
Abstract
Previous reviews suggest that child maltreatment results in worse depression symptoms during adolescence and young adulthood. However, less is known about how depression symptoms evolve throughout this critical period. This systematic review evaluates changes in depression following child maltreatment and identifies factors influencing this relationship from adolescence to young adulthood. A search of APA PsycINFO, CINAHL, Embase, and Medline until January 13, 2023, found 87 studies from 31,495 records. Studies were included if they examined child maltreatment’s effect on depression symptoms for individuals aged 0 to 24, assessed child maltreatment or abuse, and neglect subtypes, measured depression diagnosis or symptoms at a subsequent time point, and used quantitative longitudinal or cohort designs. Of the studies meeting criteria, only 13 examined depression symptom changes, with mixed results found. Most studies identified severe and worsening depression symptom trends, as shown in both linear and nonlinear depression symptom studies. Other studies examined distinct patterns of depression symptom severity within a single sample (e.g., high vs. low symptom trends) and observed some improvements over time, suggesting the influence of protective factors. However, across all studies, depression symptoms remained relatively worse than in individuals without child maltreatment histories. One-third of studies explored factors influencing depression symptom change, primarily focusing on intrapersonal and interpersonal factors, though findings were inconsistent. A smaller subset investigated environmental factors, demonstrating that school-related aspects consistently impacted the relationship. Findings highlight the importance of early detection and timely intervention through continuous screening to improve depression outcomes for adolescents with child maltreatment histories.
Defining Child Maltreatment
Child maltreatment is defined as experiences of actual or potential harm to a child (defined as an individual aged under 18 years) that impacts the child’s health, survival, development, and/or dignity (World Health Organization [WHO], 2022). This review will focus on child maltreatment as experiences of (a) physical abuse, which involves the deliberate use of force against a child’s body resulting in injury, pain, or psychological suffering; (b) emotional abuse (or psychological abuse), which involves deliberate harmful interactions that convey to a child that they are worthless, bad, unwanted, unloved, or endangered, and persistent thwarting of basic emotional needs; (c) sexual abuse, which involves contact or non-contact sexual acts between a child and an adult, intended for the adult’s sexual gratification or other gains; and (d) neglect, which involves failure to provide minimum conditions essential for the normal development of a child (Cicchetti & Toth, 2005; UNICEF, 2023; WHO, 2006).
Prevalence of Child Maltreatment
Studies of the global prevalence of child maltreatment indicate that up to one billion children aged 2 to 17 years are subject to various subtypes of violence, including physical, sexual, or emotional violence and neglect, in any given year (WHO, 2022). A systematic review of 244 studies from regions worldwide found prevalence rates of 12.70% for child sexual abuse, 22.60% for physical abuse, 36.30% for emotional abuse, 16.30% for physical neglect, and 18.40% for emotional neglect (Stoltenborgh et al., 2015). Global studies have also found that 42% to 66% of individuals with one child maltreatment experience retrospectively self-report experiencing additional types of child maltreatment (Herrenkohl & Herrenkohl, 2009).
Child Maltreatment and Depression Symptoms
In the empirical literature, one of the most consistently observed and profound consequences of child maltreatment is its link to depression symptoms (Mehta et al., 2023; Springer et al., 2003). Developmental models of depression theorize that adverse experiences can contribute to the formation of dysfunctional attitudes, thereby increasing vulnerability to depression symptoms later in life (Beck, 1967; Beck, 2008). Specifically, adverse events such as child maltreatment can foster negative self-attitudes and perceptions. Subsequent stressful life events may trigger these negative thought processes, resulting in a greater cognitive vulnerability to depression symptoms (T. T. Wells et al., 2014). Empirical research has confirmed that experiencing any child maltreatment or specific subtypes greatly contributes to depression symptoms later in life (Infurna et al., 2016; Nelson et al., 2017). However, a significant portion of this research consists of cross-sectional investigations that have not established clear causal links between child maltreatment and depression symptoms.
Longitudinal Research on Child Maltreatment and Depression Symptoms
Longitudinal empirical research has demonstrated that child maltreatment can significantly impact depression symptoms during sensitive periods of development (Gerke et al., 2018; Khan et al., 2015), with evidence suggesting worsening depression outcomes from adolescence to young adulthood (Dunn et al., 2013; LeMoult, 2020). A portion of this research has found that child maltreatment can lead to varying depression symptom trajectories during this developmental period, often significantly worse than those without child maltreatment experiences (Bayly et al., 2022; Carlson & Oshri, 2018; Lauterbach & Armour, 2016; Wang et al., 2022). For instance, Wang et al. (2022) investigated depression symptom trajectories among 890 children from China, finding that individuals with more severe child maltreatment experiences were more likely to exhibit significantly higher stable-moderate or high-decreasing depression symptom trajectories compared to low-decreasing depression symptom trajectories. Findings from this study, along with similar results from other longitudinal research (Carlson & Oshri, 2018; Lauterbach & Armour, 2016), indicate that child maltreatment results in worse depression symptoms but can fluctuate throughout adolescence and young adulthood, with some evidence of possible recovery. Despite this evidence, existing reviews have not yet consolidated this evidence to examine common trends in how child maltreatment impacts depression symptoms during this developmental stage.
Previous Reviews
Approximately 11 existing systematic reviews have confirmed a strong association between child maltreatment and depression symptoms (see Supplemental Appendix A). Only a small number of systematic reviews have included evidence on the longitudinal relationship between child maltreatment and depressive symptoms in adolescent and young adult samples, and none have analyzed longitudinal findings independently from cross-sectional data. For instance, Infurna et al. (2016) analyzed data from 12 studies (4,372 study participants) and found that the association between specific subtypes of child maltreatment was stronger in adolescence than in adulthood. The study suggests that the recency of maltreatment, the difficulties associated with this period, or a lack of protective factors may account for this finding. However, the review did not analyze whether depression symptoms persist throughout adolescence and young adulthood, nor did it explore the contributing factors. Moreover, the review only reported cross-sectional data and did not analyze findings from longitudinal studies in the “Results” section. In addition, the study exclusively employed the Childhood Experience of Care and Abuse interview (CECA) to measure child maltreatment and employed heterogeneous measures of depression, coded categorically for synthesis.
In a subsequent review, Yu et al. (2017) examined both cross-sectional and longitudinal data from 31 studies (with 24,283 study participants), reporting that the association between child maltreatment and depression symptoms was strongest during adolescence. The study suggests that this may be due to the onset of depression symptoms often occurring in adolescence and the increased vulnerability of adolescents to subsequent abuse. Despite its important findings, Yu et al.’s (2017) review did not distinguish between cross-sectional and longitudinal findings, nor did they report on factors that can affect the severity of depression symptoms following child maltreatment.
The Current Study
The overall aim of the current study was to determine common depression symptom trends that adolescents experience following child maltreatment and to evaluate research on what predicts escalating trajectories versus other trajectories. Further aims of the study were, first, to explore the extent to which child maltreatment results in changes in depression symptoms across adolescence and young adulthood, and second, to explore factors that might influence depression symptom trajectories in children with a history of child maltreatment.
Methods
Protocol and Registration
The review was registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD42023374946; Binks et al., 2022). The review is reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement (Page et al., 2021).
Information Sources and Search Strategy
In January 2023, searches were conducted in four electronic databases: APA PsychINFO, CINAHL, Embase, and Medline (see Supplemental Appendix B for the full search strategy). The dates ranged from 1930 to 2023, reflecting preliminary searches. In March 2023, keyword searches of all volumes and issues of four key journals were conducted electronically via journal homepages: Child Abuse & Neglect, Child Maltreatment, Affective Disorders, and Child and Adolescent Psychopathology.
Inclusion Criteria
Studies were included if they examined the effect of child maltreatment on depression symptoms that met the following criteria: (a) study participants were children, adolescents, or young adults aged between 0 and 24 years, reflecting both the periods when child maltreatment may occur (0–18 years) and the age range of current interest regarding outcomes, that is, adolescence and young adulthood (10–24 years); (b) studies measured exposure to at least one form of child maltreatment, including physical abuse, emotional or psychological abuse, sexual abuse, or neglect; and (c) studies reported one or more recorded self-report or interview measure of depressed symptoms or major depressive disorder at a time point following the measurement of child maltreatment. This includes studies with measurement of depressive symptoms at a single subsequent time point (prospective studies), two time points (prospective studies that can show changes in depressive symptoms), or three or more time points (trajectory studies); (d) Study designs were quantitative, including longitudinal or cohort study designs.
Exclusion Criteria
Studies were excluded: (a) with participants over the age of 24 years; (b) that measured exposure to other forms of violence such as relationship or dating violence, intimate partner violence, peer victimization, bullying or cyberbullying, neighborhood or community violence, parental substance abuse, or parental incarceration; (c) that did not measure depression during childhood, adolescence, or young adulthood, used imprecise definitions of depression (e.g., internalizing disorder/symptoms), used definitions overlapping with other constructs (i.e., suicidal ideation), or measured depression symptoms solely via tests of neurological functioning; (d) with ineligible study designs (e.g., reviews, cross-sectional studies); (e) where the full text was not available in English; and (f) animal studies (e.g., rodent experiments).
Selection Process
Search records were downloaded to EndNote 20 (Clarivate, 2013), and duplicates were removed before being imported into the web-based systematic reviewing platform Rayyan (Ouzzani et al., 2016). Rayyan was selected for its reliability in excluding irrelevant records; however, its use carries the potential risk of inadvertently omitting eligible studies (Valizadeh et al., 2022). Four reviewers, working independently, screened titles and abstracts against inclusion and exclusion criteria. Two reviewers independently screened the full text of the articles to determine eligibility. A third reviewer resolved disputes.
Data Collection and Data Items
Data were extracted from the included studies using a standardized form adapted from the Cochrane Collaboration Data Extraction and Assessment Form (Effective Practice and Organisation of Care [EPOC], 2017). Extracted data included citation, design (nationally representative, clinical vs. non-clinical, secondary data source, number of participants, number of waves, age at baseline, sex, race/ethnicity), child maltreatment (measurement tool and format, duration of measurement), depression symptoms (measurement tool, duration of measurement, validation), results (missing data, statistical method, controls/covariates, outcome), and factors influencing the relationship between child maltreatment and depression symptoms (factor, factor type, outcome, duration of measurement). The data extraction form was pilot-tested on 10 randomly selected studies and revised to include details on child maltreatment measures, depression types, and time points. Any uncertainties were discussed with another reviewer to ensure accuracy.
Quality Assessment
In the absence of a methodological appraisal tool specifically for longitudinal studies, the Newcastle–Ottawa Quality Assessment Form for Cohort Studies (NOS) was adapted (G. A. Wells et al., 2014; see Supplemental Appendix C for the adapted scale). The NOS is widely used to evaluate the effectiveness of observational studies (T. T. Wells et al., 2014; Zeng et al., 2015) and has been effectively used to appraise quality in child maltreatment studies (e.g., Baldwin et al., 2023; Li et al., 2016). The tool also includes items measuring key longitudinal factors, such as attrition and reporting methods. The tool consists of eight items assessing: (a) selection of samples (four items); (b) comparability of exposed and non-exposed individuals (one item); and (c) outcome(s) assessment (three items). The tool uses a star rating system to rate each study as good, fair, or poor. For each item, studies could be awarded a maximum of one star, except for the compatibility measure, which could be awarded a maximum of two stars. Studies with higher star ratings indicated higher methodological quality and a lower risk of bias. One reviewer independently rated each study against each criterion.
Results
Search Results
The initial search yielded 50,303 results; 31,495 remained after duplicates were removed. After all screening stages and journal hand-searching, 87 studies met the inclusion criteria. The PRISMA flowchart is shown in Figure 1.
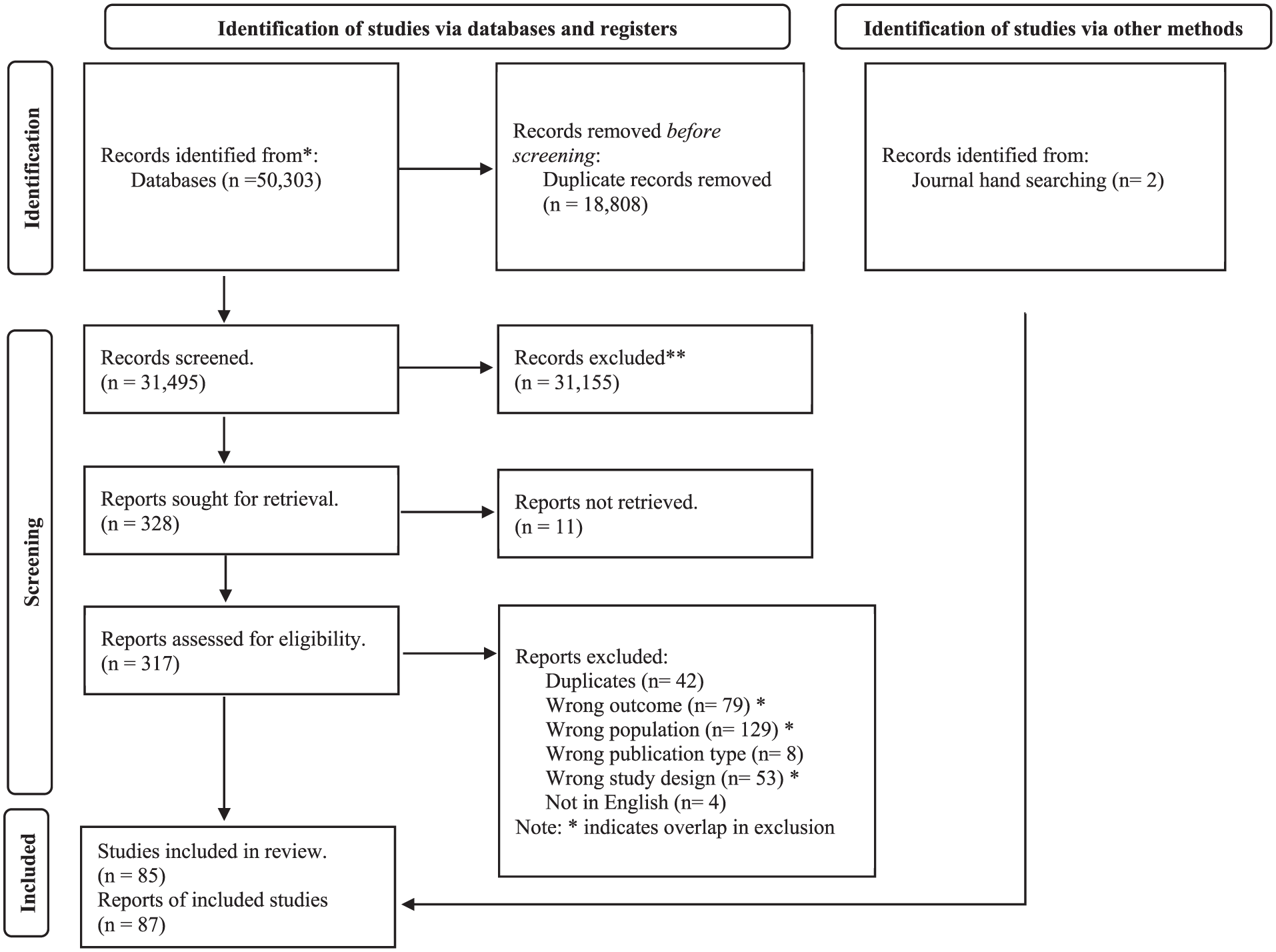
PRISMA flowchart.
Characteristics of Included Studies
Full details on study characteristics are shown in Supplemental Appendix D. Study publication dates ranged from 1995 to 2022, with the majority (66; 76%) published from 2010 and onwards. The 87 studies comprised 1,109,104 participants in total. The sample sizes from individual studies ranged from 64 to 978,647 participants. Studies were predominantly from high-income countries (78; 90%). Approximately 21 of the total number of studies were described as nationally representative (24%), and these were from the United States (15; 71%), China (1; 5%), Europe (1; 5%), Denmark (1; 5%), Pakistan (1; 5%), Spain (1; 5%), and the United Kingdom (1; 5%). The average age at baseline was 12.58 years. Most studies reported a balanced participant gender ratio; however, several studies (15; 17%) reported a female-dominant sample (in which >70% of the sample was female). Most studies reported ethnicity as white dominant (30; 34%) (in which >50% of the sample were white) and black dominant (16; 18%) (in which >50% of the sample were black). A proportion of studies did not report participant ethnicity (33; 38%).
Child Maltreatment Measurement
Examining the 87 studies, 59 studies of child maltreatment measures were obtained retrospectively (68%), 23 were obtained prospectively (26%), and 5 included both retrospective and prospective measures (6%). These assessments did not always align temporally with the time points at which depression symptoms were measured. When defining child maltreatment, most studies adopted an aggregated approach, calculating any/total maltreatment experienced (i.e., inclusive of all forms of child maltreatment; 36; 41%). A small proportion of studies, 5, defined child maltreatment as multi-type child maltreatment (6%). Across all 87 studies, 65 (75%) measured one or more subtypes of child maltreatment individually. Studies included 35 independent measures of neglect (40%), 34 of emotional abuse (39%), 32 of sexual abuse (54%), and 31 of physical abuse (36%).
Of the 87 studies, 51 studies of child maltreatment assessments utilized standardized tools (59%), 17 national child protection reports (20%), and 19 individually constructed items and questionnaires (22%). Most studies utilized standardized tools such as the Child Trauma Questionnaire (CTQ; Bernstein et al., 2003; 26; 30%) and the Conflict Tactics Scale (CTS; Straus, 1979; 14; 16%). Studies that employed individually constructed questionnaires often constructed items using pre-established child maltreatment measures (e.g., Bayly et al., 2022; Paul & Eckenrode, 2015; Schilling et al., 2007a). Studies that employed Child Protection Services (CPS) records for assessment were mostly conducted in the United States (US; 13; 15%), often utilizing shared datasets (e.g., the LONGSCAN dataset).
Depression Measurement
Examining all 87 studies revealed that 68 studies characterized depression as a depressed mood or symptom (78%) and 19 as a clinical disorder (22%). In the symptom-based studies, 15 studies used the Centre for Epidemiologic Studies Depression Scale (26%; Radloff, 1977), 13 used the Children’s Depression Inventory (CDI; 22%; Kovacs, 1992), and 6 used the Beck Depression Inventory (BDI; 11%; Beck et al., 1961). In studies that defined depression as a clinical disorder, 4 studies used the Structured Clinical Interview for DSM-IV (SCID; 21%; Spitzer et al., 1992), and another 4 used a version (children or adult version) of the Diagnostic Interview Schedule Version IV (21%; Robins et al., 2000).
Methodological Quality
Of the 87 studies, 50 received poor NOS methodological ratings (57%), 29 received fair ratings (33%), and 7 received good ratings (8%). Weaknesses in quality stemmed from a lack of representativeness, heavy reliance on self-report measures, and insufficient information on sample attrition. However, these weaknesses are typical in longitudinal child maltreatment research (Biehal, 2014; Laurin et al., 2018; van der Hoeven et al., 2023). Methodological strengths included using community-based control groups, confounder controls, adequate follow-up periods (>1 year), utilization data linkage to verify self-report information, and implementing missing data imputation when necessary.
Results for Longitudinal Studies
To interpret themes within this research, results were analyzed by categorizing studies via research intent and type of depression symptom trajectories (as outlined in Schubert et al., 2017). Initially, the studies were divided into two groups: those with two subsequent time points of depression symptoms (16 prospective studies) and those with three or more subsequent time points of depression (19 trajectory studies). Studies with only one depression prospective time point (53 studies) were excluded from the subsequent results as they are unable to ascertain change in depressive symptoms over time. Subsequently, studies were further categorized based on the type of depression symptom trends identified (linear, nonlinear, etc.) and the severity of depression symptoms explored within a single study. Full details of these studies are shown in Table 1.
Longitudinal Studies Measuring the Impact of Child Maltreatment on Depression with Two or More Depression Outcomes.
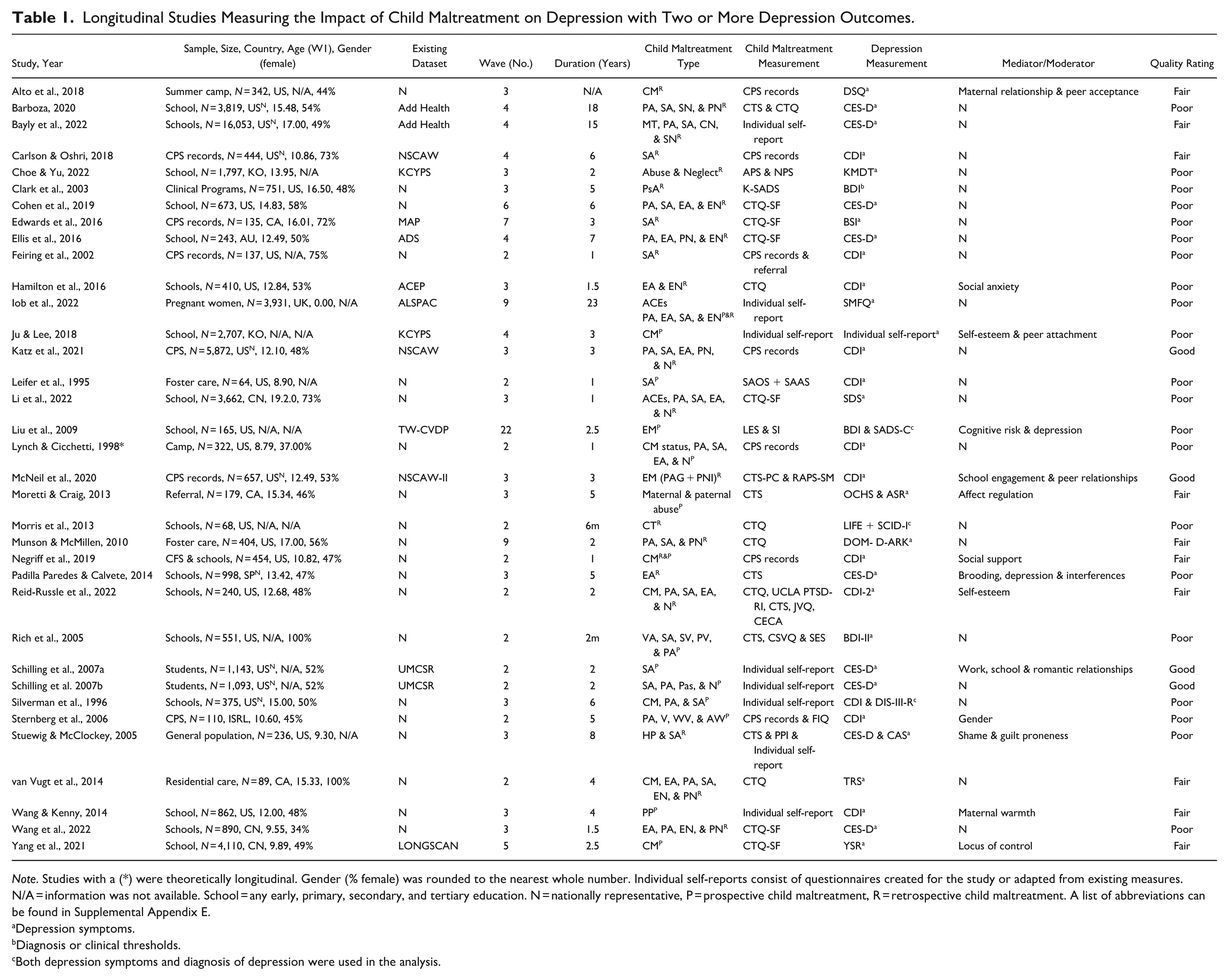
Note. Studies with a (*) were theoretically longitudinal. Gender (% female) was rounded to the nearest whole number. Individual self-reports consist of questionnaires created for the study or adapted from existing measures. N/A = information was not available. School = any early, primary, secondary, and tertiary education. N = nationally representative, P = prospective child maltreatment, R = retrospective child maltreatment. A list of abbreviations can be found in Supplemental Appendix E.
Depression symptoms.
Diagnosis or clinical thresholds.
Both depression symptoms and diagnosis of depression were used in the analysis.
Studies With Two Prospective Depression Symptoms Measurements
Among the 87 studies in the review, 16 investigated the impact of child maltreatment using two prospective measurements of depression symptoms (18% of the total studies included). However, only 2 studies examined how child maltreatment influenced changes in depressive symptoms from adolescence to young adulthood. One study (Morris et al., 2014) found that individuals with greater child trauma exposure experienced more rapid increases in depression symptoms, and the other (Leifer & Shapiro, 1995) found that depression symptoms decreased (improved) over time. Neither of these studies included a comparison group of children who had not experienced maltreatment; however, it is not clear whether depression symptoms decreased to levels observed in individuals without child maltreatment experiences.
Studies With Three or More Prospective Depression Symptoms Measurements
The remaining 19 studies explored the impact of child maltreatment on depression symptoms, with three or more depression symptom change measurements (21% of total studies included). Of these studies, 12 explored if child maltreatment impacted changes in depression symptoms (61%), including 5 studies with one continuous depression symptom measurement and 7 studies that measured patterns of depression symptom severity within a single study. Four of the studies with a single continuous measure of depression symptoms found linear patterns of depression symptoms. Three studies found that child maltreatment was associated with increasing depression symptom trajectories. These studies found that experiencing greater instances of child maltreatment was also associated with more initial depression symptoms, which gradually increased over time, compared to those with fewer frequent experiences of child maltreatment, who had lower depression symptoms (Choe & Yu, 2022; Cohen et al., 2019; Ju & Lee, 2018). However, for Cohen et al. (2019), these increases were only observed for clinical thresholds of anhedonia. One other study found that child maltreatment was associated with decreasing depression symptom trends. In this study, depression symptoms were initially high, which then rapidly decreased at first, followed by a more gradual, steady decline over time (Edwards et al., 2022). However, the study found that more severe instances of child maltreatment resulted in increasing depression symptom trends over time. An additional study found a nonlinear pattern of depression symptoms, containing both increases and decreases in single measurements of depression symptoms. The study found initial high depression symptoms that rapidly decreased during later middle adolescence, before steadily rising in later adolescence (Bayly et al., 2022). Collectively, the results of all these studies with one continuous depression symptom measurement demonstrated that the impact of child maltreatment mostly resulted in worsening depression symptom trends over time. However, these results did vary according to the subtype of child maltreatment and extent of exposure. No clear pattern emerged across studies regarding which subtypes of child maltreatment produced different patterns. Very few of these studies included a control or comparison group of non-maltreated. When they did, there were significantly fewer participants in the decreasing groups, and the findings were again not compared with a sample of non-maltreated individuals.
The remaining 7 studies examined various patterns of depression symptom severity within a single study. Of the 7 studies, 3 identified linear depression symptom trajectories that were relatively high or moderate and remained stable across the measured period of adolescence (Ellis et al., 2017; Iob et al., 2022; Li et al., 2022). Specific subtypes of child maltreatment were associated with either moderate depression symptoms that remained relatively high or consistently severe across adolescence and young adulthood. Four studies found that child maltreatment was linked to two distinct linear depression symptom trajectories, increasing and/or decreasing (Carlson & Oshri, 2018; Ellis et al., 2017; Munson & McMillen, 2010; Wang et al., 2022). For instance, Wang et al. (2022) found two depression trajectories, one with initially severe symptoms that declined, and another with stable high levels that increased suddenly. By contrast, Carlson and Oshri (2018) identified more nonlinear trajectories, where depression symptoms initially increased and then subsequently decreased or gradually decreased before increasing again. Among studies that compared various patterns of depression symptom severity, only 1 (Barboza, 2020) found that child maltreatment was linked to three distinct symptom trajectories: high-decreasing, moderate-decreasing, and low-increasing depression symptoms. Findings from studies examining various patterns of depression symptom severity in a single study were specific to certain types of maltreatment and involved relatively small sample sizes for those groups.
Factors Impacting Depression
Approximately one-third (28; 32%) of the total 87 studies explored factors that might escalate or de-escalate depression symptoms in children with a history of child maltreatment. Approximately 19 (68%) of studies investigated intrapersonal factors, 11 of which studied cognitive processes (58%), 5 emotional responses (26%), and 3 mental health outcomes (16%). Of the cognitive processes identified, there was a notable paucity of studies investigating the same factors (see Supplemental Appendix F). Self-esteem was the most frequently examined cognitive process, assessed in 4 of the studies. Among these, one study found that lower self-esteem mediated the relationship between child maltreatment and worse depression symptoms at multiple points during adolescence (Reid-Russell et al., 2022); however, another did not find evidence of this mediation (Ju & Lee, 2018). The other 2 studies examining the impact of self-esteem measured depression symptoms at a single subsequent time point and found that lower self-esteem mediated the relationship between child maltreatment and worse depression symptoms (Kim et al., 2022; Yoon et al., 2019); however, in one study, which measured the subtypes of child maltreatment, this mediation was only significant for emotional abuse (Yoon et al., 2019).
Within the studies measuring emotional responses, 3 studies assessed the impact of some form of emotion regulation on the relationship between child maltreatment and depression symptoms. For instance, Moretti and Craig (2013) examined 179 adolescents and found that greater affect dysregulation, defined as an individual’s capacity to manage emotions without undue attempts to avoid or suppress distressing emotions, mediated the relationship between maternal abuse and worse depression symptoms at three time points across adolescence (approximately 15–19 years old). Other studies found similar results when examining similar constructs; however, these only measured mediators at a single time point. For instance, Shenk et al. (2015) examined 110 female adolescents (14–19 years old) and found that greater emotion dysregulation, measured as difficulties in adjusting behaviors that influence the type, intensity, or frequency of emotional responses, mediated the relationship between child maltreatment and worse depressive symptoms. However, negative affect, measured as the intensity of a negative affective state, did not mediate the relationship between child maltreatment and depressive symptoms. Zhou and Zhen (2022) examined 1,689 adolescents (12–17 years old) and found that both greater emotional regulation and anger, individually and combined, mediated the relationship between emotional abuse and worse depression; however, results were not significant for physical abuse. These suggest that constructs related to emotional regulation play an important part in the relationship between child maltreatment and depressive symptoms, with some indication that certain factors may have a stronger influence at specific time points.
Of the 3 intrapersonal studies investigating mental health outcomes, 2 focused on examining different components of internalizing difficulties. In 1 study (Russotti et al., 2021), analyzing 391 adolescents (10–12 years old), greater internalizing symptoms, but not externalizing symptoms, mediated the association between early, recent, and chronic child maltreatment exposure and worse depression symptoms in young adults. Another study (Hamilton et al., 2016), when examining 410 early adolescents (12–13 years old), found that only depression symptoms, and not social anxiety symptoms, mediated the relationship between emotional abuse and neglect and subsequent depression symptoms at mid-adolescence (approximately 14–15 years old). However, the study by Negriff et al. (2019) examined a younger group of 454 adolescents (approximately 9–13 years) and found that depression symptoms did not mediate the relationship between child maltreatment and depression symptoms at a subsequent time point. These studies suggest that increased mental health symptoms, specifically depression symptoms, may lead to increased depression symptoms at later time points.
Among interpersonal factors, 3 studies examined the impact of parental relationships on the link between child maltreatment and depression symptoms; however, the results were conflicting. For the most part, studies did not find that family variables like parental warmth and family social support mediated the relationship between child maltreatment and depression symptoms (Negriff et al., 2019; Wang & Kenny, 2014). However, evidence did suggest that worse maternal relationship quality mediated the association between child maltreatment and greater depression symptoms; however, this was only significant for females (Alto et al., 2018). These findings suggest that the impact of parental–child relationships may depend on the sex of the individual who receives the support, and whether it was given by mothers.
Approximately half (6 studies) of the interpersonal studies examined the influence of peer relationships on the relationship between child maltreatment and depression symptoms. Three studies exploring social relationships with peers/friends, albeit measured differently in each study, found that worse peer relationship problems, peer bullying, and social acceptance impacted the relationship between child maltreatment and depression symptoms (Alto et al., 2018; Huang et al., 2021; McNeil et al., 2020). However, for some of these studies (i.e., McNeil et al., 2020), this outcome was dependent on the type of child maltreatment experienced. For instance, McNeil et al. (2020) found that worse peer relationship problems mediated the association between a form of abuse conceptually like emotional abuse, referred to as psychological aggression, but not a form like neglect, parental non-involvement, and greater depression symptoms. In addition to this evidence, 2 additional studies found that general peer social support did not have an impact on depression symptoms for those with child maltreatment experiences (Glickman et al., 2021; Negriff et al., 2019). However, in Negriff et al. (2019), social support measures were also combined with family support. Therefore, this indicates that peer relationship problems may be more influential for depression symptom outcomes for those with experiences of child maltreatment.
Two interpersonal studies (25%) explored the impact of intimate relationship quality on the association between child maltreatment and depression symptoms, with both finding that intimate relationships influenced this association. For instance, Fitzgerald (2022) found that greater relationship quality with a partner, including support, strain, and disagreements, mediated the relationship and was linked to fewer depression symptoms. Similarly, Schilling et al. (2007a) found that lower intimate relationship support mediated the relationship between child sexual abuse and depressed mood, with lower support linked to more depression symptoms. Both these studies included older adolescents and young adults. These studies suggest that intimate relationships with a partner can have a substantial influence on the relationship between child maltreatment and depression symptoms in older adolescents and young adults.
In the smaller subset of influencing factors, environmental factors, 2 studies explored the impact of school, one physical activity, and one work activity on the relationship between child maltreatment and depression symptoms. A study found that lower school engagement mediated the relationship between a form of neglect, parental non-involvement, and increasing depression symptoms, but the direction and significance of this relationship varied by race and ethnicity (McNeil et al., 2020). Another study found that greater school enjoyment and school attendance mediated the relationship between child sexual abuse and fewer depression symptoms (Schilling et al., 2007a). Other environmental factors like work experience (Schilling et al., 2007a) and physical activity (Jiang et al., 2022) were not impactful.
Discussion
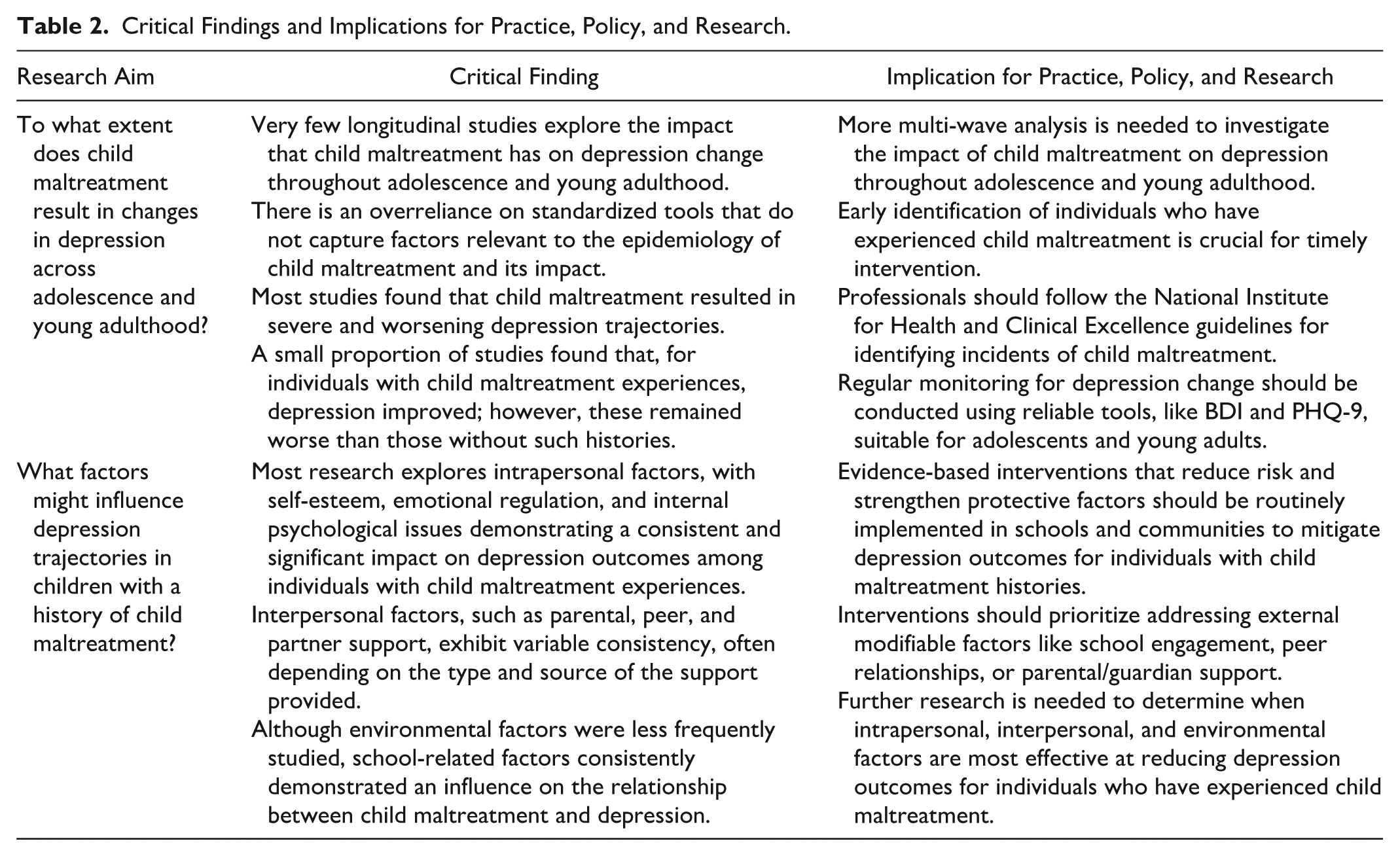
This systematic review evaluated how child maltreatment impacts changes in depression symptoms and identified factors that exacerbate or mitigate depression symptoms during adolescence and young adulthood. Results revealed that there is a paucity of studies that examine depression symptom change; most studies identified by the inclusion criteria had one measurement of child maltreatment and a single prospective measurement of depression. Studies with two prospective depression time points that measured depression change found that most studies with linear patterns of depression trends identified severe and worsening depression symptom trends. Other trajectory studies, which included three or more measures of depression change, found that studies that compared various patterns of depression symptom severity in a single study noted some improvements over time, suggesting the influence of protective factors. However, regardless of the pattern observed, outcomes for maltreated individuals remained worse than those without such histories. One-third of the studies explored factors influencing depression symptom escalation or de-escalation, mostly focusing on intrapersonal and interpersonal factors, though findings were inconsistent. A smaller subset investigated environmental factors, demonstrating that school-related factors consistently impacted the relationship. A summary of critical findings and implications for practice, policy, and research is shown in Table 2.
Critical Findings and Implications for Practice, Policy, and Research.
This is the first known review to investigate how child maltreatment impacts depression symptom changes in adolescents and young adults. The primary finding is that most adolescents and young adults with child maltreatment histories experience severe or escalating depression symptoms during this developmental period. Existing reviews, although not explicitly focusing on child maltreatment, consistently show that adolescent subgroups differ in their depression symptom development over time, particularly those exposed to stressful life events (Musliner et al., 2016; Schubert et al., 2017; Shore et al., 2018). For instance, Schubert et al. (2017) found that most adolescents and young adults normatively report lower levels of depression symptoms at baseline measurements compared with some slight normative increases at subsequent time points. However, 5–12% of the population report high and fluctuating depression symptom trajectories due to chronic stress exposure. Similarly, Shore et al. (2018) found that a subgroup of children and adolescents with high or increasing depression symptom trajectories was associated with greater stress reactivity, likely due to adverse early life events.
A novel finding from this review is that adolescents and young adults with child maltreatment histories can experience initial high depression symptoms that improve over time. Prior reviews, though not explicitly focused on child maltreatment, have reported decreasing depression symptom trends. For example, Shore et al. (2018) found that 56% of the population had no or low depression symptom trajectories, while 12% exhibited high, increasing, or decreasing depressive symptom trajectories. Musliner et al. (2016) similarly found that the proportion of individuals with decreasing depression symptom trajectories varied from 2.7% to 71% within studies. These reviews suggest that decreasing depression symptom trajectories may be linked to normative depression symptom development, such as the natural decline in depressive symptoms often observed due to aging or the influence of protective factors during these periods (Musliner et al., 2016; Schubert et al., 2017; Shore et al., 2018). Overall, both previous and current reviews underscore the dynamic relationship between child maltreatment and depression symptoms in adolescents and young adults.
Fewer studies examined factors that might escalate or de-escalate depression symptoms in children with a history of child maltreatment. However, despite their importance, there is a scarcity of reviews focusing on influential factors. Most studies within the review explored the effects of intrapersonal factors on the association between child maltreatment and depression symptoms, with many suggesting that poor cognitive, emotional, and mental health increased depression symptoms for those with child maltreatment histories. This is in line with previous reviews that examined how psychological and cognitive factors can impact the relationship between child maltreatment and depression symptoms (Klumparendt et al., 2019; Li et al., 2020; Schierholz et al., 2016; Zhao et al., 2022).
In the present review, the impact of interpersonal factors was inconsistent. There was some evidence that greater relationships with parents, social support, and intimate relationships were associated with reduced depression symptoms for those with child maltreatment experiences (Alto et al., 2018; McNeil et al., 2020; Huang et al., 2021). Prior reviews have briefly explored the impact of social and family support on the relationship between child maltreatment and depression symptoms, with most finding that low social support increases vulnerability to depression symptoms for those with child maltreatment experiences (Braithwaite et al., 2017; Fritz et al., 2018; Hoppen & Chalder, 2018; Li et al., 2020). These reviews suggest that individuals with child maltreatment histories encounter more significant difficulties forming relationships and seeking social support from others. However, very few of these reviewed studies examined the impact of family support or parental relationships on depression symptoms for those with child maltreatment experiences. This may be attributed to the difficulties associated with parents being the perpetrators of child maltreatment (Younas & Gutman, 2023).
Fewer studies have explored environmental factors, with school-related aspects, such as increased school engagement, enjoyment, and attendance, linked to reduced depression symptoms in individuals with experiences of child maltreatment. Although not explicitly focusing on depression outcomes, reviews on child maltreatment underscore the significant role of school engagement and participation in extracurricular activities in mitigating negative outcomes (Jean-Thorn et al., 2023; Scoglio et al., 2021).
Diversity and Contextual Factors in Interpreting Review Findings
Findings are limited by their focus, primarily on high-income Western countries, with over half of the studies from the United States alone. Although these are common limitations in child maltreatment research (Mikton & Butchart, 2009; Stoltenborgh et al., 2015), empirical studies indicate that cultural and socioeconomic status are significant sources of variation in child maltreatment outcomes (Lansford et al., 2015; Raman & Hodes, 2011). Findings from the current study may not be generalizable to demographics outside of high-income Western countries, as experiences of child maltreatment may differ, and fewer resources may be available to support children in those regions. Furthermore, the studies included in the review generally maintained a balanced representation of genders, enhancing the generalizability of the findings to broader populations. However, empirical research has demonstrated that types and rates of child maltreatment differ substantially by sex (Gallo et al., 2018; Moody et al., 2018). For example, Moody et al. (2018) found that girls had higher rates across maltreatment types in most studies (e.g., sexual abuse: 20.40% girls vs. 14.30% boys; emotional abuse: 33.20% girls vs. 21.00% boys; neglect: 40.50% girls vs. 16.60% boys). As a result, these studies’ findings might not fully capture how child maltreatment and depression symptoms vary by sex, making it harder to interpret the impact of child maltreatment that is specific to each sex. In addition, research has found substantial gender differences in the effects of child maltreatment and depression onset and long-term outcomes (Dong et al., 2024; Gallo et al., 2018). While some of the studies in the review reported a female-dominant sample (with >70% female participants), very few explicitly investigated gender differences regarding depression symptom outcomes. Consequently, the potential impact of gender differences should be carefully considered in interpreting these findings.
The findings of this review may be influenced by overly simplistic measurements and tools utilized to assess child maltreatment. Commonly standardized tools such as the CTQ (Bernstein et al., 1994) and CTS (Straus, 1979) were employed. Despite their reliability and validity (Jones et al., 2017; Saini et al., 2019), these tools cannot capture contextual factors relevant to the epidemiology of child maltreatment and its effects. Research suggests that findings may be susceptible to change when considering factors such as frequency, chronicity, duration, and the relationship between the perpetrator and the child (Danielson et al., 2005; Manly et al., 2001; Scott et al., 2023; Vallati et al., 2020). Moreover, many tools aggregated specific child maltreatment subtypes into a consolidated index. While the experience of multiple maltreatment subtypes is relatively common (see Higgins et al., 2023), using only a consolidated measure may obscure the attribution of outcomes to specific maltreatment subtypes or combinations of maltreatment subtypes. Consequently, the limitations of these tools may influence the review findings.
Directions for Future Research and Practical Implications
To elucidate the impact of child maltreatment on depression symptom trajectories, more longitudinal multi-wave analyses are needed. Exploring outcome differences according to geographic location, socioeconomic background, and ethnicity helps identify at-risk groups, as these characteristics can affect both vulnerability to depression symptoms and response to intervention. In turn, findings from these investigations will inform the development of culturally and contextually appropriate interventions. Simultaneously, fostering global interdisciplinary collaboration among research teams will enhance the production of consistent and cohesive research outcomes in the future. Future studies should utilize tools that capture the contextual factors of child maltreatment (Meng et al., 2018), as this approach promises more nuanced insights into the relationship between maltreatment and depression symptoms. In addition, research could also explore multiple types and combinations of child maltreatment, with an emphasis on diverse populations and contextual influences such as gender.
Findings from this review support previous research emphasizing the importance of preventing child maltreatment and mitigating its negative consequences (Carr et al., 2018; Gardner et al., 2019). Achieving this goal requires implementing evidence-based child protection policies and practices that are systematically governed, upheld, and strictly enforced. While reducing child maltreatment remains the priority, the review also highlights the importance of early detection and interventions within multi-tiered systems through regular screening for those who experience negative outcomes associated with child maltreatment, like symptoms of depression. The study suggests that interventions at specific time points during adolescence and young adulthood effectively enable recovery and improvement in depression symptoms. As such, schools, health clinics, and communities should systematically monitor and implement interventions for depression symptoms when child maltreatment has been identified. To facilitate this, professionals should employ the BDI (Beck et al., 1961) and Patient Health Questionnaire (PHQ-9; Spitzer et al., 1999), which are reliable screening tools for depression in children and adolescents (Roseman et al., 2016). When identifying incidents of child maltreatment, professionals should follow the National Institute for Health and Clinical Excellence guidance rather than relying on standardized tools (McTavish et al., 2020). Consequently, individuals should be regularly monitored for changes in depression symptoms and other comorbid conditions that may arise.
Furthermore, a thorough investigation into factors that escalate and de-escalate depression symptoms for those with child maltreatment experiences is warranted to inform interventions. Confirming initial findings of intrapersonal, interpersonal, and environmental factors is crucial, alongside examining when these factors are most effective in mitigating depression symptoms associated with child maltreatment. Evidence-based interventions that reduce risk and strengthen protective factors should be routinely implemented in schools and communities to address depression symptoms for individuals with child maltreatment histories. This review provides valuable insights for designing interventions tailored to individuals who have profiles of experiencing child maltreatment and subsequent depression.
Strengths and Limitations
Although there have been a substantial number of reviews exploring the relationship between child maltreatment and depression symptoms, this review is the first known to explore the longitudinal relationship between child maltreatment and depression symptom changes for adolescents and young adults. This review is strengthened by the wide range of search terms and the extensive number of articles screened from databases and journal hand searches. Unlike previous reviews, the study avoids limitations imposed by unrestricted methodologies (i.e., type of child maltreatment, measurement tools, and analysis type), thus providing accurate insights into the current state of research in this field.
The review is limited by potential “file-drawer bias,” whereby negative or nonsignificant results are underrepresented in publication, potentially impacting the findings obtained (Rosenthal, 1979). Second, while the findings demonstrated an association between child maltreatment and depression symptoms using longitudinal studies, the study is unable to establish causation and contains studies with varying sample sizes as well as a variety of subtypes measured, which may impact findings. Although the initial protocol planned to conduct a meta-analysis, this was not possible due to the substantial variability in the included studies’ data. Third, studies in languages other than English were excluded due to time constraints. The inclusion of non-English publications may have yielded additional evidence from different cultural perspectives and, therefore, influenced the findings of this review. Based on these limitations, the findings from this review should be interpreted with caution.
Conclusion
This review highlights the complex relationship between child maltreatment and depression symptoms in adolescence and young adulthood. While child maltreatment often leads to worsening depression symptoms, slight improvements may occur over time. Further research using multi-wave analyses and rigorous measures is needed to strengthen the evidence. Modifiable external factors could influence depression symptom changes, but more studies are required to identify the most impactful factors and timing. These findings stress the need for better early detection systems and more research on recovery from child maltreatment and depression symptoms.
Supplemental Material
sj-docx-1-tva-10.1177_15248380251361050 – Supplemental material for Depression Symptom Trajectories Following Child Maltreatment: A Systematic Review of Longitudinal Studies from Adolescence to Young Adulthood
Supplemental material, sj-docx-1-tva-10.1177_15248380251361050 for Depression Symptom Trajectories Following Child Maltreatment: A Systematic Review of Longitudinal Studies from Adolescence to Young Adulthood by Nicola Binks, Kerryann Walsh, Alimila Hayixibayi, Areana Eivers and Adrian B. Kelly in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review is supported by the QUT Research Training Program Stipend Scholarship and the Australian Government’s annual research block funding to higher education providers for support to students undertaking research higher degree studies.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.