO 7 in Supplemental file 2)
Public Members, Regulators, Voluntary Sector Organizations, and Financial Institution
Financial abuse is a significant risk for people living with dementia, who may be exploited by those close to them, such as caregivers or family members or through scams. Collaboration between banks, post offices, voluntary sectors, social services, and legal professionals is crucial in detecting and preventing financial exploitation. If financial institution staff are trained to recognize indicators of financial abuse, remain vigilant, and work closely with safeguarding teams, they can serve as an additional layer of protection for vulnerable individuals. The partnership approach facilitates the identification of financial exploitation and ensures that safeguarding measures are implemented to protect people living with dementia, their financial assets, and overall well-being (CMO 11 in Supplemental file 2) (Dalley et al., 2017; Hopkinson et al., 2021; Samsi et al., 2014; Stupple et al., 2015; Tingle, 2014).
Regulatory bodies, such as SABs, the CQC, and Clinical Commissioning Groups, oversee safeguarding practices but face challenges in enforcement, inter-agency communication, and resource allocation (CMO 11 in Supplemental file 2). The CQC monitors care home standards, but budget cuts have led to training deficiencies, impacting staff competency in safeguarding procedures (Carter, 2015). SARs highlight failures in multi-agency safeguarding coordination, with professionals expressing distrust in each other’s safeguarding responses (Dalley et al., 2017). Additionally, financial abuse cases often do not result in prosecutions (Dalley et al., 2017; Samsi et al., 2014).
Conceptualization
A significant contextual factor is the absence of clearly defined thresholds for acceptable caring practices, which contributes to challenges in recognizing and reporting abuse and neglect within dementia care (Backhouse et al., 2022). This ambiguity often leads to the normalization of abusive behaviors, where actions that are harmful, such as locking individuals with dementia indoors, forced care, or speed feeding are misconstrued as protective measures by family members, professionals, or caregivers (Backhouse et al., 2018, 2022; Benbow & Kingston, 2017; Cooper & Livingston, 2020). Such practices often become routine, particularly in institutional settings, as highlighted in studies demonstrating that victims sometimes adopt euphemistic language to describe abusive experiences, thereby diminishing perceptions regarding the severity of abuse. This normalization highlights the need for a cultural shift among all stakeholders involved in dementia care, fostering an environment where abuse and neglect are promptly recognized and reported (CMO 12, 13 in Supplemental file 2).
The complexity surrounding definitions of abuse is also significant conceptually. Definitions of abuse can vary among family members, professionals, and caregivers. This subjectivity leads to disparities in understanding about what constitutes acceptable versus unacceptable behavior, making it challenging for care workers to determine when to report perceived abuse to their managers due to unclear reporting thresholds. Although legislative frameworks, such as the Care Act 2014 and its accompanying statutory guidance, provide definitions and guidance, they are susceptible to varying interpretations, heavily relying on the level of training received by health and social care professionals (see CMOs 12–14 in Supplemental file 2) (Backhouse et al., 2018; Backhouse, 2021; Backhouse et al., 2021, 2022; Benbow & Kingston, 2017; Cooper & Livingston, 2020; Dixon et al., 2020; Greene et al., 2019; Lee et al., 2019; McGarry et al., 2014; Mileski et al., 2019; Moore, 2019, 2020; Saloniki et al., 2022).
Beyond definitional challenges, stigma and fear also play a significant role in deterring individuals with dementia and their caregivers from reporting instances of abuse (CMO 14–15 in Supplemental file 2). For example, concerns about social embarrassment, potential retaliation by an abuser, or being disbelieved contribute to underreporting (Dixon et al., 2020; Greene et al., 2019; McGarry et al., 2014). Self-neglect further complicates safeguards, as individuals may not recognize their deteriorating condition, and inconsistencies in local policies may limit appropriate intervention (CMO 16 in Supplemental file 2). Cultural differences also influence perceptions of acceptable care, highlighting the need for increased awareness and clearer communication to ensure that safeguarding measures are responsive to diverse perspectives and needs (CMO 17 in Supplemental file 2) (Backhouse et al., 2022).
Safeguarding Process and Diversity
Under the Care Act 2014, the safeguarding process is structured into four key stages: identifying and reporting a concern, information gathering and Section 42 enquiries, developing a safeguarding plan, and review. This statutory framework is designed to protect adults at risk by ensuring early identification, coordinated multi-agency responses, and systematic learning from SARs (CMO 28 in Supplemental file 2). In the identification and reporting stage, multiple barriers hinder timely intervention. Cultural stigma and fear of discrimination may prevent people living with dementia and their caregivers from disclosing abuse, particularly in the case of minority communities, older adults experiencing domestic violence and those who identify as LGBTQ+ (CMOs 21–25 in Supplemental file 2) (Cooper & Livingston, 2020; Dixon et al., 2022; Harding, 2017; Lee et al., 2019; Lonbay, 2018). Communication barriers, including the use of untrained family interpreters, may lead to misrepresentation of concerns, making it harder for professionals to assess risk accurately (CMO 22 in Supplemental file 2). Additionally, restrictive practices such as locking a person with dementia indoors or excessive restraints may be normalized in domestic or care settings, delaying the recognition of these acts as abusive (Cooper & Livingston, 2020). The presence of coercive control further complicates disclosure, as people living with dementia may fear repercussions from family members or caregivers who exert undue influence over them (CMOs 14, 18, 19 in Supplemental file 2).
The information gathering during safeguarding enquiries demands clear interagency communication and comprehensive data collection (Cooper & Livingston, 2020; Harding, 2017). However, inadequate dementia awareness and cultural beliefs that frame adversity as “God’s will” (CMOs 23–24 in Supplemental file 2) pose challenges. In some communities, dementia remains poorly understood, and families may prefer secrecy over external intervention, particularly if they fear reputational damage or retaliation. When professionals lack understanding of these sociocultural dynamics, trust may diminish, discouraging PLWD and carers from engaging in the safeguarding process (CMOS 8, 21–25 in Supplemental file 2) (Dixon et al., 2022; Sorinmade et al., 2021). Coercive control, including misuse of LPA or pressured advance decisions, complicates protection efforts (CMOs 18–19 in Supplemental file 2). Professionals may struggle to override such decisions without clear evidence, especially in cases involving financial abuse or isolation (Dixon, 2023; Stephens & Walker, 2021). These challenges are compounded when PLWD cannot recall incidents, self-neglect is not recognized, or the abuser is another vulnerable adult (PPIE).
Safeguarding plans can promote positive risk-taking (balancing potential benefits against the likelihood and severity of harm) (Stevens et al., 2018) through shared decision-making, where people living with dementia and their families are supported in identifying meaningful outcomes (CMO 20 in Supplemental file 2) (Backhouse et al., 2021; Cooper & Livingston, 2020; Dixon et al., 2022; Morgan & Andrews 2016). However, conflicts of interest arise when caregivers also hold legal authority, and weak legal safeguards in areas like forced marriage or unregulated religious advice can limit professional intervention (Harding, 2017). Addressing these complexities requires a trauma-informed, rights-based safeguarding approach (PPIE).
The review stage, including serious adult reviews (SARs), is essential for evaluating the effectiveness and outcomes of safeguarding measures, identifying systemic failures, and improving future practice (CMO 28 in Supplemental file 2) (Dixon, 2023; Dixon et al., 2022; Manthorpe & Martineau, 2016; Morgan & Andrews, 2016). Discussions with PPIE members revealed that certain risks, such as cuckooing, are addressed more effectively, where individuals living with dementia are quickly removed from exploitative situations and provided with alternative housing (CMO 14 in Supplemental file 2). However, significant limitations remain, particularly when safeguarding training is reduced to a “tick-box” exercise (CMO 29 in Supplemental file 2), which undermines professionals’ ability to navigate complex cases. Practical barriers, such as limited digital literacy among people living with dementia (PPIE discussion), hinder follow-up and access to online safeguarding resources or reporting mechanisms. Gaps in accessible signposting continue to limit awareness and engagement with safeguarding services (PPIE). To address these challenges, safeguarding approaches must become more integrated, culturally competent, and person-centered, ensuring that legal and procedural frameworks support autonomy while mitigating abuse and coercion (Cooper & Livingston, 2020; Dixon, 2023).
Safeguarding Law and Policy
The findings highlight that adequate training and funding constitute essential mechanisms for enhancing professional knowledge and ensuring that safeguarding responsibilities are carried out with due regard for individuals’ rights. When HCPs lack a comprehensive understanding of the Mental Capacity Act and its associated frameworks, such as the DoLS, there is a risk that individuals’ rights may be inadvertently compromised (Carter, 2015; Dalphinis, 2016) (CMO 33–37 in Supplemental file 2). Empirical evidence indicates that 42% of care homes mandated by the Care Commission (CQC) to make improvements exhibited deficiencies in MCA training, while 29% had not delivered adequate training on DoLS (Carter, 2015). Moreover, it was observed that one in ten care homes classified as “inadequate” were unlawfully restricting residents’ liberty due to improper implementation of DoLS, thereby suggesting a prevalent misinterpretation or misapplication of the MCA (Carter, 2015).
Within this context of limited resources and training, two main mechanisms drive outcomes. Firstly, limited application of the MCA (Baker, 2017; Harding, 2017) may lead professionals to place an undue emphasis on protective measures, potentially diminishing the consideration of individual autonomy (CMOs 35–36 in Supplemental file 2). Although the MCA intends to empower individuals who lack capacity through best-interest decisions, it is sometimes treated as a procedural formality (Backhouse, 2021). Secondly, integrating additional legal frameworks, notably the UN CRPD can encourage shared decision-making and further support autonomy (CMO 39 in Supplemental file 2). However, the literature suggests that professionals’ awareness of the CRPD varies, and there can be tension between the MCA’s best-interest principle and the CRPD’s emphasis on legal capacity and supported decision-making. Still, combining these frameworks may help practitioners strike a better balance between enabling positive risk-taking and ensuring protection (Dixon, 2023; Dixon et al., 2022).
In settings where training is prioritized, legislation is clearly understood, and interagency collaboration is strong (Care Act, 2014), safeguarding referrals increase, and professionals feel more confident in respecting the rights of people living with dementia (Carter, 2015; Dixon, 2023). The Care Act’s six principles of empowerment, protection, prevention, proportionality, partnership, and accountability alongside “making safeguarding personal,” have led to more person-centered approaches and a notable rise in safeguarding referrals. Conversely, underfunded or poorly coordinated environments perpetuate fear of liability, gaps in knowledge, and inclination toward overly prescriptive safeguarding approaches (Harding, 2017; Mileski et al., 2019). In such circumstances, individuals may face unlawful deprivations of liberty, inadequate reporting of abuse, or overly restrictive “best-interest” decisions that limit autonomy. Additional legislation, such as the Mental Health Act, the Domestic Abuse Act 2021, and human rights instruments (European Convention on Human Rights, Human Rights Act 1998), further intersects with dementia care (Thomas & Milligan, 2018), emphasizing the complexity of safeguarding in practice. Newer measures (e.g., the Forced Marriage Unit, Office of the Public Guardian) also require consistent updates to professional training to protect individuals with dementia from exploitation or coercion.
Partnership Working
The safeguarding of people living with dementia relies on effective partnership working across healthcare, social care, law enforcement, and voluntary sectors. However, the context in which these partnerships operate significantly influences their effectiveness. The findings highlight a key contextual factor is the involvement of multidisciplinary teams, which enable best practice sharing and timely intervention. However, role ambiguity among professionals can lead to ineffective safeguarding responses, particularly in cases requiring swift action, such as domestic abuse and neglect (Abrams et al., 2019; Mileski et al., 2019) (CMOs 41–42 in Supplemental file 2). Early engagement with people living with dementia and their families is crucial to ensure that person-centered practices are in place before crises arise (Backhouse et al., 2021; Baird et al., 2023; Penhale, 2014) (CMO 46 in Supplemental file 2). Additionally, care home settings pose unique challenges due to under-reporting of abuse, the power dynamics between caregivers and residents, and the lack of external oversight (Manthorpe & Martineau, 2016). Policy changes, such as the 2021 Domestic Abuse Act, have shaped the safeguarding landscape, yet professionals require clearer guidance on their responsibilities. Furthermore, inter-agency mistrust and assumptions about professional roles often delay safeguarding interventions (Dalley et al., 2017; Stephens & Walker, 2021).
The effectiveness of partnership working in safeguarding depends on key mechanisms, including communication, trust, and shared and clearly defined professional responsibilities. Communication between agencies is fundamental, with timely data-sharing improving case coordination and preventing crises (CMO 42 in Supplemental file 2). However, poor communication can result in safeguarding failures, particularly when professionals assume that another agency is responsible for acting (Hopkinson et al., 2021; Stupple et al., 2015) (CMO 43–45 in Supplemental file 2). Trust among professionals is also crucial in ensuring that safeguarding concerns are taken seriously. When agencies have confidence that referrals will be acted upon, safeguarding reporting rates are higher, creating a proactive safeguarding culture (Dalley et al., 2017; Manthorpe & Martineau, 2016). A key aspect of trust is maintaining a stance of “respectful uncertainty,” where professionals remain open to uncertainty rather than assuming all is well. Additionally, clarifying professional responsibilities strengthens safeguarding partnerships. For instance, in cases of sexual abuse, forensic assessments require coordinated multi-agency responses to support evidence collection and prosecution. However, the lack of external involvement in care home safeguarding investigations limits transparency and hinders accountability (Abrams et al., 2019; Lee et al., 2019).
These mechanisms directly impact safeguarding outcomes. Effective communication and use of relevant systems enables timely interventions, while strong inter-agency trust leads to increased reporting and prompt responses (Hopkinson et al., 2021; Stupple et al., 2015) (CMOs 47, 48 in Supplemental file 2). Conversely, poor communication between agencies can result in delayed interventions and worsened outcomes for people living with dementia. Inter-agency mistrust may lead to reluctance to report abuse, particularly in care homes where external oversight is limited (Manthorpe & Martineau, 2016). Failure to coordinate safeguarding in cases of abuse can result in missed forensic evidence collection, affecting legal outcomes (Lee et al., 2019).
Discussion
Summary of Findings
This review analyzed how collaborative processes across health, social care, and allied sectors shape the implementation and effectiveness of safeguarding interventions for people living with dementia in England. The analysis revealed that safeguarding is a dynamic process embedded in professional judgment, organizational culture, legal interpretation, and structural inequalities (Nieman, 2024; Tracy, 2024). Across the studies, what emerged most prominently was the contextual sensitivity of safeguarding outcomes. Where professionals operated within well-resourced, relationally oriented, and legally informed systems, safeguarding was more likely to be timely, rights-based, and person-centered. In such settings, mechanisms of trust, proactive communication, and shared responsibility were activated, enabling coordinated interventions that respected both protection and autonomy. Conversely, in settings marked by high staff turnover, role ambiguity, and poor inter-agency collaboration, safeguarding mechanisms were limited. The evidence suggests that merely having formal structures in place is insufficient; it is the quality of relationships, clarity of roles, and shared understanding of legal and ethical frameworks that ultimately determine effectiveness.
A critical finding is the persistent tension between autonomy and protection. While legal frameworks such as the Mental Capacity Act (2005) and the Care Act (2014) emphasize person-centered approaches, these are frequently undermined by risk-averse cultures, particularly in institutional settings. The notion of “best interest” was at times interpreted in ways that limited individual agency, particularly when a person with dementia declined care or resisted interventions. In such contexts, safeguarding became synonymous with control, leading to coercive practices sometimes framed as protection. This reflects a wider challenge in dementia care, where declining capacity, ambiguous thresholds of harm, and conflicting familial interests complicate efforts to uphold rights while managing risk. Ethical complexities of balancing individual liberty with the duty of care are evident in the literature (Braye et al., 2017; McHale & Noszlopy, 2025).
Equally striking is the conceptual ambiguity surrounding abuse and neglect. Safeguarding thresholds varied widely, not only between sectors but among professionals. Behaviors such as restrictive practices, confinement, or neglect of basic health needs were sometimes normalized, justified as necessary, particularly when framed within narratives of carer burden or institutional constraints. This normalization reflects a broader epistemic gap. In the absence of clear, context-sensitive definitions and reporting mechanisms, abuse is rendered invisible. The review highlights the urgent need for cultural change in how abuse is recognized, narrated, and addressed in dementia contexts.
Relatively few studies have explored diversity-related aspects, limiting understanding of how safeguarding practices apply across different populations with dementia. Only a minority of studies engaged with how ethnicity, gender, sexuality, socioeconomic status, or migrant status mediate safeguarding risks and outcomes. Where such considerations were addressed, they revealed how stigma, discrimination, and cultural misrecognition created additional layers of vulnerability. Minority ethnic carers reported fear of judgment and a lack of culturally appropriate services, LGBTQ+ older adults described mistrust of statutory agencies, people with limited English proficiency encountered communication barriers that inhibited disclosure. In such contexts, mechanisms of help-seeking, advocacy, and institutional trust were disrupted. The limited data and intersectional analysis make it difficult to understand how safeguarding affects different groups of people living with dementia.
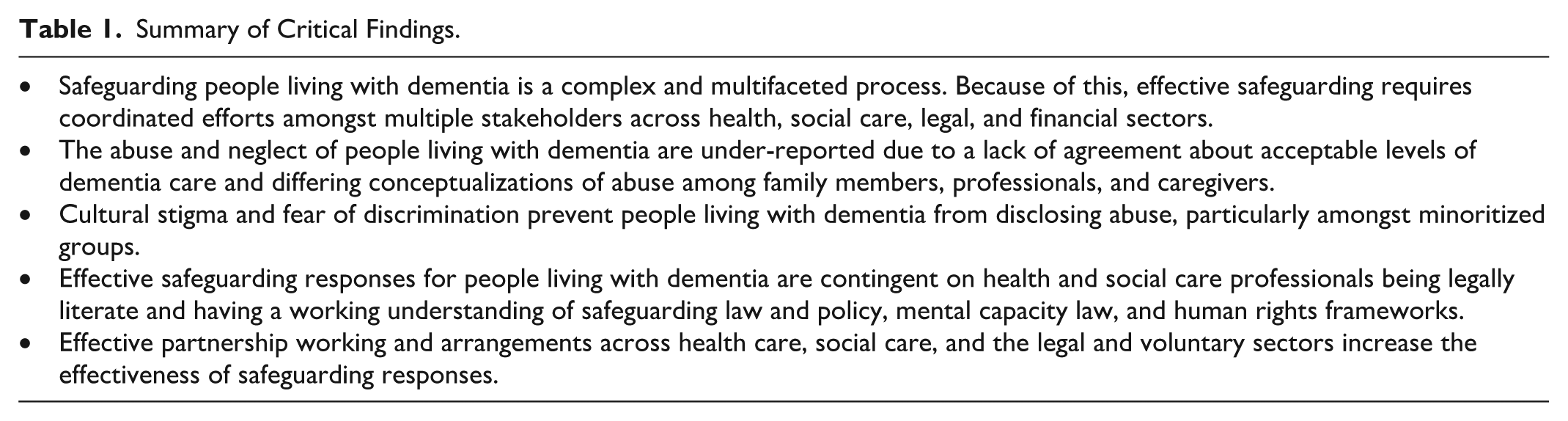
Working in partnership emerged as both an enabler and a challenge. Where inter-agency collaboration was embedded in routine practice, supported by shared protocols and mutual trust, safeguarding outcomes improved. However, persistent issues of role confusion, siloed practices, and mistrust between agencies undermined joint working. The assumption that another professional or agency “will deal with it” appeared as a recurring explanatory mechanism in safeguarding failures. These findings indicate the need for shared accountability frameworks and cross-sectoral learning environments to guide proactive professional action. Table 1 provides a concise synthesis of the critical findings identified in this review.
Summary of Critical Findings.
Implications for Practice, Policy, and Research
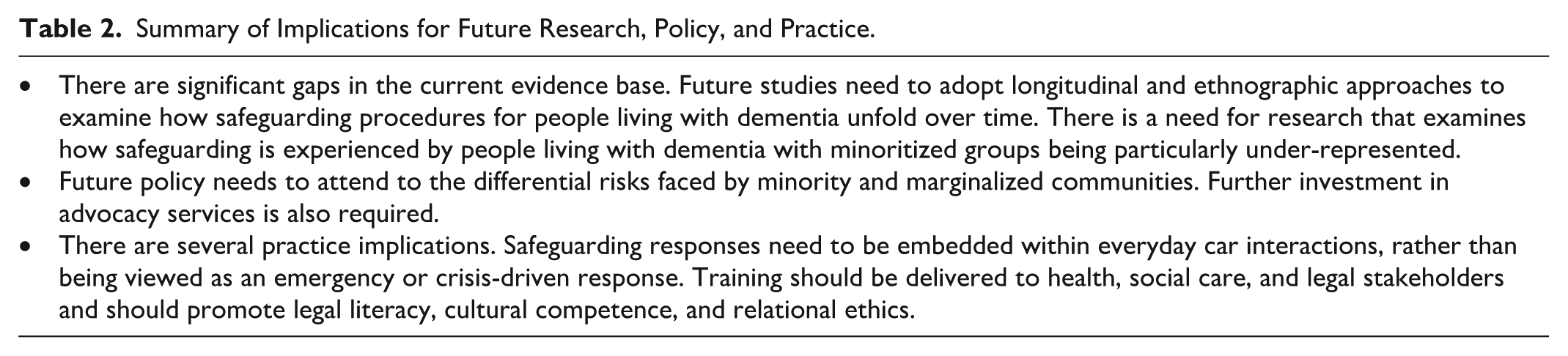
This review highlights several critical implications for professional practice, policymaking, and future research (see Table 2). The findings demonstrate that safeguarding for people living with dementia cannot be achieved through procedural interventions alone. Rather, it depends on the capacity of systems and professionals to respond relationally, contextually, and reflexively (McHale & Noszlopy, 2025; Morrison, 2023).
Summary of Implications for Future Research, Policy, and Practice.
For practice, the review highlights the importance of embedding safeguarding within everyday care interactions rather than treating it as an episodic or crisis-driven activity. Health and social care professionals must be supported to engage in nuanced decision-making that balances risk with autonomy, particularly in cases involving fluctuating capacity or coercive dynamics. Inter-agency working should be underpinned by shared accountability, routine data-sharing, and clearly defined roles (Tracy, 2024). Safeguarding training must move beyond compliance to include relational ethics, cultural competence, and legal literacy especially in applying the Mental Capacity Act and interpreting the Care Act’s principles in practice (Spreadbury & Hubbard Rachel, 2024; Squires et al., 2024). For example, promoting strength-based and person-centered safeguarding might involve regular reflective case reviews, mentorship for junior practitioners, and scenario-based training that integrates human rights and other relevant legislation into everyday decision-making.
For policy, the findings point to the limitations of current safeguarding frameworks that rely heavily on formal reporting thresholds and underplay structural inequalities. Policy interventions must attend to the differential risks faced by people from minority and marginalized communities, and ensure that safeguarding systems are culturally responsive and inclusive (Hafford-Letchfield & Cocker, 2024). Investment in advocacy services, particularly for those lacking capacity or familial support, is essential (Daniels, 2025). Furthermore, mechanisms for oversight such as CQC inspections and SABs must be resourced to identify not only institutional failings but also subtler forms of neglect and harm that are often normalized within care contexts.
For research, the review identifies significant gaps in the evidence base, particularly around intersectionality, lived experience, and the contextual dynamics of safeguarding decision-making. These gaps are consistent with findings from previous reviews in the wider vulnerable adults population, which have similarly highlighted a lack of attention to how structural inequalities, such as poverty, race, and gender, shape vulnerability and influence safeguarding responses (Braye et al., 2015; Preston-Shoot, 2017). In the context of dementia specifically, earlier reviews have tended to focus more narrowly on clinical risk and capacity, with less emphasis on the social and relational dimensions of safeguarding (Cooper & Livingston, 2014).
Future studies need to adopt longitudinal and ethnographic approaches to examine how safeguarding unfolds over time, how it is interpreted by different actors, and how structural factors such as poverty, race, and gender intersect with vulnerability (Morrison, 2023; Mwale et al., 2025). There is also a need for evaluative research into integrated safeguarding models, including the role of the voluntary and community sector, and studies that assess the real-world application of legal frameworks such as the MCA, DoLS, and CRPD. Co-produced research, involving people living with dementia and carers as partners, will be crucial in designing safeguarding approaches that are both effective and rights-affirming (Gaffy et al., 2022).
Strengths and Limitations
The inclusion of CMO configurations facilitated a layered analysis that moves beyond descriptive accounts and discusses the causal pathways influencing safeguarding practices. The review did not treat safeguarding as a linear process but instead accounted for how outcomes vary across settings, systems, professional roles, and individual experiences. The review attempted to identify and address gaps in diversity, intersectionality, and culturally responsive safeguarding areas often marginalized in dementia research. Extensive engagement with people living with dementia, family carers, practitioners, and community representatives (across anonymized) grounded the review in real-world experiences and ensured diverse perspectives were represented. The findings and theories have practical relevance for designing and improving safeguarding interventions, training, and policy development tailored to the dementia care context.
The existing literature remains limited in its empirical engagement with under-represented groups, limiting the depth of analysis in relation to race, gender, sexuality, and class. However, our review sought to address this by actively involving people from diverse backgrounds through our PPIE group and community groups across (anonymized). Secondly, the reliance on published studies means that innovative or promising practices that remain undocumented in the grey literature may have been missed. Thirdly, the absence of uniform definitions and outcome measures across studies poses a challenge to generalizability. While realist synthesis accepts heterogeneity, it also relies on interpretive judgement, which may reflect the researcher positionality and epistemic assumptions. Finally, the review is explicitly focused on England, where safeguarding is governed by the Care Act 2014. While this ensures policy and practice relevance within the English context, it may limit the generalizability of findings to other parts of the United Kingdom or international settings. However, the core conceptual challenges, such as how safeguarding is conceptualized, operationalized, and experienced in decision-making extend beyond the English context. These challenges are pertinent to broader safeguarding contexts and may offer transferable insights for comparative and international discourse on adult safeguarding.
Conclusion
Safeguarding for people living with dementia is not a uniform or purely procedural process. It is shaped by context, relational dynamics, and the capacity of professionals and systems to navigate complexity with sensitivity and skill. While legal and organizational frameworks provide the necessary structure, effective safeguarding ultimately depends on the quality of interactions between individuals, professionals, and institutions. Mechanisms such as trust, clear communication, legal literacy, and shared accountability are most impactful when situated within well-resourced and coordinated environments. Conversely, when systems are fragmented, underfunded, or overly driven by compliance, these mechanisms often fail to activate, undermining safeguarding efforts.
The review also highlights that current safeguarding practices may insufficiently address the needs of diverse populations, reflecting a broader lack of attention to ethnicity, socioeconomic status, and cultural context. Without an intersectional and person-centered approach, safeguarding risks are inconsistently applied and, at times, structurally exclusionary.
Addressing these challenges requires a shift toward values-based, relational safeguarding, an approach that centers dignity, autonomy, and cultural responsiveness. This must go beyond inter-agency cooperation to include sustained investment in training, stronger cross-sector integration, and a commitment to co-producing strategies with people living with dementia and those who support them.
Future research needs to focus on how safeguarding is experienced across diverse contexts and identities, examining the conditions under which inclusive, rights-based approaches can be meaningfully embedded in everyday practice. Prioritizing equity and the voices of those most affected is essential to ensure that safeguarding does not become, however unintentionally, a source of exclusion or harm.
Supplemental Material
sj-docx-1-tva-10.1177_15248380251375488 – Supplemental material for Understanding Safeguarding for People Living with Dementia: A Realist Review of Conceptualization and Practice
Supplemental material, sj-docx-1-tva-10.1177_15248380251375488 for Understanding Safeguarding for People Living with Dementia: A Realist Review of Conceptualization and Practice by Reena Lasrado, Katarzyna Szulewska, Jeremy Dixon, Asri Maharani, Catherine Robinson, Mark Cooper, Maria Panagioti and Thomas Blakeman in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-2-tva-10.1177_15248380251375488 – Supplemental material for Understanding Safeguarding for People Living with Dementia: A Realist Review of Conceptualization and Practice
Supplemental material, sj-docx-2-tva-10.1177_15248380251375488 for Understanding Safeguarding for People Living with Dementia: A Realist Review of Conceptualization and Practice by Reena Lasrado, Katarzyna Szulewska, Jeremy Dixon, Asri Maharani, Catherine Robinson, Mark Cooper, Maria Panagioti and Thomas Blakeman in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-3-tva-10.1177_15248380251375488 – Supplemental material for Understanding Safeguarding for People Living with Dementia: A Realist Review of Conceptualization and Practice
Supplemental material, sj-docx-3-tva-10.1177_15248380251375488 for Understanding Safeguarding for People Living with Dementia: A Realist Review of Conceptualization and Practice by Reena Lasrado, Katarzyna Szulewska, Jeremy Dixon, Asri Maharani, Catherine Robinson, Mark Cooper, Maria Panagioti and Thomas Blakeman in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
We thank the PPIE members and the health and social care professionals who contributed their expertise at various stages of this review. Their insights were critical to the development and refinement of the program theories and the interpretation of findings. We thank Dr Justin Jagosh for his expert methodological guidance during the consultation sessions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute for Health and Care Research (NIHR) School for Social Care Research (Ref: 102645/3SDRP/UMRL-DP09). The views expressed in this paper are those of the authors and are not necessarily those of the NIHR or the Department of Health and Social Care.
Ethical Approval and Informed Consent Statements
The realist review did not require ethical approval, however, the phase 3 (qualitative phase) of the overall project was approved by the HRA and Health and Care Research Wales (HCRW) committee (REC reference: 23/LO/0177).
Members of various stakeholder groups, including PPIE representatives, community organizations, and health and social care professionals participated voluntarily in a consultative capacity.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.