
Abstract
At present, our understanding of trauma’s complexity is underdeveloped, particularly with regard to intergenerational effects. In this paper, we review peer-reviewed literature on parental trauma and child well-being, focusing on mediating factors. We conducted a global systematic review of longitudinal, observational studies assessing mediators between a parent’s traumatic exposure and their children’s well-being. The primary outcome of the review was quantitative measures of child well-being (physical and psycho-social) assessed when the child was 18 years or under. We considered the following experiences as trauma exposures: intimate partner violence, rape, sexual assault, victimization during violent crime, childhood abuse, and exposure to direct, immediate threats to personal survival during war, political unrest, natural disasters, and sudden, critical injury/illness. Thirty-two studies met our inclusion criteria. The two most common mediator categories were caregiver mental health (n = 13) and parenting behavior (n = 10). Other studies measured aspects of the parent–child relationship (n = 9), maternal stress factors (n = 5), parental physical health (n = 2), and child-level factors (n = 6) as mediators. Almost all included studies (n = 28) detected a mediation effect. The majority of studies (n = 21) cited robust theoretical frameworks to support their mediator and outcome choices. Studies varied in quality, but most used appropriate, formal mediation analyses. Several study designs could be enhanced by methods to improve precision and reduce bias. Currently, there is little consistency in how similar constructs are measured between mediation studies. We did not locate any studies in low-income countries, and few studies examined aspects of family dynamics, physical health, environmental characteristics, or paternal factors.
Keywords
Background
Evidence from a number of countries suggests that the majority of adults (70%) have experienced a traumatic event in their lifetime (Benjet et al., 2016). Despite this pervasiveness, the public health implications of intergenerational trauma—experienced across the parents’ life course—are not fully characterized (Magruder et al., 2017). Furthermore, existing literature has largely focused on specific forms, rather than the full domains, of traumatic experiences; these studies often treat trauma as a “discrete entity” passed on to offspring in the form of post-traumatic stress disorder (PTSD) or other psychopathological outcomes (Chou & Buchanan, 2021). However, emerging evidence points to the intergenerational effects of trauma on a range of health and well-being outcomes.
For example, a parent’s own adverse childhood experience (ACE) has been found to correlate with poor emotional and physical health outcomes in their children (Plant et al., 2018). In a population-based household survey conducted in the United States, authors noted that the odds of poor overall health (OR = 1.19; 95% CI [1.07, 1.32]) and asthma (OR = 1.17; 95% CI [1.05, 1.30]) among children increased for each additional ACE experienced by their parents (Felice et al., 2018). Similarly, a large cohort study in Norway found that a mother’s own experience of being abused as a child was positively associated with her toddlers’ externalizing problems (emotional abuse: B = 0.6, 95% CI [0.4, 0.7]; physical/sexual abuse: B = 0.4, 95% CI [0.3, 0.6]) (Myhre et al., 2014). Concerning other forms of parental lifetime trauma, a systematic review of traumatic experiences among refugee families noted that offspring of Holocaust survivors had a greater lifetime prevalence of PTSD as well as other mental health complaints involving low mood and anxiety compared to controls (Sangalang & Vang, 2017). Similarly, a study among Australian veterans of the Vietnam War who had a PTSD diagnosis observed an increased lifetime risk of PTSD among their children (OR = 3.47, 95% CI [1.68, 7.15]) (O’Toole et al., 2018).
As indicated by this emerging evidence, the intergenerational effects of parental trauma on child well-being outcomes are wide-ranging. However, it remains unclear how these effects occur. The most well-characterized proximal effects of trauma are on common mental disorders such as anxiety and depression, as well as the trauma-specific condition known as PTSD (Kleber, 2019; Steel et al., 2002). In addition, trauma has been linked to the development of many physical health complaints, including both psychosomatic and chronic illnesses (Yaribeygi et al., 2017). Many of these proximal effects of trauma likely also affect parents in ways that shape their parenting. For instance, a systematic review found that a parent’s intimate partner violence (IPV) victimization was negatively associated with their use of positive parenting practices (r = −.08; 95% CI [−0.12, −0.04]); they also found a positive correlation between IPV and parents’ physical aggression toward children (r = .17; 95% CI [0.11, 0.23]) (Chiesa et al., 2018). In addition, a meta-analysis revealed that parents with higher levels of war exposure (with respect to both frequency and severity) exhibited lower levels of warmth and higher levels of harshness toward children (Eltanamly et al., 2019).
Existing evidence has repeatedly pointed to the importance of a parent’s role in children’s lifelong development (Collins et al., 2000; Stack et al., 2010). For instance, positive parenting aspects such as parent–child relationship quality and positive discipline are associated with child prosocial behaviors (Knafo & Plomin, 2006; Ferreira et al., 2016). Conversely, negative parenting traits such as harsh parenting and neglect have been implicated in poor child well-being (Jackson & Choi, 2018). By identifying mechanisms operating between a parent’s experience of trauma and their children’s well-being, we can isolate aspects of a parent’s traumatic experience that can be tested and targeted to improve child well-being outcomes. Improved understanding of these mediators also enhances our public health rationale to support interventions that may have multigenerational benefits.
Evidence to identify and characterize the mediating factors on the causal pathway between a parent’s exposure to a range of traumatic events and their children’s well-being has not yet been investigated systematically. In this review, we will use an expansive definition of parental trauma, including many different types of traumatic experiences that meet the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) definition of “actual or threatened death, serious injury, or sexual violence.” Through our review, we aim to (a) identify and characterize the mediators of the effect of parental lifetime trauma on child well-being; (b) summarize and critique the empirical evidence for these mediators; and (c) summarize the key theoretical mediation frameworks used to inform these analyses. Our findings will benefit both researchers and practitioners as they navigate the complex effects of trauma and establish interventions to mitigate its effects on parents and their children.
Methods
We conducted a systematic review of quantitative studies that considered potential mediators between a parent’s traumatic exposure and their children’s well-being. We present results according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021).
Search Strategy
In May 2023, we conducted a search for English-language, peer-reviewed studies in the following databases: MEDLINE, EMBASE, EBSCO, PsycINFO, PsycExtra, Global Health, Global Index Medicus, and Web of Science. We derived our search terms by conducting a scoping review of literature on parental traumatic exposure and child well-being, including synonyms for “trauma,” “abuse,” “violence,” “crime,” “adverse events,” “crisis,” “war,” “natural disasters,” and “toxic stress.” Our search strategy is in Table S1.
Inclusion and Exclusion Criteria
In our review, we only included longitudinal (at least two time points for outcome variables), observational studies with prospective or historic reports of parents’ trauma exposure status. We did not apply restrictions on types of mediators or analyses. We considered the following experiences for parents’ lifetime traumatic exposure: IPV (emotional, physical, and sexual), rape, sexual assault, victimization during a violent crime, childhood abuse/neglect (emotional, physical, and sexual), and exposure to direct, immediate threats to personal survival during war, political unrest, natural disasters and sudden, critical injury/illness. For crime exposure, we limited measures to those where parents directly answered questions regarding their personal exposure to neighborhood crime or violence. We only included studies where researchers ensured that their measurements of parental trauma exposure preceded their measurements of child well-being.
Our primary outcome was quantitative measures of child well-being (physical and psychosocial), including proxy or third-party reports. We included any type of author-defined measure of children’s physical health. With respect to psycho-social well-being, we included measures like behavioral problems, juvenile delinquency, academic progress, emotional health, peer relationships, etc. We based our criteria for child well-being measures on the UNICEF definition, which covers a broad range of factors: “the true measure of a nation’s standing is how well it attends to its children—their health and safety, their material security, their education and socialization, and their sense of being loved, valued, and included in the families and societies in which they are born” (Helseth & Haraldstad, 2014, p. 746). To be included, measures of child well-being must have been assessed when children were 18 years of age or under.
We did not include chronic illness as a form of traumatic exposure. We excluded studies that measured secondary parental trauma or those without a comparison group (e.g., mass trauma studies where everyone was exposed to the same traumatic event). We excluded neonatal child well-being outcomes measured between birth and 4 weeks old unless they were part of a series of longitudinal measures extending past this age range. We did not include ACEs as measures of child well-being, but instead considered these as a potential mechanism (not an endpoint of child well-being) by which a parent’s exposure to trauma could then go on to impact a child’s well-being. We excluded reviews and data syntheses.
Database Search and Screening
After executing the search strategy, we identified 59,814 articles generated through the databases. After excluding 17,017 duplicates, two reviewers independently screened abstracts using the inclusion criteria, but did not limit studies to mediation analyses at this point. The first author (J. K. M.) screened the majority of abstracts. The second reviewer (T. R.) screened an enriched sample of 0.5% of the total number of abstracts (a subset containing a higher proportion of included studies than in the overall sample: 50% excluded studies and 50% included studies). We used this enriched sample to calibrate the agreement rate between reviewers (98% agreement was achieved). The first author and the second reviewer resolved any inconsistencies via discussion, with the first reviewer making appropriate changes to our screening methodology. Next, J. K. M. manually excluded 8,739 out of the total of 42,670 abstracts using the Rayyan Intelligent Systematic Review software (Ouzzani et al., 2016).
Rayyan uses artificial intelligence to generate a study rating based on manual inclusions and exclusions by human reviewers. Following her manual exclusions, J. K. M. used Rayyan’s automation tool to exclude a further 32,609 studies from the remaining 33,270 abstracts, based on their obtaining a relevance rating of 2.5/5 stars or below. This rating level was chosen since it was the midpoint of the range of possible ratings. We assessed the appropriateness of this cut-off by reviewing a random selection of 5% of all abstracts that scored 2.5 and below, to lower this threshold if it was found to exclude potentially relevant studies. Our review of this sample found no abstracts eligible for inclusion and we concluded that Rayyan was correctly identifying studies for exclusion. To be conservative, we chose not to raise the threshold further. See Figure 1 for the PRISMA flow diagram of screening processes.
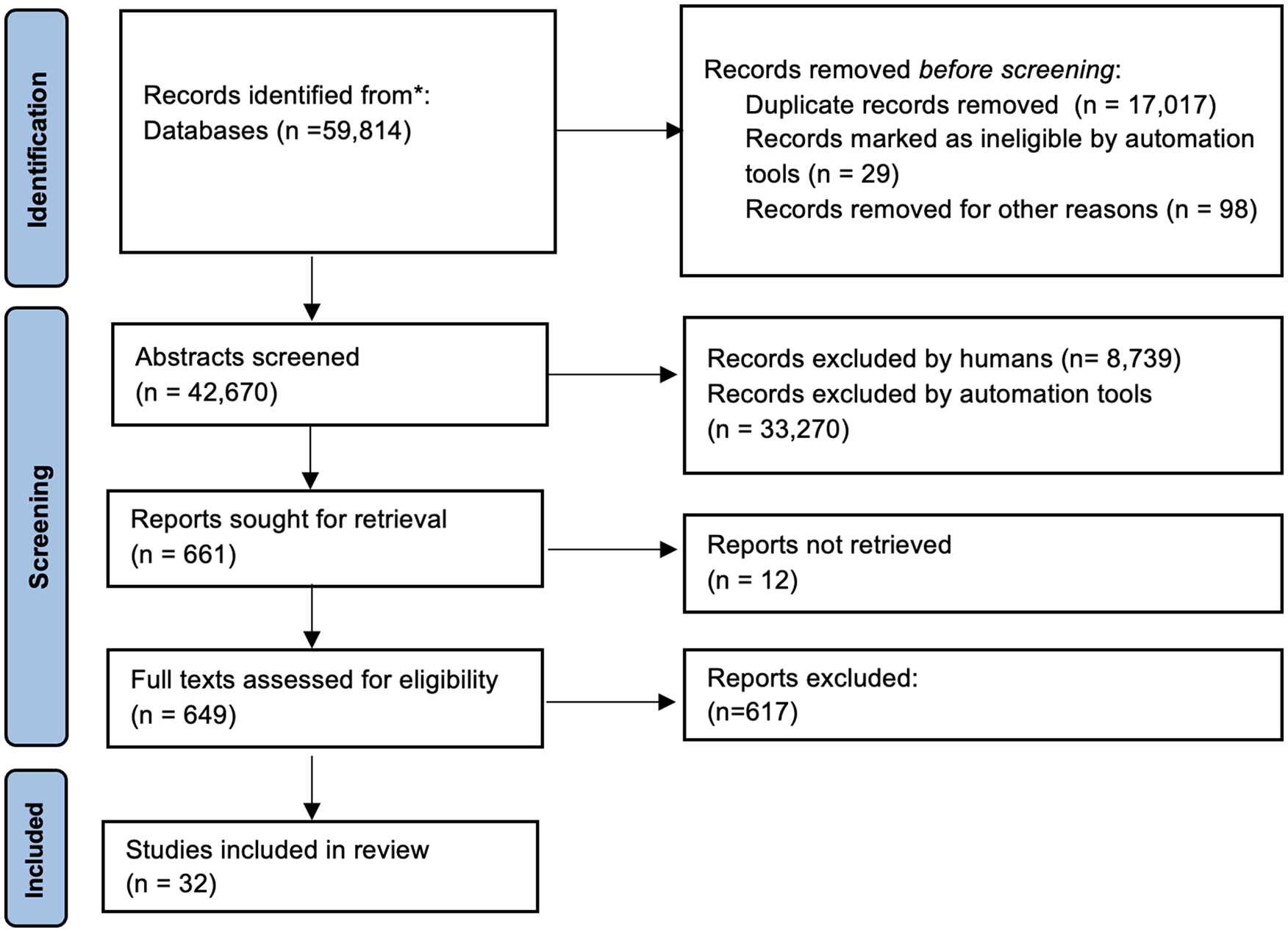
PRISMA flow diagram for systematic review (search conducted in May 2023) of mediators between a parent’s experience of trauma and their children’s well-being.
After abstract screening, J. K. M. and the third reviewer (G. M. E.) completed full-text screening for the remaining 661 studies. During this full-text screening, we used the same inclusion criteria to determine study eligibility; however, we now further limited studies to those that assessed mediation. We tested agreement between J. K. M. and G. M. E. by comparing their assessments of a random sample of 10 full-text articles (we achieved 100% agreement after comparing decisions). We were unable to locate 12 full texts despite a thorough search of available databases.
Data Extraction
J. K. M. and G. M. E., as well as two other researchers (J. L. and S. D. R.), extracted relevant study data from the included full texts (n = 32) using a form based on the CEBMA critical appraisal tool (Center for Evidence Based Management, 2014). J. K. M. then compared each extraction form with its full text to verify its accuracy. Data included information on study design, methods, details of the exposure, mediator, and outcome measures, results of overall effect measures, mediation results, study strengths, and limitations.
Quality Scoring
J. K. M. assessed all 32 included studies to determine their quality level. The quality scoring system was based on a combination of the CEBMA critical appraisal tool and an adaptation of a mediation checklist tool originally developed by Lubans et al. (2008) and later adapted by Rhodes and Pfaeffli (2010) and Teixeira et al. (2015). We rated studies using 12 questions with yes (1) and no responses (0), which were combined to compute a global score (Table S2). Questions assessed the suitability of research questions, the validity and rigor of research methodologies, and the robustness of statistical analyses.
Data Synthesis
First, J. K. M. collated relevant aspects of study characteristics and quality assessments. Next, she categorized the theoretical frameworks put forward by included studies both in a table format (see Table 2) and a narrative synthesis (Popay et al., 2006). Then, J. K. M. performed a pictorial synthesis grouping mediators into categories and highlighting the measures used for each category (see Figure 2). Next, J. K. M. summarized results of studies’ mediation analyses in a table (See Table 1; final column) and a narrative synthesis. Lastly, J. K. M. reviewed mediator categories to identify and list evidence gaps around exposure, mediator, and outcome variables (see Figure 3).
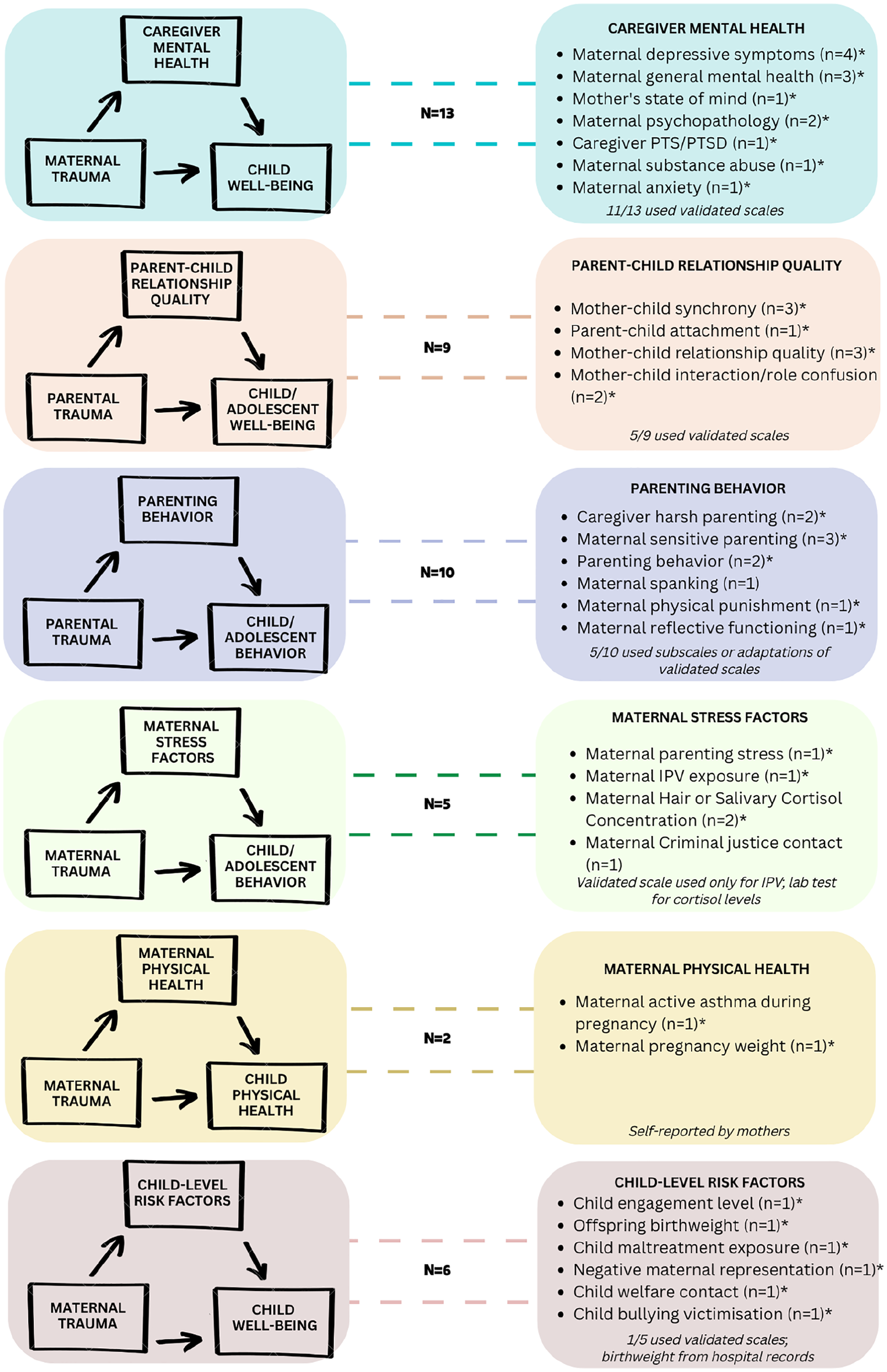
Domains of mediators assessed between parental trauma and child well-being.
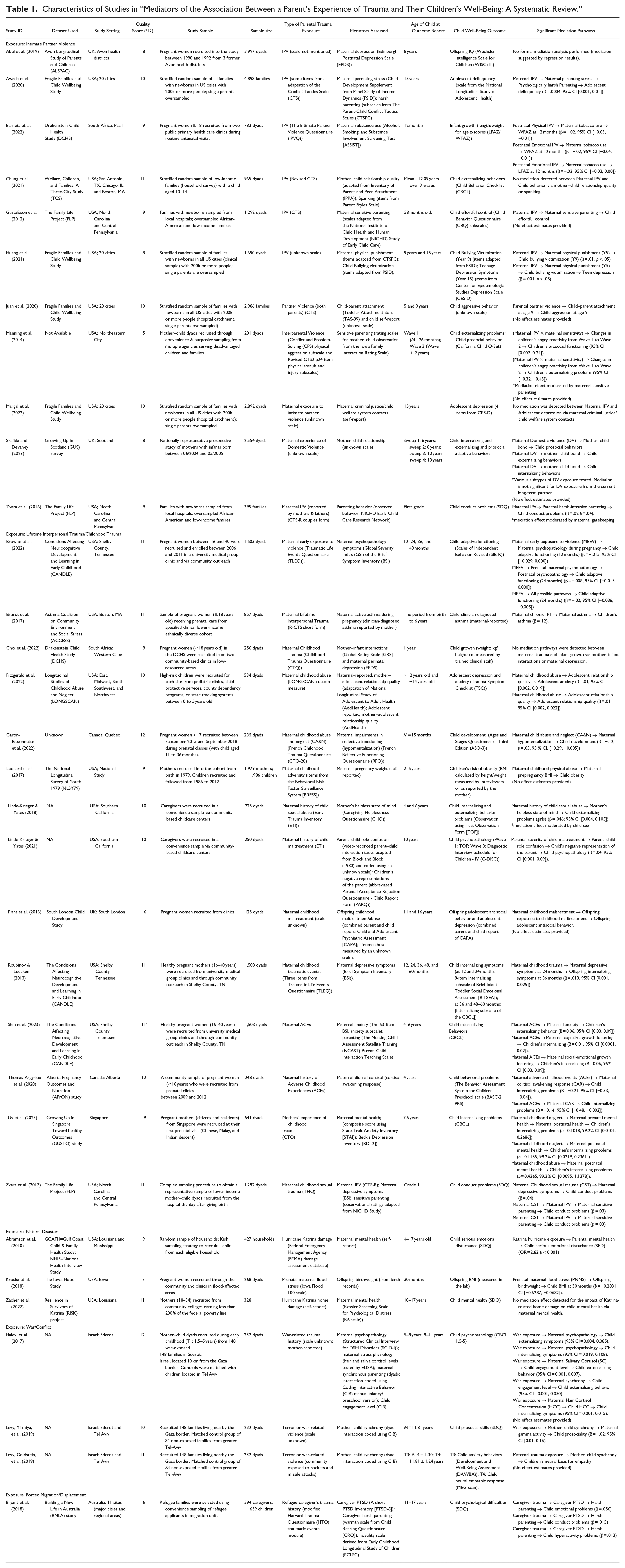
Characteristics of Studies in “Mediators of the Association Between a Parent’s Experience of Trauma and Their Children’s Well-Being: A Systematic Review.”
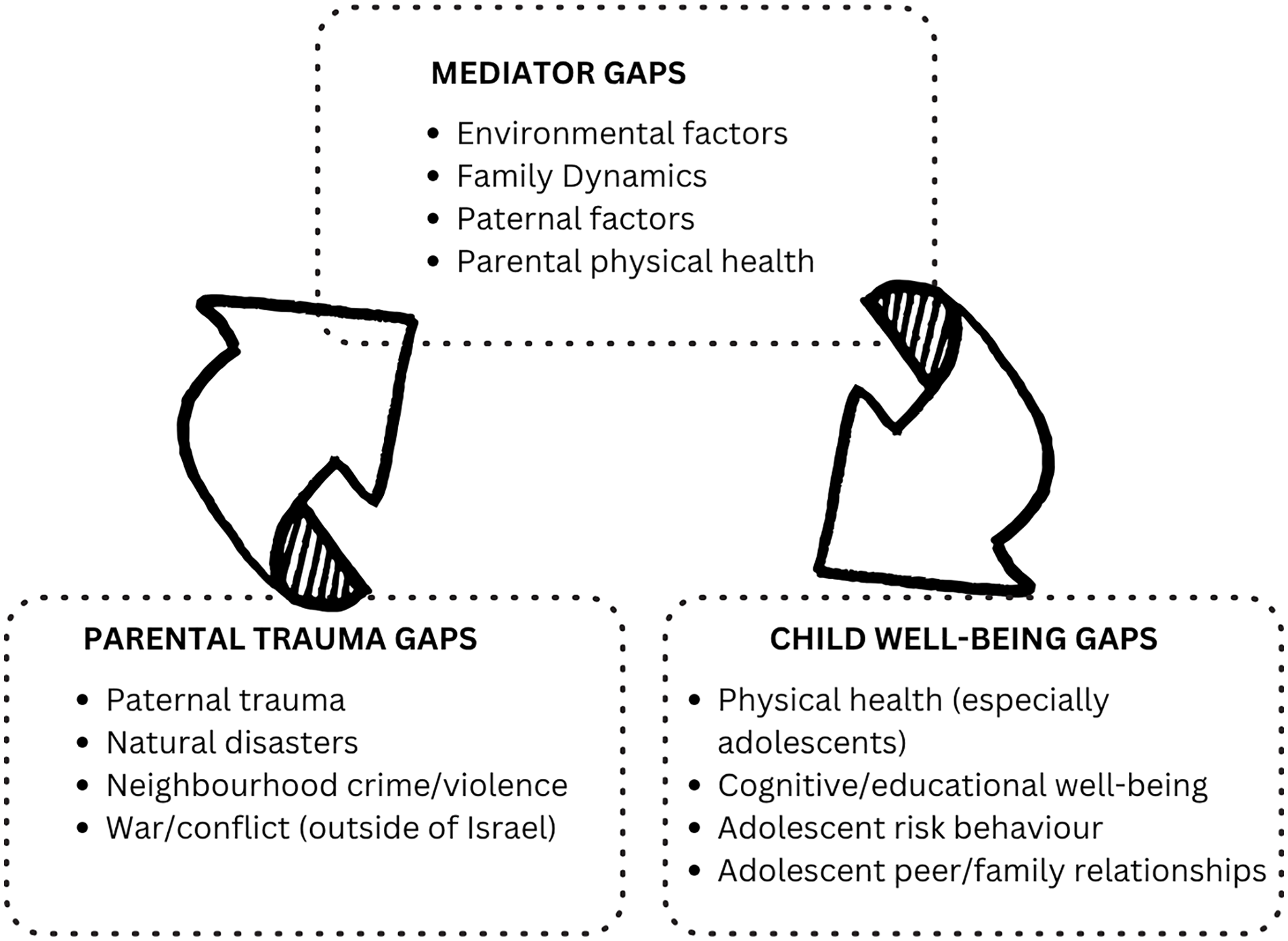
Summary of the gaps in exposure, mediator, and outcome variables among studies looking at the effect of parental trauma on child well-being in this review.
Results
Design and Characteristics of Included Studies
In total, 32 studies were identified as eligible for this review. Table 1 gives an overview of the study context, research design, and results for each of the included studies. Publication dates ranged from 2010 to 2023. Studies were based in the United States (n = 20), Canada (n = 2), the United Kingdom (n = 3), Israel (n = 3), Singapore (n = 1), South Africa (n = 2), and Australia (n = 1). There were no studies from low-income countries (LICs). Nine of the studies recruited participants via hospital catchments or clinics. Eighteen studies used household or community-based samples, and five used mixed samples (both community and clinical sources).
Most studies used cohort samples (n = 21) or cohort subsamples (n = 11). Sample sizes ranged from 250 to 4,898 child participants (median = 590). Only four studies assessed trauma exposure in both fathers and mothers. The most frequently occurring parental trauma exposure was parents’ own experience of childhood trauma (n = 13), followed by IPV (n = 11). Other studies evaluated effects of parents’ exposure to lifetime interpersonal trauma (n = 1), natural disaster (n = 3), terrorism or war (n = 3), and refugee trauma (n = 1). Measures of child well-being were assessed through a wide range of ages, from birth to 17 years old. Child well-being outcomes ranged from physical health (n = 5), intelligence measures (n = 1), mental health (n = 9), behavioral problems (n = 16), and other social-emotional difficulties (n = 8).
Quality Assessment
The quality scores of included studies are reported in Table 1. Many studies (78%) provided adequate descriptions of their cohort selections with clearly defined and objective criteria. About two-thirds of reviewed studies (69%) used validated methods or a clinical scoring system to measure exposures, and just over half (53%) used validated methods or a clinical scoring system to measure mediators and outcomes of interest. Only 63% of included studies provided estimates of precision for measures of effect (confidence intervals or standard errors). Some studies either made no mention of adjusting for confounding variables or did not control for all reasonable confounders of the exposure–outcome relationship in their analyses (66%). This determination of “reasonable confounders” was based on our expectation that studies control for variables related to parents’ age, socioeconomic status, and education level (Plant et al., 2017; Verbeek et al., 2012; Walker et al., 2020). All but one of the studies (97%) performed formal mediation analyses; Abel et al. (2019) assessed maternal depression as a covariate using simple regression rather than mediation analysis. In most studies, researchers (84%) ensured that measurements for the mediator of interest preceded those for child well-being.
Theoretical Framework Applied in Included Studies
Of the 32 included studies, 21 specified a framework for mediation analysis. Table 2 presents a summary of these 12 frameworks (in four overarching categories) and their relevance in the context of parental trauma and child well-being as described by the studies.
Theoretical Frameworks Linking Parental Trauma and Child Well-Being.
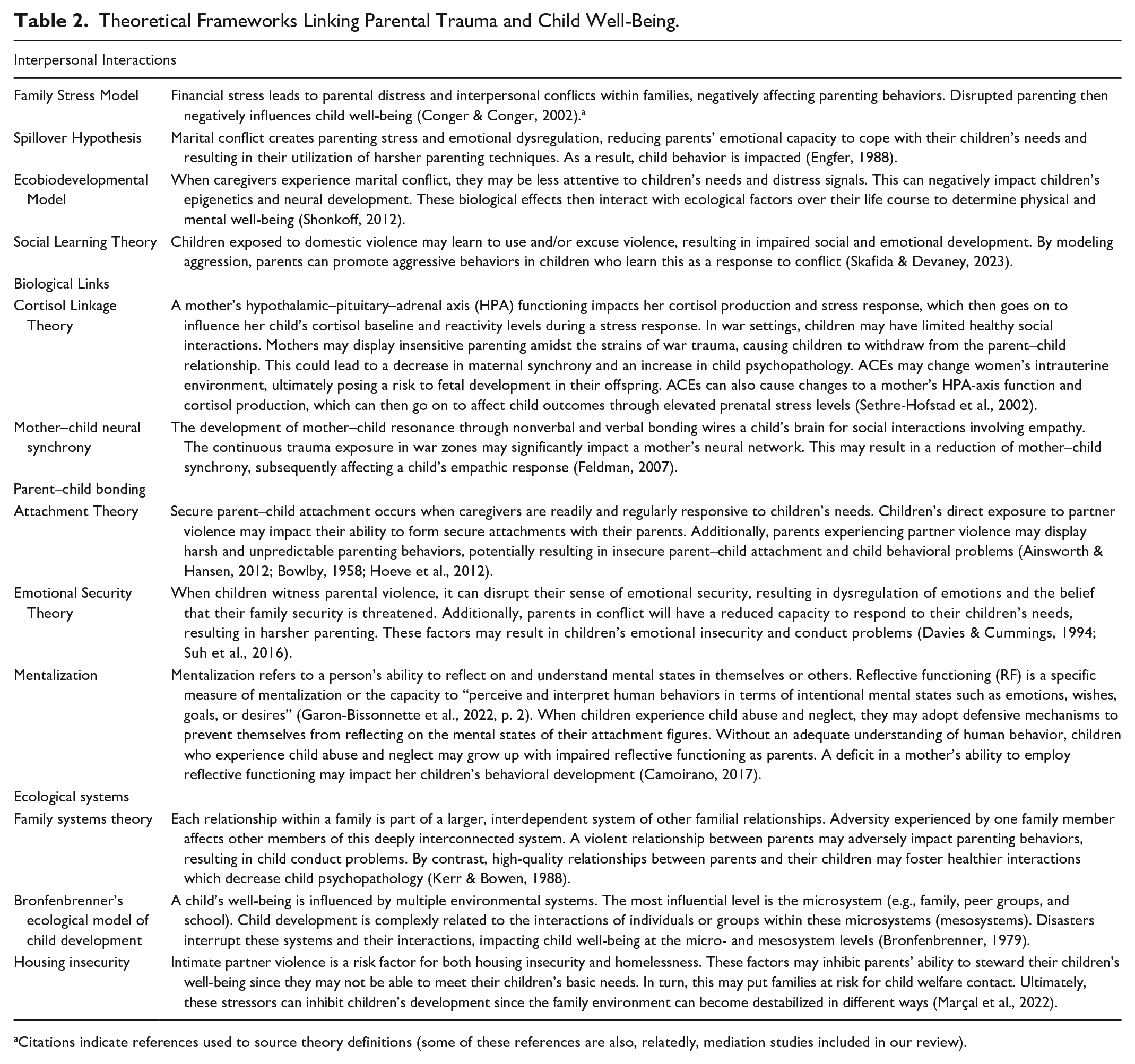
Citations indicate references used to source theory definitions (some of these references are also, relatedly, mediation studies included in our review).
Interpersonal Interactions
Five studies in our review used theoretical frameworks to describe compromised interpersonal interactions within families in the United States and the United Kingdom, and these were all in the context of parental IPV (Awada et al., 2020; Chung et al., 2021; Huang et al., 2021; Skafida & Devaney, 2023; Zvara et al., 2016). For instance, Awada et al. (2020) used the spillover hypothesis in a novel way, to explain the association between parental IPV and juvenile delinquency. Chung et al. (2021) also applied this theory innovatively in their assessment of the effect of maternal IPV on child behavioral outcomes among older children (10–14), an age group noted by Chung et al. (2021) as neglected by previous related studies. Awada et al. (2020) also referenced the family stress model to explain the relationships between maternal IPV, strained family dynamics, and compromised parenting behaviors. Skafida and Devaney (2023) referred to social learning theory to explain why some children who are exposed to parental aggression go on to engage in violence or aggression in their interpersonal interactions. Lastly, Huang et al. (2021) referred to the ecobiodevelopmental framework, postulating that maternal exposure to IPV impacts children’s future risk of depression through mothers’ use of physical punishment.
Biological Links
Our review suggests that biological links between parent and child are a growing area of mediation research. Halevi et al. (2017) used cortisol linkage theory to test maternal stress responses (as measured by salivary and hair cortisol levels) as a mediator between war exposure and child psychopathology in Israel. Thomas-Argyriou et al. (2020) examined the role of prenatal exposure to cortisol in the transmission of maternal ACEs to child behavior problems in Canada. Two other studies based in Israel mention the importance of mother–child synchrony concerning children’s neural bases for empathy in war contexts (Levy, Goldstein, et al., 2019; Levy, Yirmiya, et al., 2019).
Parent–Child Bonding
Six studies in our review employed parent–child bonding theories in their study’s background. Four studies used attachment theory to explain the relationship between parental trauma and children’s behavioral problems, all within the United States and the United Kingdom (Juan et al., 2020; Linde-Krieger & Yates, 2018; Linde-Krieger & Yates, 2021; Skafida & Devaney, 2023). Juan et al. (2020) used this framework to describe the impact of maternal IPV exposure on children’s aggression, testing this association among younger children than previously explored (5 and 9 years).
Linde-Krieger and Yates (2018) also mentioned attachment theory in their conceptualization of the role of a mother’s helpless state of mind in mediating the relationship between a mother’s experience of childhood abuse (resulting in insecure attachment to her caregivers) and her children’s behavior problems; according to Linde-Krieger and Yates (2018), such intergenerational attachment patterns are underexplored in trauma research. In a later study, Linde-Krieger and Yates (2021) considered attachment theory again in a novel application, using the theory to examine the role of parent–child role confusion and the child’s negative representation of parents in mediating the relationship between maternal childhood maltreatment and child psychopathology.
Zvara et al.’s (2016) study was the only study to cite emotional security theory, using it to explain the mediating role of parenting behavior between maternal IPV and child conduct.
Garon-Bissonnette et al. (2022) built their theoretical framework on recent evidence linking mentalization in parents to offspring development, testing reflective functioning as a mediator between maternal childhood neglect/abuse and offspring development in Canada.
Ecological Systems
The six studies that mentioned theories related to families’ ecological systems were all based in the USA. Two separate studies written by a research team at the University of North Carolina, Chapel Hill, used family systems theory to explain the role of parents’ depressive symptoms and parenting behaviors between IPV and child conduct problems (Zvara et al., 2016, 2017). Fitzgerald et al. (2022) used the family systems theory in a novel way to explain the mediating relationship of the mother–adolescent relationship quality between maternal childhood abuse and psychopathology in adolescents, an understudied age group.
Two studies mentioned Bronfenbrenner’s ecological model of child development to explain the relationship between families’ disaster exposure (Hurricane Katrina) and children’s mental health (Abramson et al., 2010; Zacher et al., 2022); however, we did not consider the variable “household stressors” as a mediating factor in our results section since Abramson et al. (2010) did not test its role as a mediator with respect to Hurricane Katrina exposure. Instead, this study was included for its robust analysis of maternal mental health as a mediator.
Similarly, in Marçal et al. (2022), housing insecurity did not meet our review’s criteria for a mediator variable since it was measured at the same time as the exposure, maternal IPV. However, we did include criminal justice and child welfare contact as mediators in that same study, which the authors linked to housing insecurity in their theoretical framework. Marçal et al. (2022) and Abramson et al. (2010) were the only two studies using ecological systems theories to measure forms of environmental stress (housing insecurity and household stressors, respectively), and as mentioned, these were not included as mediators in our review.
The frameworks identified by these studies highlight the complexity of the parenting process and also allude to the potential of familial relationships to influence each other in multi-layered and diverse ways, encompassing effects from the biological level to the broader ecological level. As seen, none of these theoretical frameworks are mutually exclusive, and therefore, in some cases, their proposed mechanisms may be working in tandem to create a complex assortment of influences on child well-being in the context of parental trauma. In addition, all theoretical frameworks documented in this review were applied to studies based in high-income, developed nations. This imbalance in the application of theories points to a need to develop appropriate frameworks for parental trauma and child well-being in diverse settings.
Mediators Identified by Review
The leftmost column of Figure 2 shows simple mediation path diagrams representing the exposure, mediator, and outcome categories tested in the review’s studies. The rightmost column lists the mediation measures used by review studies, grouped into categories.
Effect Measures and Mediation Analysis Results
The last column in Table 1 displays significant mediation pathways for each of the review’s studies. A more detailed description of the studies’ results is found in Table S3. Out of the 22 studies that tested for an association between parental trauma exposure and child well-being before performing mediation analyses, 77% detected an effect (n = 17). In addition, out of the total of 32 studies included in our review, 88% (n = 28) detected a mediation effect. Within the 28 studies with significant mediation results, 14 (50%) reported a full mediation effect. Of note, many studies did not explicitly distinguish between partial and full mediation in their analyses, nor did most calculate the proportion of the effect mediated, precluding conclusions about the extent of mediation observed.
Caregiver Mental Health
Caregiver mental health featured frequently as a mediator of interest among included studies (n = 13) and all but two of these analyses (85%) detected a mediation effect. Only one of these studies included a measure of paternal mental health (Bryant et al., 2018). Almost all studies testing the effects of caregiver mental health as a mediator focused on emotional or behavioral aspects of child well-being; only three incorporated other aspects of well-being by measuring child IQ and infant growth (Abel et al., 2019; Barnett et al., 2021; Choi et al., 2022).
Parent–Child Relationship Quality
Some studies (n = 9) measured aspects of the parent–child relationship as mediators, though only one looked at the father–child dynamic (Juan et al., 2020). Seven of these studies (78%) reported a mediation effect; however, in Levy, Yirmiya, et al. (2019), the mediation analysis revealed a surprising result: war exposure led to lower maternal–child synchrony, which predicted higher maternal gamma activity and higher levels of child prosocial behavior—a counterintuitive correlation. Though Chung et al. (2021) did not detect a mediation effect, they did detect a positive feedback loop between increased child externalizing behavior and poorer mother–child relationship quality. Lastly, two studies went a step further in their investigation of the parent–child relationship by finding evidence for sequential mediation pathways (Halevi et al., 2017; Thomas-Argyriou et al., 2020).
Parenting Behavior
Parenting behavior was frequently assessed as a mediator; studies (n = 10) evaluated both positive and negative aspects of parenting, but only two studies analyzed fathers’ behaviors (Bryant et al., 2018; Zvara et al., 2016). All of these studies examined behavioral aspects of child or adolescent well-being as outcome measures. Most studies testing parenting behavior as a mediator detected a mediation effect, apart from Chung et al. (2021).
Maternal Stress Factors
A few studies (n = 5) assessed maternal stress factors as mediators of child well-being. Three of these presented positive mediation effects (Awada et al., 2020; Halevi et al., 2017; Thomas-Argyriou et al., 2020); contrary to their hypothesis, one study observed that maternal IPV did not mediate the effect of a mother’s experience of childhood sexual abuse on her child’s conduct problems (Zvara et al., 2017). In addition, though Marçal et al. (2022) did not detect any mediation effects of their exposure, maternal IPV, on adolescent depression, they did note a positive mediation effect of maternal IPV exposure on maternal depression operating through criminal justice contact and child welfare contact.
Maternal Physical Health and Child-Level Risk Factors
All studies assessing physical aspects of parental well-being (n = 2) and child-level factors (n = 6) reported mediation effects. Within the physical health and child-level factor categories, there was no repetition of mediator variables between studies.
Discussion
Current State of Mediation Research
Our review has identified a wide range of factors that appear to mediate the effect of parental trauma on children’s well-being. Most studies included in our review found evidence for partial or full mediation of this relationship through their proposed mediating variables. Due to the intentionally heterogeneous nature of our study variables, we can comment on a diverse group of mediators linking various types of parental trauma to child well-being.
Our findings regarding sequential mediation contribute to our understanding of how a parent’s traumatic experience may impact their parenting behavior, and then go on to affect the parent–child dynamic. In Halevi et al. (2017), for instance, the positive association between maternal war exposure and children’s externalizing behavior was found to be sequentially mediated by maternal synchronous parenting and child engagement level. In another study, Thomas-Argyriou et al. (2020) reported that the severity of mothers’ experiences of child maltreatment on children’s elevated psychopathology was sequentially mediated by parent–child role confusion and children’s negative representations of the parent. The role of parenting behaviors in influencing either children’s engagement or their perception of parents on these sequential pathways is important to note since parenting behaviors are modifiable determinants of child health (O’Connell et al., 2015). These detailed and specific mediation pathways can provide valuable insight for programs aimed at mitigating the impact of parental trauma on child well-being.
Parental mental health (n = 13) and parenting behavior (n = 11) were the most commonly investigated mediator types in our review. The prominence of parental mental health among mediation studies was unsurprising given the extent to which trauma has been previously linked to psychological distress and the known impact of parental mental health on child well-being. Still, our review took an important step forward in testing mechanisms operating between parents’ mental distress and children’s physical health outcomes (Pierce et al., 2020). Though parenting behavior is an important grouping to consider, we also identified a need for more consistency in the way it is conceptualized and measured as a mediator between parental trauma and child well-being. For example, six different aspects of parenting behavior were explored using 10 different measures amongst the 11 studies in this category, with the rationale for many of these selections lacking a clear theoretical underpinning. In addition, all 11 studies assessing parenting behavior as a mediator focused on child or adolescent behavioral outcomes, with only one also including a measure of children’s social-emotional health (prosocial behavior). Since parenting behaviors have been repeatedly recognized as important determinants of a child’s overall ability to thrive (Sahithya et al., 2019; Smith, 2010; Ward & Lee, 2020), it is unlikely that behavioral health is the only area of a child’s overall well-being impacted by a parent’s traumatic experience. Testing the mediating effects of parenting behaviors on physical and social aspects of child well-being should therefore be a priority moving forward.
All nine studies looking at parent–child relationship quality were assessed as high-quality. Seven out of these nine studies found evidence for a mediation effect between a parent’s exposure to either IPV, war, or childhood adversity and their children’s well-being. In addition, six different theoretical frameworks were used by this review’s studies to support parent–child relationship quality as a mediator: spillover hypothesis, social learning theory, cortisol linkage, family systems theory, attachment theory, and mother–child neural synchrony. Other forms of trauma have the potential to impact parent–child relationship quality through the pathways described by these same theoretical frameworks. Given the high quality of these studies and their robust findings, parent–child relationship quality should be given priority in future research as a potential mediator between other types of parental trauma (e.g., other forms of violence, natural disaster exposure, forced displacement) and child well-being. Furthermore, emerging evidence suggests that parent–child relationship quality is strongly predicted by a parent’s capacity to reflect on their child’s mental state, isolating a key potential target for interventions amongst parents who have experienced trauma (Rostad & Whitaker, 2016).
Only three studies in our review explored the role of paternal mediators. All three of these studies observed a mediating effect and were conducted in high-income countries (Bryant et al., 2018; Juan et al., 2020; Zvara et al., 2016). The paucity of research regarding paternal mediators is a noteworthy discovery, given the growing consensus that fathers have unique and considerable influences on their children’s development (Videon, 2005). Furthermore, many of the trauma types in this review are disproportionately experienced by men (e.g., crime, violence, war). Given the distinct role that fathers play in their children’s development, research should not neglect fathers concerning either their own experience of trauma or the paternal mediating factors that influence children in the context of parental trauma.
Many of our review studies focused on parents’ exposure to IPV or childhood trauma, theoretically linking these forms of trauma to strained relationships that ultimately affect child well-being. Beyond the experience of IPV or childhood trauma, however, a broad range of other trauma exposures have been implicated in the degradation of interpersonal relationships (Beck et al., 2009). With the potential for compromised social networks and unhealthy interactions, caregivers might experience difficulty forming secure attachments with their children after experiencing any type of trauma. If, for example, parent–child relationship quality is found to be relevant for other parental trauma types, it will prove a key area for intervention among parents living with trauma of any kind. Further, though none of this review’s studies explored mediators related to parents’ social support, such factors might reasonably be expected to impact child well-being in the context of parental trauma. For instance, there is evidence of social support acting as a buffer (or moderator) of the intergenerational transmission of ACEs (Hatch et al., 2020; Thomas et al., 2018). It may be that some factors can be considered for their dual role as both moderators and mediators of the intergenerational effects of trauma, a point for consideration in future research. Finally, emergent mediators like mother–child synchrony, which have thus far only been explored in the context of war trauma, should be considered for their mediating role concerning other types of trauma, whereby a mother’s neural network is disrupted by continuous exposure to distressing events, ultimately affecting her children.
Though most studies in our review reported significant mediation pathways, there were a few exceptions worth noting. For example, with respect to maternal mental health, all but two studies recorded a mediation effect. Zacher et al. (2022) did not detect a mediation pathway between Hurricane Katrina-related home damage and child mental health through maternal mental distress. This may have been due to limited statistical power, given this study’s smaller sample size. However, authors did report statistically significant indirect effects of maternal stressor exposure on child internalizing symptoms through maternal psychological distress in the years following the hurricane. Though this study’s list of maternal stressors did not meet our review’s criteria for traumatic exposure, their findings suggest that disasters’ effects may negatively impact both young survivors and children born post-disaster through maternal stress exposure, which leads to long-term maternal mental health distress. Similarly, Choi et al. (2022) did not find an association between maternal childhood trauma and infant growth through perinatal depression in their Drakenstein study (Choi et al., 2022). This study may also have been underpowered to detect a mediation effect. Furthermore, its authors indicated that children in their study’s context may often be raised by multiple caregivers, potentially buffering the effect of maternal depression on child growth in the context of maternal trauma exposure. These anomalous findings highlight the importance of conducting high-powered, multidimensional studies that consider the full span of parental ecological resources in the context of trauma, as well as the potential benefit of using less traditional methods such as latent class growth analysis to assess the long-term trajectories of parental trauma on child well-being (Choi et al., 2022; Zacher et al., 2022).
Among studies assessing mother–child relationship quality as a mediator, all but one reported significant mediation results. In this case, though Chung et al. (2021) did not detect a mediation effect, they did detect a positive feedback loop whereby increased child externalizing behavior diminished the quality of the mother–child relationship. Most previous studies have found that IPV impacts parenting in ways that detrimentally affect child well-being. However, Chung et al. (2021) explain that their anomalous finding may be in part due to the older age of children in their sample (early adolescence as opposed to younger children). They posit that parents may have more tolerance for younger children’s externalizing behaviors as compared to that same behavior in older children, which may provoke harsher responses. Their inconsistent finding of a child-effects model rather than a parent-effects model emphasizes the importance of mediation studies covering a wide range of child ages across the developmental spectrum and the benefits of using more advanced methods to assess transactional relationships between children and their parents or environment (Chung et al., 2021).
Strengths and Limitations of Our Review
By limiting eligibility to longitudinal studies, we decreased the risk of reverse temporality as an explanation for exposure–mediator–outcome associations. However, this meant excluding some novel cross-sectional studies, such as those using functional magnetic resonance imaging to assess the neural effects of parental trauma. Studies were not screened for mediation analyses until read in their entirety (full text), so it is unlikely that our search strategy missed studies that performed a mediation analysis, if they were otherwise eligible for the review.
Two limitations of our review methods are relevant to our discussion. Although we used a conservative cut-off point with which none of a random selection of 5% exclusions were found to be eligible, there remains a possibility that some studies were excluded at the abstract screening stage by Rayyan’s artificial intelligence system. As more studies are published regarding the sensitivity and specificity of Rayyan’s rating system, future reviews can adjust their cutoff values accordingly (Valizadeh et al., 2022). In addition, the limitation of studies to English language texts may have resulted in fewer inclusions from LICs, possibly inflating this perceived gap.
Overall, there was a wide range of study quality. Generally, studies employed robust methodologies, acquired sufficient sample sizes, and had focused research questions, but we noted that the measurement of mediator and outcome variables could be significantly improved with increased use of validated tools. We also identified the need for more precise effect measures and for confounding factors to be more consistently considered in study designs.
A few studies did not perform sensitivity analyses or use the gold standard for mediation analyses: structural equation modeling (Gunzler et al., 2013; Iacobucci et al., 2007). In some cases, this may have limited authors’ ability to account for bias or reduced the resolution of results. Most exposures were retrospectively assessed, and many were not longitudinal, so our ability to rule out recall bias and understand the temporality of the exposure’s effect on the outcome is limited. This limitation is unavoidable since ethical constraints restrict our ability to make longitudinal, prospective measurements of trauma exposure without intervening. In addition, the statistical power to detect effects remains unclear, as most studies did not report power analyses. Future research should include a priori power analyses to ensure sample sizes are sufficient to detect meaningful effects, improving both validity and reproducibility. Lastly, though many studies oversampled for low-income communities and single parents, few researchers have compared mediation effects between sociodemographic groups to date.
Future Directions for Mediation Research
Overall, research focusing on the mediating effects of parental trauma on child well-being remains limited and would benefit from more studies across all mediator categories and demographic groups. Still, we identified five specific gaps in the current state of mediation research. First, most included studies were based in high-income countries (except for two recent studies based in South Africa, a middle-income country), precluding our ability to assess the relevance of mediators between parental trauma and child well-being in LICs. Such settings should be prioritized in future research, particularly given the higher burden of traumatic experiences in LICs. Second, only three studies considered the role of paternal trauma in shaping child well-being. The effects of paternal trauma and paternal aspects of parenting should be prioritized going forward due to a current lack of evidence in this area. Third, few studies examined the physical aspects of well-being. Despite the limited data available, our review suggests that physical aspects of well-being are important to consider as both mediators and outcomes, and should be prioritized in future mediation research (Brunst et al., 2017; Kroska et al., 2018; Leonard et al., 2017). Theories supporting biological links between parental trauma and child well-being are limited at present; yet, our review indicates that biological links play an important role in children’s outcomes following parental trauma. Fourth, our review included a few studies on natural disasters (n = 3), forced displacement (n = 1), or adult exposure to non-partner violence (n = 1), and no studies assessing neighborhood crime and violence, despite employing an exhaustive list of search terms. As indicated by our theoretical framework analysis, this may be due to a lack of strong theory currently available to support linkages between parental experiences of collective traumatic events and child well-being.
In addition, we found no studies exploring the role of mediators between parental injury or illness and child well-being, even though parental injury has been shown to impact child development through parenting behavior (Cramm et al., 2016). Future studies should prioritize these types of exposures using longitudinal designs. Lastly, despite the range of child ages covered, many of the studies (60%) collected outcome data when children were over 5 years old. Furthermore, 12 out of the 13 studies that did look at child well-being in children at or under the age of 5 measured interpersonal forms of parental trauma; this suggests a paucity of research on the effects of other types of parental trauma on early child well-being. Future studies should focus on longitudinal research from birth to adolescence to develop a life-course perspective and examine the mechanisms that link various forms of parental trauma to child well-being (which might vary depending on the type of trauma experienced).
Implications for Practice
Our results underscore the importance of prioritizing parental mental health and positive parenting behavior as targets of both parenting interventions and programs aimed at stabilizing families in the context of trauma. Furthermore, we found evidence to suggest that early markers of mother–child relationship quality, such as mother–child synchrony and mother–infant interactions, are important mediators of parental trauma and child well-being. Interventions that capitalize on improving the mother–child relationship at earlier stages of development should therefore be prioritized, particularly in communities with high rates of trauma. In addition, we observed substantial overlap among parental trauma types with respect to the theoretical frameworks used and the mediators that transmit an effect on child well-being in our review. In these instances, family interventions can address a broad range of parental trauma exposures by targeting shared mediators that link various forms of parental trauma to child well-being. Such interventions should not only highlight the need to improve parent–child interactions, but also acknowledge the importance of securing parents’ own physical, mental, and social well-being as important outcomes.
Conclusion
In conclusion, we have identified a range of factors that appear to mediate the relationship between parental trauma and child well-being. Researchers to date have been eclectic in their selection of potential mediators, yet with little consistency in how similar constructs are measured. We encourage researchers to use specific, well-defined mediators with validated measures where available to enhance our understanding in this area. Researchers in this field have overlooked low- and middle-income countries (LMICs) and have neglected aspects of family dynamics, physical health, environmental characteristics, and paternal factors. In addition, future studies should consider complex, sequential mediation analyses to investigate how biology, behavior, and family dynamics interrelate on the pathways between parental trauma and child well-being.
Critical Findings of Review.

Implications for Practice, Policy and Research.
Supplemental Material
sj-docx-1-tva-10.1177_15248380251357616 – Supplemental material for Mediators of the Association Between a Parent’s Experience of Trauma and Their Children’s Well-Being: A Systematic Review
Supplemental material, sj-docx-1-tva-10.1177_15248380251357616 for Mediators of the Association Between a Parent’s Experience of Trauma and Their Children’s Well-Being: A Systematic Review by Jihana Kristin Mottley, Karen Devries, Phil Edwards, Georgina Miguel-Esponda, Tessa Roberts, June Larrieta and Sujit D Rathod in Trauma, Violence, & Abuse
Footnotes
Data and Code Availability
The analytic code necessary to reproduce the analyses presented in this paper is publicly accessible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.