
Abstract
Although many survivors of intimate partner violence (IPV) seek psychotherapy or counseling, providers often lack consistent training in serving this population, leading to variable—and at times harmful—experiences for survivor-clients. A review of existing research is necessary to better understand the perspectives of psychotherapy and counseling professionals working with this population. This scoping review examines qualitative studies focused on the experiences of providers working with adult IPV survivors in individual therapy. Following the Joanna Briggs Institute methodology for scoping reviews and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines for scoping reviews, 21 studies were identified as meeting the inclusion criteria for this review (i.e., qualitative studies with samples of psychotherapy or counseling providers who serve adult IPV survivors). These studies reveal significant personal challenges for providers, alongside limited training, education, and supervision. Providers demonstrated varying conceptualizations of IPV, employed diverse interventions, and described the influence of cultural, identity-related, and structural factors on their work. Many providers felt that systemic and societal barriers impacted their ability to effectively serve survivors. Findings indicate the need for comprehensive training, supervision, and resources to support providers in their work with IPV survivors. Yet, as IPV is rooted in structural inequities, individual-level interventions, while important, are not sufficient to address this social problem.
Intimate partner violence (IPV)—which includes physical violence, sexual violence, stalking, psychological aggression, and economic abuse by a current or former intimate partner—affects nearly one in three women globally (World Health Organization, 2021). Gender and sexual minority adults experience IPV at even higher rates than their cisgender, heterosexual counterparts (Porsch et al., 2023). IPV has severe physical, psychological, social, and economic consequences (World Health Organization, 2021) and increases the risk of mental health issues such as post-traumatic stress disorder, depression, suicidality, and self-harm (Lohmann et al., 2024). Many survivors seek psychotherapy to cope with these effects (Barrett et al., 2020; Tutty, 2024), and when they do, they may encounter responses from providers that range from harmful to healing (Tutty, 2024). As literature continues to capture diverse provider perspectives, there is a need to summarize this research to better understand the experiences of psychotherapy providers who work with IPV survivors. This scoping review examines existing qualitative studies on providers’ experiences offering psychotherapy or counseling to adult IPV survivors and aims to highlight challenges and best practices for addressing IPV in therapeutic settings.
Psychotherapy and Intimate Partner Violence
Historically, interventions for IPV have been delivered outside of mental health systems, often by domestic violence advocacy or victim services providers. Survivors in these settings may receive support from advocates who promote empowerment-based advocacy, which has been linked to improved well-being (Trabold et al., 2020). However, many survivors also seek psychotherapy to address the mental health impacts of abuse in addition to or instead of domestic violence agency support services. Psychotherapy aims to improve functioning, increase well-being, and offer healing. Given the psychological harm associated with IPV, psychotherapy can play a crucial role for survivors. Although help-seeking varies, a significant minority of survivors seek mental health services. For instance, a Canadian survey found that 32% of women who experienced IPV sought services from a counselor or psychologist (Barrett et al., 2020).
As a potential resource for recovery, psychotherapy offers pathways to healing from abuse through evidence-based interventions such as empowerment-focused, trauma-informed, cognitive-behavioral, and feminist therapies (Arroyo et al., 2017; Iverson et al., 2022; Trabold et al., 2020). Tailored approaches that emphasize safety, coping, social support, and empowerment have yielded improvements in self-efficacy and empowerment as well as reductions in depression for survivors (Iverson et al., 2022). Despite the effectiveness of these interventions, many providers are ill-prepared to work with IPV survivors (Sutton et al., 2021). Training on IPV is inconsistent or absent in many mental health programs (Sutton et al., 2021). The World Health Organization (WHO) offers guidelines for healthcare practitioners on screening, identifying, and providing care to survivors, but in a study across 24 countries, only half of mental health professionals reported receiving IPV training and most lacked comprehensive knowledge of WHO guidelines (Burns et al., 2020).
Understanding psychotherapy providers’ perspectives on addressing IPV is critical to improving training and care. Qualitative research has begun to explore providers’ experiences, challenges, and readiness to support survivors (Wilson et al., 2018, 2021). However, no review has synthesized themes across these studies. This review aims to summarize the perceptions, attitudes, barriers, and needs of practitioners who work with IPV survivors.
Methods
In accordance with the Joanna Briggs Institute (JBI) methodology for scoping reviews (Peters et al., 2020) and the extended version of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for scoping reviews (Tricco et al., 2018), our preregistered protocol (Gutowski et al., 2023) involved six steps: (a) defining the research question, (b) identifying relevant studies, (c) study selection, (d) charting the data, (e) collating, summarizing, and reporting the results, and (f) consultation (Levac et al., 2010). Per the JBI recommendations, our review process was iterative, allowing for amendments to protocols to be made at each stage to ensure that all relevant literature was captured.
Defining the Research Question
We sought to address the question: “What are the experiences of professionals who provide individual psychotherapy and/or counseling working with adult intimate partner violence (IPV) survivors?” We aimed to summarize qualitative literature on the subjective experiences of mental health professionals providing psychotherapy/counseling to survivors of IPV.
Identifying Relevant Studies
Search Strategy
We used a three-step strategy to identify qualitative studies addressing mental health practitioner experiences providing individual psychotherapy and/or counseling to adult IPV survivors published between 2008 and 2023 (Peters et al., 2020). First, we conducted a limited search of the literature using ProQuest and Google Scholar to identify articles relevant to our research question(s) and to build a list of initial search terms. Search terms were developed to target three main concepts: the clinical concern, the population, and the content of interest (i.e., IPV, mental health service providers, and their perceptions). These terms were provided to a social sciences librarian (the sixth author) along with a test set of nine articles. Second, using this test set of articles, the librarian further refined the search strategy. The pilot search strategy was developed in PsycINFO (Ovid interface) and, in accordance with the Peer Review of Electronic Search Strategies (PRESS) framework, was peer-reviewed by a second librarian (not on the research team) (see Appendix). Following its PRESS review, this search strategy was translated into the following nine databases: PsycINFO (Ovid), MEDLINE (Ovid), Embase (Ovid), CINAHL (EBSCO), Scopus, Sociological Abstracts (ProQuest), International Bibliography of Social Sciences (ProQuest), Social Work Abstracts (Ovid), and Cochrane Library. This retrieved 2412 results. Duplicates were removed using Zotero citation management software leaving 1250 unique results. In the third step, we employed the ascendancy approach, examining sources cited in our included studies to locate additional works that met inclusion criteria.
Inclusion and Exclusion Criteria
Our review included qualitative or mixed methods studies with participants who provided individual psychotherapy and/or counseling to adults (i.e., persons over 18 years of age) with marginalized gender and/or sexual identities (i.e., cisgender women, sexual, and/or gender minority-identified) who have previous or current experience with IPV victimization. Manuscripts investigating the experiences of mental health providers exclusively treating perpetrators of IPV (including couples’ counseling) were excluded, as intervention with this population presents a unique set of considerations falling outside the scope of this review. Moreover, articles that did not have a clear focus on IPV and instead emphasized other types of abuse or abuse in general were excluded. Professions of participants included psychotherapists, counselors, psychologists, social workers, and/or clinicians working in mental healthcare and community settings. We did not include articles with mixed providers (e.g., police, physicians, nurses, and psychologists) as this review exclusively focused on the provision of psychotherapy and/or counseling. This led us to exclude some articles that described professionals’ experiences providing psychotherapy and/or counseling but in addition to therapists and counselors included nurses or other medical, social service, and/or legal professionals. Further, we did not include articles that used a general term (e.g., health service providers) when the authors did not clarify the credentials or roles of the participants. Articles with samples of social workers in mixed settings who were not clearly engaged in therapy and/or counseling were eliminated. The research foci of the included articles pertained to participants’ experiences providing psychotherapy and/or counseling (e.g., barriers, challenges, and strengths that could facilitate, impede, or otherwise influence therapeutic work with survivors). Articles that focused on other content (e.g., asking professionals to respond to case vignettes of IPV survivors instead of discussing their own clinical experiences) were excluded. We retained articles that asked professionals to discuss their conceptualizations of IPV as it relates to their clinical work and observations in the course of service provision, however. Only peer-reviewed articles available in English published after 2007 were included.
Study Selection
After removing duplicates, we screened the remaining 1250 articles that met search criteria using Rayyan, a reference manager and literature review software. First, titles and abstracts of all articles were screened by two blind, independent reviewers (the third and fourth authors) for assessment against inclusion criteria. We discussed any disagreements about eligibility in weekly team meetings with the first author serving as an auditor and the second author as a consultant. Any texts for which disagreements between reviewers remained unresolved were included for full-text review. This process resulted in 196 articles that we screened for full-text review. Three screeners (the third and fifth authors plus one research assistant) each reviewed a subset of the articles and the first author served as an auditor, reviewing the final set of articles in consultation with the second author. This process resulted in 19 articles for inclusion in this review. Finally, using the ascendancy approach to examine the reference lists of each of the included articles, we added two articles that met inclusion criteria, resulting in a final set of 21 articles (see Figure 1).
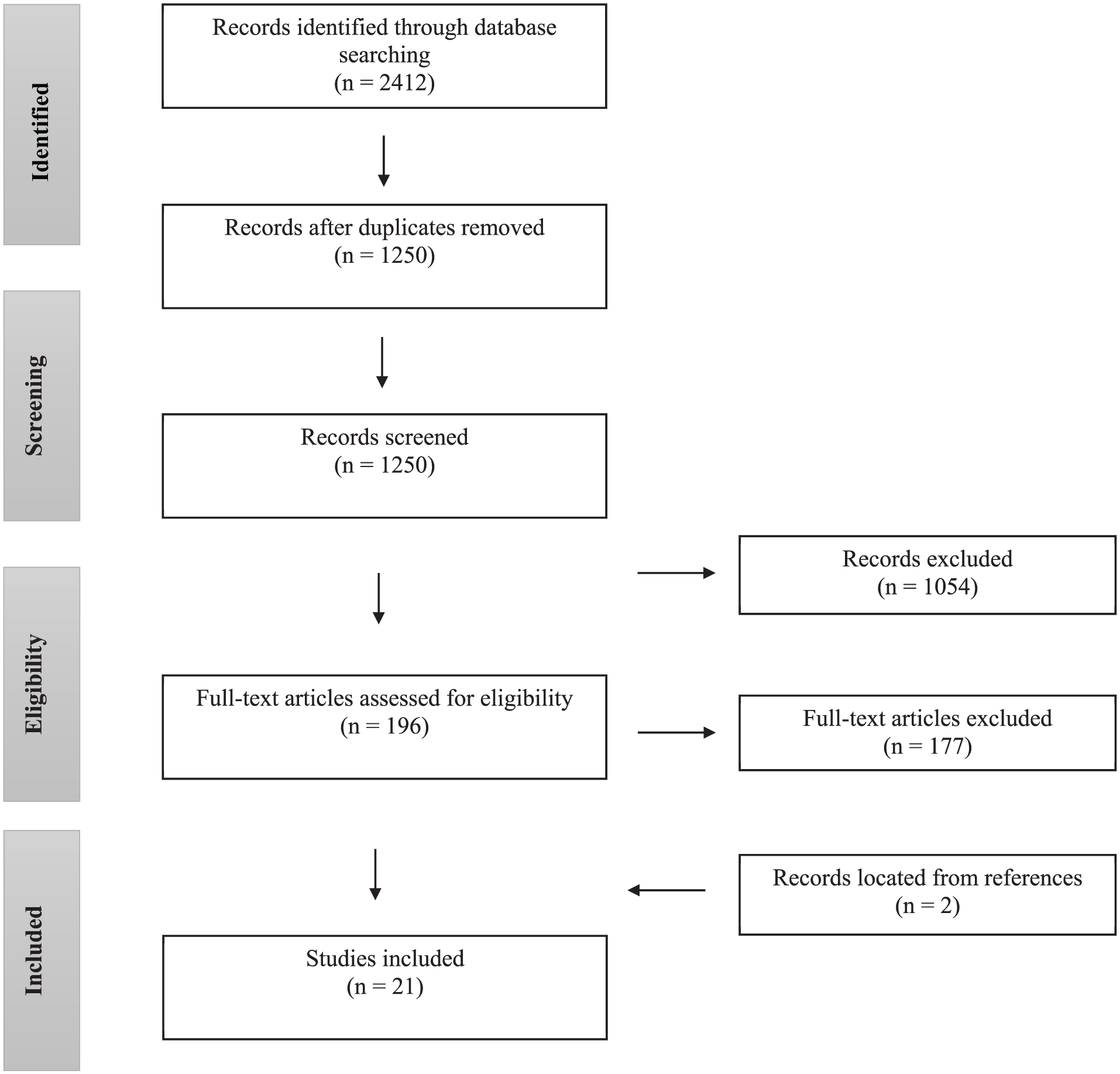
Study selection.
Charting the Data
Data Extraction
Two reviewers were involved in the data extraction process. Information from identified studies was extracted using a custom-designed form that included: general article information (e.g., author; year of publication; location; study aims); methodology (e.g., sample size; sampling method, study design; analytic approach); and findings (e.g., professional experiences working with IPV—barriers, strengths, etc.). Prior to extraction, a quality control training procedure was conducted using the form. Each reviewer independently extracted data from at least one article, and results were reviewed at team meetings and discussed to provide further guidance. Remaining studies were then distributed for data extraction. The extraction form was revised with ongoing discussion and review as several prominent themes surfaced during the extraction process. Finally, the first author audited all extraction forms, consulting with the second author.
Collating, Summarizing, and Reporting the Results
Conventional qualitative content analysis was used to analyze the included studies, as this approach is useful when existing research is limited (Hsieh & Shannon, 2005). The research team developed a codebook for this qualitative analysis. Per constant comparison methodology, this codebook evolved during the data analysis process, conducted in NVivo software.
Assessing Quality
We assessed quality using the Critical Appraisal Skills Programme (CASP, 2018) Checklist for assessing qualitative research. Similar to other scoping reviews of qualitative research using this quality assessment method (e.g., O’Dwyer et al., 2021), we assigned a score to articles by summing items on the CASP. Nine CASP items have numeric values that denoted whether an indicator of quality was present (i.e., 2 = “yes”; 1 = “don’t know”; and 0 = “no”). Total scores could range from 0 to 18. Scores above 13 indicated high quality, whereas a score below 6 represented low quality (CASP, 2018). Articles were scored by the third and fifth authors plus a research assistant and the first author audited all scoring.
Consultation
Members of our team include researcher-clinicians and students with research experience in the area of IPV and mental health. Three team members have worked extensively with survivors and have experience providing psychotherapy. The first and second authors teach and train mental health professionals who provide psychotherapy. Thus, members of the research team have experience with clinical dilemmas faced by the population of interest in this study.
Results
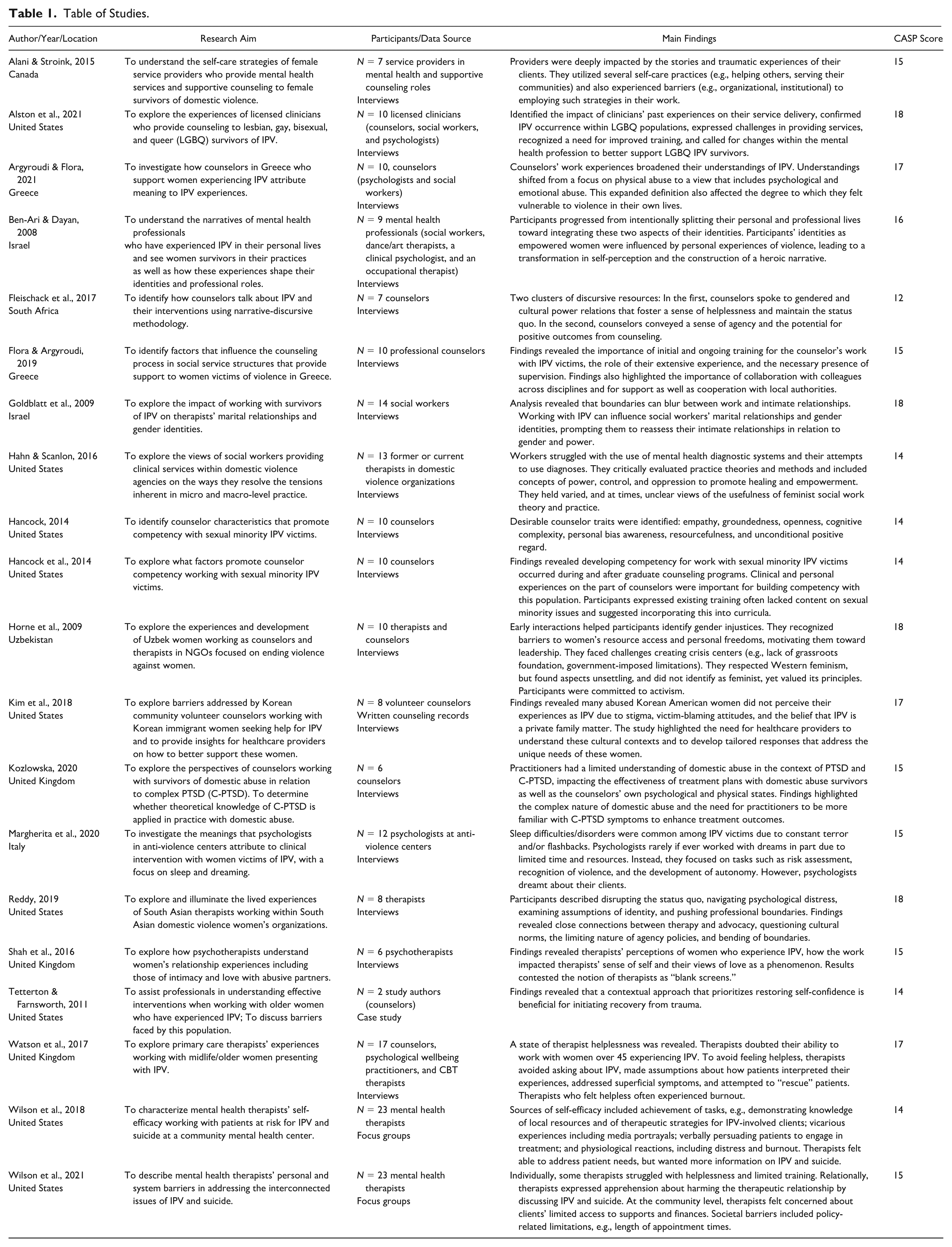
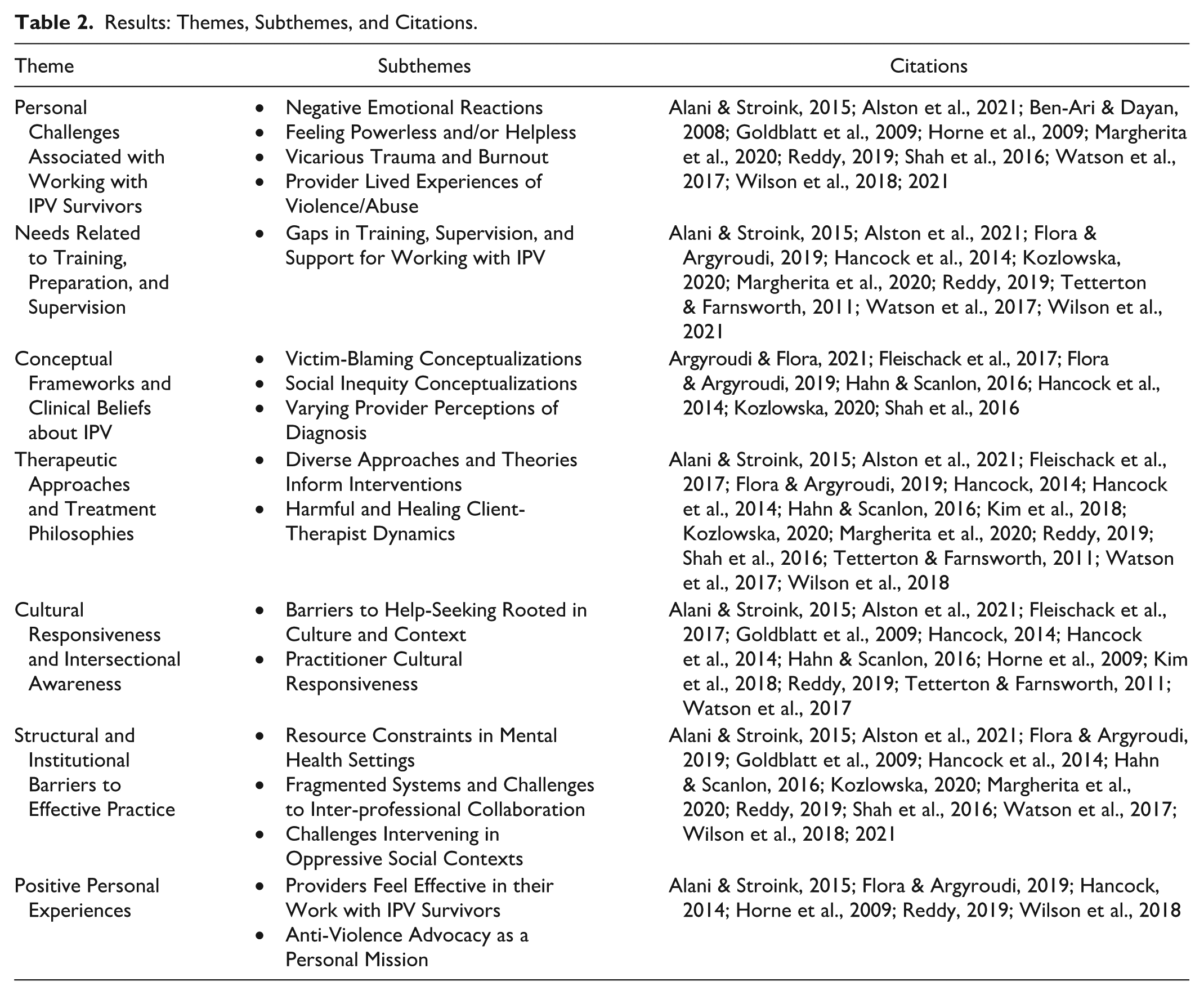
Of the 21 included articles, three described providers’ experiences working with sexual minority survivors and 18 focused on women survivors. Studies were based in the United States (n = 8), the United Kingdom (n = 5), Israel (n = 3), Greece (n = 2), Canada (n = 1), Italy (n = 1), South Africa (n = 1), and Uzbekistan (n = 1). Eighteen used data based on interviews, two on focus groups, and one on case study. Quality assessment ratings ranged from 12 (medium) to 18 (high) (CASP, 2018) and thus no studies were eliminated based on quality. To analyze the qualitative data, studies used phenomenological approaches (i.e., interpretive phenomenological analysis; other phenomenological methods) (n = 6), thematic analysis (n = 4), grounded theory (n = 4), narrative approaches (i.e., narrative analysis; narrative discursive) (n = 2), content analysis (n = 2), interpretive description (n = 1), and qualitative framework approach (n = 1). One study did not name a specific qualitative analysis method, though drew from community-based participatory research (see Table 1). The included studies covered several major themes including psychotherapy and counseling providers’ (a) personal challenges associated with working with IPV survivors; (b) needs related to training, preparation, and supervision; (c) conceptual frameworks and clinical beliefs about IPV; (d) therapeutic approaches and treatment philosophies; (e) cultural responsiveness and intersectional awareness; (f) structural and institutional barriers to effective practice; and (g) positive personal experiences of the work. See Table 2 for themes, subthemes, and relevant citations.
Table of Studies.
Results: Themes, Subthemes, and Citations.
Personal Challenges Associated with Working with IPV Survivors
Studies illuminated the challenges of working with IPV survivors for professionals providing psychotherapy or counseling, which included negative emotional reactions; feelings of powerlessness and/or helplessness; burnout and vicarious trauma; as well as the activation of thoughts, emotions, and memories related to one’s personal experiences of abuse. See Table 2.
Negative Emotional Reactions
Providers described negative emotional reactions that arose during the therapeutic work such as frustration, anger, fear, worry, shame, and/or overwhelm (Alani & Stroink, 2015; Ben-Ari & Dayan, 2008; Goldblatt et al., 2009; Margherita et al., 2020; Reddy, 2019; Watson et al., 2017; Wilson et al., 2018; 2021). Providers attributed emotional reactions to experiences such as clients not following through on referrals, not returning to therapy, and/or staying in abusive relationships (Watson et al., 2017; Wilson et al., 2018). Negative emotions surfaced when providers encountered barriers such as a lack of time/resources to do their work effectively (e.g., Alani & Stroink, 2015). They described concern for clients’ safety and questioned their competence as therapists and/or the effectiveness of therapy as an intervention for IPV (e.g., Watson et al., 2017).
Feeling Powerless and/or Helpless
Ultimately, many described feeling powerless and relayed the sense that there was only so much they could do for their clients (e.g., Watson et al., 2017). Some felt helpless in reaction to their clients’ experiences of IPV combined with racism or other forms of oppression and traumatic stress; expressed that their work was devalued due to societal prejudices against the population they served; were unable to foster client change due to systemic constraints; encountered a lack of available resources for the population served (i.e., LGBQ survivors); had few “success stories”; experienced pressure to meet unrealistic expectations with limited time; and/or viewed therapy as ineffective when clients were still in abusive relationships (Alani & Stroink, 2015; Alston et al., 2021; Margherita et al., 2020; Watson et al., 2017; Wilson et al., 2021). For many, feeling powerless was tied to a sense of incompetence (e.g., Watson et al., 2017).
Vicarious Trauma and Burnout
Providers described the intensity of the traumatic content to which they were exposed through their work and “taking the work home” when thoughts, images, or memories stayed with them after an encounter (e.g., Alani & Stroink, 2015). For some, the intensity of the work and related stress undermined well-being and accompanied a sense of burnout and vicarious trauma (e.g., Goldblatt et al., 2009; Reddy, 2019). Burnout was associated with feelings of self-doubt, powerlessness, and lack of control over one’s work; perceptions that one has little to offer one’s clients; difficulties with self-care; stresses associated with severe and complex client situations; and limited opportunities to witness client progress (Alani & Stroink, 2015; Watson et al., 2017; Wilson et al., 2018; 2021). Many providers described vicarious trauma, which was associated with difficulties effectively working with clients (e.g., Shah et al., 2016). They reported somatic symptoms; intrusive and persistent thoughts of traumatic content; nightmares; hypervigilance and distrust; distress and despair; and difficulties with intimacy and relationships (Goldblatt et al., 2009; Reddy, 2019; Shah et al., 2016; Watson et al., 2017). Vicarious trauma was linked to self-doubt and helplessness (e.g., Watson et al., 2017). To cope, providers had to manage their well-being and engage in self-work (e.g., Alani & Stroink, 2015).
Provider Lived Experiences of Violence/Abuse
Studies discussed providers’ lived experiences with violence and/or abuse (e.g., Ben-Ari & Dayan, 2008). Such experiences motivated providers to engage in therapeutic work with IPV survivors; helped them empathize and connect with clients; informed them about abuse dynamics; and facilitated their personal healing through their work (Alani & Stroink, 2015; Ben-Ari & Dayan, 2008; Horne et al., 2009; Reddy, 2019). However, providers with personal IPV experiences also experienced vicarious trauma, and/or intense emotional reactions to the work, especially when they did not engage in self-work or were early in their processes of healing (e.g., Alani & Stroink, 2015; Reddy, 2019). Providers who had ongoing experiences of abuse while providing services to IPV survivors found it difficult to reconcile helping others who were seeking help for an experience that they faced themselves (Ben-Ari & Dayan, 2008). They reported that their work made them aware of abuse in their own and others’ relationships and vigilant about gender-based inequities (e.g., Goldblatt et al., 2009). Delineating boundaries between their own and their client’s experiences was challenging. When they were able to integrate their personal and professional lives, providers accessed supports and reflected on their emotional reactions to their work (e.g., Ben-Ari & Dayan, 2008). This process helped them become better therapists and develop empathy for their clients.
Needs Related to Training, Preparation, and Supervision
As working with survivors of IPV brought about challenges as well as intense emotions and reactions for psychotherapy and counseling providers, many providers highlighted the importance of training and supervision. See Table 2.
Gaps in Training, Supervision, and Support for Working with IPV
Providers noted a desire for more training on IPV for themselves and for other professionals performing similar work. Some providers indicated insufficient or no training in IPV prior to working with survivors (e.g., Watson et al., 2017). Relatedly, some noted a need for more support and supervision (Flora & Argyroudi, 2019). Many communicated a desire for more academic, on-the-job, and continuing education on working with IPV (e.g., Alston et al., 2021; Flora & Argyroudi, 2019; Hancock et al., 2014).
Providers suggested training cover topics including gender and IPV dynamics; IPV-related symptoms and occurrence; community resources for survivors; approaches for integrating understandings of cultural and contextual factors into one’s work; skills and direct practice-based training on how to effectively work with survivors including sexual and other minority survivors; as well as risk factors, resources, and case scenarios for addressing the intersection of IPV and suicide (Alani & Stroink, 2015; Alston et al., 2021; Flora & Argyroudi, 2019; Hancock et al., 2014; Kozlowska, 2020; Wilson et al., 2018). Some expressed concerns that professionals could retraumatize or judge IPV survivor-clients when not trained, that organizations did not have sufficient resources to devote to staff training, and that academic training neglected IPV and minority (especially LGBQ) survivors as topics or was overly theoretical (e.g., Alani & Stroink, 2015; Hancock et al., 2014). For some, insufficient training was associated with discomfort assessing for and working with IPV, a sense of helplessness and ineffectiveness, and/or a tendency to avoid the topic of IPV with clients (e.g., Wilson et al., 2018; 2021).
Conceptual Frameworks and Clinical Beliefs about IPV
Several articles spoke to providers’ diverse conceptual frameworks and clinical beliefs about IPV from victim-blaming conceptualizations to understandings of IPV as an issue rooted in social inequities. Relatedly, provider attitudes on the value of diagnosing mental health concerns among survivors of IPV were mixed: Some identified that a mental health diagnosis could be harmful to survivors, while others felt that a mental health diagnosis could facilitate appropriate treatment. See Table 2.
Victim-Blaming Conceptualizations
Providers relayed victim-blaming narratives that either they believed themselves or had heard from other professionals (e.g., Flora & Argyroudi, 2019). Providers revealed beliefs that survivors were responsible for and/or contributed to the abuse due to, for example, challenging their partner’s behavior, tolerating the abuse, getting stuck in these relationships, and/or having low self-esteem (e.g., Shah et al., 2016). Some rejected the existence of relational power differentials and indicated that both parties assume roles of both “victim” and “perpetrator” (Flora & Argyroudi, 2019).
Social Inequity Conceptualizations
In contrast to victim-blaming conceptualizations, some providers shared conceptualizations of IPV that acknowledge its social roots: For example, one provider emphasized IPV as a “social problem” that creates mental health difficulties instead of an individual-level mental health problem (Hahn & Scanlon, 2016). Providers emphasized patriarchy as a system that perpetuates IPV (e.g., Horne et al., 2009). Those serving heterosexual women discussed inequities perpetuated by social norms that disadvantage women, leaving them dependent on male partners and vulnerable to abuse (e.g., Fleischack et al., 2017). Providers serving sexual minority survivors indicated that a cycle of violence in which one partner exercises power and control over another is a core dynamic, similar across survivors regardless of sexual orientation (Hancock et al, 2014). Some also noted insidious trauma unique to lesbian, gay, bisexual, and queer (LGBQ) survivors due to their being part of a marginalized group (Alston et al., 2021).
Varying Provider Perceptions of Diagnosis
Provider perceptions of diagnosis were mixed: Some named disadvantages including the potential harm of receiving such a label for those who had been manipulated by abusive partners into believing there is something wrong with them; the possibility for misdiagnosis when practitioners do not have an understanding of trauma; and/or the chance that a diagnosis could be used against survivors in court (Hahn & Scanlon, 2016). Some viewed using a mental health diagnosis positively: Some providers felt that using the diagnosis of complex post-traumatic stress disorder (C-PTSD) could facilitate effective intervention; that naming symptoms could be validating; and that ignoring mental health diagnoses could lead to neglecting treatment needs (e.g., Kozlowska, 2020). Regardless of whether they diagnosed survivor-clients with a mental health condition or not, many providers spoke of the importance of identifying that trauma is experienced differently by different clients (e.g., Tetterton & Farnsworth, 2011). Many providers also emphasized client strengths and resilience to empower survivor-clients, help them develop autonomy, and reduce self-blame for the abuse (e.g., Tetterton & Farnsworth, 2011).
Therapeutic Approaches and Treatment Philosophies
Just as conceptual frameworks and clinical beliefs about IPV were diverse and inconsistent across providers, the interventions and approaches they used for IPV survivor-clients varied widely. Providers reported an array of theories that informed their work and approaches that ranged in the extent to which they were therapist-driven or client-driven. Ultimately, these mixed approaches likely had inconsistent outcomes: Some described client-therapist dynamics that prioritized a healing therapeutic alliance, while others described dynamics that were potentially harmful. See Table 2.
Diverse Approaches and Theories Inform Interventions
Among the assorted approaches that providers used in their work with IPV survivors, some made referrals, educated clients about their rights, told clients to leave their relationships, used suggestions and/or homework, or treated surface-level symptoms (i.e., anxiety) without addressing IPV (Alston et al., 2021; Fleischack et al., 2017; Watson et al., 2017; Wilson et al., 2018). In contrast, some described using relational, theoretically sophisticated interventions that acknowledge each client’s context (Hancock, 2014; Hahn & Scanlon, 2016; Kozlowska, 2020; Reddy, 2019; Tetterton & Farnsworth, 2011). Providers who used relational interventions noted the importance of engaging clients and tailoring the approach to the individual and their stage of recovery (e.g., Hahn & Scanlon, 2016). They felt that risk assessment, recognition of violence, crisis intervention, and/or safety planning may be essential to prioritize depending on risk. These providers expressed the importance of respecting survivors’ perceptions of risk while increasing supports and discussed the value of listening to clients’ stories compassionately without judgment (e.g., Kim et al., 2018).
A range of theories informed therapeutic work with survivor-clients, including feminist (Tetterton & Farnsworth, 2011), motivational interviewing (Wilson et al., 2018), cognitive (Hahn & Scanlon, 2016; Shah et al., 2016; Tetterton & Farnsworth, 2011), and integrative approaches (Hahn & Scanlon, 2016; Tetterton & Farnsworth, 2011). Providers helped clients with coping, emotion regulation, and assertiveness/communication skills (Tetterton & Farnsworth, 2011). Many noted the value of attention to macro-level factors that influenced the client—including potential exposure to ongoing abuse (e.g., Hancock et al., 2014). In one study, providers discussed the value of non-pathologizing models developed specifically for survivors that view returning to the abusive relationship as part of the healing process (Hahn & Scanlon, 2016). Some cautioned that failing to attend to macro-level considerations could send victim-blaming messages (e.g., that clients could address their concerns solely through changes in cognition) or create unrealistic expectations for the therapy (e.g., that clients should be able to complete homework when subjected to ongoing abuse) (Hahn & Scanlon, 2016). To holistically address client needs (e.g., legal, housing) beyond therapy, some providers described working as members of interdisciplinary teams, collaborating closely with other professionals, or sharing resources with clients (e.g., Wilson et al., 2018).
Harmful and Healing Client-Therapist Dynamics
Finally, a few studies spoke to therapist-client dynamics. Therapist-client dynamics were varied in the extent to which they accounted for context, pathologized the survivor, prioritized the therapy relationship, and ultimately had the potential to be harmful and/or healing. One study revealed potentially harmful dynamics that arose as providers disclosed exercising authority over clients (Shah et al., 2016). In two studies, providers broke regular boundaries of psychotherapy by providing more time to survivor-clients, working unpaid hours and on days off (Reddy, 2019; Watson et al., 2017). In one study, providers serving sexual minorities emphasized showing they care, conveying empathy for clients’ experiences as sexual minorities, having compassion for trauma, staying grounded, being open-minded and honest, resisting urges to “fix,” applying new learnings, monitoring bias, and expressing unconditional positive regard (Hancock, 2014).
Cultural Responsiveness and Intersectional Awareness
Providers described cultural, identity-related, and contextual factors that influenced their work with survivors. Some discussed the role of these factors in IPV dynamics and occurrence. See Table 2.
Barriers to Help-Seeking Rooted in Culture and Context
Several studies discussed IPV as rooted in systems of oppression (e.g., Alani & Stroink, 2015) and influenced by cultural norms (e.g., Horne et al., 2009). Providers working in Uzbekistan described how early marriage for girls created power imbalances and providers in both Uzbekistan and South Africa described women’s financial dependency in their marriages, which made it hard to divorce and put them at risk for abuse (Fleischack et al., 2017; Horne et al., 2009). Those serving sexual minority survivors spoke of the high occurrence of IPV (Alston et al., 2021). Providers discussed intersectional concerns of survivors in addition to IPV which included poverty, housing instability, and physical and mental health challenges (Alani & Stroink, 2015). Providers expressed that cultural, identity-related, and contextual factors played a role in the process of seeking professional help for IPV. In one study, they articulated the stigma attached to both IPV and divorce for Korean American women which, in combination with racism, discrimination, and lack of familiarity with U.S. systems, made it difficult to seek help (Kim et al., 2018). In another, South African providers spoke of views of counseling as a “last resort” within traditional African culture (Fleischack et al., 2017). Providers serving sexual minority clients described these clients’ potential negative experiences within systems (e.g., legal, healthcare) and subsequent hesitation to trust providers (Alston et al., 2021; Hancock et al., 2014). Providers also spoke of discrimination clients faced based on sexual orientation, ethnicity, mental health/addiction concerns, and/or victimization experiences, which could lead to being denied services (e.g., Alani & Stroink, 2015; Alston et al., 2021). Providers serving sexual minority survivors discussed client barriers to making progress due to insidious trauma, IPV experiences, and limited resources for LGBQ survivors (Alston et al., 2021).
Practitioner Cultural Responsiveness
Providers described varying degrees of responsiveness to clients’ culturally significant experiences, worldviews, and identities. In one study, providers who served women survivors over 45 without adequate training made assumptions about their clients and based their treatment plans off of uncorroborated evaluations (Watson et al., 2017). In contrast, providers who worked with sexual minority survivors emphasized the importance of attending to intersectional identities and being knowledgeable about common experiences among sexual minority survivors (e.g., lack of family support, not being out to family, and/or friends taking the place of biological family) (Alston et al., 2021; Hancock, 2014; Hancock et al., 2014). In other studies, providers emphasized not making assumptions based on client identities, being receptive to each client’s views and experiences, and respecting differences (e.g., Reddy, 2019). Providers emphasized the value of personal reflection and bias awareness to prevent harm. Even when they shared identities with clients, providers aspired to remain humble and open to their client’s experiences.
Providers also modified psychotherapy practices to respond to their client’s cultural identities. In one study, South Asian therapists described how sharing the same ethnicities as their South Asian survivor-clients contributed positively to the therapy as they possessed a deep familiarity with their clients’ cultural norms and values (Reddy, 2019). These therapists developed close, familial relationships with clients and took actions (e.g., offering tea and cookies prior to sessions; staying in touch after termination) that they deemed culturally responsive (Reddy, 2019). Yet, these therapists worked overtime without pay as it was not possible to build such relationships within the limited time allotted for sessions (Reddy, 2019). Another study of providers in Canada who served Indigenous survivors described wanting to engage in cultural practices with clients such as smudging and sharing meals; however, such actions were against agency policies (Alani & Stroink, 2015). Providers illuminated heterosexist and Eurocentric biases within mainstream psychotherapy (Alani & Stroink, 2015; Alston et al., 2021; Reddy, 2019). They discussed how training, supervision, and practice neglected sexual minority survivors’ needs and professional norms often did not embrace cultural practices and views.
Structural and Institutional Barriers to Effective Practice
Studies discussed structural and institutional barriers to effectively serving IPV survivors. These included resource constraints, fragmented systems, and oppressive contexts. See Table 2.
Resource Constraints in Mental Health Settings
Among the barriers to practice identified by providers, the most significant was a lack of resources to effectively serve survivor-clients (e.g., Margherita et al., 2020). Providers discussed challenging session and time limits, disruptive staff shortages and turnover, as well as insufficient practical resources (i.e., stationery, heating, and meeting space) (Alani & Stroink, 2015; Flora & Argyroudi, 2019; Hahn & Scanlon, 2016; Margherita et al., 2020; Reddy, 2019; Watson et al., 2017; Wilson et al., 2018, 2021). Some felt that they did not have the resources to offer quality services, such as in-depth, long-term, relational work beyond crisis, or immediate support which was often reserved for the most severe cases (e.g., Margherita et al., 2020). They expressed broad criticisms of how funding was allocated and some felt societal minimization of violence and an overall failure to take IPV seriously contributed to resource deficits (e.g., Kozlowska, 2020). They indicated limited affordable interventions, insufficient prevention or reintegration initiatives, and short-term funding that ends right as clients develop trust, leading to further mistrust of systems for client as well as employment precarity for providers (Alani & Stroink, 2015; Flora & Argyroudi, 2019; Wilson et al., 2021).
Fragmented Systems and Challenges to Inter-professional Collaboration
Providers discussed difficulties with cross-provider and cross-discipline collaboration: They shared that their attempts to communicate with other providers, such as medical professionals, would not be reciprocated or their referrals to the police or social care would be turned away due to not meeting thresholds for severity (Watson et al., 2017; Wilson et al., 2018). Some reported that provider turnover posed barriers to inter-professional collaboration (Wilson et al., 2018). Providers noted a general lack of familiarity with outside agencies and difficulties assisting their clients with referrals (e.g., Wilson et al., 2021). Many felt that there were limited community resources available to their clients, especially LGBQ clients (e.g., Alston et al., 2021; Hancock, 2014). Some described receiving referrals to short-term services from providers who did not assess for IPV which made the task of responding overwhelming (Watson et al., 2017). Difficulties with cross-discipline collaboration were problematic, as due to the complexity of IPV, therapy work alone was often not sufficient to address survivors’ needs (e.g., Alani & Stroink, 2015).
Challenges Intervening in Oppressive Social Contexts
Social contexts that uphold systems of oppression such as patriarchy, White supremacy, and heterosexism limited provider effectiveness, perpetuated violence, and posed challenges for survivors seeking help. Some providers in Canada expressed frustration that men were not held accountable for violence (Alani & Stroink, 2015). Providers serving Korean immigrant women indicated that clients would tolerate IPV because of the patriarchal norms to which they were exposed (Kim et al., 2018). Providers in South Africa spoke of norms of men disciplining their wives (Fleischack et al., 2017). Systems of oppression also directly influenced providers’ work lives: Uzbek women counselors spoke about patriarchal notions that women should not work outside the home, interfering with their work in the gender-based violence sector (Horne et al., 2009). Some had to stand up for their right to work or hide it from family.
To address structural barriers, some providers engaged in advocacy and other initiatives to foster change. Women counselors in Uzbekistan spoke of creating crisis centers in response to the rise in rapes in the country (Horne et al., 2009). Mental health service providers in Canada spoke of contributing to their communities as a form of self-care such as by organizing clothing drives (Alani & Stroink, 2015). Clinical social workers in the United States described educating medical professionals on trauma and on the harms of misdiagnosis (Hahn & Scanlon, 2016). South Asian clinicians in the United States engaged in outreach within South Asian communities (Reddy, 2019).
Positive Personal Experiences
Studies revealed that even many providers who disclosed challenges associated with their work also spoke of their work as fueling a sense of passion, purpose, and efficacy. See Table 2.
Providers Feel Effective in their Work with IPV Survivors
Providers described sources of self-efficacy including mastery of local resources and knowledge of therapeutic strategies for IPV survivors (e.g., Wilson et al., 2018). Providers described their work settings as places where they could realize their potential and share their strengths, which engendered hope (e.g., Horne et al., 2009). For example, one provider expressed that she has a way of letting clients know she cares (Hancock, 2014).
Anti-Violence Advocacy as a Personal Mission
Some felt that advocating for women’s rights was a personal mission and many spoke of the sense of fulfillment they gained (e.g., Alani & Stroink, 2015). Providers described their work as important and expressed the powerful nature of engaging in therapeutic relationships with clients (e.g., Flora & Argyroudi, 2019). They spoke of their stance as activists against gender-based violence in their communities and their fight against misogyny and sexism (e.g., Reddy, 2019).
Discussion
This scoping review included 21 qualitative studies that investigated the experiences of psychotherapy and counseling providers who work with survivors of IPV. The findings reveal several important themes. First, while many providers found purpose and passion in their work, they also reported significant challenges such as emotional distress, burnout, and vicarious trauma (Alani & Stroink, 2015; Alston et al., 2021; Ben-Ari & Dayan, 2008; Goldblatt et al., 2009; Horne et al., 2009; Margherita et al., 2020; Reddy, 2019; Watson et al., 2017; Wilson et al., 2018, 2021). Often these challenges were due to the intensity of the trauma brought into therapy by IPV survivors. Many providers were left feeling overwhelmed and unsupported in their roles, particularly when supports like supervision and training were lacking (Alani & Stroink, 2015; Watson et al., 2017).
Second, the findings of this review uncover significant variability in the preparedness and approaches of psychotherapy providers working with IPV survivors. Some professionals recognized IPV as a structural issue rooted in power imbalances and oppression (Alston et al., 2021; Argyroudi & Flora, 2021; Flora & Argyroudi, 2019; Hahn & Scanlon, 2016). Many also engaged in interdisciplinary collaboration to meet survivor-clients’ needs (Flora & Argyroudi, 2019; Margherita et al., 2020). This informed perspective aligns therapeutic interventions with survivors’ lived experiences and acknowledges intersecting forms of oppression that influence their trauma. Others held harmful, victim-blaming views that perpetuate societal myths about abuse (Fleischack et al., 2017; Kozlowska, 2020; Shah et al., 2016). Such misconceptions can lead to interventions that do not address survivors’ needs or retraumatize them.
Third, providers articulated a clear need for consistent IPV education and training. Many providers expressed a lack of confidence in their ability to assess and address the complexities of IPV, citing insufficient training and supervision as key issues (Alani & Stroink, 2015; Alston et al., 2021; Flora & Argyroudi, 2019; Hancock et al., 2014; Kozlowska, 2020; Watson et al., 2017; Wilson et al., 2018, 2021). Given the high prevalence of IPV and its profound mental health impacts (Lohmann et al., 2024), this lack of preparedness is troubling. Without adequate training, providers may cause harm—by, for example, downplaying survivors’ experiences or failing to recognize ongoing abuse.
Fourth, the value of cultural responsiveness and intersectional awareness was key across studies. Providers serving marginalized populations, including LGBQ survivors, emphasized the unique challenges faced by their clients, which were compounded by oppression and insidious trauma (Alston et al., 2021; Hancock et al., 2014). Providers highlighted the importance of culturally responsive care and tailored their interventions to the unique cultural and contextual needs of each survivor (Alston et al., 2021; Hancock, 2014; Hancock et al., 2014; Reddy, 2019). Yet, many felt that training for work with marginalized survivors was inadequate and/or had little institutional support for this work (Alani & Stroink, 2015; Alston et al., 2021; Reddy, 2019).
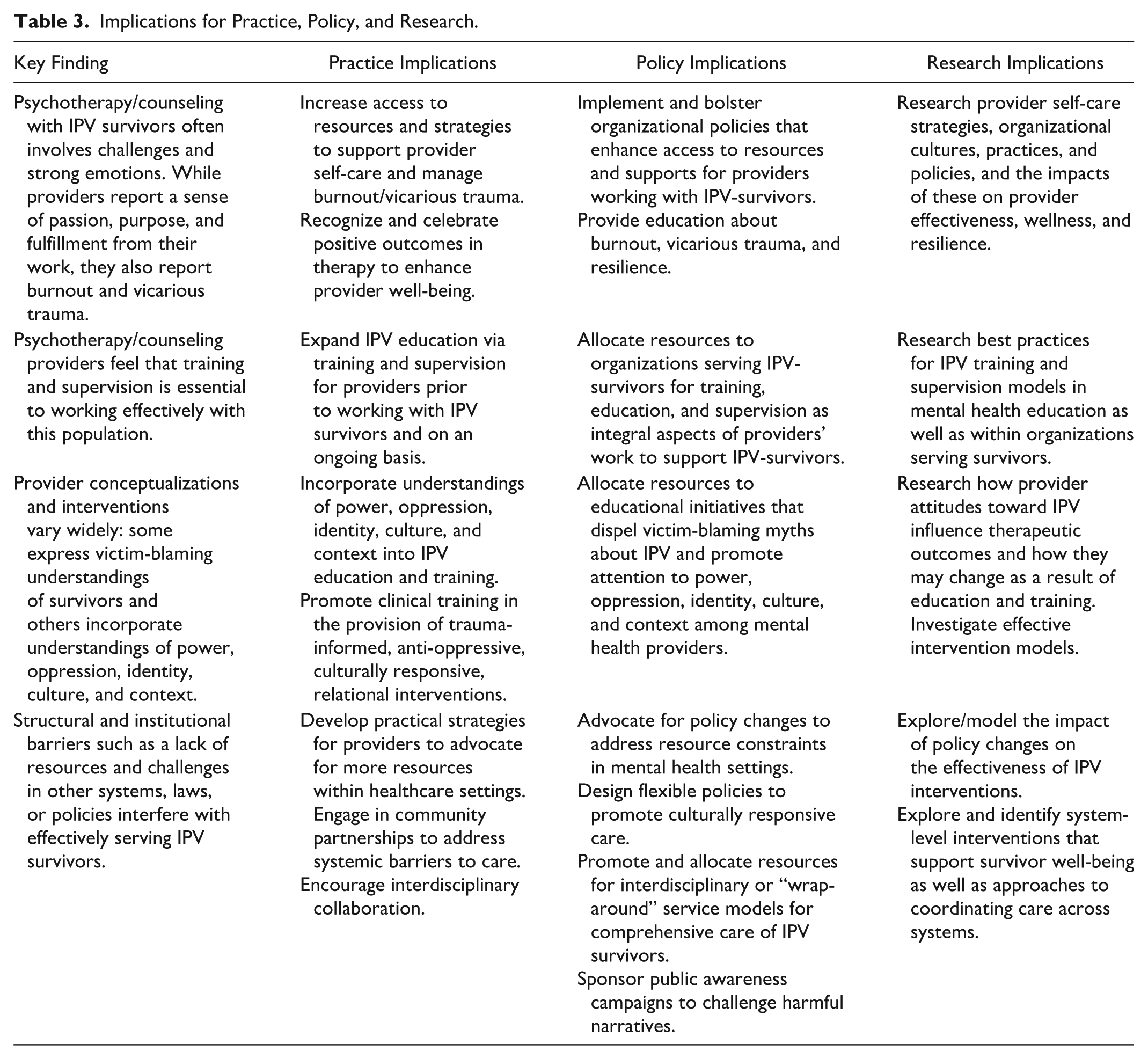
Finally, institutional and structural barriers significantly hindered providers’ ability to offer effective care. Many reported insufficient resources, including time and funding, as well as societal attitudes that minimize IPV and perpetuate harmful stereotypes (Kozlowska, 2020; Margherita et al., 2020; Watson et al., 2017). Providers noted that addressing these systemic barriers would require policy reforms and increased resources to improve both provider capacity and survivor outcomes (Wilson et al., 2021; Fleischack et al., 2017). Yet, providers struggled to intervene within patriarchal and oppressive contexts (Alani & Stroink, 2015; Fleischack et al., 2017; Goldblatt et al., 2009; Hahn & Scanlon, 2016; Horne et al., 2009; Kim et al., 2018). Collectively, findings highlight the complexity of providing psychotherapy to IPV survivors and emphasize the need for provider training and support, policy change, and further research (see Table 3).
Implications for Practice, Policy, and Research.
Implications for Research, Practice, and Policy
The review reveals critical gaps in training, supervision, and resources available to psychotherapy and counseling providers working with IPV survivors. The emotional and psychological burden carried by these providers underscores the importance of access to resources, strategies, and supports to promote their self-care and manage burnout/vicarious trauma. There is a need for policy change to bolster such essential supports. Providers may benefit from education about burnout, vicarious trauma, and resilience, as well as regular, trauma-informed supervision and peer support. When providers feel supported and understood, they can remain engaged and effective in their roles, ultimately benefiting both themselves and the survivors they serve (Singh et al., 2020). In the context of such supports, providers may be able to recognize and celebrate positive outcomes of therapy to maintain hope (Alani & Stroink, 2015). Future research can explore provider self-care strategies, organizational cultures, practices, and policies, and the impacts of these on provider effectiveness, wellness, and resilience for those serving IPV survivors.
Resources are clearly needed to promote educational initiatives that dispel harmful, victim-blaming myths about IPV and promote attention to power, oppression, identity, culture, and context among mental health providers (Alston et al., 2021). Making this training a standard part of curricula and professional development would better equip providers for the complexities of working with IPV survivors. Providers may benefit from initial and ongoing education in trauma-informed, anti-oppressive, culturally responsive, and relational practices. Such training should address not only the clinical aspects of IPV but also the societal and structural factors that sustain it. Training should prepare providers to recognize and respond to the intersectionalities of IPV survivors who often face overlapping forms of oppression. Providers who understand IPV in its broader contexts are better equipped to offer interventions that are effective and compassionate (Hahn & Scanlon, 2016; Reddy, 2019). Ongoing research is also needed on best practices for IPV training, supervision, and practice in mental health education as well as within organizations serving survivors. Research can examine how provider attitudes toward IPV influence therapeutic outcomes and/or how they may change as a result of education and training as well as the impacts of training programs on provider competence and survivor outcomes.
Addressing systemic barriers to effectively serving IPV survivors is also crucial. Adequate funding for mental health services is needed to improve access to longer-term, quality therapeutic interventions. Flexible organizational policies should allow for culturally responsive care. Given the wide-ranging consequences of IPV and multiple needs that many survivors experience (e.g., for legal, social, housing supports), coordination across disciplines is necessary to effectively address this social issue. Clinical training and supervision should incorporate methods for supporting interdisciplinary work. Expanding access to interdisciplinary or “wrap-around” services, especially those that are low-cost or subsidized, should be a priority to ensure providers have the resources to offer comprehensive care. Research can identify system-level interventions that support survivor well-being as well as approaches to coordinating care across systems.
Finally, broader societal changes are needed that address harmful societal norms and attitudes. Research can model the impact of macro-level policy changes on the effectiveness of IPV interventions. As IPV is an issue rooted in social inequities, without these changes, survivors will continue to face significant barriers to recovery.
Strengths and Limitations
This scoping review provides valuable insights into the experiences of psychotherapy and counseling providers working with IPV survivors. Strengths of this review include the peer-reviewed search strategy that we developed in consultation with a research librarian, the use of blind reviewers and auditing procedures we employed during article screening, the use of the ascendancy approach to identify articles, and the overall quality of included studies (CASP, 2018). Despite these measures to promote methodological rigor, it is always possible that studies meeting eligibility criteria could have been missed.
To address the research question, this review focused on qualitative research, which, while rich in descriptive detail, does not provide information that is generalizable across contexts. The subjective nature of the experiences captured in these studies likely reflects the specific cultural, regional, and institutional environments in which the research was conducted. Importantly, while our search yielded an international sample of studies, studies predominantly were conducted in Western countries such as the United States and the United Kingdom, which limits the applicability of findings globally. Additionally, the articles identified for inclusion in this review disproportionately focused on provider experiences working with women-identified and largely heterosexual survivors, with only three studies focusing on sexual minority survivors (Alston et al., 2021; Hancock, 2014; Hancock et al., 2014) and no studies focusing on gender minority survivors. Moreover, although some of the studies provided rich, valuable information on how cultural identities of survivors shape IPV, help-seeking, and therapy experiences (e.g., Kim et al., 2018; Reddy, 2019), many cultural identities and contexts were not represented. Furthermore, potentially salient survivor experiences with identity (e.g., disability, motherhood/parenthood, and those coping with serious mental illness) were not extensively captured by the included studies. Future research may include more information from a diverse range of geographic locations, cultural contexts, and intersectional identities among survivor-clients.
Conclusion
This review highlights significant challenges psychotherapy and counseling providers face when working with IPV survivors, including emotional distress, vicarious trauma, and burnout. Providers’ varying beliefs about IPV—ranging from contextual understandings to victim-blaming narratives—lead to a wide spectrum of interventions. The lack of consistent training and supervision leaves many unprepared, while systemic barriers and societal norms further hinder their work. To improve care, comprehensive trauma-informed and culturally responsive training is essential, alongside policy reforms that address structural inequities and increase resources for mental health services. Without these changes, both providers and survivors will continue to be constrained by systems that fail to fully support healing and recovery.
Footnotes
Appendix
Search strategy in APA PsychInfo.
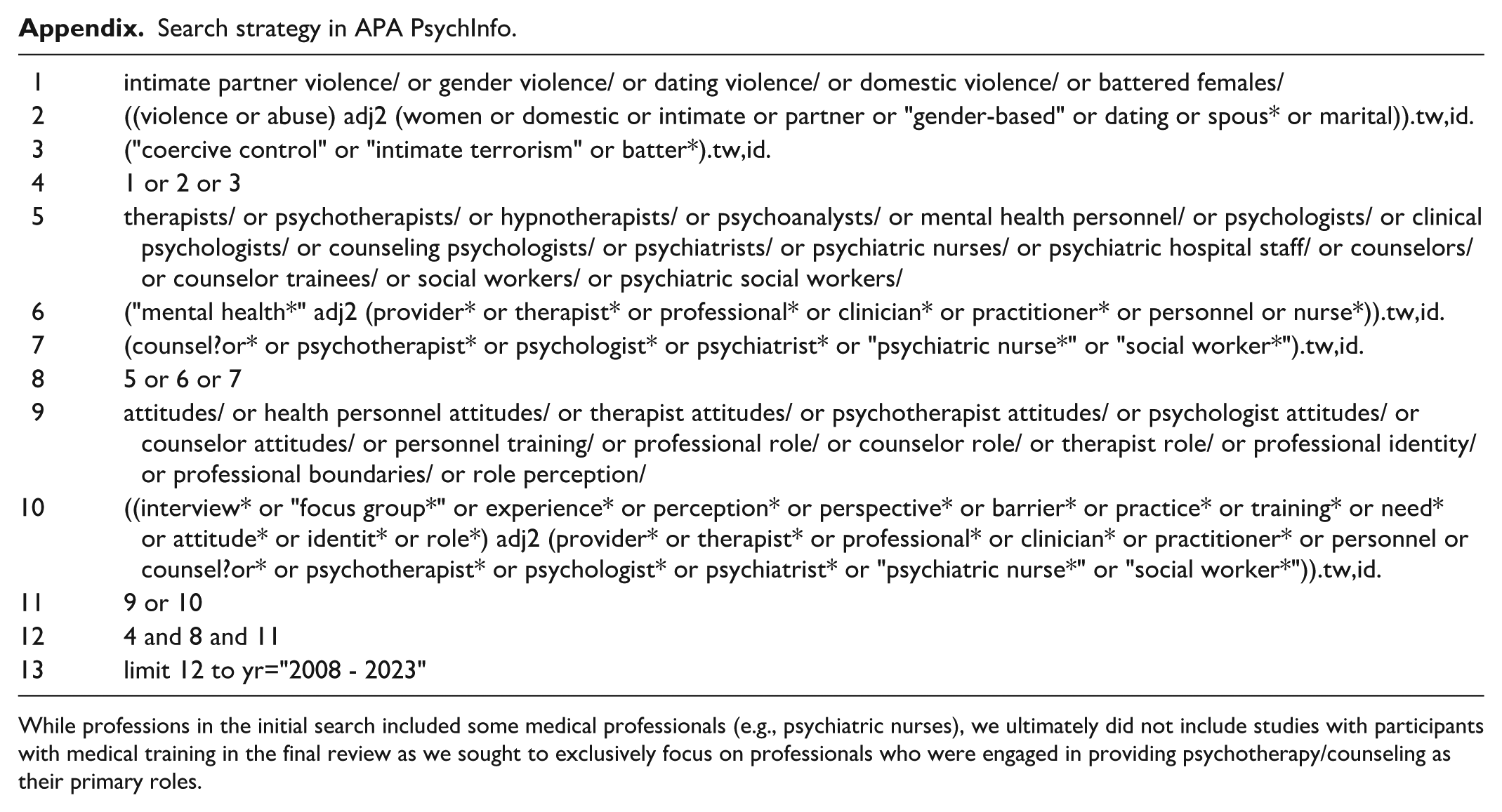
| 1 | intimate partner violence/ or gender violence/ or dating violence/ or domestic violence/ or battered females/ |
| 2 | ((violence or abuse) adj2 (women or domestic or intimate or partner or “gender-based” or dating or spous* or marital)).tw,id. |
| 3 | (“coercive control” or “intimate terrorism” or batter*).tw,id. |
| 4 | 1 or 2 or 3 |
| 5 | therapists/ or psychotherapists/ or hypnotherapists/ or psychoanalysts/ or mental health personnel/ or psychologists/ or clinical psychologists/ or counseling psychologists/ or psychiatrists/ or psychiatric nurses/ or psychiatric hospital staff/ or counselors/ or counselor trainees/ or social workers/ or psychiatric social workers/ |
| 6 | ("mental health*" adj2 (provider* or therapist* or professional* or clinician* or practitioner* or personnel or nurse*)).tw,id. |
| 7 | (counsel?or* or psychotherapist* or psychologist* or psychiatrist* or “psychiatric nurse*” or “social worker*”).tw,id. |
| 8 | 5 or 6 or 7 |
| 9 | attitudes/ or health personnel attitudes/ or therapist attitudes/ or psychotherapist attitudes/ or psychologist attitudes/ or counselor attitudes/ or personnel training/ or professional role/ or counselor role/ or therapist role/ or professional identity/ or professional boundaries/ or role perception/ |
| 10 | ((interview* or “focus group*” or experience* or perception* or perspective* or barrier* or practice* or training* or need* or attitude* or identit* or role*) adj2 (provider* or therapist* or professional* or clinician* or practitioner* or personnel or counsel?or* or psychotherapist* or psychologist* or psychiatrist* or “psychiatric nurse*” or “social worker*”)).tw,id. |
| 11 | 9 or 10 |
| 12 | 4 and 8 and 11 |
| 13 | limit 12 to yr="2008 - 2023" |
While professions in the initial search included some medical professionals (e.g., psychiatric nurses), we ultimately did not include studies with participants with medical training in the final review as we sought to exclusively focus on professionals who were engaged in providing psychotherapy/counseling as their primary roles.
Acknowledgements
The authors would like to acknowledge Alena Lawrence and Huda Salha for their research assistance in earlier phases of the project.
Data Availability Statement
There are no associated data with this review article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was funded in part by an SSHRC Institutional Grant made available through the University of Toronto. This article is published with funding available through University of Toronto.
Ethical Approval
No ethical approvals were required for this review article.